
Abstract
The patients increasing number and growing shortage of medical staff are acute problems that face the healthcare industry today. Healthcare robots are being installed to solve this problem, since they have sufficient potential to solve the problems. The healthcare robot initiative success is not only based on the executives’ decisions and robot designers but also on medical staff members’ willingness to adopt healthcare robots. Nowadays, there are gaps in our understanding about the evaluation of staff changes in using robots. This study investigated the factors involved in the robots using in Thai government hospitals based on the results of 466 questionnaire respondents. The medical staff was selected randomly for data collection. The Confirmatory factor analysis (CFA) and a structural equation modeling (SEM) are tools used in data analysis. The findings confirmed that all four UTAUT constructs of the study, namely, the facilitating conditions, social influence, effort expectancy, performance expectancy, and concerns about safety, significantly predicted the use of robots (p < .01). Medical practitioners under 35 years of age tended to accept the technology better than their more senior counterparts. The staff’s intentions and facilitation of support played a key role in adopting and using robots. Lack of technical knowledge was perceived as a barrier to technology adoption. The results also indicate a significant negative effect in the relationship between the medical staff’s behavioral intention and barrier/resistance to the healthcare robot using. This study also identifies key factors for medical staff to make acceptance decisions in relation to healthcare robots.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Currently, one of the key problems facing healthcare organizations is that the number of patients (adult, senior, and impaired) has increased while the number of medical staff (physician, nurse, and other staff) has decreased over time. Therefore, there are not enough doctors and staff for patients [1], which is a major problem that the healthcare industry is facing worldwide [2]. The increasing patient population has caused organizations to resort to healthcare technology to solve these problems and to increase healthcare service performance [3, 4].
Now, the healthcare technology is being developed both in the research section and actual use for healthcare service [5] because they have the potential to improve healthcare service quality. Previously, most studies in the healthcare technology field have focused on the healthcare information technology topic [5, 6]. Due to the increasing needs of patients, medical robots are therefore used to meet these needs [7].
Healthcare robots have become an important tool, since they can improve diagnostics and treatment capabilities, reduce rest time, reduce the medical errors number and improve the overall quality and cost effectiveness of healthcare service systems [4, 8]. However, the healthcare robot initiative success is not only based on robot designers and corporate executives but also depends on the intention of medical staff to bring these robots to health as well because medical staff members are the healthcare robot users who provide services to patients. The executives and robot designers must understand the factors and facilities that cause medical staff to accept the use of healthcare robots. Therefore, one of the ways to meet the need of patients are to explore the factors related to the adoption of healthcare robot technology to improve the service quality of medical staff [1].
Previously, robot study for healthcare mainly has focused on the use of technical and design [7], and an adoption study represents a new topic in this field. From the literature review, it was found that the acceptance model has been applied to specific cases of healthcare robot adoption and they have identified critical factors for this context, the example is the study of Alaiad A and Zhou L, which studied the factors of home healthcare robot adoption [6]. However, when the organizations outlay in new technology, dealing with user resistance cannot be avoided [8]. Therefore, it is necessary to determine which key factors influence technology adoption and the examination of obstacles as well as the relationship between the behavioral intention of using robots and obstacles.
Now, the healthcare robot using studies have been limited, and most of them do not check the resistance/barrier factors of users [9]. The Cenfetelli’s research is inspiration of this study observing that previous technology usage theories, the example is the technology acceptance model (TAM), remained to focus on the positive (enabling) awareness of user involved in the use of technology while ignoring the negative (inhibiting) awareness that may prevent technology usage [10]. Although the specific technology usage inhibitors was done identify in Cenfetelli’s research, he only helped us understand the impact the technology usage inhibiting perceptions [11]. Based on our literature review, the barrier factor in this research is adapted from the barrier theory in suitable healthcare robot contexts.
According to technology acceptance theory, the UTAUT model is used for healthcare robot factor usage. This research offers that a user’s use behavior regarding healthcare robots is based on two enablers: facilitating conditions and behavioral intention. At the same time, the inhibitors (barrier factors) affect the behavioral intention to healthcare robots using. From a practical perspective, the barrier factors cause the user to resist technology use: understanding why users exhibit anti-robot behavior can help hospital management and healthcare administrators design appropriate intervention management to reduce the user barriers and their effects on healthcare policy. Thus, this study objectives include 1) identifying the acceptance factors that affect medical staff’s to healthcare robots adoption and what enablers most influence to use healthcare robot; 2) investigating whether the medical staff’s barrier to healthcare robot use significantly affects to the robots using; and 3) to clarify that barriers most influence the decision to resist the healthcare robots.
2 Background
2.1 Healthcare problems and trend
Currently, healthcare institutions face inadequate healthcare facilities, and there are not enough medical staff to address patient problems [1, 12, 13]. This situation causes diagnostic errors and longer wait time for treatment and lowers the effectiveness of the process due to the fatigue and stress of the medical staff, which has an effect on patient safety [12].
Now each healthcare organization has installed healthcare technology for solving the problem and optimizing its service quality. First, hospitals had installed information technology, which is an indispensable facilitator [1]. After that, healthcare technology has grown and developed in parallel with the evolution of healthcare services and along with the needs of the patients, especially in the robot field. So, the healthcare organizations have installed healthcare robots, because they can improve the healthcare services quality.
2.2 Robots
Now, robots have been widely used and developed, but robot is not clear definition for acceptance from the general public, they don’t have consensus on what qualifies as a robot [13]. Therefore, to understand the Thai definition of robots in this research, the robots are identified by multiple theories. First, a robot is a machine that can work, and some can operate on their own, while others need an instructor, according to NASA [6]. Second, the robot should do one or more of the following: 1). move slightly; 2). Work the mechanical arm; 3). feeling and dealing with the environment; and 4). showing intelligent behavior, as per Thailand Center of Excellence for Life Sciences [13]. Third, a robot is a mechanical tool and the internal mechanisms that can combine integrated with a human or a human agent and can rearrange their work process, according to Saranukromthai’s book 36 [14].
