
Abstract
Background
Medication adherence is important for secondary stroke prevention. However, suboptimal adherence to medication among patients after stroke or transient ischemic attack is reportedly 30.9%. We assessed medication adherence of Korean stroke survivors within 1 year of acute ischemic stroke and identified factors that influence adherence.
Methods
We consecutively enrolled ischemic stroke survivors who visited the Department of Neurology of a university hospital from March 9 to June 15, 2016. Data were collected by face-to-face interviews using a structured questionnaire which assessed general characteristics, clinical characteristics, medication beliefs, social support, and depression. Medication adherence was measured using the 8-item Morisky Medication Adherence Scale. Multiple logistic regression was used to identify factors independently associated with medication adherence.
Results
Of the total 250 participants, 183 (73%) were in the optimal adherence group. Age (p = 0.035), smoking (p = 0.020), number of prescribed medicines (p = 0.037), frequency of daily doses (p = 0.040), and beliefs about medication (p < 0.001) were associated with medication adherence. Optimal medication adherence was associated with being a non-smoker (OR, 3.19; 95% CI, 1.29–7.87; p = 0.012), more prescribed medicines (OR, 1.27; 95% CI, 1.05–1.54; p = 0.014), less frequency of daily doses (OR, 0.37; 95% CI, 0.18–0.79; p = 0.010), and stronger beliefs about medication (OR, 1.09; 95% CI, 1.03–1.15; p = 0.004).
Conclusion
To improve medication adherence of stroke survivors, post-stroke care should focus on bolstering patients’ belief in the necessity of medication and encouraging lifestyle modifications, such as quitting smoking, as well as prescribing medicine with simple regimens.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stroke is the third leading cause of morality in Korea, following cancer and heart disease [1]. The burden of stroke amounted to approximately $3.8 billion in 2010 [2]. The number of stroke survivor is persistently increasing, while the incidence of hemorrhagic strokes continues to decline [3]. This may be due to lifestyle changes, which have exacerbated the impact of risk factors for stroke, such as hypertension, diabetes mellitus, and dyslipidemia [4,5,6]. Stroke is related to a high risk of mortality and recurrence, which aggravates the risk of disability or death. The risk of recurrence within 5 years of the first stroke event is nearly 30%, while that within 1 year of the first stroke event is 13%: 15 times higher than the risk of a first stroke in the general population [7]. Therefore, secondary prevention of stroke recurrence is an important public health concern for both survivors and society.
For the secondary prevention of ischemic stroke, it is important to regularly administer anti-thrombotic agents, as well as manage correctable risks factors, including atrial fibrillation, hypertension, diabetes mellitus, and dyslipidemia; anti-thrombotic agents, such as aspirin or warfarin, are particularly useful in significantly decreasing the risk of stroke recurrence in patients with ischemic stroke [8]. Discontinuation of anti-thrombotic agents within 1 year of stroke increases the risk of recurrence by as much as 1.57 times [9]. In patients with atrial fibrillation, the failure to maintain an international normalized ratio (INR) of 2.0 or greater of warfarin significantly increases the incidence of stroke [10]. In addition, the 1- to 2-week discontinuation of anti-platelets required for the performance of invasive procedures or examinations significantly increases the risk of stroke; moreover, such temporary interruptions often become permanent [11, 12]. Therefore, continuous and regular administration of anti-thrombotic agents is important for successful secondary prevention among stroke survivors.
Hypertension control as well as anti-platelet therapy has contributed significantly to the decreased recurrence of stroke in Korea over the past 50 years [13]. This observation agrees with that of another meta-analysis: hypertension treatment reduces the risk of recurrence of stroke as well as that of stroke-related disability [14]. Blood glucose control is another important factor in the secondary prevention of stroke. The administration of pioglitazone to insulin-resistant diabetic patients with a history of stroke led to a reduced risk of stroke and myocardial infarction relative to those who received only a placebo [15]. Furthermore, the discontinuation of statin, which lowers LDL, improves endothelial function, and maintains plaque stability, reportedly increased the risk of mortality and disability after stroke [16, 17]. Thus, the regular use of medication for controlling comorbidities of stroke is also important when determining the recurrence and prognosis of stroke. However, the actual adherence of stroke survivors to medication is generally poor for a variety of reasons that may be caused by not only the patients themselves but also healthcare providers or healthcare systems. It reportedly decreases to 65.9% by 1 year following the stroke event [18], and a systematic review of adherence after stroke or transient ischemic attack (TIA) reported a pooled, prevalent non-adherence rate of 30.9% [19]. A study on medication adherence at a local public health center in Korea found that only 41.2% of stroke survivors continued to take medication for the secondary prevention of stroke [20].
