
Abstract
Extranodal NK/T-cell lymphoma (ENKTL), nasal type, is a rare type of non-Hodgkin lymphoma that is commonly seen in East Asian countries and is associated with Epstein-Barr virus infection. This is a retrospective study where we describe nine cases of ENKTL; nasal type diagnosed and treated at our center over a period of 2 years. These cases were analyzed retrospectively for clinical presentation (age, sex, site of involvement), immunophenotype, treatment, response and toxicity profile. Sino-nasal symptoms (blocked nose, headache, epistaxis, regurgitation) were the most common presenting complaints (n = 8). Almost 67 % (n = 6/9) of the cases were referred from Bhutan. Necrosis and angiocentricity were the commonest histological features. Depending on the stage of the disease patient were initially treated with chemotherapy (SMILE/CHOP) and Radiotherapy (IFRT). We describe our experience of management of ENKTL, where we observe that Bhutan could be endemic region for this rare tumour.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Extranodal NK/T-cell lymphoma (ENKTL), nasal type is a rare, very distinct type of lymphoproliferative disorder known to arise from the NK/T cells. Previously called as angiocentric lymphoma in the REAL classification, this disorder was renamed as NK/T cell lymphoma, nasal type in the WHO classification 2008. It has got a specific geographical predilection for Asian and South American populations where it may comprise 2–7 % of all non Hodgkin lymphomas [1–3]. This disease is known for its predominant involvement of the nasopharynx, strong association with Epstein–Barr virus (EBV) and caries a poor prognosis with a 5 year cumulative probability of survival ranging from 30 to 40 %. [4, 5] One of the postulated reasons is the high concentration of P-glycoprotein on natural killer (NK) cells which leads to multi-drug resistance, hence response to traditional anthracycline containing regimens is poor. Incorporation of drugs like L Asparginase which bypass the effect of P-glycoprotein has improved the outlook for this disease. Here we describe our experience in management of this disease.
Materials and Methods
This is a retrospective study carried out at our center over a period of 3 years from 2011 to 2014, and included 9 patients with histopathological diagnosis of NK/T-cell lymphoma. Data on clinical history, physical examination, performance status, baseline haematological and biochemical parameters, histology, imaging and bone marrow studies were collected from the computer database. The study included biopsy/excision material of patients registered within the hospital as well as those referred from outside. The cases were reviewed by two pathologists (NA/IA). Tissue was processed in 10 % formalin, and 4 μm paraffin sections were stained with hematoxylin and eosin (H & E). Immunohistochemistry (IHC) along with appropriate positive and negative controls was performed in all cases using a Ventana Benchmark XT auto-stainer with antibodies obtained mainly from Dako (Glostrup, Denmark). In situ hybridization for EBER was performed using a Ventana EBER-ISH detection kit on a Ventana Benchmark XT auto-stainer. Formalin fixed, paraffin-embedded tissue Sections (4 μ m) were floated on silane-coated slides and incubated at 60° C for 3–4 h. De-paraffinised slides were further processed in the Ventana auto-stainer, which included conditioning, treatment with Protease II for 8 min, application of an INRORM EBER probe and Blue Detection reagent, and counter staining with Ventana Red Stain II. A known EBVLMP1 positive lymphoma was used as positive control.
Treatment records were reviewed and the nature of treatment, duration, toxicity and nature of responses were collected and rates of complete remission, overall survival and progression free survival were calculated for this cohort. Response evaluation was done as per standard criteria. Toxicity has been documented as per Common Terminology Criteria for Adverse Events version 4.0. Progression was defined as the time at which a second line therapy was started or death due to any cause.
Results
Patients
A total of 09 patients were diagnosed with NK/T cell lymphoma over a 3 year period (Table 1) and included 5 females and 4 males. The median age of this cohort was 39 years (range 29–64 years). Six patients from this cohort were residents of Bhutan. The other three cases were of Indian ethnicity (West Bengal). Sino-nasal symptoms (blocked nose, headache, epistaxis, regurgitation) were the most common presenting complaints (n = 8). B symptoms were noted in over one-third of the patients (n = 4/9). An ulcerative, necrotic mass lesion in the nose and/or hard palate along with cervical lymphadenopathy was the commonest physical finding (n = 8/9). Haepatosplenomegaly was seen in a single case. Only two patients had poor performance status at presentation. Seven out of these 9 patients had elevated LDH, 3/9 patients had advanced stage disease (stage III/IV) and 2/9 patients had high IPI (>3). None of the patients had bone marrow involvement. The median follow up was 10 months (range 03–36 months).
Morphology/Immunophenotype
Morphologically, the neoplastic cells were predominantly medium sized in most cases. Ulceration (6/8), necrosis (7/8) and vascular invasion (4/8) were the common histopathologic findings (Table 1). All cases were positive for CD56 and CD3 except one case which was negative for CD3 (UPN1). This case was CD2+, CD56+, CD30 (focal and weak) positive and negative for CD20 and PAX5. EBER status of this case was not available for evaluation. Weak and focal CD30 expression was documented in all these cases. EBER-ISH/LMP1 was done in 6 patients and was positive in all 6 patients. The MIB proliferation index ranged from 40 to 90 %.
