
Abstract
The endothelium covering the aortic, pulmonary, mitral, and tricuspid valves looks much like the endothelium throughout the vasculature, in terms of general morphology and expression of many endothelial markers. Closer examination, however, reveals important differences and hints of a unique phenotype that reflects the valvular endothelium's embryonic history, and potentially, its ability to maintain integrity and function over a life span of dynamic mechanical stress. A well-studied property that sets the cardiac valvular endothelium apart is the ability to transition from an endothelial to a mesenchymal phenotype—an event known as epithelial to mesenchymal transition (EMT). EMT is a critical step during embryonic valvulogenesis, it can occur in post-natal valves and has recently been implicated in the adaptive response of mitral valve leaflets exposed to a controlled in vivo setting designed to mimic the leaflet tethering that occurs in ischemic mitral regurgitation. In this review, we will discuss what is known about valvular endothelial cells, with a particular focus on post-natal, adult valves. We will put forth the idea that at subset of valvular endothelial cells are progenitor cells, which may serve to replenish valvular cells during normal cellular turnover and in response to injury and disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Phenotype of Cardiac Valve Endothelial Cells
The two most prominent cellular components of cardiac valves are the endothelial cells (VECs) and interstitial cells (VICs). The VECs reside along the entire surface of the cusps or leaflets and are in continuity with the endocardium, the aorta, and the pulmonary artery. The VICs make up the collection of mesenchymal cells that reside within specialized extracellular matrix (ECM) subcompartments—the fibrosa, spongiosa, and ventricularis/atrialis layers (Fig. 1). Lineage tracing studies using Tie2-cre x ROSA26R mice have shown that the VICs of all four cardiac valves and the supporting chordae tendineae arise from the endothelial cells of the endocardial cushions [1]—the structure from which the valves are formed during embryonic development. Using a similar approach to specifically label myocardial, neural crest, and endothelial populations, de Lange and colleagues also concluded that VICs are derived from endocardial endothelial cells [2]. The morphology and phenotype of the VICs has been reviewed recently [3]. The cells reside in sub-endothelial locations, dispersed throughout the specialized ECM layers of the valves, and are responsible for synthesizing and assembling the ECM of each of these layers.

Schematic of aortic and mitral valves
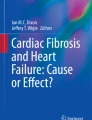
The morphologic features of heart valve endothelium have been examined in developing human, avian, and murine embryos, with a particular eye towards defining changes that occur with onset of hemodynamic forces. An extensive study of human aortic and pulmonary valves, with specimens ranging from 3 weeks gestation to 10 years of age, showed a progressive elongation and flattening of the VECs on the ventricular side of the cusps whereas VECs along the arterial side appeared cuboidal [4]. Figure 2 highlights this by immunostaining the endothelial cells in a fetal aortic valve section with anti-CD31; note elongated VECs on the ventricular side and cuboidal VECs on the aortic side. Hurle described similar side-specific morphology in avian and murine semilunar heart valves, and noted the presence of endothelial microvilli on the arterial side [5–7]. Viewed by both scanning and transmission electron microscopy, the authors observed cellular contacts between VECs and VICs and presence of extracellular collagen fibers but no sign of a basal lamina separating the endothelium from sub-endothelial VICs. This may ease the way for VECs as they undergo epithelial to mesenchymal transition (EMT) and migrate into the interstitium and perhaps for VEC–VIC communication. In a study of canine aortic valve samples, it was discovered unexpectedly that the endothelial cells are oriented circumferentially. This was observed even on the left ventricular surface, which is exposed to substantial shear stress during systole [8]. Porcine aortic valve ECs exposed to steady laminar shear stress in vitro were found to align perpendicular to the direction of flow (akin to the circumferential orientation in vivo), whereas aortic ECs aligned parallel to the direction of flow [9], indicating that the physiologic orientation can be re-established in vitro. At present, the physiologic significance of the side-specific cellular features is not known.

