
Abstract
Computerised medical diagnosing systems are very important to all healthcare professionals, especially clinicians who help in clinical decision-making in complex situations. The acceptance of automated or computerised medical diagnosing system for Tuberculosis (TB) among clinicians is very essential for its effective implementation and usage. This paper proposes a framework that aims to examine factors that influence clinician’s acceptance and use of computerised TB detection system. An extended Unified Theory of Acceptance and Use of Technology (UTAUT) model is adopted in the healthcare context of a developing country for this purpose. The proposed framework is expected to help researchers and clinicians to assess the uptake of modern technology by health care professionals and the tool could be used in other healthcare contexts also. This paper also reviewed previous research adopting UTAUT model, for identifying the constructs promoting the adoption of technology acceptance in health care context.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Health information technology (HIT) is the use of information technology in the field of healthcare, which helps to improve treatment quality, care, productivity, efficiency, patient safety, and thereby, clinical outcome. It can be defined as “the application of information processing that deals with the storage, retrieval, sharing and use of healthcare data for decision making and communication” [1]. Use of HIT has many potential advantages such as early detection of contagious diseases, improved patient care, and better follow up of chronic diseases [2]. HIT has improved the quality of treatment, reduced clinical errors [3] and helps the medical professionals to handle chaotic situations. Computers and Personal Digital Assistance (PDAs) are among the common HIT tools used by healthcare professionals [4]. Health care professionals are considered the end users of HIT, which they should be using to improve patient outcomes. Nowadays, these devices are also used by patients and non-clinical healthcare providers such as social workers or health workers.
The success of any technology in health care area greatly depends upon the end-users adoption behaviour [5]. Evaluating and quantifying end users acceptance and use of new technology is an actively growing research area coming under information systems. Health care professionals’ belief towards HIT helps to promote the usage of that technology in their daily clinical life for decision making. So the adoption nature (usage or non-usage) of any IT-based clinical diagnosing system is determined in the health professional’s clinical or practicing environment itself. Many studies [5–12] in the field of HIT are related to technology adoption (purchase and use IT), which is done by medical professionals, researchers, hospitals and clinics, for medical management and decision making. In all the above mentioned studies, the authors focused on the factors or key determinants that influence the technology acceptance and use. To accomplish this, social psychology or social approach has been used to explain the determinants or factors of end users’ usage or behavioural intention.
The overall aim of any hospital organization is to provide quality treatments [8] wherein computerized medical diagnosing (CMD) systems or automated diagnosing systems, can play an important role. This paper focused on studying the factors that influence the clinician’s acceptance and use (adoption) of CMD system for Tuberculosis (TB) detection. In this study, we focused on modified Unified Theory of Acceptance and Use of Technology (UTAUT) model which is used to examine the clinician’s adoption of CMD system for TB detection from sputum smear images.
This paper is structured as follows: Section 2 provides an overview of the computerized medical diagnosing system for detecting TB bacilli using conventional microscope; Section 3 discusses the framework (UTAUT) used in this study. We also review previous health care adoption studies based on UTAUT model and the potential limitations of technology acceptance model in health care context. The proposed research framework and research hypotheses are explained in Section 4, and in Section 5, different hypotheses and their paths are discussed. Discussions and future work are drawn in Section 6.
2 Computerized medical diagnosing system for tuberculosis
Medical diagnosis and treatment is a cognitive process [13] for all medical professionals especially clinicians. In general, the expertise level of each medical professional depends on his/her knowledge and experience, and sometimes (in complex situations) they may fail to provide effective treatment to the needed ones in certain instances [13]. According to the analysis in the Journal of the American Medical Association (in 2003), at least one in 12 patients died due to incorrect diagnosis [14]. So to handle the above situations, nowadays clinicians forced to use computerized systems for diagnosing and treatments. Also there is a shortage of well qualified medical professionals, especially in some rural and remote areas [13]. Automated or computerised diagnostic systems became a handy tool in such situations [13]. Nowadays, CMD systems are widely used in many hospitals for reducing the cost of treatments [15] and for providing better or positive impact in the healthcare sector. But these enhancements will exist only if physicians have utilized the key functions in CMD systems and use them judiciously in their clinical practice. Thus, the utilization of computers for clinical work has the potential to bring in better patient outcome.
The two major types of HIT systems used in healthcare domain are Electronic Medical Report (EMR) systems and CMD Systems [15]. This study focused on CMD system for TB. TB is caused by the bacteria, Mycobacterium tuberculosis and is the second leading cause of deaths in the world, besides HIV/AIDS. According to the World Health Organization (WHO 2015) report, in 2014, an estimated 1.5 million people died of TB [16]. The burden of TB is concentrated in developing countries like India and Africa, where almost 40 % of individuals who fall ill with the disease, go undiagnosed [17]. India shares 23 % of the global burden and ranks first among the top ten TB incidence countries (based on World TB Report 2015) [16]. In India, an estimated 2 million new cases occurs annually, that comes to approximately one fifth of the global incidence [18]. We focus our study in Indian developing country perspective in this context.
