
Abstract
Intolerance of uncertainty (IU) has often been studied in the context of internalizing disorders, but no studies to our knowledge have explored the relation between IU and externalizing disorders. Given the proposed link between IU and emotion regulation, the current study sought to examine levels of IU in an externalizing clinical population with known emotion regulation difficulties—attention-deficit/hyperactivity disorder (ADHD). IU levels in this population were compared to a clinical population known to experience elevated levels of IU. Participants in present study were ninety-three children (36 anxiety disorder, 28 ADHD, 29 unaffected children) ages 7–13, who completed the Intolerance of Uncertainty Scale—Short Version (IUS). Responses on the IUS were converted to total IU, prospective IU, and inhibitory IU. A linear mixed model analysis of covariance was conducted while controlling for age, sex, and ADHD medications. A significant interaction was observed between diagnostic status and IU scale. Planned contrasts indicated that children with anxiety disorders and ADHD reported significantly higher levels of IU relative to unaffected children, and children with ADHD reported comparable levels of inhibitory IU relative to children with anxiety disorders. The current results contribute to a growing literature on the link between IU and psychopathology. IU appears to be a transdiagnostic construct present among children with internalizing and externalizing disorders, and may be broadly associated with emotion regulation deficits rather than specific disorder symptoms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Intolerance of uncertainty
Elevated levels of intolerance of uncertainty (IU) have been identified across numerous emotional disorders (Mahoney and McEvoy 2012), including internalizing disorders such as anxiety disorders (Carleton et al. 2012a), obsessive compulsive disorder (OCD; Tolin et al. 2003), posttraumatic stress disorder (PTSD; Fetzner et al. 2013), and major depressive disorder (MDD; Gentes and Ruscio 2011); however, there is a paucity of literature examining IU among externalizing disorders. Attention-deficit/hyperactivity disorder (ADHD) is one externalizing disorder frequently associated with co-occurring emotional difficulties (Rosen and Factor 2015; Rosen et al. 2015; Shaw et al. 2014). Given the increasing evidence that IU can be identified during early development and is present among a wide range of disorders, current theories of IU posit that it is a foundational and transdiagnostic mechanism through which psychopathology emerges (Carleton 2016a). Therefore, the current study sought to evaluate the proposed transdiagnostic nature of IU by extending work examining IU in internalizing populations to an externalizing population, children with ADHD.
IU is defined as the extent to which an individual is unable to tolerate an aversive response to the perceived lack of information in an environment (Carleton 2016b). IU captures an individual’s emotional reactivity to unknowns, and their capacity to endure that reactivity. IU, as it was originally defined, encompassed the cognitive and behavioral responses associated with uncertainty as well (Freeston et al. 1994). Worry, avoidance, and emotional reactivity, for instance, arise from a fear of the unknown and contribute to psychopathology in both youth and adults (Carleton 2012, 2016a). IU has been conceptualized as the filter through which negative responses emerge. Reliably identified by age seven, IU remains stable through adolescence and early adulthood (Fialko et al. 2012; Thielsch et al. 2015) suggesting that it represents a dispositional incapacity to endure uncertainty. Examination of IU in early childhood appears critical for understanding developmental trajectories of psychopathology (Read et al. 2013).
Intolerance of uncertainty as a transdiagnostic risk factor
An individual’s capacity to resolve uncertainty depends on the context in which it arises, and IU is thought to emerge among individuals who experience a higher need for certainty across situations, and become distressed by the reactions associated with uncertainty (Carleton 2016b). Though the internal processes associated with uncertainty are not yet well understood, uncertainty is known to elicit increases in affect (Bar-Anan et al. 2009) and executive functioning (Mushtaq et al. 2011). Experimental manipulations of uncertainty have found that individuals experience increased affect when uncertainty is induced, regardless of the objective amount of information present in the environment (Greco and Roger 2003; Paulus and Yu 2012). Neuroimaging studies provide evidence that the amygdala, largely associated with emotional processing, is activated by environmental uncertainty (Rosen and Donley 2006). Uncertainty may increase affect to enhance the salience of environmental cues, thus increasing the perceived amount of information available to an individual (Bar-Anan et al. 2009).
Uncertainty elicits increases in cognitive control as well. Cognitive control, or executive function, refers to the higher order, top-down processes responsible for goal-directed activity. When top-down representations of the present environment do not match the true availability of information, signaling uncertainty, cognitive control is likely employed to resolve this uncertainty by increasing information processing (Mushtaq et al. 2011). Here, too, neuroimaging studies provide evidence to suggest that brain regions involved in cognitive control or executive function tasks are activated by uncertainty, namely the dorsolateral prefrontal cortex (Huettel et al. 2005), the posterior parietal cortex (Volz et al. 2003), and the anterior cingulate cortex (Stern et al. 2010).
Taken together, current literature indicates that people may resolve uncertainty in two ways: through increases in emotion and through the cognitive control of this emotion. The inability to tolerate uncertainty, then, may arise among individuals who experience dysregulation in these two areas. Indeed, disorders associated with high levels of IU also demonstrate emotion dysregulation and difficulties with cognitive control. Individuals with anxiety disorders report greater emotional reactivity, experience more difficulty recognizing emotions, and are more likely to use maladaptive emotion regulation strategies, such as emotional avoidance (Cisler et al. 2010; Salters-Pedneault et al. 2006). The development of anxiety disorders is also associated with differences in executive functions such as attentional control and working memory capacity (Hsu et al. 2015; Mogg et al. 2015; Reinholdt-Dunne et al. 2015). Similarly, differences in emotion regulation and cognitive control have been identified among other disorders associated with high levels of IU such as MDD (Bylsma et al. 2008; Rive et al. 2013), OCD (Snyder et al. 2015; Stern et al. 2014), and PTSD (Blair et al. 2015; Ehring and Ehlers 2014).
