
Abstract
This study employed a paired stimulus paradigm to compare phasic changes in heart rate among children (age categories 6–8, 9–10, and 11–12) and adults (age categories 18–19 and 20–22) with attention-deficit/hyperactivity disorder (ADHD) and age-matched controls. A sample of 95 participants (19 ADHD-diagnosed children, 34 controls, 20 ADHD-diagnosed adults, and 22 controls) solved a planning task, the Tower of London, through 4 levels of difficulty. It was hypothesized that groups with ADHD would show greater heart rate acceleration and less final deceleration than would controls, and that these heart rate responses would change with age and difficulty level as well. Though heart rate differences were found among age categories and difficulty levels, none were found between participants with ADHD and controls. The lack of ADHD differences are not consistent with the behavioral evidence that planning by itself is one of the marked executive function deficits in ADHD. Because ADHD differences were not evident, the effects either were not present or were smaller than that of difficulty level and age. Possible explanations for this lack of difference and future directions are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Executive functions are complex brain functions associated with the frontal lobes and include inhibition, manipulation and updating of information, planning, and attentional set-shifting (Berg and Byrd 2009). They allow a person to engage in autonomous, purposeful, self-serving behavior (Lezak 1995), and most children develop basic executive functions, such as searching and planning, by age 6, with higher functions, such as complex working memory and verbal fluency, developing after age 12 (Welsh et al. 1991). Individuals with attention-deficit/hyperactivity disorder (ADHD) tend to exhibit poorer performance on many executive functioning tasks (Willcutt et al. 2005), including the N-Back, a measure of working memory (Shallice et al. 2002), the continuous performance task, an index of sustained attention (Berlin et al. 2004), the day–night stroop, a measure of inhibition (Berlin et al. 2004), and the Dresden Breakfast Task, tapping time-based prospective memory (Altgassen et al. 2012). Uniting the multiple executive functions into a unified theory of ADHD, Barkley (1997) proposed that “Most, if not all, of the cognitive deficits associated with ADHD seem to fall within the realm of self-regulation or executive functions” (p. 67).
Executive function tasks lend themselves to the Stimulus 1/Stimulus 2 paradigm, which presents participants with two successive stimuli. Stimulus 1 (S1) warns the participant of the upcoming Stimulus 2 (S2), and a fixed wait period, known as the inter-stimulus interval (ISI), separates the two stimuli. Because behavioral research using S1–S2 paradigms focuses on the motor response after the S2, inferences about cognitive events during the ISI must be made retroactively. Psychophysiological research using the S1–S2, however, focuses on the cognitive events during the ISI, providing direct information about those events (Berg and Byrd 2002).
To tap into the cognitive events occurring during the ISI in S1–S2 paradigms, researchers can examine heart rate fluctuations with an electrocardiogram (ECG). When the ISI in an S1–S2 paradigm is at least 5–6 s long, a triphasic structure emerges in participants’ heart rate patterns (Bohlin and Kjellberg 1979; Koers et al. 1997; Berg and Byrd 2009). This triphasic heart rate pattern involves an initial deceleration (D1), acceleration (A), and a second deceleration (D2). Lacey (1959) proposed that heart rate deceleration is the result of processing sensory input, or detecting and “accepting” the environment. Deceleration occurs with the presentation of a novel stimulus (Graham and Clifton 1966), and Graham and Clifton (1966) referred to deceleration as an “orienting response.” Heart rate acceleration, then, occurs as a result of the opposite reaction, or focusing on internal mental processes (Lacey and Lacey 1970).
In the triphasic heart rate pattern, the initial heart rate deceleration (D1) occurs immediately after S1 to focus participants’ attention on the stimulus (Porges 1984) by optimally tuning the appropriate sensory receptor organs (Sokolov 1963). Focus then turns from the stimulus to the cognitive requirements accompanying that stimulus, causing acceleration (A). The A component is larger with greater task difficulty (Walter and Porges 1976; Dennis and Mulcahy 1980), strong anticipation of S2 (Coles and Duncan-Johnson 1975; Griffin et al. 1995), and younger age groups (Byrd and Berg 2002). It is considered to reflect deeper stimulus processing, decision making, and executive functioning (Berg and Byrd 2009). The third component, D2, appears as a participant focuses back on the environment, anticipating the onset of S2 or preparing a motor response (Koers et al. 1997), and D2 peaks at the appearance of S2 (Bohlin and Kjellberg 1979). D2 can also be seen as a result of motor inhibition at the central nervous system level (Jennings et al. 1997), as a participant must delay motor response until S2.