Treatment
Four out of nine patients received CHOP as the first line treatment (Table 2) and the rest received a regimen comprising Methotrexate, L-Asparginase and Etoposide (SMILE) as the first line therapy [6]. The median number of cycles received by patients was 6 (range 1–6) in the CHOP group and 3 (range 1–4) in the SMILE group. Additionally two patients received SMILE as salvage therapy. Five patients received further radiotherapy to the nasal primary with a median dose of 50.4 gy.
Response
Majority of patients on CHOP (N = 3/4) progressed on therapy, except one who achieved CR and continues to remain in CR after 34 months of follow up. Of these 3 progressive cases, 2 were salvaged with SMILE + radiotherapy while one was palliated due to poor general condition. The two patients who received salvage therapy achieved CR after 4 cycles of SMILE followed by radiotherapy.
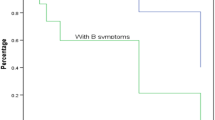
Amongst the five patients who received SMILE as first line therapy two achieved complete response, one died due to therapy related complications (gram negative sepsis), another had progressive disease and one patient had severe toxicity after the Ist cycle and hence could not receive further chemotherapy. The median overall survival (OS) and progression free survival (PFS) of this entire cohort was 10 months (range 03–36 months) and 5.5 months (range 01–34 months). The median PFS following therapy with SMILE was 9 months.
Toxicity
CHOP was generally well tolerated with no major haematologic or non haematologic toxicity. On the other hand, haematologic toxicity was ubiquitous following therapy with SMILE. All patients developed Grade IV neutropenia and 6/7 patients developed grade IV thrombocytopenia. Deep venous thrombosis was seen in two patients and in both these cases, this was related to central vascular access devices. There were no instances of pancreatitis or liver dysfunction in this cohort. There was one treatment related death in a patient who received SMILE (gram negative sepsis).
Discussion
NK/T-cell lymphoma is a distinct clinico-pathologic entity associated with EBV and is more commonly seen in Asian and South American populations.
An interesting observation from this series is the clustering of patients from region of Bhutan (n = 6/9, 66 %). Bhutan is a small landlocked country in south East Asia with a population of 776000 (Source: Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat, World Population Prospects: The 2012 Revision). There is no published data on epidemiology of lymphomas from Bhutan. NK/T cell lymphoma comprised 26 % (n = 6/23) of all cases of non-Hodgkin lymphomas in patients of Bhutanese ethnicity treated in our center. Of the only 2 large series comprising of 37 cases and 84 cases of ENKTCL described from India, only one study has actually documented the ethnicity of the patients with these neoplasms. Almost half of the cases in that study were from western India where as East India (West Bengal/Assam) constituted 20 % of the overall ENKTCL [7, 8].
NK/T cell lymphoma is a disease of young adults and most patients present with sino-nasal symptoms. A necrotic, ulcerating mass in the nasopharynx is the most common clinical finding which is similar our findings. Generalised lymphadenopathy and hepatosplenomegaly are usually features of disseminated disease. These cases were previously referred to as “non-nasal NK/T cell lymphoma”. However modern imaging with PET CT has shown that most if not all “non-nasal NK/T cell lymphomas” have an occult nasal primary. [9].
Histopathology of the tumour commonly shows angicentricity and angio-destruction leading to extensive necrosis and ulceration. The tumour cells have a cytotoxic T-cell phenotype and are for CD2, CD3, CD56 and EBV. However CD3 negative cases have been previously reported. [7] In this present series all cases were positive for CD56 and CD3 except one patient in whom CD3 was negative. EBER was positive in all cases wherever available.
Congruent with other studies, standard anthracycline based chemotherapy was ineffective in 3 out of 4 patients progressing on CHOP in this present series [10]. The median PFS following therapy with CHOP was 4.5 months (range 2–34 months). Patients treated with L-Asparginase based regimen showed better response with CR rate of 50 %. In patients with early stage disease the CR rate was better at 66 %. Patients with advanced disease (higher stage, high IPI) tended to do poorly irrespective of the modality of treatment. These figures are comparable with previously published studies on L-Asparaginase based therapy for NK/T cell lymphoma [11].
Haematologic complications are the most common toxicity associated with SMILE therapy and this usually requires dose reduction in subsequent cycles. The other reported toxicities include hepatotoxicity and pancreatitis, although none of the patients in this cohort developed these toxicities. L-Asparginase may induce a pro-coagulant state and result in thrombosis. This is particularly problematic as patients receiving treatment with SMILE often require central venous access devices.
NK/T cell lymphoma is a radio-sensitive disease. In initial studies, when used as the only treatment modality, complete responses were observed in 52–100 % of patients with a overall response rate between 77 and 100 %. [5, 12, 13] However the rates of systemic relapse were as high as 45 %. [5] Therefore it is not recommended to use radiotherapy alone in management of this disorder. Additionally the dose and radiation fields are important considerations. It is recommended to use at least 50 Gy over an extended field incorporating the para-nasal sinuses, nasopharynx and palate for optimum results [5, 12, 14].