2.3 Healthcare robots
According to NASA, a robot is a machine that can be used to operate, and some can operate on their own but other need an instructor to make the robot work. When these jobs mean healthcare, these robots are called healthcare robots [6]. Now, the large hospitals such as Siriraj hospital, the Bangkok hospital have been recently installed and used for healthcare service. In Thailand, the healthcare process can be divided into detecting the symptoms, diagnosing the disease, treating the disease and preventing the disease, and the healthcare robots can facilitate both direct and indirect patient care to reduce medical errors by developing screening and auditing to improve the accuracy in the system. Healthcare robots used to support the medical staff’s activities will remove some of the workload and improve their productivity. Thai healthcare robots can be divided into three major categories: treatment robots (such as a rehabilitation robot, diagnosis robot, and surgery robot), support robots (such as the physical robot) and medical service robots (such as a pharmacy robot, nurse robot, telemedicine network robot) [4].
Healthcare robots have become an important tool in improving the healthcare system and assist the medical staff at every step of the healthcare process in Thailand, from diagnosis research assistance to training officials to make the system more efficient [4]. Healthcare robots considered in this research, include 1. surgery robots, 2. telemedicine robots, 3. nurse robots, 4. pharmacy robots, 5. physical robots, 6. radiographic diagnostic robot, and 7. a specific healthcare robot.
2.4 Technology acceptance model
Currently, many technology acceptance theories many theories have been proposed, and many researchers have previously applied these theories to explain the health information technologies acceptance [5, 15, 16]. However, these acceptance theories have not been used to describe the acceptance of the use of robot for healthcare in Thai government hospitals. Moreover, previous studies have not considered barrier factors to explain behavioral intention along with adoption behavior. Therefore, this study is the beginning of research on healthcare robot adoption in Thai government hospitals and guides future research about robots in healthcare settings.
The UTAUT was selected for this healthcare robot acceptance study because it was used to study the technology acceptance of each person in the business sector; the theory matches target hospitals, and these factors cover the context of technology adoption because they are combined from other models, thus comprehensively covering all technology acceptance factors. In addition, in the context of previous research, it has shown the accuracy and reliability of the model as well [17, 18].
2.5 Technology adoption and resistance
When a new technology is introduced, the user may accept or resist it. The decision is based on evaluating the changes related to the new system [19]. Due to the failure of healthcare technology efforts, these failures are caused by resistance/barrier of the user [16]. Resistance (Bhattacherjee A and Hikmet N) is not equal to inactivity, as it may mean that the users who use technology do not know about the new technology or are evaluating the technology before implementing it. But, resistance means the technology was considered and rejected by the users [17]. Moreover, Cenfetelli showed that resistance is markedly enhanced by changes in behavior but not using does not lead to such a result. However, the relationship in opposition and technology acceptance must be verified together with theoretical model, because user resistance is an important barrier to using an information system [10]. Currently, the barrier/resistance factor topic is still being neglected and is rarely addressed; therefore, organizations do not receive the benefits of technology as they should. Thus, this research focused on the user barriers, i.e. the user conflict with the changes related to the use of new technology. Moreover, Hsieh and Pi-Jung’s research confirmed that accepted anti-obstruction factors in healthcare technology have a negative impact on behavioral intentions. [20, 21].
2.6 Healthcare robot barrier factors
The obstacles to diffusion research theories involve explaining the differences between inventors and beginners and other ideal behavior [22]. Each barrier factor is very relevant to the problem with the equipment used for all work, which makes the technology acceptance barrier specific with different methods and theories suitable for work [22]. Currently, researchers have conducted studies on the theory of obstacles. Each work has different characteristics depending on the equipment used in the study such as Pagani, (2004).
Pagani’s barrier model is applied because it emphasizes the important characteristics of technology, and each factors suit the healthcare robot context [23]. The model includes (lack of) ease of use, functional usability, security and privacy. It presents a comprehensive specific barrier, including technical, safety, time barriers and change resistance factors.
3 Research model and hypotheses development
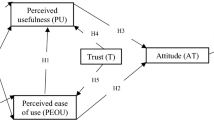
From previous discussions, we use the acceptance and barrier theories as an important theoretical foundation to explain medical staff’s adoption and resistance to healthcare robots. Thus, we propose that medical staff’s use behavior of new healthcare technology is based on two opposing forces: enabling and inhibiting perceptions. In the enabling perceptions, the original UTAUT model is used by not making any structural changes, and the healthcare robot use behavior is based on two enablers of healthcare technology usage: behavior intention and facilitating conditions. The intentions of behavior is influenced by performance expectancy, effort expectancy and social influence. In terms of inhibiting perceptions, we add four barrier factors to new constructs, including a technical barrier (lack of ease of use and a functional usability barrier), safety barrier, time barrier (long time training and setting up barriers), and change resistance. Following Hsieh and Pi-Jung’s research, these barriers are selected as the barrier factors affecting behavioral intention. Healthcare robots are the platform for new technologies in healthcare services; thus, the introduction of a healthcare robot causes significant changes for medical staff in the healthcare process. If the change is large enough due to the natural inclination of human to combat the change, there will be medical staff who are more likely to resist the healthcare robots, resulting in reduced usage behavior. However, the literature review states that few previous studies have cited the relationship between technology adoption and obstacles, and no research has addressed this topic in regard to the healthcare robot field. Therefore, we also examine the relationship between usage behavior and barriers, which is shown in Fig. 1.

The acceptance and barriers in the healthcare robot technology model in this research
According to the UTAUT model, performance expectancy influences behavioral intention. Performance expectancy (PE) is the levels of individual belief that the technology can help increase the efficiency of the technology user [18, 22]. There is a lot of evidence showing the impact of performance expectations on usage intention [24] and even showing that performance predictions are the strongest predictor of intention to use the technology [21]. The performance expectancy rankings are measured by the sufficiency of the medical staff who use the healthcare robots. The ranking of the healthcare robots considers the robot’s nature, which includes reducing waiting time and working time, reducing errors in the process, and increasing safety for patients and management. Robots also helps staff deal with their job more easily. Therefore, we propose the following assumptions about the relationship between performance expectancy and behavioral intention:
-
H1: Performance expectancy has a positive effect on the behavioral intention to use healthcare robots.