The ABC (Ascertaining Barriers to Compliance) team provided consensus taxonomy and terminology in medication adherence and also provided definitions that could serve the needs of both clinical research and medical practice [21]. Adherence is defined as “the process by which patients take their medications as prescribed.” Persistence is defined as “the length of time between initiation and the last dose, which immediately precedes discontinuation.” Assessments of adherence to medication should, therefore, measure not only whether the appropriate dose is regularly taken but also the persistence of the prescription. Therefore, the persistence of medication is important for secondary prevention among stroke survivors, but medication adherence taking the dose as prescribed regularly is of more clinical importance. However, previous studies have primarily focused on the persistence of stroke treatment rather than medication adherence [22, 23]. Also, a meta-analysis study related to the adherence of the medication in stroke survivors also included studies measuring persistence, confirming that the two terms are often used interchangeably without explicit distinction in definition [19]. In addition, in Korea, many patients favor Korean Oriental medical therapy over the regimen recommended by the hospital. In particular, after the acute stage of stroke, patients tend to prefer Oriental medicine hospitals for early rehabilitation or sometimes opt for receiving the two forms of treatment concurrently [24]. Though the preference of Korean Oriental medical therapies may also affect adherence to stroke medication, this has remained unexplored.
The purpose of this study was to investigate medication adherence among Korean stroke survivors within 1 year of their acute ischemic stroke and to identify the factors influencing their medication adherence.
Methods
Participants
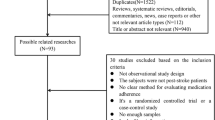
Stroke survivors who visited the outpatient stroke clinic of a tertiary university hospital from March to June 2016 were assessed for eligibility according to the following inclusion criteria: a first diagnosis of cerebral infarction or transient ischemic attack (TIA), a stroke event having occurred between 3 months and 1 year prior, an ability to communicate and complete a questionnaire, and the provision of agreement to participate in the study. TIA is predictive of future stroke and has a pathophysiologic mechanism and treatment plan similar to those of ischemic stroke [25]; we have therefore included TIA in this study. Stroke survivors were excluded if they had significant aphasia/dysarthria (National Institutes of Health Stroke Scale (NIHSS) best language and dysarthria scores of > 2), major physical disability (modified Rankin scale (mRS) of > 4), and/or cognitive impairment or preexisting dementia (Korean Mini-Mental State Examination score of < 24). Stroke survivors who visited our outpatient clinic for regular follow-up while being hospitalized at another clinical facility, such as a rehabilitation or Oriental medicine hospital, were also excluded because the patient’s medication would be managed by the nurse. The required sample size was calculated with a multiple logistic regression analysis performed using the 3.19 version of the G*Power program [26]; an odds ratio of 1.5, a power of 0.85, and at a two-tailed α of < 0.05 were used as inputs. The G*Power results indicated that a sample size of 236 individuals was required. After accounting for a predicted incomplete response rate of 5%, the total required sample size was 257.
Measures
To improve the patient’s ability to follow a medication regimen, potential barriers to adherence were considered. We adapted a conceptual model of barriers to medication adherence by Osterberg and Blaschke [27], according to which various factors resulting from the interaction among patients, health providers, and the healthcare system affect medication adherence. Thus, to identify factors associated with medication adherence in this study, we investigated factors related to the interaction of patient-health providers and patient-healthcare system and those previously identified to relate to patients [19, 28] (see Fig. 1). Factors related to the interaction of health provider and healthcare system, such as provider’s knowledge of drug costs or the provider’s job satisfaction, were excluded because this study was conducted in one center and they could not be considered as corresponding to intervention strategies addressing the improvement of patients’ medication adherence.

Conceptual model of medication adherence in this study
Medication adherence, beliefs about medicine, social support, depression, and activities of daily living were investigated using validated tools, as shown below.