In this series we describe our experience of management of a small series of ENKTL from eastern India. Our data suggests that Standard anthracycline based chemotherapy is ineffective and suggest that patients with limited stage disease be treated with combination chemotherapy with L-Asparginase based regimens along with radiotherapy to the nasal primary. In addition we observe that Bhutan could be endemic region for this rare tumour. This though is a first report of NK/T cell lymphoma in patients of Bhutanese origin and would require a large study to confirm these initial observations.
References
Au W-Y, Ma S-Y, Chim C-S, Choy C, Loong F, Lie AKW et al (2005) Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the world health organization classification scheme: a single center experience of 10 years. Ann Oncol 16(2):206–214
The world health organization classification of malignant lymphomas in japan: incidence of recently recognized entities. Lymphoma Study Group of Japanese Pathologists. Pathol Int. 2000 50(9):696–702
Arber DA, Weiss LM, Albújar PF, Chen YY, Jaffe ES (1993) Nasal lymphomas in Peru. High incidence of T-cell immunophenotype and Epstein-Barr virus infection. Am J Surg Pathol 17(4):392–399
Chim C-S, Ma S-Y, Au W-Y, Choy C, Lie AKW, Liang R et al (2004) Primary nasal natural killer cell lymphoma: long-term treatment outcome and relationship with the International Prognostic Index. Blood 103(1):216–221
Cheung MMC, Chan JKC, Lau W, Ngan RKC, Foo WWL (2002) Early stage nasal NK/T-cell lymphoma: clinical outcome, prognostic factors, and the effect of treatment modality. Int J Radiat Oncol Biol Phys 54(1):182–190
Yamaguchi M, Kwong Y-L, Kim WS, Maeda Y, Hashimoto C, Suh C et al (2011) Phase II study of SMILE chemotherapy for newly diagnosed stage IV, relapsed, or refractory extranodal natural killer (NK)/T-cell lymphoma, nasal type: the NK-cell tumor study group study. J Clin Oncol Off J Am Soc Clin Oncol. 29(33):4410–4416
Shet T, Suryawanshi P, Epari S, Sengar M, Rangarajan V, Menon H et al (2014) Extranodal natural killer/T cell lymphomas with extranasal disease in non-endemic regions are disseminated or have nasal primary: a study of 84 cases from India. Leuk Lymphoma 55(12):2748–2753
Bugalia A, Manipadam MT, Nair S (2013) Immunomorphologic profile and Epstein-Barr virus status of a cohort of 35 cases of extranodal natural killer/T-cell lymphoma, nasal type of upper aerodigestive tract from a tertiary care center in South India. Leuk Lymphoma 54(6):1201–1207
Khong P-L, Pang CBY, Liang R, Kwong Y-L, Au W-Y (2008) Fluorine-18 fluorodeoxyglucose positron emission tomography in mature T-cell and natural killer cell malignancies. Ann ≠Hematol 87(8):613–621
Kim WS, Song SY, Ahn YC, Ko YH, Baek CH, Kim DY et al (2001) CHOP followed by involved field radiation: is it optimal for localized nasal natural killer/T-cell lymphoma? Ann Oncol 12(3):349–352
Kwong Y-L, Kim WS, Lim ST, Kim SJ, Tang T, Tse E et al (2012) SMILE for natural killer/T-cell lymphoma: analysis of safety and efficacy from the Asia Lymphoma Study Group. Blood 120(15):2973–2980
Li Y-X, Yao B, Jin J, Wang W-H, Liu Y-P, Song Y-W et al (2006) Radiotherapy as primary treatment for stage IE and IIE nasal natural killer/T-cell lymphoma. J Clin Oncol Off J Am Soc Clin Oncol. 24(1):181–189
Wang Z-Y, Li Y-X, Wang W-H, Jin J, Wang H, Song Y-W et al (2009) Primary radiotherapy showed favorable outcome in treating extranodal nasal-type NK/T-cell lymphoma in children and adolescents. Blood 114(23):4771–4776
Koom WS, Chung EJ, Yang W-I, Shim SJ, Suh CO, Roh JK et al (2004) Angiocentric T-cell and NK/T-cell lymphomas: radiotherapeutic viewpoints. Int J Radiat Oncol Biol Phys 59(4):1127–1137
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest to declare.
Ethical standards
This is a retrospective studies, therefore for this type of study formal consent is not required.
Additional information
Presentation at a meeting: APCON 2014 AFMC, Pune.
Rights and permissions
About this article

Cite this article
Arora, N., Mehta, A., Ravichandran, S. et al. NK/T Cell Lymphoma: A Tertiary Centre Experience. Indian J Hematol Blood Transfus 33, 69–73 (2017). https://doi.org/10.1007/s12288-016-0675-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12288-016-0675-x