Effort expectancy (EE) is the degree of the ease of using that technology or the degree of the ease of using the technology in respect to how easy-to-use the technology appears [25]. The more that the technology can be used easily, the more the users will accept to use the technology. A lot of empirical evidence shows that the expectations of an effort have a direct effect on behavioral intention of the use of technology [26]. Therefore, the healthcare robot adoption should depend on whether the robot is easy to use and does not require any effort. This factor can be distinguished as follows: 1. the healthcare robot is easy to use equipment; 2. the healthcare robot is easy to learn by the user on his or her own; 3. the healthcare robot helps make the user’s job easier, and 4. the healthcare robot is easy to troubleshoot. Therefore, we propose the following assumptions:
-
H2: Effort expectancy has a positive effect on the behavioral intention to use healthcare robots.
Social influence (SI) is the individual perception that the person who is important to the technology user has expectations or believes that each person who uses the technology should use the new technology [25]. The more that the user perceives that other people think that he/she is participating in a particular behavior, the more motivated to follow. In the organization field, this means that the important person in the corporation shows his or her opinions, expectations and beliefs about allowing his or her staff to use new technologies in their own company. In this research, the leader and colleagues of the user believe that healthcare robots can help the user work more efficiently. Previous studies have shown that social influence is important in establishing behavioral intention for using new technology [18, 27]. Therefore, we propose the following hypothesis:
-
H3. Social influence has a positive effect on the behavioral intention to use healthcare robots.
Facilitation conditions (FC) represent the degree of human belief that the corporate foundational structure will support and accommodate the use of new technologies [25]. Sponsorship of technology users may be a type of convenience condition that affects the use of the system. [28]. Users need to have the skills, knowledge, resources, training, and support needed to use robot for healthcare. Some are tentative about the adoption of robots since they lack resources and technical support. There is empirical evidence showing the significant impact of conditions on facilitating the use of intention [29]. Therefore, we expect that recognition of facilitating resources, including support, training, knowledge and skills, supporting the organization and time will affect the behavior to use healthcare robots.
-
H5. Facilitating conditions have a positive effect on the behavior to use healthcare robots.
According to the UTAUT model, the behavioral intention (BI) is the intention to make a judgement regarding the acceptance of some technology. The behavioral intention can be determined by three factors: performance expectancy, effort expectancy, and social influence. Previous studies on technology acceptance confirm that behavioral intention influence is significant for the behavior to use (USE) the new technology [30].
-
H4. Behavioral intention has a positive effect on the behavior to use healthcare robots.
In general, the mediators are personal factors that do not directly affect the making of decisions regarding whether to use new technologies, but they will support behavioral intention (BI) via performance expectancy, effort expectancy, social influence, and facilitating conditions. According to the UTAUT model, there are four mediators: age, gender, experience, and the voluntary use.
-
H6. Different gender has different interaction effects on healthcare robot acceptance.
-
H7. Age has positive effects on healthcare robot acceptance.
-
H8. The user’s experience has positive effects on healthcare robot acceptance.
-
H9. User’s voluntariness has positive effects on the social influence of the user.
Norzaidi et al. examined the relation between user resistance/barriers and usage [8]. Suggestions for new systems often make important changes to the user’s original work process. The users who reject the new technology for the first time, they may finally accept the use because they do not have any other options. In order for their work to be completed, it is necessary to use it. Therefore, the medical staff are forced to use the healthcare robots to achieve their objectives since there are no alternatives. There are also cases in which the medical staff may use the system voluntarily, but they may stop using the system later. Another factor that may be an obstacle that make anti- robot users healthcare is prior bad experience. Medical staff may feel comfortable, because the healthcare robot can respond to their job, reduce their errors, and offer benefits that they expect; however, if the robot fails to help in their job, then the staff may be unwilling to use the robot. Previous studies have shown the negative impact of behavioral barriers on new technology [21, 24, 31].
(Lack of) ease of use barriers represent a person’s feeling that the technology was difficult to use when he or she actually had to use it, that it was not flexible and that he or she had to study hard. BenMessaoud, Kharrazi, & MacDorman proposed that a lack of ease of use was the factor that causes medical staff to refuse surgery robots. The staff want easy to use equipment and if the healthcare robot is complicated, then they will use the traditional tool [3]. In addition, a complex technological system is often unacceptable, and the users are usually hate to dedicate their time and energy to training in use or implementation [27]. In addition, Alaboudi et al. confirm that if the technology is not easy to learn, the medical staffs will not waste a lot of time and need a lot of technical support to use that technology [32]. This research indicates that medical staff find healthcare robots complicated, difficult to use when they actually need to work and that they find the learning difficult. Previous research confirms which the lack of ease of use is a barrier for healthcare technology adoption [3, 33]. Therefore, the obstacles in (lack of) ease of use has a negative impact on the behavioral intention of using robot for healthcare.
The functional usability barrier is the feelings of users that technology cannot meet their work needs or help their job effectively enough. BenMessaoud, Kharrazi, & MacDorman confirmed that the functional usability barrier is one of the main constructs which has a negative impact on the use of robot technology. Some doctors stated that surgery robots are just a marketing tool and that they lost patients to the surgeons who perform robotic surgery. Additionally, some surgical doctors are unable to show robot use due to the limited number of patients that can use robots [3]. Moreover, Alaboudi et al. found that if healthcare robots cannot respond to their jobs, the medical staff will not all of a sudden accept the use of healthcare robots [32]. This means that the medical staff feels that the healthcare robots cannot meet their needs. Prior research shows that this factor is the barrier to using healthcare robots [3, 33]. Therefore, the functional usability barrier has a negative effect on behavioral intention of using robot for healthcare.
(Lack of) ease of use barriers and functional usability barriers are the barriers in the working process, and they are the same type of healthcare robot barrier. We combine the two factors together to create a technical barrier (B1). Therefore, technical barriers have an influence on behavioral intention.
-
H10a. Technical barrier (B1) has a negative effect on the behavioral intention to use healthcare robots.