In many developing countries, the prevailing tool for the identification of different bacterial and parasitic infections (malaria, tuberculosis etc.), is microscopy. Most of the developing countries follow sputum smear microscopy and its enhancement (high quality smear microscopy) helps to screen and diagnosis TB more accurately [17]. “The manual screening for detecting TB bacilli has the following drawbacks: the method has a huge sensitivity variation and is labor-intensive, the procedure needs mental concentration and results to eye strain, and takes time between 40 minutes and 3 hours depending on patient’s level of infection for the screening”[19]. A clinician is anticipated to spend at least 15 min per slide to analyse at least 100 oil immersion fields in each slide, and can therefore only analyse very few TB slides in a day [20]. It is alarming to note that the failure rates of the present day screening techniques are in the range of 33–50 %, even by conservative estimates [21].
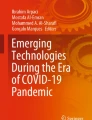
To address this issue, many researchers developed semi [21] and fully [22–24] automatic (computerised) TB detection methods using conventional and fluorescent microscope (sample one shown in Fig. 1). Among them, conventional microscope is the most popular and is widely used tool in low and middle-income countries due to its ease of maintenance and low cost [13]. This study focused on TB detection using conventional microscope only. “With the help of automated microscopy, computers (machine) can screen more number of fields and can identify many TB cases easily in the beginning stage itself” [21]. Recently introduced computerised techniques are successful in screening the images of TB bacilli, thereby saving the time, improving the patient outcome and quality of diagnosis; thus increasing efficiency in health care [13]. In addition, the ease of use and low eye strain are the added advantages of this automated system (AS). Thus, CMD system for TB, along with its unique features, needs to be studied to delineate the factors influencing the use of automated system for TB in healthcare.

a Computerized TB detection system, b Image of TB bacilli
3 Literature review
This section discusses the limitations of the commonly used framework, Technology Acceptance Model (TAM) in the evaluation of CMD system for TB, and the relevance of UTAUT model as observed by various researchers in the context of health care. We also reviewed previous research studies adopting UTAUT model in health care context.
3.1 Unified Theory of Acceptance and Use of Technology (UTAUT)
For explaining the technological adoption, many researchers already implemented several important theoretical models. In general, technological adoption can be studied in two ways: “some researchers focused on the relationship between technological adoption and the variables affecting it, like UTAUT and TAM; others took the “process” approach and study its in-depth process” [25]. UTAUT, a technology acceptance model, was developed by Venkatesh et al. in 2003, with four key determinants (Performance Expectancy, Effort Expectancy, Social Influence, and Facilitating Condition) of intension and usage [26]. The authors tested this model empirically and suggested that “it performed better than the other eight models and it effectively integrated the entire key constructs present in the previous models such as Theory of Reasoned Action (TRA), TAM, Theory of Planned Behaviour (TPB), Model of PC Utilization (MPCU), a model combining TAM and the TPB, the Motivational Model (MM), the social cognitive theory, and the Innovation Diffusion Theory (IDT)” [26]. UTAUT was mainly developed for the purpose of banking, accounting, entertainment, telecommunication services, etc. [5] and it is also applied on large data sets in the real world for empirical study. In 2012, an extended version of UTAUT, called UTAUT2, was developed by Venkatesh et al. [27] by adding three new constructs such as hedonic motivation, habit, and price value to the actual UTAUT model. The authors developed the new version of UTAUT in the consumer context, so additional factors of UTAUT2 are not relevant to this study.
Earlier in 1989, Davis [28] developed TAM model, which gained much attention and was widely used by many researchers for the acceptance and use of IT. However, lot of disadvantages or challenges of TAM in health care context was reported recently. Very recently, Holden et al. [1] mentioned that “TAM theory only estimates a significant part of the use or acceptance of HIT; but that theory needs some modifications and additions of new variables and relationships for its benefits”. They also suggested that TAM has no influence on the health care context and it is somewhat a good standard for industries; also, some of its measures and key aspects may not appear important to healthcare researchers [1]. The same authors also had an opinion about the poor fit of TAM in telemedicine IT among physicians and also suggested that there is a need for further enhancement. In 2011, Melas et al. [9] mentioned in their article that only few systematic studies have been carried out on TAM in health care and also discussed several inconsistencies and disadvantages of TAM in healthcare context. Many other short comings about TAM are also discussed by Hung et al. [8] in 2012, such as “TAM is not suitable for analysing health care professional’s technology acceptance, especially clinicians because their characteristics or behaviour are different from other typical technological users”. Based on the above limitations of TAM, this study adopted a modified UTAUT model.