Though not yet tested explicitly, transdiagnostic models of IU suggest that it is linked to psychopathology through the cognitive control of emotions, or emotion regulation (Einstein 2014). Emotion regulation is a multifaceted and multidimensional process (Rosen and Epstein 2010) whereby individuals control and modify the valence and intensity of their emotional states to adapt to internal and external demands (Cole et al. 2004). Studies have found that children with ADHD also experience emotion dysregulation, including more intense experiences of emotions, and more intense shifts in mood (Barkley 2015; Sobanski et al. 2010). Given the relation between IU and emotion dysregulation observed in many internalizing disorders, children with ADHD may also demonstrate similar IU impairment due to deficits in managing and coping with intense and frequent negative emotions.
Intolerance of uncertainty and ADHD
ADHD is a neurodevelopmental disorder characterized by symptoms of impulsivity, inattention, and hyperactivity (American Psychiatric Association 2013). ADHD affects an estimated 5% of school-aged children and is associated with dysfunction across domains, including home, school, and interpersonal relationships (Polanczyk et al. 2007). As with the disorders discussed above, emotion dysregulation is a core component of ADHD (Barkley 2014; Martel 2009; Rosen et al. 2015; Shaw et al. 2014). Emotion dysregulation in this population is often attributed to executive inhibitory deficits, including difficulty inhibiting emotional reactivity, and difficulty controlling this reactivity (Barkley 1997), and may contribute to impaired peer relationships and academic difficulties beyond the effects of ADHD alone (Wehmeier et al. 2010).
While children with internalizing disorders may experience sadness or anxiety in response to uncertainty, children with ADHD may be more likely to experience frustration (Douglas and Parry 1994; Milich and Okazaki 1991) as they fail to effectively cope with and manage intense negative emotions. Studies examining the behavior of children with ADHD during problem-solving tasks have found that children with ADHD experience and express greater frustration relative to typically developing children. Further, children with ADHD attempt to solve fewer problems, and frequently quit tasks sooner than typically developing children (Scime and Norvilitis 2006; Walcott and Landau 2004). Children with ADHD may demonstrate impaired functioning and an inability to complete difficult tasks due to feelings of uncertainty over whether or not they will fail. It is possible that the uncertainty associated with an unsolved problem elicits increased affect among children with ADHD beyond that of typically developing children, which is intolerable, and reduced through maladaptive emotion regulation strategies, thereby increasing levels of IU within this population.
Research questions
Though emotion dysregulation is present among both internalizing and externalizing disorders, current literature has focused on addressing the mechanism of IU among the former. Therefore, the current study sought to evaluate IU as a transdiagnostic construct present among disorders associated with emotion dysregulation by comparing IU among children with ADHD to IU among children with known increases in IU (i.e., anxiety disorders), and to typically developing children. Child populations were chosen to inform models of the developmental psychopathology of IU (Read et al. 2013) and to address questions regarding the foundational nature of IU (Shihata et al. 2016). The current study examined total IU, prospective IU (i.e., desire for predictability), and inhibitory IU (i.e., paralysis and impaired functioning arising from uncertainty) in the three populations of interest (Birrell et al. 2011; Hong and Lee 2015).
Given the evidence that children with ADHD experience heightened affect in uncertain situations, beyond that of typically developing children, and demonstrate maladaptive behaviors as a response, the current study posited the following hypotheses: (1) Children with anxiety disorders and ADHD will demonstrate significantly more total IU, prospective IU, and inhibitory IU relative to unaffected children; (2) children with anxiety disorders will demonstrate significantly greater prospective IU relative to children with ADHD due to the anticipatory nature of anxiety disorders (Kertz and Woodruff-Borden 2013) and children with ADHD will demonstrate significantly greater inhibitory IU relative to children with anxiety disorders due to difficulties controlling behavioral responses to increased affect (Scime and Norvilitis 2006).
Methods
The current study was conducted using participants from two larger samples; therefore, only procedures relevant to the current study are outlined. Participants were recruited through elementary and middle schools, contacts in the local community, and flyers distributed throughout the community. Study procedures were approved by the Institutional Review Board at the University of Louisville. Parents of children provided informed consent and children provided assent prior to initiation of any study procedures.
Children without anxiety disorders and ADHD represented a community sample rather than a healthy control sample; thus, children were not excluded from the study if they had symptoms of anxiety disorders or ADHD but did not meet criteria for diagnosis. To ensure that the non-anxiety sample and the non-ADHD sample represented a true community sample, children were included in the study regardless of the presence of disorders other than anxiety disorders and ADHD.
The ethnic composition of the study sample was reflective of the area from which the population was collected (US Census Bureau, 2010) with 71.0% non-Hispanic White/Caucasian, 18.3% non-Hispanic Black/African-American, 2.2% Hispanic/Latino, 2.2% Asian/Pacific Islander, and 6.4% other racial/ethnic background.
Sample 1
Participants included a total of 51 children: 36 children with anxiety disorders (16 boys, 20 girls; mean age = 9.83 ± 1.73) and 15 children without anxiety disorders or ADHD (8 boys, 7 girls; mean age = 9.47 ± 1.89; Table 1).