Elongated versus flattened endothelial morphology. Human fetal aortic valve section immunostained with anti-CD31 reveals elongated endothelial morphology along the ventricular side (V) and cuboidal morphology along the aortic side (A)
Several years later, the transcriptional profile of the ventricular versus aortic side was analyzed by isolating endothelium from each face of porcine aortic valves and immediately preparing RNA. The analysis revealed that the aortic side of the valve is relatively anti-oxidative but also pro-osteogenic, i.e., the presence of both protective and pathologic transcripts in a region prone to calcification and valve disease were found [10]. A similar study also reported a non-inflammatory phenotype for porcine aortic VECs in comparison to aortic ECs [11]. This was followed by experiments in which pigs were fed a high-cholesterol diet to promote aortic valve disease; the authors reported increased responsiveness on the aortic side endothelium compared to the ventricular side [12]. Going further, Sucosky and colleagues explanted porcine aortic valves into culture dishes, ventricular side up, or aortic side up, and then exposed the explants to normal or altered shear stress conditions. The ex vivo-applied altered hemodynamics caused increased expression of endothelial activation genes (VCAM-1, ICAM-1, BMP-4, and TGFβ1)—considered inflammatory markers—on the aortic face [13]. Interestingly, VCAM-1 is expressed during the development and maturation of human fetal valves, suggesting that altered hemodynamics re-activates a fetal phenotype [14]. In summary, the side-specific molecular profiles support the early insights from morphological studies on the cellular features observed on aortic and ventricular sides of the cusps.
Global gene expression analyses have shown that specific profiles persist even as endothelial cells are expanded in vitro [15]. For example, the intrinsic gene expression programs between large vessel and microvascular ECs, between arterial and venous, and among ECs from different tissue beds remain over many cellular population doublings. This provides reassurance that in vitro examination provides a sound approach for gaining insight into the cellular and molecular properties of VECs. VECs from porcine aortic valve specimens were studied as early as 1983 [16]; the cells were found to synthesize about 1/10th the level of fibronectin as found in aortic ECs. A follow-up study showed that both aortic and mitral valve ECs produced much less fibronectin when compared to ECs from several other sites, and thereby provided the first indication that gene/protein expression in VECs might be unique [17]. Another early study showed that human aortic and mitral VECs expressed high levels of major histocompatibility complex antigens, which suggested that the valvular endothelium is immunogenic [18].
EMT in Valvulogenesis
EMT is a required step in the formation of valves from the endocardial cushions. From the pioneering work of Markwald and colleagues in the mid-1970s [19, 20], we learned that a subset of endocardial cushion ECs detach from the endothelium, transiently upregulate the contractile protein α-smooth muscle actin (α-SMA) and migrate into the interstitium to populate the nascent valve with mesenchymal cells. Autoradiography of biosynthetic activity in the nascent valve revealed that the cushion mesenchymal cells begin produce and remodel extracellular matrix proteins. The transformation of endocardial VECs into mesenchyme is initiated in part by multiprotein complexes secreted by the mycocardium into the intervening space known as cardiac jelly [21, 22]. In addition, bone morphogenic protein (BMP)-2 was shown to be sufficient to initiate EMT in vitro in endocardial cushion explants, with subsequent in vivo studies providing strong support for BMP signals emanating from the myocardium, causing induction of TGFβ2 within the endocarium [23–25]. TGFβ was first reported to initiate EMT by Brown and colleagues [26]; species-specific preferences for different TGFβ family members, TGFβ1-3, have been well-documented and reviewed [27]. TGFβ signaling promotes endothelial activation, that is decrease in cell–cell contacts, induction of α-SMA, followed by migration of the activated cells into sub-endothelial space. Other pathways, for example, beta-catenin [28] and NOTCH signaling, are required for EMT in the endocardial cushions. NOTCH1 signaling increases Snail (pro-migration) and at the same time decreases VE-cadherin, thereby facilitating movement of endocardial VECs into the cushion mesenchyme [29]. Several excellent and comprehensive reviews of the cell biology and molecular regulation of EMT in cardiac cushions [27, 30, 31] will provide the reader with an appreciation for this burgeoning field of research, which has laid much ground work for studies on EMT in cancer and in fibrosis.