UTAUT model can be used to forecast and interpret behaviour across many domains such as healthcare, medical, education, business, IT, etc. Most of the studies based on this model have taken place in developed countries health care context [5]. Besides, “this model showed up to 70% of the variance in usage intention, while other competing models showed only 30–40% of IT acceptance and this exhibits the importance of adoption”[12]. “UTAUT model always tries to describe the usage intention to use a system or technology and the subsequent usage behaviour” [15]. If the technology is more user-friendly and it improves the job performance, then the end-users have a tendency to accept and use that technology in their daily life. In 1989, Davis [28] suggested that the end users unwillingness towards the new technology always block the performance gains. Under this circumstance this study proposes a research framework that utilizes a modified UTAUT model, to study the determinants that predict the usage intention of CMD system for TB detection. In this study, we consider an additional factor “technological trust”, which was not present in the original UTAUT model. Many researchers [12, 29] proved in their studies that trust has a significant influence on usage intention, for the use of clinical decision support system among medical professionals. Shibl et al. [12] and Tung et al. [29] considered trust as a separate factor in their study.
3.2 Technology acceptance in health care
At present, there is only very limited literature in health care context that focused on the adoption of computerised medical diagnosing system, which indicates a knowledge gap or research gap [6, 7]. The acceptance of a pharmacokinetics-based clinical decision support system among physicians in Taiwan was examined based on UTAUT model by Chang et al. [7] in 2007; in the same year itself, Information and Communication Technology (ICT) acceptance and its use was examined by Schaper et al. [11] and they conducted their study by using the same model, among occupational therapists in Australia. They also suggested about the better explanation capability and quality of the UTAUT model in health care. Recently in 2009, the adoption of HIT in Thailand Community Health Centers (CHC) was examined by Kijsanayotin et al. [5], using a modified UTAUT model. In that study, authors concluded that people who worked in Thailand CHCs showed a very good acceptance rate of HIT. In 2009 itself, usage of IT in hospitals was examined by Aggelidis et al. [6] based on a modified UTAUT model.
Physician’s acceptance of the Medline system was studied by Hung et al. [8] in 2012, for evaluating the practice of evidence-based medicine. Due to the limitations of TAM, they used a decomposed TPB model for the study purpose and they also mentioned that the decomposed TPB model has low explanation capability than the UTAUT model. In 2012, physicians perceived professional autonomy, involvement level, and belief in adopting clinical decision support systems were examined by Sambasivan et al. [15] based on the UTAUT model. Very recently, decision support system’s acceptance among general practitioners was examined by Shibl et al. [12] in 2013, by using an extended UTAUT model. In 2015, the acceptance of telemedicine for the management of diabetic patients was examined by Rho et al. [10] and they selected the UTAUT model due to the fact that many previous studies used the same model in health care context. Also, this model was later extended to mobile-health (m-health) adoption by Dwivedi et al. [30] in 2015, for studying the citizens’ attitude towards m-health. All the above cases showed the use of UTAUT model in health care context. Motivated by the aforementioned studies, we also adopt a modified UTAUT model for examining the factors influencing the adoption of CMD system for TB. Table 1 shows the details of previous research studies with differing constructs, their relationships (major findings), and the study contexts.
From the above table (Table 1), we can observe that most of the studies related to HIT adoption have taken place in developed countries like Taiwan, Australia, Greece, USA, Canada, and only very few studies in developing countries like Malaysia, Thailand, and Bangladesh.
4 The proposed research framework
Proposed research model is also an application of HIT and this study wants to apply that model in the health care context of TB, which is shown in Fig. 2. The detailed explanation of each constructs is given below.

The Proposed Research Model
4.1 Performance expectancy
Performance Expectancy (PE) is one of the major desirable constructs of all technology acceptance models that have been proposed by Venkatesh et al. in 2003 and is defined as “the degree to which user or stake holder believes that the use of particular technology would help to improve or enhance the performance of his/her job”[26]. PE not only improves job performance, but also helps to increase efficiency, reduce cost and enhance quality and care [1]. It shows high resemblance to Perceived Usefulness (PU) of TAM [26] and it directly influences usage intension. It has been used as one of the basic construct in many surveys related to UTAUT, such as adoption of health IT [5], adoption of decision support system in healthcare [12] etc. Other researcher’s findings indicated that technology’s PE or usefulness is very important for physicians’ acceptance and use of IT-based systems [12]. The positive significance of PE/usefulness and Usage Intention (UI) in health care IT was strongly mentioned by Holden et al. [1] in 2010 and Kijsanayotin et al. [5] in 2009. Also, many studies [7, 10, 28, 30–33] already showed its significance on intention to use IT. In this paper, we redefine PE as the degree to which clinicians believe that using this CMD system for TB will help to enhance the performance of their clinical work.