Medication Adherence
Adherence to medication was measured using the 8-item Morisky Medication Adherence Questionnaire (MMAS-8ⓒ) [29]. We used the Korean version of the MMAS-8 provided by the original author. MMAS-8 is a self-report measure of adherence that features good measurement properties. Each of the 8 items assesses specific medication-taking behaviors, such as forgetting or ceasing to take medication when a patient perceives his or her medical condition to be under control. Sample items include “Do you sometimes forget to take your medicine?” and “Have you ever cut back or stopped taking your medicine without telling your doctor because you felt worse when you took it?” According to the MMAS-8, adherence was categorized as high adherence (a score of 8), medium adherence (a score of 6 to < 8), and low adherence (a score of < 6). The MMAS-8 has been shown to be reliable (alpha reliability = 0.83) for the assessment of medication adherence in outpatients with hypertension and was significantly associated with blood pressure control when a score of 6 was used as a delimiting value [29], showing that the MMAS-8 features enough validity to screen a patient’s medication adherence. To explore the factors associated with medication adherence, we divided the patients into two groups in a manner similar to that employed in previous studies [30, 31]: participants who scored less than 6 points on the MMAS-8 were allocated to the suboptimal adherence group, and participants who scored 6 to 8 points were the optimal adherence group. The Cronbach’s α for the scale in the current sample was 0.64.
Beliefs About Medication
Belief about medications was assessed using a Korean version [32] of the Beliefs about Medicines Questionnaire (BMQ), which was developed by Horne et al. [33]. The BMQ is a self-report scale which assesses the beliefs of chronic patients in their prescribed medication. The questionnaire is divided into two scales: The first scale assesses specific necessity and concerns about the belief of patients in their prescribed medication, and the second scale measures patients’ opinions about general harm and overuse of medicines. The present study only used the former: the BMQ-specific scale, which has two subscales (necessity and concern) with a total of 10 questions. The BMQ-specific necessity subscale includes five items, including “My health, at present, depends on my medicine” and “My life would be impossible without my medicine.” The BMQ-specific concerns subscale assesses fears of potential adverse outcomes or side effects of the lifelong consumption of medication, such as stroke medication. Examples of the five items include “My medicines are a mystery to me” and “I sometimes worry about the long-term effects of my medicine.” Patients indicated their agreement to such statements using a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = uncertain, 4 = agree, and 5 = strongly agree); thus, scores for either BMQ subscale ranged from 5 to 25. Higher BMQ-specific necessity scores indicate stronger perceptions of a personal need for the medication to maintain health, both now and in the future, and higher BMQ-specific concerns scores indicate stronger concerns about the potential negative effects of the medication. Beliefs about medication were calculated as the difference between the BMQ-specific necessity and the BMQ-specific concern scores: A positive differential score indicates stronger beliefs in the necessity of medication than concerns about consequences, and on the contrary, a negative score indicates stronger concerns. Therefore, higher scores indicated stronger beliefs about medication. The Cronbach’s α was 0.77 for the BMQ-specific necessity scale in the current sample and 0.71 for the BMQ-specific concern scale.
Social Support
Social support was assessed using a Korean version [34] of the ENRICHED Social Support Inventory (ESSI) [35]. The 7-item ESSI was developed to measure functional social support, especially emotional support. The ESSI assesses the level of support received during the past month and marital status. Structural, instrumental, and emotional support are assessed by rating items on a 5-point scale (from 1 = none of the time to 5 = all of the time). Item 7 (living with a spouse) is scored as 4 (yes) or 2 (no). The total EESI score ranges from 8 to 34, where higher scores indicate higher levels of social support. The Cronbach’s α for the ESSI in the current sample was 0.87.
Depression
Depressive symptoms were assessed using the Korean version of the Center for Epidemiologic Studies Depression scale (KCES-D) [36]. The CES-D is a commonly used 20-item self-rating scale designed to measure depressive symptomatology in both clinical and non-clinical settings. The CES-D contains 20 items that are rated on a 4-point Likert scale (from 0 to 3); the total score ranges from 0 to 60. Higher scores indicate more severe depressive symptoms. The Cronbach’s α for CES-D in the current sample was 0.87.