Parents completed the Anxiety Disorders Interview Schedule-IV-Parent Version (ADIS-P) and children completed the Anxiety Disorders Interview Schedule-IV-Child Version (ADIS-C; Albano and Silverman 1996) to assess for the presence of anxiety disorders and/or ADHD. The ADIS-C/P is a semi-structured interview that assesses for anxiety and mood disorders as outlined in the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., text revision (APA 1994). The interview is organized by initial screening questions for each of the disorders, with in-depth modules administered following affirmative responses. The ADIS-C/P has strong psychometric properties, with good to excellent levels of reliability for the majority of DSM-IV categories (Silverman et al. 2001). Children completed the Intolerance Uncertainty Scale (IUS; Freeston et al. 1994) to assess child self-perceived IU. The IUS is a 27-item child self-report measure that assesses reactions to uncertainty, ambiguous situations, and the future (Carleton et al. 2007). Item responses are based on a 5-point Likert-type scale. The IUS is most commonly summed as a total score (Antony et al. 2001) and has demonstrated excellent internal consistency (Freeston et al. 1994) and good test–retest reliability (Dugas et al. 1997). The IUS was converted to the Intolerance of Uncertainty Scale—Short Version (IUS-12; Carleton et al. 2007) to allow for comparison to participants in sample 2. Though participants in sample 1 did not complete measure items in the same order as those in sample 2, this is unlikely to be problematic, based on previous psychometric examinations of the IUS (Carleton et al. 2012b). Monetary compensation was given to families. Exclusion criteria for children included being younger than 7 years or older than 12 years, being the non-biological child of their parent, having developmental delays, and receiving a diagnosis of ADHD.
Sample 2
Participants included a total of 42 children: 28 children with ADHD (20 boys, 8 girls; mean age = 8.96 ± 1.45) and 14 children without ADHD or anxiety disorders (9 boys, 5 girls; mean age = 9.14 ± 1.29; see Table 1). The ADHD module of the DISC-P contains a question related to current use of psychotropic medications to treat ADHD (stimulant and non-stimulant). This question was used to assess active ADHD medication usage, and 9 of 28 children with ADHD were receiving medication treatment at baseline.
Parents completed the Diagnostic Structured Interview for Children-Version IV, Parent Report (DISC-P; Shaffer et al. 2000) to assess for ADHD diagnostic status and/or presence of anxiety disorders. The DISC-P was used to provide diagnostic assessment of children in the study. The DISC-P is a diagnostic structured interview that provides a reliable means of assessing for the presence of psychological disorders in children and has demonstrated reliability and validity in a broad array of settings (Shaffer et al. 2000). Children completed an adapted version of the Intolerance Uncertainty Scale—Short Version (IUS-12; Carleton et al. 2007) to assess child self-perceived IU. The reduced IUS-12 has been shown to retain exemplary internal consistency and correlated well with the original IUS (Carleton et al. 2007). Furthermore, the IUS-12 allows for comparison of a total IU, and a two-factor structure which represent both anxious (IU-Prospective) and avoidance (IU-Inhibitory) components of IU (Carleton et al. 2007). Monetary compensation was given to families. Exclusion criteria for children included being younger than 7 years or older than 13 years, and receiving a diagnosis of an anxiety disorder.
Statistical analyses
First, one-way analyses of variance (ANOVAs) were used to investigate demographic differences (i.e., age, sex, ethnicity) between anxiety disorders, ADHD, and unaffected samples. Next, a 3 (Group: unaffected, anxiety disorder, or ADHD) × 3 (Scale: total IU, prospective IU, or inhibitory IU) linear mixed model (LMM) analysis of covariance (ANCOVA) was used to examine study hypotheses. An LMM procedure was used to accommodate the nested structure of the data, as prospective and inhibitory IU subscale scores are also components of total IU. While general linear model (GLM) analyses assume that all observations are independent of one another, LMM permits observations to exhibit correlated variability (Jensen et al. 2008; Peugh 2010). Because LMM does not allow for multiple dependent variables, a repeated measures approach was employed. Given previous research suggesting that ADHD medications may reduce symptoms of impulsivity, inattention, and hyperactivity (Pelham and Fabiano 2008), ADHD stimulant medication was included as a covariate, in addition to age and sex. Two planned contrasts were used to test study hypotheses. The first examined total IU, prospective IU, and inhibitory IU in unaffected children relative to children with ADHD and anxiety disorders. The second examined an interaction contrast (Group × Scale) for anxiety disorder and ADHD groups, and prospective and inhibitory IU scales only. To protect against inflating the Type I error rate, the Bonferroni procedure was employed for the two planned contrasts (α = .05/2 = .025). All data were analyzed using SPSS® 23 software (Armonk, NY).
Results
Preliminary analysis
The homogeneity-of-regression assumption indicated that the relationship between the covariates and total IU did not differ significantly as a function of child diagnostic status (F(2,90) = .11, p = .90). The relationships between the covariates and prospective IU (F(2,90) = .13, p = .88) and inhibitory IU (F(2,90) = 2.25, p = .11) also did not differ significantly as a function of child diagnostic status.