One of the main features that we want to include in PE is professional development, which is referred as whether the clinicians believed that the use of CMD system for TB would help them to enhance their professional skills [12]. In 2004, the similar concept is discussed by Lin et al. [34] in their article that the technology can be utilized for “working” benefits rather than personal intentions. This encouraged our study, because CMD system for TB that we want to study is used by clinicians for clinical purpose and it is work related, thus supported this feature.
Another feature that we want to include in the PE is time saver/time effective. Less time-consumption is the major factor that influences the clinician’s intention to use new IT technology [9]. An “easy to use system” is considered as a time saver system and it has additional features such as operational simplicity, user friendliness, fast access, effective recording, information retrieval etc. With the help of computerised system for TB, physicians can handle more number of clinical cases daily. In 1997, Brailer et al. [35] mentioned that the use of computer assisted interpretation of ECG system reduced the time needed for the clinician by an average of 28 % than the conventional interpretation method. Also, in the context of TB, the same advantage is discussed by many researchers [21–23, 36] and they suggested that the computerised system for TB aims to minimize the dependency of the clinicians, speeding up the clinical process and increase the accuracy of TB detection. Based on the above assumptions, we suggest the following hypothesis:
-
H1:
Performance Expectancy has a significant positive relationship with the Usage Intention of CMD system for TB.
4.2 Effort expectancy
Like PE, Effort Expectancy (EE) is also a prominent basic variable and is used in many health care related UTAUT models such as adoption of health IT [5], adoption decision support system in healthcare [12] etc. It is defined as “the degree of ease associated in using the new technology” [26]. It shows high resemblance to Perceived Ease of Use (PEOU) of TAM [26]. It was suggested by Venkatesh et al. [26] in 2003 and they took this construct from previous eight models. Generally, systems which can be operated more easily will have high preference than the one that is more difficult to operate. A system with difficulty in usage will lead to non-usage [37]. PEOU was found to be more important to some clinicians, especially those who have very little knowledge of computer. This is also discussed in other research articles [38, 39]. If learning and using of CMD system for TB is relatively easy for clinicians, the usage rate of the system is expected to grow accordingly. Also, many studies [5, 7, 10, 28, 30, 31] already showed that EE has sufficiently great influence on Usage Intention. We redefine this concept as the degree of ease associated with the use of CMD system for TB among clinicians. This extensive and positive relation of EE on the usage intention in different contexts of health care helps us to think that the same mechanics will also work here. As we expected, it is also an enabling factor for the use of CMD system for TB. Thus, we suggest the following hypothesis:
-
H2:
Effort Expectancy has a significant positive relationship with Usage Intention of CMD system for TB.
4.3 Social influence
Social Influence (SI) was proposed by Venkatesh et al. in 2003 and is defined as “the degree to which an individual perceives that it is important for others to believe that one should use the new technology” [26]. Based on SI, each one changed his or her usage intention. Venkatesh et al. [26] took this construct from other previous eight models. In this study, we altered this concept as the degree to which each clinician perceives that important others believe that he or she should use the CMD system for TB in their daily clinical life. Many researchers [5, 7, 10, 30] already showed that SI has a significant influence on usage intention. Peer influence is very crucial here. For example if the technology is endorsed by professional bodies of health professionals like Indian Medical Association and Nurses organizations, then it will have better intake. Likewise, official endorsement by the top leadership in the health sector will force both government and private establishments to adopt newer technology. Public demand could be yet another influencing factor that might prompt health professionals to adopt technology. Based on the above statements, this study can also expect a positive significant relationship between SI and usage intention of CMD system for TB. Thus, we suggest the following hypothesis:
-
H3:
Social Influence has a significant positive relationship with Usage Intention of CMD system for TB.
4.4 Technological trust
Clinician’s trust in HIT should influence the adoption behaviour of that particular technology in health care. To establish HIT infrastructure, a high degree of trust is required; and the lack of trust potentially leads to misuse of the technology. Thus, trust plays a significant role in the adoption of health care technology. The higher level of trust towards the system indicates better utilization of the system [12] for healthcare productivity. Three types of trust are discussed by Montague [40] in 2010; those are interpersonal trust (trust between persons), social trust (individuals trust with an institution or system), and technological trust (a person’s trust with technology). In this study, we focused on Technological Trust (TT) and is defined as the clinician’s level of belief on a particular technology, including its process and policies. It is a very important concept because clinicians today greatly rely on computerised medical diagnosing systems for their clinical work to handle complex situations.