Since children often exert more effort than adults on the same cognitive task, children’s A components tend to be larger (Anthony and Putnam 1982; Lawler et al. 1978; Byrd and Berg 2002) and are delayed in peak amplitude (Anthony and Putnam 1982; Byrd and Berg 2002). Heart rate research has also shown differences for ADHD populations, as children with inattention problems exhibited significantly less heart rate deceleration (D2) before simple reaction stimuli (Sroufe et al. 1973; Zahn et al. 1978). Sroufe et al. (1973) compared the heart rates of these children on and off methylphenidate (Ritalin), finding that the drug increased D2 amplitude. Despite the studies on heart rate deceleration and ADHD, some even using an S1–S2 paradigm, research on the triphasic heart rate response in ADHD populations has, to our knowledge, not been undertaken.
Current study
This study used a computerized version of the Tower of London (TOL; Shallice 1982) presented in an S1–S2 paradigm with a 6-s ISI to examine differences in the A and D2 components of the triphasic heart rate with respect to the following independent variables: ADHD status, age category, and problem difficulty. The TOL was specifically chosen because it primarily measures planning (Berg and Byrd 2002; Unterrainer et al. 2004), as well visuo-spatial working memory and inhibition (Welsch et al. 1999). Planning in particular has been shown to be reduced in individuals with ADHD (e.g., Desjardins et al. 2010; Fuermaier et al. 2013). The TOL has commonly been considered an index of planning in children (Culbertson and Zillmer 1998) and adults (Berg and Byrd 2002; Riccio et al. 2004), and adults with ADHD have been shown to have reduced performance than controls on the TOL (Tucha et al. 2011). Although planning tasks typically involve longer time than 6 s, this 6-s ISI was chosen additionally to tap working memory and to elicit the triphasic heart rate response.
It is proposed that because participants with ADHD must exert greater cognitive effort and attentional control to match their non-ADHD counterparts, the ADHD group will show triphasic heart rate components indicative of a greater engagement of mental effort and attempts at attentional control with regard to A amplitude and latency, as well as D2 amplitude, as the research to date has suggested these components to be most reflective of executive function engagement. This study differs from previous ADHD studies because it taps not only inhibition with the fixed foreperiod reaction time paradigm, but more directly working memory and planning ability, as the varied difficulty of TOL problems can more precisely measure cognitive load.
Methods
Participants
Child participants for this study were contacted through local schools, churches, and doctors’ offices. Adults were recruited from a university’s introductory psychology classes and from flyers distributed on campus. ADHD-diagnosed participants received $25 for participating, non-ADHD-diagnosed participants received $15, and students participating in the study to fulfill a class research requirement received credit. From the initial sample of 171, 10 participants were excluded for having IQ scores below 80, 18 for being under the influence of psychotropic medications at time of testing, 21 for poor ECG data quality primarily due to high impedances in the electrodes or excessive motor movement from participants, 7 due to computer and research errors, 12 for having a disparity between self-report of ADHD and clinical assessment, and 8 participants for being unavailable for the clinical assessments, leaving a total of 95 participants for analyses. Measures used to assess ADHD are described below.
Participants fell into one of the four categories as follows: ADHD-diagnosed children (n = 19), non-ADHD-diagnosed children (n = 34), ADHD-diagnosed adults (n = 20), and non-ADHD-diagnosed adults (n = 22). To examine developmental differences and age interactions with ADHD, both the child and adult groups were subdivided by age, creating 3 categories for children (6–8, 9–10, and 11–12) and 2 for adults (18–19 and 20–22). A participant demographic summary appears in Table 1.
Measures
Tower of London (TOL)
Participants completed a modified version of the TOL presented on a 30 × 22-cm computer screen at arm’s length. To solve the TOL, participants rearrange three colored balls placed variously on three pegs shown in one image to match the arrangement of the balls on a second image in the least number of moves. Each image contained a board with three pegs, arranged in decreasing length that could hold three, two, and one ball, respectively. Rather than actually moving the balls to solve the TOL, as is typically done in this task, participants instead were asked to mentally re-arrange the balls. This change was designed to enhance considerably the working memory aspects of the task. Participants were instructed on how to play the TOL and asked to indicate their solution by pressing a colored button on a number pad keyboard for the color of the last ball they had mentally moved. All selected problems had only a single solution requiring one particular final ball for a correct, minimal-move solution. Corrections for correct responses obtained by chance are described below.
Each participant completed 96 TOL problems, broken up into four blocks of 24, with each block lasting approximately 5 min. TOL problems in this study involved 0, 1, 2, and 3 moves for children and 0, 2, 3, and 4 moves for adults. Pilot testing showed that 4-move problems were too difficult for children, so they received an easier set of problems. For 0-move problems, the baseline condition, both pictures already matched, and participants were to respond by pressing a black button. This served as a control because participants saw the same visual information (a TOL board) and performed the same motor response. This condition required little or no working memory, nor other executive function requirement. Participants received 6 of each of the 4 types of problems in each block in a pseudo-random order.