Hypothesis testing
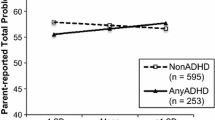
The LMM analysis of repeated measures indicated a significant Scale by Group interaction (F(4180) = 6.30, p < .001). Estimated marginal means for each Scale by Group are represented in Fig. 1. The contrast between the two clinical groups (i.e., anxiety disorders and ADHD) and the unaffected group was significant for Scale (t(90) = 2.37, p = .02), indicating that children in the clinical groups reported significantly higher total IU, prospective IU, and inhibitory IU scores than unaffected children. The contrast between the anxiety disorder and ADHD groups for prospective IU and inhibitory IU scores was also significant (t(180) = 3.75, p < .001) indicating an interaction between the two affected groups at the subscale level. Pairwise comparisons of estimated marginal means revealed that inhibitory IU did not significantly differ between anxiety disorder (M = 12.13) and ADHD (M = 12.38) groups (95% CI [− 3.44, 2.96]). A post hoc power analysis was computed to determine whether nonsignificant results were due to issues with power. Though there is no agreed upon method for determining power in LMM analyses, effect sizes for GLM ANOVA can be substituted to estimate achieved power (Edwards et al. 2008). A Cohen’s ƒ of .34 was obtained based on study analyses and yielded power = .97 (Faul et al. 2007). A medium effect size is consistent with past studies examining IU and child psychopathology (Osmanagaoglu et al. 2017).

Total IU, prospective IU, and inhibitory IU by child diagnostic status
Discussion
The current results represent a step toward understanding IU as a transdiagnostic mechanism through which childhood psychopathology develops. To our knowledge, this is the first study to examine IU in an externalizing population diagnosed with ADHD. Consistent with our first hypothesis, children with anxiety disorders and ADHD demonstrated significantly greater total IU, prospective IU, and inhibitory IU relative to unaffected children. Regarding our second hypothesis, anxiety and ADHD groups did significantly differ by subscale score. Though graphical interpretation confirmed that children with anxiety disorders report significantly more prospective IU compared to children with ADHD, follow-up analyses revealed that inhibitory IU levels were comparable between these two groups.
Implications
Childhood IU has typically been associated with internalizing disorders; however, the current study reveals that IU levels in children with ADHD are comparable to those of children with anxiety disorders. The current results may suggest that IU is linked to emotion dysregulation broadly, rather than being a risk factor for the development of a specific disorder. Emotion dysregulation has consistently been identified as a core component of childhood anxiety disorders (Suveg and Zeman 2004; Tan et al. 2012). Children with anxiety disorders experience intense and uncontrollable affect, and report little confidence in managing these experiences (Hannesdottir and Ollendick 2007). Similar deficits in emotional regulation and control are central to an ADHD diagnosis as well (Shaw et al. 2014). While aspects of emotion regulation were not measured here, given the link between IU, emotion, and emotion regulation, the current study suggests that IU arises among children who experience emotion dysregulation regardless of whether symptoms are primarily internalizing or externalizing. Uncertainty elicits and increases affect and is perceived as being more aversive across the population (FeldmanHall et al. 2016). Among individuals who already experience emotion as being uncontrollable and unpleasant, uncertainty may become intolerable.
Our results of increased IU among children with anxiety disorders are supported by current literature. Research suggests that among this population, uncertainty signals threat, which triggers perseverative worry about what may happen in the future as a result of current uncertainty (Fialko et al. 2012). Among internalizing disorders, IU is linked to anxiety and sadness (Mahoney and McEvoy 2012). Children with ADHD, however, appear to primarily experience frustration in response to uncertainty (Scime and Norvilitis 2006). Problem-solving paradigms contain inherent uncertainty. When children with ADHD are faced with problem-solving tasks, they are exposed to the uncertainty associated with information processing, solution generation, decision making, etc. In the presence of reactivity and inability to regulate the frustration associated with this uncertainty, children with ADHD are more likely to demonstrate maladaptive behaviors such as avoiding further problem-solving and engaging in aggression (Walcott and Landau 2004). Accordingly, children with ADHD reported significantly higher levels of inhibitory IU as compared to typically developing children in this sample. This suggests that children with ADHD experience uncertainty as intolerable because they believe uncertainty restricts their ability to act. In previous studies, individuals who exhibited higher levels of inhibitory IU were more likely to “freeze-up” and use avoidance-based strategies during uncertain conditions (Hong and Lee 2015).
Though the current study hypothesized that children with ADHD would experience significantly higher inhibitory IU, compared to anxious children, as a result of this tendency to freeze-up and avoid uncertainty, results did not reveal statistically significant differences in inhibitory IU between children with ADHD and children with anxiety disorders. Previous studies have found that inhibitory IU measures some aspects of behavioral inhibition, a risk factor for the development of anxiety disorders (Carleton 2016b). While anxious children demonstrated significantly more prospective IU than children with ADHD, they may also endorse high levels of inhibitory IU as well due to increased behavioral inhibition in this population.
The current study has implications for the treatment of childhood psychopathology as well. New treatments for emotional disorders have targeted IU with promising results (McEvoy and Erceg-Hurn 2015). Among emotional disorders, reductions in IU throughout treatment have predicted reductions in overall severity and distress (Boswell et al. 2013). Further, cutting edge treatments aimed at increasing tolerance for uncertainty have shown promising results in the reduction of anxiety symptoms among youth (Rodgers et al. 2016). IU may be an important treatment target for externalizing populations as well. Future studies should continue to investigate how IU is linked to ADHD, and how treatments aimed at reducing IU may aid in the treatment of ADHD. Future studies should also continue to investigate IU as a transdiagnostic construct by examining levels of IU among other externalizing disorders, and elucidating which factors link IU to psychopathology broadly, rather than to diagnoses specifically.