EMT in VECs
Studies of VECs were begun in our group as part of a multi-disciplinary effort to create tissue-engineered heart valves that could be used in place of bioprosthetic or mechanical valves. Our initial experience with aortic and pulmonary VECs isolated from healthy juvenile sheep was that the cells formed a typical cobblestone monolayer characteristic of ECs. However, the EC phenotype was not stable under the culture conditions we used: cells with mesenchymal morphology became prominent in the culture dish within 1–2 weeks. The morphologic changes were reminiscent of EMT or transdifferentiation during embryonic valvulogenesis described above and reviewed in [27].
To determine if the ovine aortic VECs we had isolated from juvenile sheep might retain the ability to undergo EMT, we first expanded clonal populations by plating single VECs in 96-well dishes in an endothelial medium that contained fetal bovine serum (10%) and basic fibroblast growth factor (bFGF) [32]. The homogenous cobblestone morphology of one expanded ovine aortic VEC clone is shown in Fig. 3. What is remarkable is that a single VEC was able to grow in isolation, without a feeder cell layer, to a confluent monolayer that could then be trypsinized and sub-cultured repeatedly, while maintaining an endothelial phenotype. This suggested robust self-renewal potential and provided the first hint of a “stem” or “progenitor” cell quality.

Ovine aortic VEC clone. Homogeneous cobblestone morphology, characteristic of endothelial cells, exhibited by ovine aortic VECs expanded from a single VEC [32]. Scale bar 50 μm
Nine clones of ovine aortic VECs were assayed for ability to undergo EMT [32]. Three were found to undergo EMT in response to TGF-β1; three were not induced by TGF-β1 but instead underwent EMT in response to removal of bFGF and serum from the endothelial growth medium. We assayed EMT primarily by induction of α-SMA but also other hallmarks of EMT: decreased expression of CD31, loss of cell–cell contacts, and increased cellular migration. Figure 4a depicts changes in phenotype indicative of EMT: note the co-expression of CD31/PECAM-1, an endothelial marker (red) and α-SMA (green) in individual cells in the right panel. Similar results were obtained with clonal populations from ovine pulmonary VECs (unpublished data). We also detected rare cells co-expressing endothelial and α-SMA in histological sections of ovine and human aortic valves [32]. We hypothesized in our 2001 publication that adult valvular endothelium contains a subset of progenitor-like cells capable of undergoing EMT and that their purpose is to replenish the VIC population on an as-needed basis. We extended our studies to human pulmonary VECs and found these cells were induced to undergo EMT specifically in response to TGFβ2 [33] (ovine VECs undergo EMT equally well in response TGFβs 1, 2, and 3). VEGF-A was found to oppose TGFβ-mediated EMT in some clones, while NOTCH1 was found to promote EMT downstream of TGFβ [33, 34] (Fig. 5), in agreement with in vivo murine studies [29]. We also analyzed co-expression of CD31 and α-SMA in paraffin sections from fetal and post-natal human semilunar valves [33]. Five to 10% of the CD31-positive cells in fetal valves were also positive for α-SMA, whereas the level dropped to approximately 1% in post-natal valves (Fig. 4b, c). This again suggested the presence of progenitor-like cells, residing in the valvular endothelium as bona fide endothelial cells that might serve to replenish VICs throughout life by re-activating an embryonic program for EMT.