If clinicians did not trust in the CMD system for TB, then they will not use it. If clinicians trusted in the computerised system for TB, then they would become more comfortable and skilful in using it. For studying the factors influencing the acceptance of decision support system among general practitioners (GP), Shibl et al. [12] in 2013, utilized the construct “trust in the knowledge base”. They took this construct after conducting a qualitative interview with the GP and suggested that it was not suitable with any of the constructs in UTAUT model, so they considered it as a separate factor. They found that this construct was an enabler of decision support system usage. Similar trust concept is also used by Tung et al. [29] in 2008 for studying the adoption of the electronic logistics information system among nurses; and they also suggested that trust has higher positive effect on usage intention. Over all, a trusted system is likely to be used more than an un-trusted system [12]. Increased end user (clinicians) trust can promote the usage intention. We expect that TT is also an important influencing factor in this context of TB because literature [17, 21–23] says most of the TB automation methods produced high accurate results than manual detection method. Based on the above facts, we also expect a positive significant relationship between technological trust and usage intention of automated system. Thus, we suggest the following hypothesis:
-
H4:
Technological trust has a significant positive relationship with Usage Intention of CMD system for TB.
4.5 Usage intention (UI) of CMD system for TB
One of the most important factors that influence the actual use of automated system for TB is usage intention (UI). This is generally considered as acceptance or end-user satisfaction [1]. UI predicts the actual use of the technology and is a measurable construct (dependent variable) which is influenced by other independent variables like PE, EE, SI etc. In previous technological acceptance studies [7, 26, 32, 33] UI is well explained and documented. It also showed that it is a powerful predictor of actual system usage either in other domains or in health care sector [6]. Based on the above theoretical assumption, we suggest the following hypothesis:
-
H5:
Usage Intension of automated system has a positive significant relationship with actual use of CMD system for TB.
4.6 Computer skill
Health IT is a very diverse area and it is changing rapidly; so some skills and knowledge are needed for the proper implementation and the successful working of HIT projects. These knowledge and skills may differ from job to job and it mainly includes the knowledge about socio-technical aspects of IT. Today, many IT based systems are used in various sectors like health care, to serve medical professionals in their day-to-day clinical work for managing patients and hospitals. In 2012, Sambasivan et al. [15] suggested that clinician’s adoption of new automated technology greatly depends on their computer knowledge. Computer Skill (CS) can be defined as “individual’s confidence in using the computer” [41] and its applications. Higher computer skill means that one can operate the computer systems and software’s without any support or assistance [41]. For examining the adoption of HIT in Thailand CHC, Kijsanayotin et al. [5] (2009), utilized the “IT knowledge” and they checked only the basic knowledge of computer and Internet. Also, for studying the adoption of clinical information systems among the hospital staffs, Melas et al. [9] (2011) took “computer skill” of clinician as a key construct. Thus, computer knowledge or IT knowledge generally plays an important role in the interaction between clinicians and automated decision making system. Nowadays health care professional’s poor knowledge of computer may affect their professional development also. Many researchers [5, 9, 41] found that computer skill was found to make a considerable effect on the actual usage of the system. Thus we expect that, clinician’s belief in computer knowledge will surely help to develop skills in using the CMD system for TB. As a result, we propose the following hypotheses:
-
H6:
Computer Skill has a positive significant relationship with actual use of CMD system for TB.
4.7 Actual use (AU) Of CMD system for TB
Actual use is the function of usage intention and computer skills (from Fig. 2). Clinicians can use the CMD system for TB for the following purposes such as patient record use, data transmission, and automatic analysis and decision making.
4.7.1 Patient record &data transmission
Nowadays, the transmission of data and images through Internet are attracting the attention of many medical practitioners. In modern healthcare, computer and internet may be used to enhance the communication between different healthcare professionals and thus improving the co-ordination within the healthcare systems. Healthcare information system’s success rate is always determined by the communication between the healthcare professionals [42]. Several other researchers also supported the salient characteristics of healthcare work such as transfer of information, communication among health workers and coordination of activities [43]. Similar attempt was done by Kijsanayotin et al. [5] in 2009, for examining the HIT adoption; they utilized the constructs such as “care and report use” and “communication use”. In these constructs, authors focused more on recording of patient information, information searching and collaboration with colleagues. If medical images were send from one rural health centre to another through internet [17], then they can share their knowledge and experience with other staffs; thus they can provide better or quality treatments. Thus, connecting computer technology to clinical work has a considerable power to enhance the quality of diagnostic services [13] in low and middle income countries, where poor settings of clinical resources are available, especially in rural and remote areas.