Safety barrier (B2) is the feeling of user that using the technology will not be safe for the user and the patients. Robotic surgical techniques can help enable surgery with complex tasks more than other surgery techniques and achieve better efficacy for specific operations [34]. However, the surgery robot lacks tangible and force feedback [35, 36], causing the surgery doctors to have less control over patient safety and [33], which increases the risk of failure. Moreover, previous research shows that safety is the main obstacle to healthcare robot use, since it is the regulation of healthcare robots that is important to human life [4]. Studies have defined safety as a barrier to healthcare robot adoption [3, 37]. In this research, this factor means that the medical staff have a feeling regarding the use of healthcare robots. It is not safe for them and their patients when the robots are in actual use. Therefore, the safety barrier has a negative effect on the behavioral intention to use healthcare robots.
-
H10b. The safety barrier (B2) has a negative result on the behavioral intention to use healthcare robots.
The long-term training barrier is the time which the user must spent on training to use the new technology is too much and that they feel it is a waste of time and that they are bored. Studies show that when medical staff must spend too much time and energy on being trained to use or adopt, they will reject the use of healthcare robots [33, 38]. BenMessaoud, Kharrazi, & MacDorman said that the lack of adoption may be the cause of the challenges with coping with new tools, with modifying new equipment kinds, and learning new operative plans. It takes too much time to attend educational programs, seminars, and training, and medical staff therefore do not accept to use the technology [3]. Moreover, previous studies show that long-term training is an obstacle to healthcare robots use [3, 38]. Therefore, it can be concluded that training staff in using a technology for too long will become a barrier to the adoption of the technology.
Long time-setting barriers involves the users’ feeling that it takes too much time to set up the technology and that the staff cannot help the patient in time. The disadvantage of a surgery robot is that the time spent on setting up the robot takes longer than a standard laparoscopic procedure [39], which becomes the factor that causes medical staff to reject healthcare robot use. The research confirms that the long-term setting of healthcare robots is a barrier to healthcare robot adoption [3]. Thus, the long time-setting is one of the barrier factors of technology acceptance.
In this research, a long time-setting and training barrier is combined with the time barrier, as they are the same type of factor. Thus, the time barrier influences the resistance to healthcare robot adoption.
-
H10c. The time barrier (B3) has a negative effect on the behavioral intention to use healthcare robots.
Change resistance (B4) means that the users do not want to change traditional healthcare to use new technology to care for patients for personal reasons. Some surgeons believe that traditional practices are adequate for the treatment of their patients. They think surgery robot use in general surgery does not improve the efficiency of the services to patients since they lack clear benefits; therefore, they do not change to use the surgery robots in their operations [39], and there are studies that support that the lack of a clear benefit causes medical staff to resist changes in treatment [40, 41]. The research on robotic colorectal surgery shows that although the robot is able to reduce work time and increase work performance, the staff may feel uneasy because the operation has changed, and they are not familiar with the new operation. In addition, medical staff have seen the benefits of traditional surgery, which are good, and so it is not necessary to change [40]. This happens because of their fear of the new technology because they think the new technology will do something, and they do not understand how it may affect healthcare performance and fear losing their work [40,41,42]. Many previous studies show that change resistance affects the perceptions, attitudes of acceptance and use of technology by users [43, 44]. Thus, change resistance influences behavioral intention.
-
H10d. Change resistance (B4) has a negative effect on the behavioral intention to use healthcare robots.
4 Research methodology
The research model was adopted from prior literature as shown in Fig.1. To ensure reliability and validity, we employed the Cronbach’s Alpha with a 1–5 Likert scale and item-objective congruence (IOC) testing techniques. Medical staff using healthcare robots in their jobs from local government hospitals in Thailand represented the target participants. They either worked in: university hospitals or tertiary care centers. A total of questionnaires 466(93.2%), were valid and used for data analysis; 19.74% were male and 80.26%, female.
This model was analyzed using confirmatory factor analysis (CFA) and structural equation modeling (SEM) to test the hypotheses and check the loading of each factor.
5 Results
5.1 Sample profile
There is a total of 466 responses that complete and accurate data for analysis. All complete data are shown in Table 1.
As shown in Table 2, females represent 80.26% of the participants, while males represent only 19.74%. Most participants were in the age group under 35 years (62.02%), and approximately two out of five of the participants had a certificate/bachelor’s degree (85.62%). Most respondents were nurses (47%), followed by physicians (33.48%), and most respondents had experience of 1–5 years (36.27%). The healthcare robot type that was used the most was the nurse robot (49.14%), while the pharmacy robot and telemedicine robot were used the least (1.93%).
5.2 Measurement model validation
The reliability analysis was performed by using Cronbach’s alpha which should be greater than 0.7 [45, 46]. All latent variable scales of Cronbach’s alpha exceeded 0.70 for each factor group and for the overall questionnaires, which have therefore “passed”.
To test the validity of this research, item-objective congruence (IOC) testing techniques were performed. The IOC concept explained that the value of all questions must be greater than 0.5 [47]. In this research, all questions obtain an IOC score greater than 0.50, which therefore “passed”, according to the IOC concept.
The correlation matrix and descriptive statistics of the main constructs are shown in Tables 2 and 3 respectively. These results indicated acceptable reliability, convergent validity, and discriminant validity. Multiple regression analyses were conducted to evaluate the effects of thirteen predictor variables on the intention to use and resistance to use.
5.3 Testing the structural model
This research model was analyzed by using confirmatory factor analysis (CFA) and structural equation modeling (SEM) to test the hypotheses and check the factors loading. The testing showed how to calculate the value of each latent factor that is created in the form of UTAUT according to each measurement list and how to indicate which items or factors are on the list of measures that the medical staff most perceived or expected; thus, all data observed for the latent variables were checked, and each measurement item loading is specified by using CFA. Then, SEM is analyzed in this model and the data obtained from the observation model are tested by recognizing whether the observation model is consistent with the theoretical model. This tests the relationship between the factors that are created in the model. The path coefficients indicate the strengths of relationships between constructs [44].