Clinical assessments
In addition to the TOL, all participants received two clinical assessments of ADHD symptoms. The first assessment was the ADD Brown Scales (Brown 1996) to identify propensity toward ADHD in controls and to re-affirm diagnoses in ADHD-diagnosed participants. This assessment included statements such as, “Has difficulty sitting still and acts as if ‘driven by a motor,’” (4-point scale with labeled endpoints, with 0 = “Never” and 3 = “Almost Daily”). We excluded from the study all participants who claimed to have been professionally diagnosed with ADHD but received Brown Scale scores of 7 or more points below the cutoff for ADHD (50 for adults and 55 for children). We also excluded all controls who received scores showing significant ADHD-like symptoms (7 or more points into the ADHD range). During this exclusion process, we looked solely at ADD total scores for adults and ADD total standardized scores for children.
The second assessment was the Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS; Geller et al. 2001), used here as an alternative source for identifying ADHD-like symptoms when ADHD participants received Brown Scale scores 1–6 points into the non-ADHD range or when control participants received Brown Scale scores 1–6 points into the ADHD range. This assessment was semi-structured, including open-ended questions such as, “Does your child often forget things at home that he or she needs for school or work?” The semi-structured nature allowed parents and participants to provide whatever additional information they thought important in the assessment. A researcher, blind to participant diagnosis, rated the ADHD section of the KSADS for high or low possibility of ADHD. When these ratings were compared with participants’ clinical official diagnoses, any discrepancy resulted in excluding the participant from the study.
Verbal IQ assessment
Participants received the Peabody Picture Vocabulary Test (PPVT) to estimate their verbal IQ and ability to understand receptive language. In the test, four pictures appeared on a computer screen as the researcher read a word aloud. Participants then pointed to the picture they thought best represented the word. Scores were later standardized and calculated into a verbal IQ, and a minimum verbal IQ score of 80 was necessary for inclusion in the study.
Electrophysiological instruments
ECG was recorded from three sintered electrodes in a modified type II configuration. The two active leads were located at the mastoid behind the ear and the inside the left ankle, and a lead on the frontal area of the cap served as the ground lead. Electro-gel, a Compumedics conductive gel, was inserted into the electrodes to provide a conductance between the skin and the electrodes. Neuroscan computer software recorded the ECG waveform with a Neuroscan Synamps amplifier. Custom offline software converted inter-beat intervals (time between R-waves) to beats per minute for each full second, dividing each trial into 7-s intervals with the 1 s prior to S1 as a baseline. An investigator, blind to the participants’ ADHD diagnoses, also used custom software to detect and correct erroneous inter-beat intervals (ones unreasonably short or long).
Procedure
Either before or after participants came into the laboratory for ECG testing, parents completed over the phone the Brown Scales and KSADS for their children in the study, and adult participants completed both phone assessments themselves. Once in the laboratory, participants were first given the PPVT and then seated in a dental chair in a soundproof room. They were fitted with the EEG cap, ECG, and respiration band. All impedances for heart rate were below 10 kΩ. Before participants began the 96 problems, they received TOL directions and a training block with 12 problems, not included in data analysis. Participants could only move onto the test problems if they were able to complete the easiest levels, namely 0- and 1-move for children and 0- and 2-move for adults. If the researchers felt that participants still did not understand the rules after the training block, they gave them a second training block and explained the directions on paper if necessary.
In the sequence, first a fixation screen with the word “Wait…” appeared for a randomly varying duration of 3–7 s. The TOL then appeared for 6 s during which participants mentally re-arranged the balls. Then, the response command word “NOW!” appeared for 2 s, and participants were to immediately press a button for the color of the last ball they had moved into place. Another screen then appeared for 2 s indicating whether the problem was correct and allotting participants points based on their answers. The feedback was used to keep participants interested and engaged in the task. The feedback had four levels including early answer, which was a response prior to the “NOW!,” (zero points and a clock picture), late or no answer (zero points and a question mark picture), correct answer (two points and a star), or incorrect answer (one point and a blue smiley face). This point-total screen gave way to the varying interval 3–7-s wait screen, and the cycle began again for a new problem. Once participants finished all 96 problems, the electrodes were removed.
Data analysis
A visual examination of the full heart rate waveform was used to help determine whether there was clear support for separate analyses of the individual triphasic components. If this visual examination identified the waveform, analyses were run separately for children and adults using the triphasic heart rate from the baseline second through the 6-s anticipatory/planning interval as a dependent variable. The primary analyses were repeated measures analyses of variance (ANOVAs) in a 7 (seconds) by 4 (difficulty levels) by 2 (ADHD status) by 3 (age—for children) or by 2 (age—for adults) setup. These analyses included the following dependent variables: A amplitude, A latency, and D2 amplitude. The behavioral-dependent variables were proportion correct and reaction time for correct responses. Simes’ (1986) modified Bonferroni procedure was used to control for alpha error accumulation across multiple analyses within a single group of heart rate or behavioral analyses (e.g., based upon ADHD status, problem difficulty, and age).