Hallmarks of EMT: loss of cell–cell contacts, induction of α-SMA. a Ovine aortic VEC clone treated without (left) or with (right) TGFβ1 (1 ng/ml) for 5 days [32]. Cells were double-labeled with anti-CD31 (red) and anti-α-SMA (green). Cells co-expressing both markers appear yellow/orange. b EMT in fetal and adult semilunar valves [33]. Sections were double-labeled with anti-CD31 (green) and anti-α-SMA (red). Arrows indicate double-positive cells; inset in the lower right panel shows rare double-positive cells in adult valves. c Quantification of CD31+/α-SMA + cells in b: fetal valves from 14 to 19 weeks gestation, 10.8 ± 3.3% (n = 11); 20–39 weeks gestation, 5.6 ± 2.0%, (n = 10); and adult valves, 1.0 ± 0.5%, (n = 10)

Opposing actions of Notch1 and VEGF-A. Adapted from Yang et al. [34]
EMT in Ischemic Mitral Regurgitation
EMT in adult VECs prompted the formation of our collaboration with the Levine laboratory at the Massachusetts General Hospital to investigate whether EMT might be re-activated in ischemic mitral regurgitation (MR). In humans with ischemic MR, increased mitral valve leaflet area was discovered by Levine and colleagues. They proposed that the growth represents an adaptive mechanism to minimize or prevent MR [35]. To explore the mechanisms that underlie the apparent adaptation, Levine's group devised a surgical model, in sheep, to tether the mitral valve leaflets in a way that mimics the altered geometry imposed by ischemic MR, but without myocardial infarction or regurgitation [36]. This isolates the effects of tethering from effects of myocardial infarction and turbulent flow due to MR. Sheep were subjected to the surgical procedure to produce tethering and monitored to verify the absence of MR. After 2 months, leaflet size was measured by 3D echocardiography. MVs were then explanted for histopathological analyses and flow cytometry. As expected, there was little to no α-SMA detected in sham-operated MV sections, but a dramatic increase in α-SMA-positive cells was seen within the endothelium and interstitium in the tethered MVs (Fig. 6a). Notably, the morphology of the CD31+ cells along the endothelium was altered in the tethered MVs (Fig. 6b). Leaflet area and thickness were measured and found significantly increased, with a concomitant four-fold increase in endothelial cells undergoing EMT [36]. This was the first indication that a cellular process reminiscent of embryonic EMT could be activated in adult heart valves in a disease setting. Furthermore, the findings indicate that the plasticity observed in vitro with isolated VECs could occur in living functioning mitral valves.

Increased α-SMA in tethered MV. Ovine MV leaflets after 2 months of tethering [36] were immunostained for CD31 and α-SMA. α-SMA-positive cells extended into the interstitium and endothelial CD31 decreased consistent with loss of cell–cell contacts allowing migration
Mitral VECs with Osteogenic and Chondrogenic Differentiation Potential
Since developmental models of valvulogenesis and cell culture models have shown the VECs give rise to VICs, we asked whether VECs might be able to differentiate into VICs with specialized phenotypes that have been described: fibrosa VICs are bone-like; spongiosa VICs are cartilage-like; atrialis/ventricularis VICs are smooth muscle-like [37]. We used ovine mitral valve leaflets to prepare a primary culture of VECs, and subsequently isolated and analyzed eight different clonal populations of mitral VECs. Mitral VEC clones were tested for TGFβ1-induced EMT, as in previous studies, and for ability to undergo osteogenic, chondrogenic, or adipogenic differentiation using well-established in vitro protocols [38]. Five of the eight clones could be induced to express high levels of α-SMA after 5–6 days of exposure to TGFβ1, and three of these five could be induced to differentiate towards an osteogenic phenotype, as measured by loss of CD31 and onset of expression of osteocalcin, osteopontin, and osteonectin—all markers of bone cells [39]. Chondrogenic differentiation was also seen in two of the mitral VEC clones, measured by glycosaminoglycan accumulation, and collagen type 2a1 and Sox9 mRNA transcripts. Adipogenic differentiation was not observed in the mitral VEC clones in that cytoplasmic lipid droplets were not observed; however, a low level of PPARγ2 mRNA was detected. In contrast, we did not detect osteogenic or chondrogenic differentiation in four different normal ovine EC cultures: two EC clones from ovine carotid artery and two ECs isolated from ovine peripheral blood. (The arterial ECs and VECs are similar in phenotype in terms of cobblestone morphology, expression of endothelial markers such as CD31 and absence of α-SMA [39].) We also tested human umbilical cord blood-derived endothelial progenitor cells (EPCs) [40], which are also called endothelial colony forming cells (ECFCs) [41] and human microvascular endothelial cells isolated from newborn foreskin [42]. These experiments indicate a unique plasticity in subsets of valvular ECs. Furthermore, the results indicate that mitral VECs can differentiate into VICs with phenotypes that correlate with phenotypes described in the fibrosa and spongiosa layers of the valve. Evidence for osteogenic differentiation potential in vivo was seen in double-labeled mitral valve sections from tethered mitral valve leaflets from the Dal-Bianco study [36] described above. In tethered, but not control sham-operated mitral valves, focal regions of osteocalcin+/CD31+ endothelium were detected (Fig. 7). These focal regions of endothelium positive for osteocalcin correlate with the atrial changes, increased α-SMA and collagen deposition, seen in the tethered (i.e., stretched) mitral valves [36].