Activities of Daily Living
Activities of daily living were assessed using the Korean version of the Modified Barthel Index (K-MBI) [37]. The K-MBI indicates the degree of independence of a patient from any assistance. It covers the following 10 domains of functioning/activities: bowel and bladder control, help with grooming, toilet use, feeding, chair/bed transfers, walking, dressing, climbing stairs, and bathing. The K-MBI has three different rating scales as follows: a score range of 0–5 (bathing and personal hygiene), a score range of 0–10 (feeding, dressing, toilet use, bladder control, bowel control, and stair climbing), and a score range of 0–15 (chair/bed transfers and ambulation). Total K-MBI scores range from 0 to 100, where a higher score indicates more independence in performing basic activities of daily living. The Cronbach’s α for the K-BMI in the current sample was 0.80.
Data Collection
A preliminary survey was performed to confirm the adequacy of and time required for the survey questions and estimates the distribution of the adherence group. For this, we selected 30 stroke survivors from the outpatient stroke clinic who fulfilled the aforementioned inclusion criteria and excluded them from the subsequent survey. The survey took about 20 min to complete, and the survey questionnaires were confirmed to be appropriate.
After the preliminary survey, we delivered the survey using structured questionnaires from March 1, 2016. First, we reviewed electronic medical records to screen for eligibility. The purpose and procedure of the study were explained to eligible participants. The survey lasted for about 20–25 min. Patient’s medical history data, including “Trial of ORG 10172 in Acute Stroke Treatment” (TOAST), NIHSS and mRS scores at discharge, stroke risk factors, numbers of prescribed medicines, and frequency of daily doses, were collected from the patients’ electronic medical records. The study was approved by the Ethics Committee at the Chonnam National University Hospital. All participants consented to participate through a consent form at the beginning of the study.
Statistical Analyses
To measure the reliability of instruments used in this study, the Cronbach’s alpha coefficients were used. All data are expressed as numbers and percentages, means and standard deviations, or medians and ranges. To compare various characteristics between adherence and non-adherence group, the Chi-square test, Fisher’s exact test, linear-by-linear association, independent t-test, or Mann-Whitney U test was used. To test the normality of continuous variables, we used the standardized skewness and regarded as a significant skewness when the absolute values of z score exceeding 3.29 [38]. Multiple logistic regression analysis was used to identify independent factors related to medication adherence. Variables were selected for entry into the model based on the results of univariate analyses (p < 0.05). All statistical analyses were performed using SPSS statistical software (version 21.0; SPSS Inc., Chicago, IL, USA), and statistical significance was defined as a two-tailed P < 0.05.
Results
While a total of 257 stroke survivors were initially included, 7 were excluded because of incomplete data. Of the 250 patients; their mean (± SD) age was 62.2 (± 12.9) years, 164 (65.6%) were men, the mean (± SD) time since stroke was 7.4 (± 3.8) months, the median (range) MBI score was 100 (73–100), the median (range) MMAS-8 was 7.0 (5.8–8.0) and 183 (73.2%) and 67 (26.8%) patients were categorized into the optimal adherence and suboptimal adherence groups, respectively.
Between-Group Comparison of Various Characteristics
Stroke survivors in the optimal adherence group were significantly younger than those in the suboptimal adherence group (p = 0.035), and there were significantly fewer smokers in the optimal adherence group (p = 0.020) (see Table 1). Stroke survivors in the optimal adherence group were prescribed more medication at discharge (p = 0.037), but their prescriptions required significantly less frequency of daily doses (p = 0.040). There were no between-group differences in the duration since stroke, stroke subtype and mechanism with TOAST, stroke severity with NIHSS and mRS, or stroke risk factors. The belief about medication by necessity-concern score difference was significantly higher in the optimal adherence group than in the suboptimal groups (p < 0.001); this was because the belief scores for necessity were significantly higher in the optimal adherence group (p < 0.001), whereas belief scores for concern were higher in the suboptimal group (p = 0.076).
Approximately 50% of participants were educated about their medication, and the perceived importance of continuously taking the prescribed medication was similar in both groups. Ninety-two (36.8%) stroke survivors in this study had received some form of Korean Oriental medicine, such as acupuncture, chiropractic, physiotherapy, and/or herbal medicine, after the stroke event, but these experiences did not differ between two groups (see Table 1).