A mobile-phone based image transfer system was developed by Tuijn et al. [44] in 2011, which captures the images from the microscope and sends these images to other experts through the internet for better clinical opinion. A similar approach was done by Tapley et al. [17] in 2013 for detecting TB automatically. They proposed a digital fluorescence microscope called CellScope and suggested that the digital images (TB image) taken by CellScope can be send to distant experts for evaluation, and this idea has been successfully demonstrated by some other researchers also. By utilizing these type of automated systems, clinicians can took the images of malaria, TB bacilli etc. and can share with other laboratory staff through the Internet for expert opinion [45]. Recording of TB image can also play a vital role in education and research purpose. In education context, it can make high impact among school and college students (health professionals). i.e., all students in a class room can visually see the image of TB bacilli through the computer screen at the same time rather than looking each one through the microscope.
This study utilized the connectivity of microscopy with computer and internet for TB diagnosis, for achieving better outcome in healthcare sector. Thus the overall advantages of these key constructs are (a) better diagnosis (quality treatment) (b) suitability for education and research (c) strengthening of communication among different health care players.
4.7.2 Automatic image analysis and decision making
In modern healthcare, medical imaging plays a fundamental role in decision making (i.e., disease detection and prediction) and the wide usage of the automated systems has resulted in automatic image analysis and detection. Since 1950s, many different automated diagnosing techniques have been attempted in many fields of medicine for decision making [46]. Change in the healthcare sector by the use of advance medical diagnostic systems (computerised systems) will bring more positive results in clinical decision making and treatment [47]. Automatic image analysis for TB may facilitate on-the-spot or immediate diagnosis, enhance accuracy by helping to examine larger number of fields than the manual evaluation and improve the specificity through rigid and reliable criteria for TB bacilli identification [17]. The same authors also suggested that the automated system for TB is well suitable to integrate computationally and can perform intensive image analysis and decision making [17].
A fully automatic TB detection system for identifying TB bacteria from ZN-stained Sputum Smear images for conventional microscope was developed by Zhai et al. in 2010 [24]. These systems captured and stored the sputum smear images in the computer and performed automatic image analysis and accurate decision making (TB or not). Many other researchers [21–23, 48] also proposed similar semi and fully automatic detection methods for TB and they also suggested that these methods could assist clinicians in clinical diagnosis and decision making.
5 Research hypothesis and paths
In order to find out the factors influencing the clinician’s acceptance of automated TB diagnosing system, hypotheses are developed based on the above research framework. The research frame work is composed of constructs such as performance expectancy, effort expectancy, social influence, technological trust, computer skill, usage intention, and actual use. We developed six hypotheses based on the above research framework. We expect that the following hypotheses (shown in Table 2) and paths are suitable for the future empirical study.
6 Discussions and future work
Computerized medical diagnosis is an area coming under medical informatics and it has become one of the rapidly growing research areas in medical imaging and clinical diagnosis. The success of any technology related projects in health care greatly depends upon the end-users acceptance and use behaviour [5]. This study tried to find the factors that influence the clinician’s acceptance and use of CMD system for TB by using a modified UTAUT model, and this model mainly focused on the prediction of two theoretical constructs—the usage intention and actual use of computerised TB detection system. The proposed research framework showed that usage intention is a function of PE (enhance job performance), EE (free of effort), SI, and TT. Also, actual use is a function of usage intention and computer skill. In 2010, Ayatollahi et al. [49] suggested that the identification of these factors can help the researchers in healthcare to develop a strategy for implementing similar systems in future.
The adoption of CMD system for TB enhances the clinical support towards TB detection. It has several advantages than the conventional method as discussed earlier (in Section 2). In developing countries health care context, there is only limited number of studies based on UTAUT model for studying the adoption of technology [5]. The authors in [5] showed that the modified UTAUT model can provide better understanding of technology adoption and its applicability in developing countries health care settings. Based on the above observation, we can also conclude that our proposed research framework is a modified form of UTAUT and is greatly applicable for the studies of developing countries health care context for the adoption of automated TB detection system among the clinicians. In 2015, McNerney et al. [50] suggested that there is a need for new technology and its assessment programs in health care sector for controlling and eradication of TB disease; that indicates a research gap. The adoption of CMD system for TB detection from sputum smear images has not been studied yet in the developing countries health care context. Thus, the perception about these systems and its adoption greatly influence the persons in the health care domain, and this will accelerate the development and the process of implementation. This research aims to add more contribution or knowledge to the health care area of technology acceptance (through quantitative study) by providing support from the UTAUT model and refining it to automated systems acceptance, especially in the context of clinicians. We constructed the proposed framework after discussing the relevance and impact of the topic with many clinicians and subject experts. This study is also useful for researchers and medical professionals who are currently working with HIT implementation projects and health information systems. In the future, this model can be applied to other studies related to automatic detection of other various contagious diseases.