Limitations
This study provided encouraging support for the presence of IU in children with externalizing disorders. However, several limitations must be acknowledged. This study represented an initial and preliminary examination of IU in children presenting with externalizing disorders. Although this study demonstrated that elevated IU is present in both children with internalizing and externalizing disorders, all data in this study were obtained concurrently. Thus, it is not possible to deconstruct the direction of the effects demonstrated in this study. Further studies are needed to demonstrate the longitudinal direction of this relation to determine if the IU assessed in this study is caused by or is the result of psychopathology in children. Indeed, it is possible that a dynamic and bidirectional effect exists between IU and internalizing and externalizing disorders. Future studies should also seek to investigate IU in a larger sample of children with internalizing and externalizing disorders.
The current study included participants from two separate samples. Although the use of two samples was necessary given the aims of the study, each sample recruited participants independently and administered somewhat disparate measures of IU. Sample one employed the IUS (Freeston et al. 1994) and sample 2 administered an adapted version of the IUS-12 (Carleton et al. 2007). Fortunately, the IUS (Freeston et al. 1994) can be converted to the IUS-12 (Carleton et al. 2007) by selecting 12 questions directly from the original IUS developed by Freeston et al. (1994). Given that the IUS-12 correlates well with the original IUS and retains exemplary internal consistency (Carleton et al. 2007), the decision to convert the IUS to the IUS-12 allowed for comparison of IU across children with internalizing and externalizing disorders. Furthermore, conversion of the original IUS (Freeston et al. 1994) to the IUS-12 (Carleton et al. 2007) allowed for comparison of total IU, prospective IU, and inhibitory IU in children with internalizing and externalizing disorders.
Additionally, disparate methods were employed to assess for the presence of anxiety disorders and ADHD in the two samples. Sample one utilized the ADIS-C/P (Albano and Silverman 1996) to diagnose anxiety disorders, and sample two utilized the DISC-P (Shaffer et al. 2000) to diagnose ADHD. Although this is a limitation, the ADIS-C/P has demonstrated strong psychometric properties, with good to excellent levels of reliability for the majority of DSM-IV categories (Silverman et al. 2001), and the DISC-P has demonstrated reliability and validity in the assessment of psychological disorders in children (Shaffer et al. 2000). Further, each diagnostic tool was selected specifically for the intended population. Thus, the ADIS-C/P is indicated as one of the most valid assessments of childhood anxiety disorders, while the DISC-P is one of the most valid tools for the assessment of childhood ADHD. Children with anxiety disorders were only included in the study if they did not meet criteria for ADHD, and children with ADHD were only included in the study if they did not meet criteria for an anxiety disorder. Therefore, although disparate methods of measurement were employed in the current study, only children affected by anxiety disorders or ADHD were included in the current study to allow for comparison of IU in children with internalizing and externalizing disorders. This is also a study strength, as levels of IU in our child ADHD sample cannot be attributed to the presence of clinical anxiety among the ADHD group.
Given that anxiety disorders and ADHD have been shown to be highly comorbid and often results in greater child impairment (Schatz and Rostain 2006), future studies should seek to compare IU in children with anxiety disorders and ADHD to children with comorbid anxiety disorders and ADHD. Furthermore, though anxiety disorder status was determined through a multi-informant approach, ADHD diagnostic status was determined by parent report alone due to practical limitations. Future studies should attempt to incorporate a multi-informant approach when diagnosing ADHD in children.
Conclusion
The current study is the first to demonstrate that IU is present among children with externalizing disorders, and further substantiates literature regarding the presence of IU in children with internalizing disorders. IU may arise in children who experience emotional reactivity and dysregulation broadly, as the inability to regulate and control negative emotions elicited by uncertainty causes distress and leads to maladaptive coping behaviors. This pattern of impairment may be differentially related to children with internalizing and externalizing disorders. For children with internalizing disorders, the inability to modulate emotional reactivity and regulation when thinking about future uncertainty may lead to elevated ratings of prospective IU, whereas for externalizing disorders, the inability to modulate emotional reactivity and regulation in the presence of uncertain events may lead to elevated ratings of inhibitory IU.