Independent Factors Influencing Medication Adherence
Age, smoking status, number of prescribed medicines at discharge, frequency of daily doses, and beliefs about medication showed significant differences between the two groups by univariate analysis, and they were inserted into the model for the multivariate analysis. The logistic regression analysis revealed that non-smoking status (OR, 3.19; 95% CI, 1.29–7.87; p = 0.012), more prescribed medicines (OR, 1.27; 95% CI, 1.05–1.54; p = 0.014), less frequency of daily doses (OR, 0.37; 95% CI, 0.18–0.79; p = 0.010), and higher beliefs about medication (OR, 1.09; 95% CI, 1.03–1.15; p = 0.004) as factors are significantly associated with optimal medication adherence (see Table 2).
Discussion
This study shows that medication adherence among Korean stroke survivors decreased to about 73% within 1 year and that smoking status, number of prescribed medicines, frequency of daily doses, and belief about medication were independent factors affecting medication adherence.
According to the “European Society for Patient Adherence, COMpliance, and Persistence Medication Adherence Reporting Guidelines (EMERGE)” [39], this study was an “implementation” phase study to see how accurately and regularly medication was being used by stroke patients. We found that an evaluation of prescriptions to stroke survivors indicated that while 100% of them were on medication, self-reports showed that only approximately 73% of the patients well adhered to their prescribed regimens. This number is lower than the 75.5–81% adherence rate reported at 3-month post-stroke [40, 41] and higher than the 41.2% adherence rate reported among chronic stroke survivors in local communities [20]. Altogether, these findings suggest that medication adherence may decrease as the time following the stroke event increases.
Of the factors related to patients, including general, disease-related, and psychosocial characteristics, only smoking status in this study was found to be an independent factor that affected medication adherence: Smokers were more likely to be suboptimal adherents, which were consistent with the results of previous studies on factors affecting medication adherence among patients with chronic disease, hypertension, and stroke [42,43,44]. These results highlight the importance of lifestyle modification for the prevention of stroke recurrence and may suggest that suboptimal adherent patients had less understanding of the importance of secondary prevention or less motivation to improve their lifestyles.
The present study observed that stroke survivors in the optimal adherence group were significantly younger than those in the suboptimal adherence group, even though this result was not replicated by multivariate analyses. This finding conflicted with those of previous studies, which found positive correlations between medication adherence and age [41, 45]. These results were probably due to various factors such as memory, cognition, irregular lifestyle, and social activities rather than age itself [46,47,48]. Therefore, when seeking strategies to improve medication adherence among stroke survivors, not only the age of the survivors but also the aforementioned related factors must be taken into account. In addition, unlike previous studies [49,50,51,52], we found that social support and depression were not significant contributors to optimal adherence. This might not indicate a difference between the two groups because about 83% of stroke survivors included in this study lived with their family or the majority of survivors had mild symptoms enough to self-administer their medication.
We investigated several factors affecting medication adherence related to the interaction between stroke survivors and health providers. We found that the belief about medication, the amounts of prescribed medication at discharge, and the frequency of drug dosing were significantly associated with medication adherence. Especially, the belief about medication was a strong predictor of adherence, which is consistent with previous findings [19, 53, 54]. Strong beliefs in the necessity of medication were more strongly associated with actual adherence than concerns regarding the side effects of long-term drug administration. These results recommend the need for healthcare providers to implement strategic interventions to change the beliefs of stroke survivors as to why drugs are necessary for secondary prevention rather than simply providing information about medication.
According to the World Health Organization, simplifying the frequency of medication administration increases adherence [28]; our results support this recommendation. On the other hand, less medication was prescribed at discharge in the suboptimal adherence group than in optimal adherence group. This finding is contrary to the prior findings that the prescription of more medication may worsen adherence [55, 56]. Our results may be accounted for by the tendency in Korea to bundle several medicines into groups to be taken at different times of day rather than providing medicines individually. Patients taking medication for chronic comorbidities having become better at medication adherence relative to their treatment-naive counterparts provide an alternative explanation [57]; regardless of the number of drugs taken, the presence of comorbidities may have helped the patients to establish the habit of taking medication continuously. Physicians could thus encourage medication adherence by simplifying frequency rather than reducing the number of prescribed medicines at discharge, especially among patients without prior experience of lengthy medication regimens.