The testing results in the structural model that is presented in Fig. 2. The t-values must be significant to support the hypothesized paths. The model has to have a t-value greater than 2.58 to be considered accepted with statistical significance at the confidence level of 0.01. As a result, hypotheses 1, 2, 3, 4, 5, 7b, 10a, and 10b are supported. The hypotheses regarding H6, H8, H9, H10c, and H10d are rejected. The model value indicates an overall fit with the theory, as shown in Table 4.

Main structural model of UTAUT-based healthcare robot acceptance model (mediated model with barrier perception)
6 Discussion
In this empirical study, we analyzed medical staff acceptance and the barriers to healthcare robots using a model based on the UTAUT model. First, we analyzed the relationship of the four main structural factors of the UTAUT model. We checked the medical staff’s use behavior with BI and FC. Then, we checked the relationship between the three structural factors (PE, EE and SI) and BI. Second, we analyzed the mediators (gender, age, experience, and voluntariness of use) with the 4 basic factors of the UTAUT model to find the factors which have been affected by the 4 basic factors of the UTAUT model (PE, EE, SI, and FC). Third, the relationship between behavioral intention and barrier to use of healthcare robots was analyzed. The research results showed that the acceptance model for healthcare robot adoption by medical staff was compatible with the theoretical UTAUT model. Every core factor constructed in the model significantly affected healthcare robot acceptance. This result agrees with the findings of previous studies on healthcare technology adoption [1, 18]. This implies that the proposed model could be used effectively for predicting medical staff intentions to use similar healthcare technologies.
Our study confirmed that use behavior of medical staff is influenced by facilitating conditions and behavioral intention. There is a significant negative impact on the relationship between behavioral intention and obstacle factors. This result is consistent with the findings of previous studies on healthcare robots [20, 21]. As such, a higher barrier to users will reduce the behavioral intention of medical staff to use robot for healthcare.
Facilitating conditions is the most important factor affecting healthcare robot use behavior, following behavior intention. This illustrates the important role of facilitating conditions decision making in accepting robot for healthcare acceptance by individual medical personnel and therefore distinguishes the acceptance factors into two types: facilitating conditions and behavioral intention for successful healthcare robot implementation.
Regarding facilitating conditions, medical staff were aware of the resources needed for healthcare robot implementation. They worried about too little training on healthcare robot use, which caused them to not be confident in using the robots. Moreover, the staff were also greatly concerned about the healthcare robots being checked by a specialized staff team. The staff wanted to be confident that the healthcare robots were monitored and that they were ready for use at all times and that they must be able to be used safely. In addition, the staff wanted to have healthcare robot knowledge and abilities before healthcare robot use.
Among the adoption factors under study, the results indicated that the BI, that was, the intention of the medical staff to make the decision to accept-and-use healthcare robot technology, could be determined by PE, EE, SI, age mediators with effort expectancy (Age-EE), B1, and safety B2. BI was mainly caused by the B2, while age-EE, SI, EE, and PE were the factors that were the decreasing components. These factors had a positive effect on behavior intention, but the technical barrier (B1) reduced the intention of medical staff to use healthcare robots.
Regarding PE, medical staff need the healthcare robots to reduce healthcare process errors, speed up the time that it took to process work, increase the safety feeling in their work, help manage their time, and better manage the job characteristics. PE was an influential factor in the medical staff’s behavior intention to use healthcare robots. The staff also knew that healthcare robots were good healthcare equipment and that the robots must help deliver healthcare services as normal. However, in practice, medical staff did not use the healthcare robots to increase their service to full capacity because the healthcare robots are too small. Some of them still used conventional treatment tools that result in an inability to improve the staff performance, as expected. Some healthcare robot features were not able to meet the staff needs.
EE was determined by the simplicity of using the healthcare robots’ hardware and program; the robot’s ability to help make the staff’s work more easy and convenient; the ease of learning of how to use the healthcare robot system; the healthcare robots’ results being clear and easy to understand; the healthcare robot being capable of being modified immediately; and by how easy it was to solve the problems with learning healthcare robots. Effort expectancy was an influential factor on the medical staff’s behavior intention to healthcare robots using. However, in practice, medical staff focused only on the simplicity of using the hardware and software. Medical staff would not dare repair a healthcare robot; they will only solve basic problems, so that the robots can be used only in times of emergency because healthcare robots had a very high cost.
Regarding age mediators with effort expectancy (Age-EE), the Age-EE was completely supported and agreed with the EE. Age-EE was the factor of personal age that indicates the age range of the medical staff who used healthcare robots. If the medical staff was under the age of 35 and the healthcare robots were easy to use, then the staff were more likely to want to use the robots than staff who were over 35 years old. The younger staff were curious, and they were more driven than older staff. When the medical staff were over 35 years old, the motivation to work automatically decreases, and they were too tired to learn new things even if the robots are easy to use.
SI was measured by the pressures of expectations from colleagues and supervisors, the hospital management team, the specialized staff team and the staff themselves. Colleagues and supervisors had little influence, while the most powerful persons or medical staff were hospital management teams, specialized staff teams and the staff themselves. Every decision of the hospital management team had a significant impact on medical staff. The opinion of the medical staff themselves had a great influence on the decision to use the robots. However, the expectation of their colleagues and supervisors were only suggestions for them: when it was time to decide what to do, the medical staff will look at their readiness and executive orders. The expectations at the hospitals were increasing, because the management was hiring a team of specialized staff to look after the healthcare robots and the medical staff users. It was expected that medical personnel should use the medical robots, as the hospitals had already invested in specialized personnel. The largest department, the medical staff, normally used healthcare robots as expected by the hospital administrators, but some of the staff still use the robots only a little because the equipment is not enough to meet their needs (surgery department).
Regarding inhibitors, our study confirmed that the medical staff’s barrier to use was caused by technical barriers and safety barriers that were significantly related to healthcare robot acceptance perception barriers of the medical staff at Thai government hospitals. This study showed the perils of avoiding the determination of user resistance. Lessons from previous experience had shown that the staff avoid regretful consequences. If such situations occur, this will make the medical staff more likely to resist the use of healthcare robots.