References
Albano AM, Silverman WK (1996) The anxiety disorders interview schedule for children for DSM-IV: clinician manual (child and parent versions). Psychological Corporation, San Antonio
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington. https://doi.org/10.1176/appi.books.9780890425596.744053
Antony MM, Orsillo SM, Roemer L (2001) Practitioner’s guide to empirically based measures of anxiety. New York. https://doi.org/10.1007/b108176
APA (1994) Diagnostic and statistical manual of mental disorders, 4th edn. American Psychiatric Publishing, Washington, DC, pp 69–81
Bar-Anan Y, Wilson TD, Gilbert DT (2009) The feeling of uncertainty intensifies affective reactions. Emotion 9(1):123–127. https://doi.org/10.1037/a0014607
Barkley RA (1997) Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull 121(1):65–94. https://doi.org/10.1037/0033-2909.121.1.65
Barkley R (2014) Attention-deficit hyperactivity disorder: a handbook for diagnosis and treatment, vol 628. Guilford Press, New York
Barkley RA (2015) Emotional dysregulation is a core component of ADHD. Atten Deficit Hyperact Disord Handb Diagn Treat 4:81–115
Birrell J, Meares K, Wilkinson A, Freeston M (2011) Toward a definition of intolerance of uncertainty: a review of factor analytical studies of the intolerance of uncertainty scale. Clin Psychol Rev 31(7):1198–1208. https://doi.org/10.1016/j.cpr.2011.07.009
Blair KS, Vythilingam M, Crowe SL, Mccaffrey DE, Ng P, Wu CC et al (2015) Cognitive control of attention is differentially affected in trauma-exposed individuals with and without post-traumatic stress disorder. Psychol Med 43(1):85–95. https://doi.org/10.1017/S0033291712000840.Cognitive
Boswell JF, Thompson-Hollands J, Farchione TJ, Barlow DH (2013) Intolerance of uncertainty: a common factor in the treatment of emotional disorders. J Clin Psychol 69(6):1–16. https://doi.org/10.1002/jclp.21965
Bylsma LM, Morris BH, Rottenberg J (2008) A meta-analysis of emotional reactivity in major depressive disorder. Clin Psychol Rev 28(4):676–691. https://doi.org/10.1016/j.cpr.2007.10.001
Carleton RN (2012) The intolerance of uncertainty construct in the context of anxiety disorders: theoretical and practical perspectives. Expert Rev Neurother 12(8):937–947. https://doi.org/10.1586/ern.12.82
Carleton RN (2016a) Fear of the unknown: one fear to rule them all? J Anxiety Disord 41:5–21. https://doi.org/10.1016/j.janxdis.2016.03.011
Carleton RN (2016b) Into the unknown: a review and synthesis of contemporary models involving uncertainty. J Anxiety Disord 39:30–43. https://doi.org/10.1016/j.janxdis.2016.02.007
Carleton RN, Norton MAPJ, Asmundson GJG (2007) Fearing the unknown: a short version of the intolerance of uncertainty scale. J Anxiety Disord 21(1):105–117. https://doi.org/10.1016/j.janxdis.2006.03.014
Carleton RN, Mulvogue MK, Thibodeau MA, McCabe RE, Antony MM, Asmundson GJG (2012a) Increasingly certain about uncertainty: intolerance of uncertainty across anxiety and depression. J Anxiety Disord 26(3):468–479. https://doi.org/10.1016/j.janxdis.2012.01.011
Carleton RN, Thibodeau MA, Osborne JW, Asmundson GJG (2012b) Exploring item order in anxiety-related constructs: practical impacts of serial position. Pract Assess Res Eval 17(7):1–15
Cisler JM, Olatunji BO, Feldner MT, Forsyth JP (2010) Emotion regulation and the anxiety disorders: an integrative review. J Psychopathol Behav Assess. https://doi.org/10.1007/s10862-009-9161-1
Cole PM, Martin SE, Dennis TA (2004) Emotion regulation as a scientific construct : methodological challenges and directions for child development research. Chil Dev 75(2):317–333
Douglas VI, Parry PA (1994) Effects of reward and nonreward on frustration and attention in attention deficit disorder. J Abnorm Child Psychol 22(3):281–302. https://doi.org/10.1007/BF02168075
Dugas MJ, Freeston MH, Ladouceur R (1997) Intolerance of uncertainty and problem orientation in worry. Cogn Ther Res 21(6):593–606. https://doi.org/10.1023/A:1021890322153
Edwards L, Muller K, Wolfinger R, Qaqish B, Schabenberger O (2008) An R2 statistic for fixed effects in the linear mixed model. Stat Med 27(29):6137–6157. https://doi.org/10.1002/sim.3429.An
Ehring T, Ehlers A (2014) Does rumination mediate the relationship between emotion regulation ability and posttraumatic stress disorder? Eur J Psychotraumatol 5:1–7. https://doi.org/10.3402/ejpt.v5.23547
Einstein DA (2014) Extension of the transdiagnostic model to focus on intolerance of uncertainty: a review of the literature and implications for treatment. Clin Psychol Sci Pract 21(3):280–300. https://doi.org/10.1111/cpsp.12077
Faul F, Erdfelder E, Lang A-G, Buchner A (2007) G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39(2):175–191. https://doi.org/10.3758/BF03193146
FeldmanHall O, Glimcher P, Baker AL, Phelps EA (2016) Emotion and decision-making under uncertainty: physiological arousal predicts increased gambling during ambiguity but not risk. J Exp Psychol Gen 145(10):1255–1262. https://doi.org/10.1037/xge0000205
Fetzner MG, Horswill SC, Boelen PA, Carleton RN (2013) Intolerance of uncertainty and PTSD symptoms: exploring the construct relationship in a community sample with a heterogeneous trauma history. Cogn Ther Res 37(4):725–734. https://doi.org/10.1007/s10608-013-9531-6