Finally, we investigated the use of Korean Oriental therapy or medicines as a factor related to the interaction between the patient and the healthcare system, but there was no difference between the two groups. This finding may be due to the recruited stroke survivors having already decided to take the medications prescribed at the clinic and visited the outpatient clinic. While stroke survivors have received Western therapy in combination with Oriental therapy, such as herbal medication or acupuncture [24, 58, 59], this study confirmed that Oriental therapy did not affect medication adherence.
This study is subject to several limitations. First, we used a self-reported questionnaire to evaluate medication adherence; thus, reported medication adherence might have been higher than the actual adherence. Second, this study was a cross-sectional study of stroke survivors who had already visited the outpatient clinic, and the 1-year medication adherence may have been overestimated because none of the stroke survivors were followed up prospectively after the acute stroke event. Finally, this study was conducted at a single center, and patients with severe symptoms such as global aphasia or cognitive impairment were excluded from the survey. Therefore, the generalizability of our findings to Korean stroke survivors is limited. Nevertheless, the self-report measures of adherence used in this study are often highly correlated with objective measures and have been proven to be a reliable tool by showing that suboptimal adherence measured with this tool is a predictor of poor clinical outcomes in several studies. This study is meaningful in that, among Korean stroke survivors, the rate of medication adherence within 1 year of the acute stroke event was ascertained with the valid tool, and factors related to the identified adherence and based on an established conceptual model were confirmed. Of note, this study revealed that by paying careful attention to simplifying the frequency of daily doses, improving patients’ beliefs about medication, and encouraging patients to make lifestyle changes, such as quitting smoking, clinicians could help to improve medication adherence among stroke survivors.
Future, prospective, longitudinal, multicenter research is needed to better elucidate the degree of medication adherence among Korean stroke survivors and identify predictors for adherence. In addition, the development of various strategic interventions, as well as verifications of their efficacies, is warranted.
References
Korean Statistical Information Service (KOSIS). Annual report on the cause of death statistics 2016 [Internet] Daejeon: Statistics Korea; [cited 2017 Oct 25]. Available from: http://kosis.kr/eng/search/searchList.do.
Kim J, Son M. National health insurance statistical yearbook. Seoul: Health Insurance Review and Assessment Service and National Health Insurance Service; 2015.
Kim JY, Kang K, Kang J, Koo J, Kim D-H, Kim BJ, et al. Executive summary of stroke statistics in Korea 2018: a report from the epidemiology research Council of the Korean Stroke Society. J Stroke. 2019;21:42–59.
Chan JCN, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon K-H, et al. Diabetes in Asia. JAMA. 2009;301:2129.
Kokubo Y. Prevention of hypertension and cardiovascular diseases. Hypertension. 2014;63:655–60.
Choi-Kwon S, Kim JS. Lifestyle factors and risk of stroke in Seoul, South Korea. J Stroke Cerebrovasc Dis. 1998;7:414–20.
Burn J, Dennis M, Bamford J, Sandercock P, Wade D, Warlow C. Long-term risk of recurrent stroke after a first-ever stroke. Oxfordshire Community Stroke Proj Stroke. 1994;25:333–7.
Kwok CS, Shoamanesh A, Copley HC, Myint PK, Loke YK, Benavente OR. Efficacy of antiplatelet therapy in secondary prevention following lacunar stroke. Stroke. 2015;46(4):1014–23.
Shaya FT, El Khoury AC, Mullins CD, et al. Drug therapy persistence and stroke recurrence. Am J Manag Care. 2006;12(6):313–9.
Morgan CL, McEwan P, Tukiendorf A, Robinson PA, Clemens A, Plumb JM. Warfarin treatment in patients with atrial fibrillation: observing outcomes associated with varying levels of INR control. Thromb Res. 2009;124:37–41.
Wagner ML, Khoury JC, Alwell K, Rademacher E, Woo D, Flaherty ML, et al. Withdrawal of antithrombotic agents and the risk of stroke. J Stroke Cerebrovasc Dis. 2016;25(4):902–6.
Sibon I, Orgogozo J-M. Antiplatelet drug discontinuation is a risk factor for ischemic stroke. Neurology. 2004;62(7):1187–9.
Hong K-S, Yegiaian S, Lee M, Lee J, Saver JL. Declining stroke and vascular event recurrence rates in secondary prevention trials over the past 50 years and consequences for current trial design. Circulation. 2011;123:2111–9.