Results
Heart rate waveform analyses
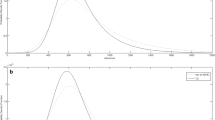
Prior to proceeding with the analyses of components, it is important to demonstrate that the various groups show all three components of the triphasic wave. As shown in Figs. 1 and 2, the response curves showed evidence of all three components of the expected triphasic response in both children and adults: an initial brief deceleration (D1) at approximately 0.5 s post-S1 for all but the oldest adults, a marked acceleration (A) at approximately 1.5 s post-S1, above baseline for all but the youngest children, and a clear late deceleration (D2) maximal at the end of the 6-s interval. Therefore, for all analyses to follow, heart rate results were analyzed in terms of A amplitude, A latency, and D2 amplitude, examining separately the child and adult groups.

Child: triphasic heart rate waveform

Adult: triphasic heart rate waveform
Heart rate acceleration (A) amplitude
ADHD
It was expected that participants with ADHD would exhibit a larger A amplitude than age-matched controls when solving problems of the same difficulty. However, there were no differences in A amplitude between participants with ADHD and age-matched controls among children, F(1, 47) < 1, or adults, F(1, 38) = 1.19, p = .282.
Problem difficulty
It was expected that all four groups would exhibit a larger A component as problem difficulty increased. This was not supported for children, and in fact, A amplitude decreased with increasing problem difficulty, an effect found to be marginally significant, F(1, 47) = 3.69, p = .061. This was also not supported for adults, as no significant linear trend was found in A amplitude across difficulty level, F(1, 38) < 1.
Age
It was expected that younger children, more so than older children, and younger adults, more so than older adults, would exhibit a longer A latency when solving problems of the same difficulty. This was not supported for children, F(1, 47) < 1, or adults, F(1, 38) = 1.01, p = .321. Children and adults were not compared directly because of the differences in difficulty levels and the large age gap between the oldest children and youngest adults.
Heart rate acceleration (A) latency
ADHD
It was expected that ADHD-diagnosed participants would show a later A peak than normal controls during problems of the same difficulty. This hypothesis was not supported for children, F(1, 47) = 1.51, p = .226, or adults, F(1, 38) < 1.
Problem difficulty
It was expected that both children and adults would exhibit a delayed acceleratory component as problem difficulty increased. This hypothesis was not supported for children, F(1, 47) < 1. For adults, there was a very significant effect, but it was for the opposite linear trend, that of earlier latency with greater problem difficulty, F(1, 38) = 11.578, p = .002 (Fig. 3).

Adult: A latency across problem difficulty
Age
It was expected that younger children, more so than older children, and younger adults, more so than older adults, would exhibit a longer A latency when solving problems of the same difficulty. This was not supported for children, F(1, 47) = 3.24, p = .096, or for adults, F(1, 38) < 1.
Heart rate deceleration (D2) amplitude
ADHD
It was expected that both ADHD-diagnosed groups would show a smaller D2 amplitude before the onset of S2 compared to age-matched controls when solving problems of the same difficulty. This hypothesis was not supported for children, F(1, 47) < 1, nor for adults, F(1, 38) = 1.28, p = .264.
Problem difficulty
It was expected that both children and adults would exhibit a smaller D2 amplitude as problem difficulty increased. This effect was not apparent among children, F(3, 141) < 1. For adults, however, this was supported across 0-, 2-, and 3-move problems, as a significant quadratic trend emerged among difficulty levels, F(1, 38) = 11.26, p = .004 (Fig. 4). D2 amplitude decreased with difficulty as expected up to 3-move problems, but then abruptly reversed for the most difficult 4-move problems.

Adult: D2 amplitude across difficulty levels
Age
It was expected that younger children, more so than older children, and younger adults, more so than older adults, would exhibit smaller D2 amplitudes when solving problems of the same difficulty. This effect approached significance with decreasing amplitude for older children F(2, 47) = 2.55, p = .089, but not for adults, F(1, 38) = 1.28, p = .264.
Exploratory analysis
The previous heart rate analyses all considered children and adult groups separately, in part because different difficulty levels were employed for the two age groups. Though age effects were marginal at best with this approach, evidence did suggest that a comparison across all ages may be more fruitful. Therefore, an exploratory D2 amplitude mixed factors 2 (ADHD status) × 5 (age categories) × 3 (difficulty levels) ANOVA was performed. Only the overlapping problem difficulties were analyzed (namely 0-, 2-, and 3-moves). The only significant main effect in this analysis was for age category, F(4, 85) = 4.58, p = .002, with D2 amplitude decreasing for older participants (Fig. 5).