Fialko L, Bolton D, Perrin S (2012) Applicability of a cognitive model of worry to children and adolescents. Behav Res Ther 50(5):341–349. https://doi.org/10.1016/j.brat.2012.02.003
Freeston MH, Rhéaume J, Letarte H, Dugas MJ, Ladouceur R (1994) Why do people worry? Personal Individ Differ 17(6):791–802. https://doi.org/10.1016/0191-8869(94)90048-5
Gentes EL, Ruscio AM (2011) A meta-analysis of the relation of intolerance of uncertainty to symptoms of generalized anxiety disorder, major depressive disorder, and obsessive-compulsive disorder. Clin Psychol Rev 31(6):923–933. https://doi.org/10.1016/j.cpr.2011.05.001
Greco V, Roger D (2003) Uncertainty, stress, and health. Personal Individ Differ 34(6):1057–1068. https://doi.org/10.1016/S0191-8869(02)00091-0
Hannesdottir DK, Ollendick TH (2007) The role of emotion regulation in the treatment of child anxiety disorders. Clin Child Fam Psychol Rev 10(3):275–293. https://doi.org/10.1007/s10567-007-0024-6
Hong RY, Lee SSM (2015) Further clarifying prospective and inhibitory intolerance of uncertainty: factorial and construct validity of test scores from the intolerance of uncertainty scale. Psychol Assess 27(2):605–620. https://doi.org/10.1037/pas0000074
Hsu KJ, Beard C, Rifkin L, Dillon DG, Pizzagalli DA, Björgvinsson T (2015) Transdiagnostic mechanisms in depression and anxiety : the role of rumination and attentional control. J Affect Disord 188:22–27. https://doi.org/10.1016/j.jad.2015.08.008
Huettel SA, Song AW, McCarthy G (2005) Decisions under uncertainty: probabilistic context influences activation of prefrontal and parietal cortices. J Neurosci 25(13):3304–3311. https://doi.org/10.1523/JNEUROSCI.5070-04.2005
Jensen WA, Birch JB, Woodall WH (2008) Monitoring correlation within linear profiles using mixed models. J Qual Technol 40:167–183
Kertz S, Woodruff-Borden J (2013) The role of metacognition, intolerance of uncertainty, and negative problem orientation in children’s worry. Behav Cogn Psychother 41(2):243–248. https://doi.org/10.1017/S1352465812000641
Mahoney AEJ, McEvoy PM (2012) A transdiagnostic examination of intolerance of uncertainty across anxiety and depressive disorders. Cogn Behav Ther 41(3):212–222. https://doi.org/10.1080/16506073.2011.622130
Martel MM (2009) Research review: a new perspective on attention-deficit/hyperactivity disorder: emotion dysregulation and trait models. J Child Psychol Psychiatry 50(9):1042–1051
McEvoy PM, Erceg-Hurn DM (2015) The search for universal transdiagnostic and trans-therapy change processes: evidence for intolerance of uncertainty. J Anxiety Disord 41:96–107. https://doi.org/10.1016/j.janxdis.2016.02.002
Milich R, Okazaki M (1991) An examination of learned helplessness among attention-deficit hyperactivity disordered boys. J Abnorm Child Psychol 19(5):607–623. https://doi.org/10.1007/BF00925823
Mogg K, Salum GA, Bradley BP, Gadelha A, Pan P, Alvarenga P et al (2015) Attention network functioning in children with anxiety disorders, attention-deficit/hyperactivity disorder and non-clinical anxiety. Psychol Med 45:2633–2646. https://doi.org/10.1017/S0033291715000586
Mushtaq F, Bland AR, Schaefer A (2011) Uncertainty and cognitive control. Front Psychol 2:1–14. https://doi.org/10.3389/fpsyg.2011.00249
Osmanagaoglu N, Creswell C, Dodd HF (2017) Intolerance of uncertainty, anxiety, and worry in children and adolescents: a meta-analysis. J Affect Disord. https://doi.org/10.1016/j.jad.2017.07.035
Paulus MP, Yu AJ (2012) Emotion and decision-making: affect-driven belief systems in anxiety and depression. Trends Cogn Sci 16(9):133–149. https://doi.org/10.1016/j.tics.2012.07.009.Emotion
Pelham WE, Fabiano GA (2008) Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. https://doi.org/10.1080/15374410701818681
Peugh JL (2010) A practical guide to multilevel modeling. J Sch Psychol 48(1):85–112. https://doi.org/10.1016/j.jsp.2009.09.002
Polanczyk G, De Lima MS, Horta BL, Biederman J, Rohde LA (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164(6):942–948. https://doi.org/10.1176/appi.ajp.164.6.942
Read KL, Comer JS, Kendall PC (2013) The intolerance of uncertainty scale for children (IUSC): discriminating principal anxiety diagnoses and severity. Psychol Assess 25(3):722–729. https://doi.org/10.1037/a0032392
Reinholdt-Dunne ML, Mogg K, Vangkilde SA, Bradley BP, Esbjorn BH, Esbjørn BH, Esbjorn BH (2015) Attention control and attention to emotional stimuli in anxious children before and after cognitive behavioral therapy. Cogn Ther Res 39(6):785–796. https://doi.org/10.1007/s10608-015-9708-2
Rive MM, van Rooijen G, Veltman DJ, Phillips ML, Schene AH, Ruhe HG (2013) Neural correlates of dysfunctional emotion regulation in major depressive disorder. A systematic review of neuroimaging studies. Neurosci Biobehav Rev 37(10 Pt 2):2529–2553. https://doi.org/10.1016/j.neubiorev.2013.07.018
Rodgers J, Hodgson A, Shields K, Wright C, Honey E, Freeston M (2016) Towards a treatment for intolerance of uncertainty in young people with autism spectrum disorder: development of the coping with uncertainty in everyday situations (CUES??) programme. J Autism Dev Disord 0(0):1–8. https://doi.org/10.1007/s10803-016-2924-0