B1 is defined as the difference between needed technological characteristics and the infrastructure support. The barrier can be viewed as a lack of the medical staff members’ technical training and support from the hospital, as the complexity of the system, and as a lack of clarity in the data obtained or limitations of the system. The barrier had a direct negative effect on the medical staff’s behavior intention, meaning that less training and support results in higher resistance to using healthcare robots, which necessitates training on healthcare robot use [48]. Moreover, if the healthcare robot system was complex and lacks clarity of data, the staff will not want to use the robots [36]. Therefore, medical staff needed training and support from the hospital. In addition, healthcare robots must respond to the medical staff’s work.
B2 was caused by a lack of basic knowledge and sufficient expertise to use healthcare robots, which makes medical staff anxious, because they did not have direct contact with patients, and they were anxious about their own safety and that of their patients. This was caused by personal fear. According to theory, the safety barrier had a negative result on medical staff and behavioral intention, but in practice, the safety barrier had a positive result on behavioral intention. The medical staff thought that they must learn how to use the healthcare robots and to gain basic knowledge and expertise, because the hospital had begun to change from conventional treatments to using more healthcare robots. This happens when the staff were concerned about safety when using the healthcare robots but when they still need to use the robots, and so they must learn how to use them. This results in the staff being able to use the healthcare robots. After that, when the medical staff saw that the medical robots were able to reduce errors and respond to their work, they wanted to use the healthcare robots. Therefore, this barrier had become a driving force for medical staff using healthcare robots.
B3 and B4 did not have a direct negative effect on medical staff’s behavior intention. The medical staff did not think that the training, preparation of the device and learning of the system was a waste of time for them. If these activities can help them understand healthcare robot use, the medical staff will engage in them. In addition, when healthcare robots were also convenient to use and provide significantly better results than traditional methods, the staff switched to using these robots without hesitation.
Previous research had suggested solutions to these barriers as follows: first, hospital management need to assess the level of knowledge and skills of medical personnel to plan training for the use of robots for healthcare [49]. They had to choose the right training package according to the needs of the staff [36]. Finally, there was a need for user evaluation after training and use to identify additional training needs [50]. These processes would reduce the safety barrier and eventually eliminate it, since everyone who finished these training sessions to obtain work in any healthcare organization will have basic knowledge about using healthcare robots [51]. Second, healthcare robots should be designed to be more user friendly [3]. Third, the robot designers needed to design the usage conditions of the healthcare robots to be similar to the original conditions [52, 53]. Fourth, the functionality of the healthcare robots must respond to the medical staff work and be better than the original work [3].
6.1 Implications for research
This study has many definitions and research result. The main support is the inspection of technology adoption and barrier theories to determine how users evaluate overall change in relation to new technology This research uses the theory of acceptance and obstacle and uses the literature of technology acceptance (UTAUT) to combine and add relevant concepts from Pagani’s barrier theory. Therefore, we offer in-depth information about the theories for researchers that may help encourage medical staff to use new healthcare technology (healthcare robots). Second, in the previous research, enablers and inhibitors have not yet been clearly defined or measured. Therefore, we prove the acceptance and barrier technology theories and find the acceptance and resistance factors by clearly defining concepts and measuring individual-level enablers and inhibitors. Our research confirms that facilitating conditions and behavioral intention are important factors of use behavior in healthcare robots. In addition, only age-mediated via-EE mediators have a positive effect on medical staff’s behavioral intention. While the role of an inhibitor (only technical barrier) is significant, the driving forces would have a negative effect, i.e., the resistance of medical staff in using robots for healthcare. However, the safety barrier is the opposite, creating more acceptance of use at the Thai government hospitals. The results of this research could support researchers who are developing healthcare technology adoption and barrier models. The acceptance and barrier theories can provide theoretical explanations that can enhance the structure and relationships in addition to the previous models. Because this study is a novel research field in Thailand, this study has shown how the UTAUT theory can be used to explain the acceptance of medical staff and resistance to change related to new healthcare technology. Therefore, this tool is a reliable and accurate tool. Making it more effective for researchers to assess user behavior; it is possible to fine-tune and compare differences in terms of study results.
6.2 Implications for practice
The study results suggest management recommendations on how to increase user acceptance and lower user barriers to healthcare robot implementation. First, the facilitating conditions higher level and behavioral intention encourage medical staff to have a more positive attitude toward the system. The healthcare robots should be designed to reduce healthcare process errors and work fast and an automatic safety function should be developed. Medical staff should be able to use the healthcare robots with ease both in terms of the hardware and the program, as well as be able to repair basic systems easily. The robots should provide clear and easy-to-understand results for users. Moreover, healthcare robot acceptance is mainly influenced by the facilitating conditions, which help achieve the goal of persuading medical personnel to use healthcare robots. The hospital managers should pay attention to the following: (a) the medical staff should have more training, which if the medical staff members are under 35 years of age, will lead to better performance; (b) the hospital managers must hire specialized staff teams to check that the healthcare robots are ready for use at all times; (c) managers should provide sufficient resources for medical personnel using robot for healthcare; and (d) the hospital management should emphasize service by using healthcare robots, so that the medical staff will be able to use the robots comfortably. Second, management should be aware of the significant effect of inhibitors on user resistance. Management design can reduce the cause of technological barriers by (a) making sure the robot design is easy to use; (b) explaining the use and details of the robots so that they are easily understood by an expert; (c) designing the robots so that they are suitable for each department’s work; and, (d) making sure that the results are accurate enough. Third, management should aim to increase the perceived value of change in order to reduce user resistance. To increase the perceived value of the benefits of robot for health should be emphasized from the perspective of medical staff and healthcare professionals. The benefits of adoption therefore require clear communication between medical staff and hospital management before negotiating with the supplier company and implementing the healthcare robots. Furthermore, most healthcare technology designs tend to focus on system considerations or new functions instead of considering the users, such as the impact that the system will have on the user’s healthcare behavior and on potential user resistance. A better understanding of users’ resistance to healthcare technology may lead to improved design of robots.