Katsanos AH, Filippatou A, Manios E, Deftereos S, Parissis J, Frogoudaki A, et al. Blood pressure reduction and secondary stroke prevention. Hypertension. 2017;69:171–9.
Kernan WN, Viscoli CM, Furie KL, Young LH, Inzucchi SE, Gorman M, et al. Pioglitazone after ischemic stroke or transient ischemic attack. N Engl J Med. 2016;374(14):1321–31.
Montecucco F, Quercioli A, Mirabelli-Badenier M, Luciano Viviani G, Mach F. Statins in the treatment of acute ischemic stroke. Curr Pharm. 2012;13:68–76.
Hong K-S, Lee JS. Statins in acute ischemic stroke: a systematic review. J Stroke. 2015;17:282–301.
Kobayashi A, Tamura A, Ichihara T, Minagawa T. Factors associated with changes over time in medication-taking behavior up to 12 months after initial mild cerebral infarction onset. J Med Invest. 2017;64(1.2):85–95.
Al AlShaikh S, Quinn T, Dunn W, Walters M, Dawson J. Predictive factors of non-adherence to secondary preventative medication after stroke or transient ischaemic attack: a systematic review and meta-analyses. Eur Stroke J. 2016;1(2):65–75.
Kim YT, Park KS, Bae SG. Predictors of persistence and adherence with secondary preventive medication in stroke patients. J Agric Med Community Health. 2015;40(1):9–20.
Vrijens B, De Geest S, Hughes DA, Przemyslaw K, Demonceau J, Ruppar T, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73:691–705.
Ji R, Liu G, Shen H, Wang Y, Li H, Peterson E, et al. Persistence of secondary prevention medications after acute ischemic stroke or transient ischemic attack in Chinese population: data from China National Stroke Registry. Neurol Res. 2013;35:29–36.
Bushnell CD, Olson DM, Zhao X, Pan W, Zimmer LO, Goldstein LB, et al. Secondary preventive medication persistence and adherence 1 year after stroke. Neurology. 2011;77:1182–90.
Kim LS. The experience of the stroke patients about the use of oriental medicine. J Korean Publ Health Nurs. 1997;11(1):82–92.
Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack. Stroke. 2014;45:2160–236.
Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G* power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–60.
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–97.
Sabaté E. Adherence to long-term therapies: evidence for action: World Health Organization; 2003.
Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–54.
Moon SJ, Lee W-Y, Hwang JS, Hong YP, Morisky DE. Accuracy of a screening tool for medication adherence: a systematic review and meta-analysis of the Morisky medication adherence scale-8. PLoS One. 2017;12:e0187139.
Lee GKY, Wang HHX, Liu KQL, Cheung Y, Morisky DE, Wong MCS. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky medication adherence scale. PLoS One. 2013;8:e62775.
Jung JH, Kim YH, Han DJ, Kim KS, Chu SH. Medication adherence in patients taking immunosuppressants after kidney transplantation. J Korean Soc Transplant. 2010;24:289–97.
Horne R, Weinman J. Patients' beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–67.
Suh M, Choi-Kwon S. Structural equation modeling on quality of life in stroke survivors. J Korean Acad Nurs. 2010;40(4):533–41.
Mitchell PH, Powell L, Blumenthal J, et al. A short social support measure for patients recovering from myocardial infarction: the ENRICHD social support inventory. J Cardiopulm Rehabil Prev. 2003;23(6):398–403.
Chon KK, Choi SC, Yang BC. Integrated adaptation of CES - D in Korea. Korean J Health Psychol. 2001;6(1):59–76.
Jung HY, Park BK, Shin HS, et al. Development of the Korean version of modified Barthel index (K-MBI): multi-center study for subjects with stroke. J Korean Acad Rehab Med. 2007;31(3):283–97.
Field AP. Discovering statistics using SPSS. Los Angeles: Sage publications; 2009.
De Geest S, Zullig LL, Dunbar-Jacob J, Helmy R, Hughes DA, Wilson IB, et al. ESPACOMP medication adherence reporting guideline (EMERGE). Ann Intern Med. 2018;169:30.