References
Holden RJ, Karsh BT. The technology acceptance model: its past and its future in health care. J Biomed Inform. 2010;43:159–72.
Huser V, Narus SP, Rocha RA. Evaluation of a flowchart-based EHR query system: a case study of Retro Guide. J Biomed Inform. 2010;43(1):41–50.
Bates DW, Cohen M, Leape LL, Overhage JM, Shabot MM, Sheridan T. Reducing the frequency of errors in medicine using information technology. J Am Med Inform Assoc. 2001;8:299–308.
Yi MY, Jackson JD, Park JS, Probst JC. Understanding information technology acceptance by individual professionals: toward an integrative view. Information and Management. 2006;43:350–63.
Kijsanayotin B, Pannarunothai S, Speedie SM. Factors influencing health information technology adoption in Thailand’s community health centers: applying the UTAUT model. Int J Med Inform. 2009;78:404–16.
Aggelidis VP, Chatzoglou PD. Using a modified technology acceptance model in hospitals. Int J Med Inform. 2009;78:115–26.
Chang IC, Hwang HG, Hung WF, Li YC. Physicians’ acceptance of pharmacokinetics-based clinical decision support systems. Expert Syst Appl. 2007;33(2):296–303.
Hung S, Kub Y, Chien J. Understanding physicians’ acceptance of the Medline system for practicing evidence-based medicine: a decomposed TPB model. Int J Med Inform. 2012;81:130–42.
Melas CD, Zampetakis LA, Dimopoulou A, Moustakis V. Modeling the acceptance of clinical information systems among hospital medical staff: an extended TAM model. J Biomed Inform. 2011;44:553–64.
Rho MJ, Kim HS, Chung K, Choi IY. Factors influencing the acceptance of telemedicine for diabetes management. Clust Comput. 2015;18:321–31.
Schaper LK, Pervan GP 2007. ICT and OTs: a model of information and communication technology acceptance and utilisation by occupational therapists. Int J Med Inform. 7 6 S: S212–S221.
Shibl R, Lawley M, Debuse J. Factors influencing decision support system acceptance. Decis Support Syst. 2013;54:953–61.
Panicker RO, Soman B, Saini G, Rajan J. A review of automatic methods based on image processing techniques for tuberculosis detection from microscopic sputum smear images. J Med Syst. 2016;40:17. doi:10.1007/s10916-015-0388-y.
Shojania KG, Burton EC, McDonald KMMM, Goldman L. Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA. 2003;289(21):2849–56.
Sambasivan M, Esmaeilzadeh P, Kumar N, Nezakati H. Intention to adopt clinical decision support systems in a developing country: effect of Physician’s perceived professional autonomy, involvement and belief: a cross-sectional study. BMC Med Inform Dec Making. 2012;12:142.
WHO. Global tuberculosis report 2015. . Available from: http://www.who.int/tb/publications/global report/en/.
Tapley A, Switz N, Reber C, Davis JL, Miller C, Matovu JB, Worodria W, Huang L, Fletcher DA, Cattamanchi A. Mobile digital fluorescence microscopy for diagnosis of tuberculosis. J Clin Microbiol. 2013;51(6):1774–8.
Kanabus A. Information about tuberculosis Available from: www.tbfacts.org Accessed 1985.
Costa MGF, Filho CCF, Junior KA, Levy PC, Xavier CM, Fujimoto LB. A sputum smear microscopy image database for automatic bacilli detection in conventional microscopy. ConfProc IEEE Eng Med Biol Soc. 2014;2841–4.
Osibote OA, Dendere R, Krishnan S, Douglas TS. Automated focusing in bright-field microscopy for tuberculosis detection. J Microsc. 2010;240(2):155–63.
Veropoulos K, Campbell C, Learmonth G, Knight B, Simpson J. The automated identification of tubercle bacilli using image processing and neural computing techniques. Proceedings of the 8th International Conference on Artificial Neural Networks; Sweden. 1998;2:797-802.
Forero MG, Sroubek F, Cristóbal G 2004. Identification of tuberculosis bacteria based on shape and color. Real-Time Imaging 10: 252–262.
Forero-Vargas M, Sroubek F, Alvarez-Borrego J, Malpica N, Cristóbal G, Alcalá L, Alcala L, Desco M, and Cohen L 2002. Segmentation, autofocusing and signature extraction of tuberculosis sputum images. SPIE Proc Photonic Devices and Algorithms for Computing IV 4788; 171–182.