All age categories: D2 amplitude
Behavioral analyses
There were no differences between ADHD-diagnosed participants and age-matched controls on proportion of correct answers for either children, F(1, 47) < 1, or adults, F(1, 38) < 1. However, longer response latencies for correct answers emerged for adults with ADHD than controls, F(1, 38) = 6.30, p = .016, but not for children with ADHD than controls, F(1, 47) < 1.
Collapsing across ADHD-diagnosed participants and controls, as problem difficulty increased, the proportion of correct answers decreased in children with a significant linear trend, F(1, 47) = 207.10, p < .001. Follow-up t tests revealed significant differences among all four difficulty levels, all ps < .001. This same effect emerged for adults, as there were significant effects of difficulty level for the linear trend, F(1, 38) = 208.94, p < .001. Follow-up t tests revealed significant differences among all difficulty levels, all ps < .001, except between 2- and 3-move problems, t(41) = −.16, p = .876.
As problem difficulty increased, reaction time for correct answers increased for children, and trends were both linear, F(1, 47) = 82.07, p < .001, and quadratic, F(1, 47) = 8.02, p = .042. Follow-up t tests revealed significant differences among all difficulty levels, all ps < .001, except between 0- and 1-move problems, t(52) = −1.45, p = .153. This same effect emerged for adults, as significant trends in difficulty level were found to be linear, F(1, 38) = 98.60, p < .001, and quadratic, F(1, 38) = 24.84, p < .001. Follow-up t tests revealed significant differences among all difficulty levels, all ps < .035.
The proportion of correct answers did not increase with a corresponding increase in age category within each age group for children, F(2, 47) = 2.02, p = .144, nor for adults, F(1, 38) < 1. When the children’s proportion correct was collapsed across all three groups and examined with respect to first half versus second half, no differences were found between halves, F(1, 52) < 1. The parallel adult analyses also revealed no differences, F(1, 38) < 1.
Reaction time for correct answers did not decrease with an increase in age category within each age group for children, F(2, 47) < 1, or adults, F(1, 38) < 1. In parallel half analyses to proportion correct, reaction time for correct answers also showed no differences between halves for children, F(1, 52) < 1, or adults, F(1, 38) = 1.05, p = .311. However, exploratory ANOVAs collapsed the child and adult groups on their overlapping problem difficulties (0-, 2-, and 3-moves) and found adults to have a larger proportion of correct answers across all three problem difficulties, all Fs > 16.00, all ps < .001, and a corresponding quicker reaction time, all Fs > 17.14, all ps < .001.
Discussion
This study used the TOL to examine planning in participants with ADHD and controls across the childhood and adult years. During this task, individual triphasic heart rate components differed with respect to the level of executive function engagement. Adults’ A peak latency decreased with increasing problem difficulty, and D2 amplitude decreased across increasing age categories from children through adults. Though triphasic heart rate component differences appeared, none were found between participants with ADHD and controls. This lack of ADHD differences is not consistent with previous suggestions (Barkley 1997; Culbertson and Zillmer 1998) that planning is one of the marked executive function deficits in ADHD, although because triphasic heart rate differences did not appear consistently across all measures, these findings appropriately fall into question.
It was surprising that in this paradigm, no differences emerged between participants with ADHD and controls for their proportions of correct answers, although differences did emerge based on problem difficulty level and when comparing children and adults. Barkley’s arguments would suggest that at least behavioral differences should be evident with a task that engages executive functioning. The only behavioral difference emerging in the current study was that adults with ADHD had a slightly longer reaction time for correct answers than controls, although this effect did not emerge for child participants. A number of studies using the TOL have similarly found no differences in main effects of performance between participants with ADHD and controls (Scheres et al. 2004; Houghton et al. 1999; Riccio et al. 2004; Wiers et al. 1998), all of which employ a physical wooden version of the task. One study, however, found poorer performance in children with ADHD (Culbertson and Zillmer 1998), although the authors allotted participants a maximum of 2 min to solve each TOL problem, perhaps giving sustained attention deficits in children with ADHD enough time to interfere with planning, problem solving ability, and visuo-spatial working memory. The current study allotted only 6 s for each problem, more carefully controlling for sustained attention deficits and giving a clearer picture of the other three executive functions. Some other studies have shown participants with ADHD performing with less accuracy on the Tower of Hanoi (TOH), a similar task to the TOL (Pennington et al. 1993; Aman et al. 1998), but others have not (Ozonoff and Jensen 1999).
Extending the scope of the TOL to ADHD, Barkley (1997) specifically cited three executive functions represented in his ADHD model that, he hints, may be sensitive to tower tasks like the TOL: working memory, problem solving, and planning. The current study’s behavioral data generally do not support these ADHD differences that should appear under Barkley’s (1997) theory. Just as many of the previous TOL studies on ADHD, the current study does not support the aspect of the theory that adds working memory, problem solving, and planning into the group of executive functioning deficits in ADHD.