Rosen JB, Donley MP (2006) Animal studies of amygdala function in fear and uncertainty: relevance to human research. Biol Psychol 73(1):49–60. https://doi.org/10.1016/j.biopsycho.2006.01.007
Rosen PJ, Epstein JN (2010) A pilot study of ecological momentary assessment of emotion dysregulation in children. J ADHD Relat Disord 1(4):39–52
Rosen PJ, Factor PI (2015) Emotional impulsivity and emotional and behavioral difficulties among children with adhd: an ecological momentary assessment study. J Atten Disord 19(9):779–793. https://doi.org/10.1177/1087054712463064
Rosen PJ, Walerius DM, Fogleman ND, Factor PI (2015) The association of emotional lability and emotional and behavioral difficulties among children with and without ADHD. ADHD Atten Deficit Hyperact Disord 7(4):281–294. https://doi.org/10.1007/s12402-015-0175-0
Salters-Pedneault K, Roemer L, Tull MT, Rucker L, Mennin DS (2006) Evidence of broad deficits in emotion regulation associated with chronic worry and generalized anxiety disorder. Cogn Ther Res 30(4):469–480. https://doi.org/10.1007/s10608-006-9055-4
Schatz DB, Rostain AL (2006) ADHD with comorbid anxiety: a review of the current literature. J Atten Disord 10:141–149. https://doi.org/10.1177/1087054706286698
Scime M, Norvilitis JM (2006) Task performance and response to frustration in children with attention deficit hyperactivity disorder. Psychol Sch 43(3):377–386. https://doi.org/10.1002/pits.20151
Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME (2000) NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry 39(1):28–38. https://doi.org/10.1097/00004583-200001000-00014
Shaw P, Stringaris A, Nigg J, Leibenluft E (2014) Emotional dysregulation and attention-deficit/hyperactivity disorder. Am J Psychiatry 171(3):276–293. https://doi.org/10.1176/appi.ajp.2013.13070966
Shihata S, McEvoy PM, Mullan BA, Carleton RN (2016) Intolerance of uncertainty in emotional disorders: what uncertainties remain? J Anxiety Disord 41:115–124. https://doi.org/10.1016/j.janxdis.2016.05.001
Silverman WK, Saavedra LM, Pina AA (2001) Test-retest reliability of anxiety symptoms and diagnoses with the anxiety disorders interview schedule for DSM-IV: child and parent versions. J Am Acad Child Adolesc Psychiatry 40(8):937–944. https://doi.org/10.1097/00004583-200108000-00016
Snyder HR, Kaiser RH, Warren SL, Heller W (2015) Obsessive-compulsive disorder is associated with broad impairments in executive function: a meta-analysis. Clin Psychol Sci 3(2):301–330. https://doi.org/10.1177/2167702614534210
Sobanski E, Banaschewski T, Asherson P, Buitelaar J, Chen W, Franke B et al (2010) Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): clinical correlates and familial prevalence. J Child Psychol Psychiatry Allied Discip 51(8):915–923. https://doi.org/10.1111/j.1469-7610.2010.02217.x
Stern ER, Gonzalez R, Welsh RC, Taylor SF (2010) Updating beliefs for a decision: neural correlates of uncertainty and underconfidence. J Neurosci 30(23):8032–8041. https://doi.org/10.1523/JNEUROSCI.4729-09.2010
Stern MR, Nota JA, Heimberg RG, Holaway RM, Coles ME (2014) An initial examination of emotion regulation and obsessive compulsive symptoms. J Obsessive Compuls Relat Disord 3(2):109–114. https://doi.org/10.1016/j.jocrd.2014.02.005
Suveg C, Zeman J (2004) Emotion regulation in children with anxiety disorders. J Clin Child Adolesc Psychol 33(4):750–759. https://doi.org/10.1207/s15374424jccp3304_10
Tan PZ, Forbes EE, Dahl RE, Ryan ND, Siegle GJ, Ladouceur CD, Silk JS (2012) Emotional reactivity and regulation in anxious and nonanxious youth: a cell-phone ecological momentary assessment study. J Child Psychol Psychiatry Allied Discip 53(2):197–206. https://doi.org/10.1111/j.1469-7610.2011.02469.x
Thielsch C, Andor T, Ehring T (2015) Do metacognitions and intolerance of uncertainty predict worry in everyday life? an ecological momentary assessment study. Behav Ther 46(4):532–543. https://doi.org/10.1016/j.beth.2015.05.001
Tolin DF, Abramowitz JS, Brigidi BD, Foa EB (2003) Intolerance of uncertainty in obsessive-compulsive disorder. J Anxiety Disord 17(2):233–242. https://doi.org/10.1016/S0887-6185(02)00182-2
Volz KG, Schubotz RI, Von Cramon DY (2003) Predicting events of varying probability: uncertainty investigated by fMRI. NeuroImage 19(2):271–280. https://doi.org/10.1016/S1053-8119(03)00122-8
Walcott CM, Landau S (2004) The relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder the relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol 33(4):772–782. https://doi.org/10.1207/s15374424jccp3304
Wehmeier PM, Schacht A, Barkley RA (2010) Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. J Adolesc Health. https://doi.org/10.1016/j.jadohealth.2009.09.009
Acknowledgements
Colette Gramszlo and Nicholas D. Fogleman contributed equally to this manuscript.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Gramszlo, C., Fogleman, N.D., Rosen, P.J. et al. Intolerance of uncertainty in children with attention-deficit/hyperactivity disorder. ADHD Atten Def Hyp Disord 10, 189–197 (2018). https://doi.org/10.1007/s12402-017-0244-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12402-017-0244-7