7 Limitations and conclusion
The limitations of this research should be accepted. The first is the selection of factors based on previous literature and observing the behavior of our medical staff in our study. There may be other enablers of healthcare robot usage that were not included in this study and may be subject to future research. Second, this research studied only the robot use behavior for health of medical staff in Thai government hospitals. The findings and implications of this study cannot be summarized to other groups, such as patients or private hospitals.
This research contributes to help fill the research gap and initiate research by examining the causal relationships between the behavioral intention to use and the resistance to healthcare robots in Thai government hospitals. The novelty of this research lies in the combination of the critical factors (e.g., enablers and inhibitors) that influence the behavioral intention to use a technology and barriers to using healthcare robots. Our study confirmed that FC are the most important positive factors affecting healthcare robot use behavior, followed by BI. BI, that is, the intention of the medical staff to make the decision to accept-and-use healthcare robot technology, can be determined by PE, EE, SI, Age-EE, B1, B2. This study supported our initial expectation that barrier factors have a significant negative impact on behavioral intention. We hope that this study will stimulate future interest in the acceptance of healthcare robot and resistance phenomenon, guide healthcare robot design and encourages researchers to examine more in-depth the unexplored research areas.
References
Alaiad A, Zhou L. An Empirical Study of Home Healthcare Robots Adoption using UTAUT Model. Transaction of International Conference on Health Information Technology Enhancement (ICHITE). 2013;185–198
Natarajan N, Aparna S, Kumar J. Robot aided remote medical assistance system using LabVIEW. Int J Comput Appl. 2012;38:6–10. https://doi.org/10.5120/4578-6753.
BenMessaoud C, Kharrazi H, MacDorman KF. Facilitators and barriers to adopting robotic-assisted surgery: contextualizing the unified theory of acceptance and use of technology. PLoS One. 2011;6:e16395. https://doi.org/10.1371/journal.pone.0016395.
Wongpiromsarn T, Damrongchai N, Vatananan-Thcscnvitz R. Technology development roadmap for medical robotics in Thailand. 2016 PortlandInternational Conference on Management of Engineering and Technology (PICMET). 2016;3240–3248. https://doi.org/10.1109/PICMET.2016.7806571
Phichitchaisopa N, Naenna T. Factors affecting the adoption of healthcare information technology. EXCLI J. 2013;12:413–36.
Alaiad A, Zhou L. The determinants of home healthcare robots adoption: an empirical investigation. Int J Med Inform. 2014;83:825–40. https://doi.org/10.1016/j.ijmedinf.2014.07.003.
King C-H, Chen TL, Fan Z, Glass JD, Kemp CC. Dusty: an assistive mobile manipulator that retrieves dropped objects for people with motor impairments. Disabil Rehab Assistive Technol. 2012;7:168–79. https://doi.org/10.3109/17483107.2011.615374.
Norzaidi M, Mohamed I, Chong S-C, Kamarudin R. A study of intranet usage and resistance in Malaysia’s port industry. J Comput Inf Syst. 2008;49:37–47. https://doi.org/10.1080/08874417.2008.11645304.
Hsieh P-J. An empirical investigation of patients’ acceptance and resistance toward the health cloud: the dual factor perspective. Comput Hum Behav. 2016;63:959–69. https://doi.org/10.1016/j.chb.2016.06.029.
Cenfetelli RT. Inhibitors and enablers as dual factor concepts in technology usage. Journal of the Association for Information Systems. 2004;5(11):16
Kim H-W, Kankanhalli A. Investigating user resistance to information systems implementation: a status quo Bias perspective. MIS Q. 2009;33:567–82. https://doi.org/10.2307/20650309.
Punchaipetch T. The Application of Lean and Six Sigma in Hospital Pharmacy Department: A Case Study in Thailand. PhD diss., Mahidol University. 2014.
Damrongchai N. T. C. of E. for L. S. Thailand Center of Excellence for Life Sciences, Medical Robotics Technology Development Roadmap for the Center for Advanced Medical Robotics, Thailand Center of Excellence for Life Sciences 2015-2019, 1st ed (Bangkok: กระทรวงวิทยาศาสตร์และเทคโนโลยี, 2015). 2019.
Laowattana D, Charoenseang S, Saimek S, Songschon S, Maneewarn T, Suphamani A, Chuamgchod S. saranukromthai’s book 36. (2002). http://saranukromthai.or.th/sub/book/book.php?book=36&page=main. Accessed 27 Sept 2019.
Aarts J, Gorman P. IT in health care: sociotechnical approaches" to err is system". Int J Med Inform. 2007;76:1–3.
Bartos CE, Butler BS, Crowley RS. Ranked levels of influence model: selecting influence techniques to minimize IT resistance. J Biomed Inform. 2011;44:497–504. https://doi.org/10.1016/j.jbi.2010.02.007.
Bhattacherjee A, Hikmet N. Physicians’ resistance toward healthcare information technology: a theoretical model and empirical test. Eur J Inf Syst. 2007;16:725–37. https://doi.org/10.1057/palgrave.ejis.3000717.
Hsieh P-J. Healthcare professionals’ use of health clouds: integrating technology acceptance and status quo bias perspectives. Int J Med Inform. 2015;84:512–23. https://doi.org/10.1016/j.ijmedinf.2015.03.004.
Joshi K. Understanding user resistance and acceptance during the implementation of an order management system: a case study using the equity implementation model. J Inform Technol Case Appl Res. 2005;7:6–20. https://doi.org/10.1080/15228053.2005.10856057.
Fleming KC, Evans JM, Chutka DS. Caregiver and clinician shortages in an aging nation. Mayo Clin Proc. 2003;78:1026–40. https://doi.org/10.4065/78.8.1026.
Compeau DR, Higgins CA. Computer self-efficacy: development of a measure and initial test. MIS Q. 1995;19:189–211. https://doi.org/10.2307/249688.
Bouwman H, Carlsson C, Molina-Castillo FJ, Walden P. Barriers and drivers in the adoption of current and future mobile services in Finland. Telematics Inform. 2007;24:145–60. https://doi.org/10.1016/j.tele.2006.08.001.
Pagani M. Determinants of adoption of third generation mobile multimedia services. J Interact Mark. 2004;18:46–59. https://doi.org/10.1002/dir.20011.