Heart rate results and ADHD
The current study takes the previous TOL behavioral research on ADHD a step further by adding the assessment of the triphasic heart rate components. And as with most of the behavioral data reported here, there were no main effects in the individual triphasic heart rate components during the TOL for participants with ADHD. Though these differences did not appear, there were main effects in A component latency for difficulty level in adults, as well as main effects in the D2 component amplitude for age category in both children and adults. The presence of these age category and difficulty main effects shows that the individual heart rate components cannot be viewed simply as insensitive to either cognitive or group variables during the TOL. The fact that ADHD differences were not evident may mean that the effects either are not present, or are smaller than those of difficulty level and age.
Previous heart rate research on ADHD has found that children with inattention problems exhibited significantly less heart rate deceleration before a reaction stimulus (Sroufe et al. 1973; Zahn et al. 1978). Both of these studies used simple reaction stimuli at S1 and S2 (either a tone or a light) and required participants to either flip a switch or release a button at S2 after a 5-s ISI. The paradigms of these two studies only tapped inhibition and attention, as participants had to refrain from an early response and wait attentively for the onset of S2. The current study’s paradigm, however, most strongly tapped planning, problem solving, visuo-spatial working memory, and—probably to a lesser degree—inhibition. The current finding of no differences for participants with ADHD in D2 amplitude generally falls in line with the larger body of literature questioning whether planning is a marked deficit in ADHD.
Interpretations of heart rate results for difficulty levels and age
A amplitude
There were no significant main effects for A amplitude. This was one of the more surprising findings in the study, because A amplitude has been found to be larger with increasing task difficulty (Walter and Porges 1976; Dennis and Mulcahy 1980) and in children than in adults (Anthony and Putnam 1982; Lawler et al. 1978; Byrd and Berg 2002). This lack of significance perhaps suggests that the current paradigm was not sensitive enough to measure A amplitude, perhaps because of the extreme complexity of executive function requirements needed to solve TOL problems.
A latency
Unlike A amplitude, main effects for A latency were found, and A latency decreased for problem difficulty in adults. A possible explanation is that for the more difficult problems, adults had to more fully engage their executive functions sooner. When they saw more difficult problems, they possibly knew they would have to put in the extra effort immediately, resulting in an earlier A peak.
D2 amplitude
Similarly to A latency, strong effects also appeared for D2 amplitude. For adults, a quadratic pattern appeared across difficulty level, showing that D2 amplitude decreased with increasing problem difficulty until the 4-move problems, when it increased. Since D2 is thought to reflect preparation for a motor response (Putnam 1990; Koers et al. 1997), a plausible interpretation is that adults had to spend progressively more time working on the 0-, 2-, and then 3-move problems and less time focusing on the motor response required at S2. When they performed 4-move problems, however, the adults had a harder time solving them and possibly focused in anticipation on the S2, not wanting it to come because they needed more time, or perhaps they gave up on these problems early on thinking them too difficult to solve.
Limitations and future directions
Though several heart rate results for A latency and D2 amplitude were significantly different among age categories and problem difficulties, many were not. For example, adults showed differences in D2 amplitude for problem difficulty, while children did not. Since the individual triphasic heart rate component findings were not consistent, the sensitivity of HR measures in this paradigm falls into question. Similarly, since no differences in A or D2 appeared between participants with ADHD and controls, this paradigm may not be sensitive enough to pick up those differences if they actually exist. With respect to these debatable sensitivities, this study does not concretely refute the aspect of Barkley’s (1997) unified executive functioning theory of ADHD that includes planning, visuo-spatial working memory, and problem solving as ADHD deficits. However, the study does raise suspicions in this regard and highlight the need for more psychophysiological research on executive functions in ADHD.
One study (Borger et al. 1999) examined HRV in children with ADHD using a continuous performance task and found the ADHD group to exhibit a greater 0.10-Hz component than controls. Typically, HRV involves examining heart rate over longer epochs than triphasic heart rate, the type used in the current paradigm. Since in the current study, participants only solved the TOL for 6 s epochs, sustained attention deficits were unlikely to interfere with problem solving. An HRV paradigm would have participants solve the TOL for 20 s or more, allowing sustained attention deficits typical of ADHD to play a greater role in problem solving.
In the current paradigm, after each TOL problem, participants received feedback on their performance, which could have confounded individual differences in feedback processing (based on the potential for different error rates) and influence motivation and performance in subsequent trials and blocks. Future studies should therefore manipulate whether participants receive feedback on their performance and examine its effects on performance. Additionally, it would be fruitful for future research to employ various executive function tasks during heart rate recording to determine whether multiple types of sustained executive functions (e.g., Willcutt et al. 2005) show differences in individuals with ADHD on sustained attention tasks with different designs.