Focal regions of osteogenic endothelium in tethered mitral valves. Ovine MV leaflets after 2 months of tethering [36] were double-labeled with anti-osteocalcin and anti-CD31 (top panels) anti-α-SMA and anti-CD31 (middle panels) or with anti-α-SMA and anti-osteocalcin (bottom panels) [39]. Magnification ×400
VICs with Osteogenic Potential
Prior reports have clearly demonstrated that VICs have osteogenic differentiation potential and can become calcifying cells within aortic valves [43–46]. In our study described above, a clonal population of mitral VICs was studied in parallel with mitral VECs, and also found to have osteogenic, chondrogenic, and adipogenic differentiation potential [39], which may reflect their heritage. Using state-of-the-art molecular imaging, Aikawa and colleagues found evidence for endothelial activation (VCAM1) and osteogenic VICs (osteocalcin, osteopontin, osterix, Runx2/Cbfa/NOTCH1), but no calcium deposition in a model of aortic valve stenosis, and further suggested that these events enable the onset of disease [47]. The finding that mitral VEC clones can undergo EMT and have osteogenic and chondrogenic differentiation potential strongly suggests osteogenic VICs are progeny of the progenitor-like VECs. We speculate that disease, injury, or stress to the mitral valve may trigger progenitor-like VECs residing in the endothelium to undergo EMT, migrate into the interstitium, and undergo osteogenic differentiation, initially as part of pro-adaptive response. However, without the context of the molecular and environmental cues present during development, the adaptive processes may be inadequate and instead lead to fibrosis, stiffness, and sub-optimal function. Under steady-state conditions and perhaps even as a result of normal aging, we propose that EMT and further differentiation towards a VIC phenotype appropriate for a given location with the leaflet is needed to replenish the interstitium with healthy, robust cells that can synthesis the appropriate ECM and thereby maintain integrity and function of the valve over the life span of the organism.
EMT and Mesenchymal Plasticity in Non-Valvular Endothelium
EMT has been observed in cultured non-valvular endothelial cells as early as 1992 when Arciniegas and colleagues showed that TGFβ1 induced expression of smooth muscle markers in bovine aortic endothelial cells, and further showed that removal of TGFβ1 restored the endothelial phenotype [48]. Similar results were reported by Frid and colleagues in 2002 [49] and Ishisaki and colleagues in 2003 [50]. Frid found that only 0.01–0.03% of endothelial cells in the culture dish were able to undergo EMT, while Ishisaki found up to 8% of a clonal population of human umbilical vein ECs (HUVECs) co-expressed von Willebrand factor and calponin. This required 2 weeks of TGFβ-treatment after removal of fibroblast growth factor from the culture medium. This is consistent with our findings of little to no EMT in non-valvular cultures exposed to TGFβ for shorter time periods—typically 5–7 days [32, 33, 39]. An important caveat to keep in mind is that the details of the culture conditions are critical—factors such as VEGF-A, bFGF, BMP-7, or high serum can inhibit EMT. Although VEC EMT appears to be robust, it is not complete: approximately half of the VECs undergo EMT (see red only cells in Fig. 4a, right panel). This suggests that an equilibrium is reached, perhaps due to feedback from the nascent VICs. In summary, EMT that can be induced in microvascular or large vessel bovine or human ECs, but it appears to be very modest when compared to VECs.
However, clonally isolated prostate tumor endothelial cells have been shown to undergo robust EMT, and differentiation toward osteogenic and chondrogenic phenotypes [51]. Unlike MVECs that have differentiated towards an osteogenic phenotype, prostate tumor EC continue to co-express the endothelial marker CD31, which indicates the tumor ECs do not downregulate the endothelial program prior to or upon osteogenic differentiation. This difference could reflect the possibility that while mitral VEC differentiation towards osteogenic- and chondrogenic-like VICs represents a physiologic process, the osteogenic phenotype of prostate tumor endothelium represents an abnormality caused by the tumor environment.