Hamann GF, Weimar C, Glahn J, Busse O, Diener H-C. Adherence to secondary stroke prevention strategies – results from the German stroke data Bank. Cerebrovascular diseases [internet]. S. Karger A. 2003;15:282–8.
Bushnell CD. Persistence with stroke prevention medications 3 months after hospitalization. Arch Neurol. 2010;67:1456.
Menditto E, Guerriero F, Orlando V, et al. Self-assessment of adherence to medication: a case study in Campania region community-dwelling population. J Aging Res. 2015;2015.
Cho E, Lee CY, Kim I, et al. Factors influencing medication adherence in patients with hypertension: based on the 2008 Korean National Health and nutrition examination survey. J Korean Acad Community Health Nurs. 2013;24(4):419–26.
Wang Y, Wu D, Wang Y, Ma R, Wang C, Zhao W. A survey on adherence to secondary ischemic stroke prevention. Neurol Res. 2006;28(1):16–20.
Stewart RB, Caranasos GJ. Medication Compliance in the elderly. Med Clin N Am. 1989;73:1551–63.
Smith D, Lovell J, Weller C, Kennedy B, Winbolt M, Young C, et al. A systematic review of medication non-adherence in persons with dementia or cognitive impairment. Chen K, editor. PLoS One. 2017;12:e0170651.
Chambers JA, O’Carroll RE, Hamilton B, Whittaker J, Johnston M, Sudlow C, et al. Adherence to medication in stroke survivors: a qualitative comparison of low and high adherers. Br J Health Psychol. 2010;16:592–609.
Jamison J, Graffy J, Mullis R, Mant J, Sutton S. Barriers to medication adherence for the secondary prevention of stroke: a qualitative interview study in primary care. Br J Gen Pract. 2016;66:e568–76.
Zhang H, Qian HZ, Meng SQ, Shu M, Gao YZ, Xu Y, et al. Psychological distress, social support and medication adherence in patients with ischemic stroke in the mainland of China. J Huazhong Univ Sci Technol. 2015;35(3):405–10.
Bae SG, Jeon HJ, Yang HS, Kim BK, Park KS. Medication adherence and its predictors in community elderly patients with hypertension. Korean J Health Promot. 2015;15(3):121–8.
Kim YH, Lee MK, Lee SJ, Cho MS, Hwang MS. Medication status and adherence of the elderly under home care nursing. J Korean Acad Community Health Nurs. 2011;22(3):290–301.
Grenard JL, Munjas BA, Adams JL, Suttorp M, Maglione M, McGlynn E, et al. Depression and medication adherence in the treatment of chronic diseases in the United States: a meta-analysis. J Gen Intern Med. 2011;26(10):1175–82.
Horne R, Chapman SCE, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633.
Wei L, Champman S, Li X, Li X, Li S, Chen R, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ Open. 2017;7(10):e017293.
Pasina L, Brucato AL, Falcone C, Cucchi E, Bresciani A, Sottocorno M, et al. Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs Aging. 2014;31:283–9.
Ulley J, Harrop D, Ali A, Alton S, Fowler DS. Deprescribing interventions and their impact on medication adherence in community-dwelling older adults with polypharmacy: a systematic review. BMC Geriatr. 2019;19.
An J, Nichol MB. Multiple medication adherence and its effect on clinical outcomes among patients with comorbid type 2 diabetes and hypertension. Med Care. 2013;51(10):879–87.
Han J-S, Kim Y-S, Moon Y-S, et al. Experiences of stroke patients with combined treatment of self-selected oriental and Western medicine. J Digit Converg. 2014;12(6):375–84.
Wu P, Mills E, Moher D, Seely D. Acupuncture in poststroke rehabilitation: a systematic review and meta-analysis of randomized trials. Stroke. 2010;41(4):e171–e9.
Acknowledgments
The use of the ⓒMMAS is protected by US copyright laws. Permission for use is required. A license agreement is available from Donald E. Morisky, MMAS Research LLC 14725 NE 20th St. Bellevue WA 98007 or from dmorisky@gmail.com.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kim, GG., Chae, DH., Park, MS. et al. Factors Influencing 1-Year Medication Adherence of Korean Ischemic Stroke Survivors. Int.J. Behav. Med. 27, 225–234 (2020). https://doi.org/10.1007/s12529-020-09854-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-020-09854-z