Barkley and Murphy (2011) cite some concerns about executive functioning and its measurement. Executive functioning tests can be heavily influenced by intelligence, and Barkley and Murphy (2011) further report that some researchers have suggested that ADHD may not be a disorder of executive functioning, as executive functioning deficits appear to be apparent in only a minority of those with ADHD (Biederman et al. 2006; Willcutt et al. 2005). As for the measurement of executive functioning, Barkley and Murphy (2011) state that executive functioning tests have questionable ecological validity, because executive functioning tests correlate poorly with self-report ratings of executive functioning activities in everyday life. Despite these limitations to this study, the current findings contribute to the dialogue on whether executive dysfunction truly is one of the hallmark deficits of ADHD.
References
Altgassen M, Kretschmer A, Kliegel M (2012) Task dissociation in prospective memory performance in individuals with attention deficit hyperactivity disorder. J Atten Disord (epub ahead of print)
Aman CJ, Roberts RJ, Pennington BF (1998) A neuropsychological examination of the underlying deficit in attention deficit hyperactivity disorder: frontal lobe versus right parietal lobe theories. Dev Psychol 34:956–969
Anthony BJ, Putnam LE (1982) Cardiac and blink reflex concomitants of attentional selectivity: a comparison of adults and young children. Psychophysiology 22:508–516
Barkley RA (1997) Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull 121:65–94
Barkley RA, Murphy KR (2011) The nature of executive function (EF) deficits in daily life activities in adults with ADHD and their relationship to performance on EF tests. J Psychopathol Behav Assess 33:137–158
Berg WK, Byrd D (2002) The Tower of London spatial problem-solving task: enhancing clinical and research implementation. J Clin Exp Neuropsychol 24:586–604
Berg WK, Byrd DL (2009) Examining cognitive development using psychophysiological correlates: evidence of a hierarchy of future-oriented processes across measures. In: Schmidt LA, Segalowitz SJ (eds) Developmental psychophysiology: theory, systems, and applications. Cambridge University Press, New York
Berlin L, Bohlin G, Nyberg L, Janols L (2004) How well do measures of inhibition and other executive functions discriminate between children with ADHD and controls? Child Neuropsychol 10:1–13
Biederman J, Petty C, Fried R, Fontanella J, Doyle AE, Seidman L et al (2006) Impact of psychometrically defined deficits of executive functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 163:1730–1738
Bohlin G, Kjellberg A (1979) Orienting activity in two-stimulus paradigms as reflected in heart rate. In: Kimmel HD, van Olst EH, Orlebeke JF (eds) The orienting reflex in humans. Lawrence Erlbaum Associates, Hillsdale, NJ, pp 169–197
Borger N, van der Meere J, Ronner A, Alberts E, Geuze R, Bogte H (1999) Heart rate variability and sustained attention in ADHD children. J Abnorm Child Psychol 27:25–33
Brown TE (1996) Brown attention-deficit disorder scales: manual. The Psychological Corporation, San Antonio, TX
Byrd DL, Berg WK (2002) Developmental differences in the preparatory heart rate response: childhood through adulthood. Biol Psychol 61:271–276
Coles MGH, Duncan-Johnson CC (1975) Cardiac activity and information processing: the effects of stimulus significance and detection and response requirements. J Exp Psychol Hum Percept Perform 1:418–428
Culbertson WC, Zillmer EA (1998) The Tower of LondonDX: a standardized approach to assessing executive functioning in Children. Arch Clin Neuropsychol 13:285–301
Dennis SS, Mulcahy RF (1980) Heart-rate changes during covert rehearsal and response execution. Percept Mot Skills 50:595–602
Desjardins C, Scherzer P, Braun CMJ, Godbout L, Poissant H (2010) A verbal planning impairment in adult ADHD indexed by script generation tasks. J Atten Disord 14:220–231
Fuermaier ABM, Tucha L, Koerts J, Aschenbrenner S, Westermann C, Weisbrod M et al (2013) Complex prospective memory in adults with attention deficit hyperactivity disorder. PLoS ONE 8:e58338
Geller B, Zimerman B, Williams M, Bolhofner K, Craney JL, DelBello MP, Soutullo C (2001) Reliability of the Washington University in St Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-KSADS). J Am Acad Child Adolesc Psychiatry 40:450–455
Graham FK, Clifton RK (1966) Heart rate changes as a component of the orienting response. Psychol Bull 65:305–320
Griffin CJ, Davis LJ, Berg WK, Garner EE (1995) Anticipation in 3 and 5-yr-old children: cardiac responses while awaiting a cued, interesting event. Paper presented at the meeting of the Society for Research in Child Development. Indianapolis, IN