Zhai Y, Liu Y, Zhou D, Liu S. Automatic identification of mycobacterium tuberculosis from ZN-stained sputum smear: algorithm and system design. IEEE International Conference on Robotics and Biomimetics; China. 2010;41-46.
Im I, Hong S, Kang MS. An international comparison of technology adoption: testing the UTAUT model. Inf Manag. 2011;48:1–8.
Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. MIS Q. 2003;27(3):425–78.
Venkatesh V, Thong JYL, Xu X. Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Q. 2012;36(1):157–78.
Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13:319–39.
Tung F, Chang S, Chou C. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry. Int J Med Inform. 2008;77:324–35.
Dwivedi YK, Shareef MA, Simintiras AC, Lal B, Weerakkody V. A generalised adoption model for services: A cross-country comparison of mobile health (m-health). Gov Inf Q. 2015;33(1):174–87.
Jeng DJ, Tzeng G. Social influence on the use of clinical decision support systems: revisiting the unified theory of acceptance and use of technology by the fuzzy DEMATEL technique. Comput Ind Eng. 2012;62:819–28.
Taylor S, Todd P. Understanding information technology usage: a test of competing models. ISR. 1995;6(2):144–76.
Venkatesh V, Davis F. A theoretical extension of the technology acceptance model: four longitudinal field studies. Manag Sci. 2000;46(2):186–204.
Lin J, Chan H, Jin Y. Instant messaging acceptance and use among college students. The 7th Pacific Asia Conference on Information Systems; Australia; 2004; 181–194.4.
Brailer DJ, Kroch E, Pauly MV. The impact of computer-assisted test interpretation on physician decision making, the case of electrocardiograms. J Med Dec Making. 1997;82–6.
Jager KD, Fickling S, Krishnan S, Jabbari M, Learmonth GW, Douglas TS. Automated Fluorescence Microscope for Tuberculosis Detection Journal of Medical Devices. 2014;8.
Pennington R, Kelton S, DeVries D. The effects of qualitative overload on technology acceptance. J Inf Syst. 2006;20(2):25–36.
Hu PJ, Chau P, Sheng O, Tam K. Examining the technology acceptance model using physician acceptance of telemedicine technology. J Manag Inf Syst. 1999;16(2):91–112.
Igbaria M, Zinatelli N, Cragg P, Cavaye ALM. Personal computing acceptance factors in small firms: a structural equation model. MIS Q. 1997;21(3):279–305.
Montague E. Validation of a trust in medical technology instrument. Appl Ergon. 2010;41:812–21.
Compeau DR, Higgins CA. Computer self-efficacy: development of a measure and initial test. MIS Q. 1995;189–211.
Hayrinen K, Saranto K, Nykanen P. Definition, structure, content, use and impacts of electronic health records: are view of the research literature. Int J Med Inform. 2008;77:291–304.
Viitanen J, Hyppönen H, Lääveri T, Vänskä J, Reponene J, Winblad I. National questionnaire study on clinical ICT systems proofs: Physicians suffer from poor usability. Int J Med Inform. 2011;80:708–25.
Tuijn CJ, Hoefman BJ, Beijma HV, Oskam L, Chevrollier N. Data and image transfer using mobile phones to strengthen microscopy-based diagnostic services in low and middle income country laboratories. PLoS ONE Mobile Phones to Support Microscopy Diagnosis. 2011;6(12).
Frean J. Microscopic images transmitted by mobile cameraphone. Trans R Soc Trop Med Hyg. 2007;101:1053.
Doi K. Computer-aided diagnosis in medical imaging: historical review, current status and future potential. Comput Med Imaging Graph. 2007;31:198–211.
Pagliari C, Sloan D, Gregor P, Sullivan F, Detmer D, Kahan JP, Oortwijn W, Gillivray SM. What is eHealth: a scoping exercise to map the field. J Med Internet Res. 2005;7(1):e9.
Chayadevi ML, Raju GT. Automated colour segmentation of tuberculosis bacteria thru region growing: a novel approach. Bangalore: Fifth International Conference on Applications of Digital Information and Web Technologies (ICADIWT); 2014. p. 154–9.
Ayatollahi H, Bath PA, Goodacre S. Factors influencing the use of IT in the emergency department: a qualitative study. Health Inform J. 2010;16(3):189.
McNerney R, Cunningham J. New tuberculosis diagnostics and rollout. Int J Infect Dis. 2015;32:81–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Panicker, R.O., Soman, B., Gangadharan, K.V. et al. An adoption model describing clinician’s acceptance of automated diagnostic system for tuberculosis. Health Technol. 6, 247–257 (2016). https://doi.org/10.1007/s12553-016-0136-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12553-016-0136-4