AlAwadhi S, Morris A. The Use of the UTAUT Model in the Adoption of E-government Services in Kuwait. Proceedings of the 41st annual Hawaii international conference on system sciences (HICSS), Ieee. 2008; 219–219
Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. MIS Q. 2003;27:425–78. https://doi.org/10.2307/30036540.
Kijsanayotin B, Pannarunothai S, Speedie SM. Factors influencing health information technology adoption in Thailand’s community health centers: applying the UTAUT model. Int J Med Inform. 2009;78:404–16. https://doi.org/10.1016/j.ijmedinf.2008.12.005.
Treister NW. Physician acceptance of new medical information systems: The Field of Dreams.(Surfing the Information Technology Wave). Physician Executive. 1998;24:20–5.
Taylor S, Todd PA. Understanding information technology usage: a test of competing models. Inf Syst Res. 1995;6:144–76.
Zhou T. Examining location-based services usage from the perspectives of unified theory of acceptance and use of technology and privacy risk. J Electron Commer Res. 2012;13:135.
Escobar-Rodríguez T, Carvajal-Trujillo E. Online purchasing tickets for low cost carriers: an application of the unified theory of acceptance and use of technology (UTAUT) model. Tour Manag. 2014;43:70–88. https://doi.org/10.1016/j.tourman.2014.01.017.
Gomez G. Emerging technology in surgery: informatics, electronics, robotics. Townsend CM, Beauchamp RD, Evers BM. Sabiston Textbook of Surgery. 18th ed. Philadelphia: Saunders Elsevier; 2007.
Alaboudi A, Atkins A, Sharp B, Alzahrani M, Balkhair A, Sunbul T. Perceptions and attitudes of clinical staff towards telemedicine acceptance in Saudi Arabia. 2016 IEEE/ACS 13th International Conference of Computer Systems and Applications (AICCSA). 2016;1–8. https://doi.org/10.1109/AICCSA.2016.7945714
Finan MA, Rocconi RP. Overcoming technical challenges with robotic surgery in gynecologic oncology. Surg Endosc. 2010;24:1256–60.
Lanfranco AR, Castellanos AE, Desai JP, Meyers WC. Robotic surgery: a current perspective. Ann Surg. 2004;239:14–21. https://doi.org/10.1097/01.sla.0000103020.19595.7d.
El-Sofany H, Al-Tourki T, Al-Howimel H, Al-Sadoon A. E-government in Saudi Arabia: barriers, Challenges and its Role of Development. Int J Comput Appl. 2012;48:16–22. https://doi.org/10.5120/7344-0119.
Hasanain RA, Cooper H. Solutions to overcome technical and social barriers to electronic health records implementation in Saudi public and private hospitals. J Health Inform Develop Countries. 2014;8:46–63.
Xue Y, Liang H, Mbarika V, Hauser R, Schwager P. Understanding Healthcare Professionals’ Resistance of Telemedicine: an Empirical Study in Ethiopia. PACIS. 2014:225.
Talamini MA, Hanly EJ. Technology in the operating suite. JAMA. 2005;293:863–6.
Marescaux J, Rubino F. Robotic surgery: potentials, barriers, and limitations. Eur Surg. 2005;37:279–83. https://doi.org/10.1007/s10353-005-0182-z.
Panteleimonitis S, Parvaiz A. Robotic colorectal surgery. Surg-Oxford Int Edition. 2017;35:151–6. https://doi.org/10.1016/j.mpsur.2016.12.004.
Brewster L, Mountain G, Wessels B, Kelly C, Hawley M. Factors affecting front line staff acceptance of telehealth technologies: a mixed-method systematic review. J Adv Nurs. 2014;70:21–33. https://doi.org/10.1111/jan.12196.
Hair JF Jr, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. 7th ed. Upper Saddle River: Pearson; 2010.
Kline P. Handbook of psychological testing. Routledge, 2013
Chin WW. The partial least squares approach to structural equation modeling. Mod Methods Bus Res. 1998;295:295–336.
Alateyah S, Crowder RM, Wills GB. Identified factors affecting the citizen’s intention to adopt e-government in Saudi Arabia. Int J Social Human Sci Eng. 2013;7:244–52.
Almutairi B. A strategic roadmap for achieving the potential benefits of electronic health record system in the state of Kuwait." PhD diss., UCL (University College London). 2011
Rovinelli RJ, Hambleton RK. On the use of content specialists in the assessment of criterion-referenced test item validity. Tijdschrift voor Onderwijsres. 1977;2:49–60.
Yee S. Transoral robotic surgery. AORN J. 2017;105:73–84.
Ginsberg D. Successful preparation and implementation of an electronic health records system. Best Practices: A guide for improving the efficiency and quality of your practice. 2007.
Abdulai T. Implementing Ehr in a developing country: potential challenges and benefits (a case study from Ghana). Clinical Medicine. 2009.
Abdulai T. Implementing EHR in a developing country: potential challenges and benefits. Master’s thesis, Universitetet i Tromsø. 2009
Alateyah S, Crowder RM, Wills GB. Identified factors affecting the citizen’s intention to adopt e-government in Saudi Arabia. International Journal of Social, Human Science and Engineering. 2013;7:244–252.
Almutairi B. A strategic roadmap for achieving the potential benefits of electronic health record system in the state of Kuwait. 2011.
Acknowledgments
The author(s) gratefully thank Associate Professor Damrong Attaprechakul, Language Institute (Thammasat University) for article review, Siriraj Hospital (Mahidol University) for data collection place.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article examines human acceptance factors and behavior with the permission of Mahidol University - Central Institutional Review Board (MU-CIRB) and Institutional Review Board, Faculty of Medicine Siriraj Hospital (SIRB) Before collecting the data.
Statements of informal consent
Informed consent was obtained from. All individual participants included in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vichitkraivin, P., Naenna, T. Factors of healthcare robot adoption by medical staff in Thai government hospitals. Health Technol. 11, 139–151 (2021). https://doi.org/10.1007/s12553-020-00489-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12553-020-00489-4