Houghton S, Douglas G, West J, Whiting K, Wall M, Langsford S, Powell L, Carroll A (1999) Differential patterns of executive function in children with attention-deficit hyperactivity disorder according to gender and subtype. J Child Neurol 14:801–805
Jennings JR, van der Molen MW, Pelham W, Debski KB, Hoza B (1997) Inhibition in boys with attention deficit hyperactivity disorder as indexed by heart rate change. Dev Psychol 33:308–318
Koers G, Gaillard AWK, Mulder G (1997) Evoked heart rate and blood pressure in an S1/S2 paradigm. Biol Psychol 46:247–274
Lacey JI (1959) Psychophysiological approaches to the evaluation of psychotherapeutic process and outcome. In: Rubinstein EA, Parloff MB (eds) Research in psychotherapy. American Psychological Association, Washington, DC, pp 160–208
Lacey JI, Lacey BC (1970) Some autonomic-central nervous system interrelationships. In: Black P (ed) Physiological correlates of emotion. Academic Press, New York
Lawler KA, Obrist PA, Lawler JE (1978) Cardiac and somatic response patterns during a reaction time task in children and adults. Psychophysiology 13:448–455
Lezak MD (1995) Neuropsychological assessment. Oxford University Press, New York
Ozonoff S, Jensen J (1999) Brief report: specific executive function profiles in three neurodevelopmental disorders. J Autism Dev Disord 29:171–177
Pennington BF, Groshier D, Welsh MC (1993) Contrasting cognitive deficits in attention deficit hyperactivity disorder versus reading disability. Dev Psychol 29:511–523
Porges SW (1984) Physiologic correlates of attention: a core process underlying learning disorders. Pediatr Clin North Am 31:371–385
Putnam LE (1990) Great expectations: anticipatory responses of the heart and brain. In: Rohrbaugh JW, Parasuraman R (eds) Event-related brain potentials: basic issues and applications. Oxford University Press, New York, pp 109–129
Riccio CA, Wolfe ME, Romine C, Davis B, Sullivan JR (2004) The Tower of London and neuropsychological assessment of ADHD in adults. Arch Clin Neuropsychol 19:661–671
Scheres A, Oosterlaan J, Geurts H, Morein-Zamir S, Meiran N, Schut H, Vlasveld L, Sergeant JA (2004) Executive functioning in boys with ADHD: primarily and inhibition deficit? Arch Clin Neuropsychol 19:569–594
Shallice T (1982) Specific impairments of planning. Philos Trans R Soc Lond Biol 298:199–209
Shallice T, Marzocchi GM, Coser S, Del Salvio M, Meuter RF, Rumiati RI (2002) Executive function profile of children with attention deficit hyperactivity disorder. Dev Neuropsychol 21:43–71
Simes RJ (1986) An improved Bonferroni procedure for multiple tests of significance. Biometrika 73:751–754
Sokolov EN (1963) Perception and the conditioned reflex. Macmillan, New York
Sroufe LA, Sonies BC, West WD, Wright FS (1973) Anticipatory heart rate deceleration and reaction time in children with and without referral for learning disability. Child Dev 44:267–273
Tucha L, Tucha O, Sontag TA, Stasik D, Laufkoetter R, Lange KW (2011) Differential effects of methylphenidate on problem solving in adults with ADHD. J Atten Disord 15:161–173
Unterrainer JM, Rahm B, Kaller CP, Leonhart R, Quiske K, Hoppe-Seyler K, Meier C, Müller C, Halsband U (2004) Planning abilities and the Tower of London: is this task measuring a discrete cognitive function? J Clin Exp Neuropsychol 26:846–856
Walter GF, Porges SW (1976) Heart rate and respiratory responses as a function of task difficulty: the use of discriminant analysis in the selection of psychologically sensitive physiological responses. Psychophysiology 13:563–571
Welsch MC, Satterlee-Cartmell T, Stine M (1999) Towers of Hanoi and London: contribution of working memory and inhibition to performance. Brain Cogn 41:231–242
Welsh MC, Pennington BF, Groisser DB (1991) A normative-developmental study of executive function: a window on prefrontal function in children. Dev Neuropsychol 7:131–149
Wiers RW, Gunning WB, Sergeant JA (1998) Is a deficit in executive functions in boys related to childhood ADHD or to parental multigenerational alcoholism? J Abnorm Child Psychol 26:415–430
Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF (2005) Validity of the executive function theory of attention deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry 57:1336–1346
Zahn TP, Little BC, Wender PH (1978) Pupillary and heart rate reactivity in children with minimal brain dysfunction. J Abnorm Child Psychol 6:135–147
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Perrin, P.B., Case, K.H., Byrd, D.L. et al. Executive functioning in attention-deficit/hyperactivity disorder: questioning the notion of planning deficits with heart rate reactivity. ADHD Atten Def Hyp Disord 6, 1–10 (2014). https://doi.org/10.1007/s12402-013-0118-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12402-013-0118-6