A lineage tracing study in murine hearts showed a significant contribution of endothelial cells to the fibroblast population in fibrotic hearts. Up to 30% of the cardiac fibroblasts co-expressed the Tie1 promoter driven β-galactosidase [52, 53]. Interestingly, bone morphogenic protein-7 (BMP-7) was shown to effectively reverse the EndMT [52]. (Note: To distinguish endothelial to mesenchymal transition from the more general term epithelial to mesenchymal transition (i.e., EMT), the authors use the term EndMT.) More recently, EndMT has been shown to contribute to the heterotopic ossification caused by activating mutations in activin-like kinase 2 (ALK2) receptor in fibrodysplasia ossificans progressive (FOP) [54]. In human FOP samples and in a murine transgenic model in which mutant ALK2 is expressed, chondrocytes and osteoblasts co-expressing endothelial markers were detected. Furthermore, human ECs were shown to revert to a “stem cell-like” phenotype when expressing the ALK2 mutation in that the cells exhibited osteogenic, chondrogenic, and adipogenic differentiation potential. These three studies indicate that both in vivo and in the culture dish, the ability to undergo EMT may be a property of many types of endothelium.
Summary
Endothelial cells lining cardiac valves exhibit many of the same properties as endothelial cells from other sites in the vasculature, in particular when they are assayed for expression of typical endothelial markers and behaviors. Close examination, however, has revealed an essential distinction: VECs can recapitulate EMT, a critical event in embryonic valvulogenesis. EMT can be induced in vitro and is strongly increased in vivo in response to mechanical stretch, suggesting that EMT plays a role in adaptation to pathophysiologic conditions. The mesenchymal differentiation potential can be directed towards osteogenic and chondrogenic phenotypes, which we suggest reflects an ability to generate VICs that reside in specific regions of the valve. The multi-lineage differentiation potential of VECs combined with a robust capacity for self-renewal strongly suggests that at least a subset of VECs are progenitor cells. Such progenitor cells may be essential for health and longevity of the valve, and may also become activated during disease. Whether these cells can be harnessed or manipulated to prevent or limit valve disease will be an exciting direction for translational research.
References
Lincoln, J., Alfieri, C. M., & Yutzey, K. E. (2004). Development of heart valve leaflets and supporting apparatus in chicken and mouse embryos. Developmental Dynamics, 230, 239–250.
de Lange, F. J., Moorman, A. F., Anderson, R. H., Manner, J., Soufan, A. T., de Gier-de Vries, C., et al. (2004). Lineage and morphogenetic analysis of the cardiac valves. Circulation Research, 95, 645–654.
Liu, A. C., Joag, V. R., & Gotlieb, A. I. (2007). The emerging role of valve interstitial cell phenotypes in regulating heart valve pathobiology. American Journal of Pathology, 171, 1407–1418.
Maron, B. J., & Hutchins, G. M. (1974). The development of the semilunar valves in the human heart. American Journal of Pathology, 74, 331–344.
Hurle, J. M. (1979). Scanning and light microscope studies of the development of the chick embryo semilunar heart valves. Anatomy and Embryology, 157, 69–80.
Hurle, J. M., Colvee, E., & Blanco, A. M. (1980). Development of mouse semilunar valves. Anatomy and Embryology, 160, 83–91.
Hurle, J. M., & Colvee, E. (1983). Changes in the endothelial morphology of the developing semilunar heart valves. A tem and sem study in the chick. Anatomy and Embryology, 167, 67–83.
Deck, J. D. (1986). Endothelial cell orientation on aortic valve leaflets. Cardiovascular Research, 20, 760–767.
Butcher, J. T., Penrod, A. M., Garcia, A. J., & Nerem, R. M. (2004). Unique morphology and focal adhesion development of valvular endothelial cells in static and fluid flow environments. Arteriosclerosis, Thrombosis, and Vascular Biology, 24, 1429–1434.
Simmons, C. A., Grant, G. R., Manduchi, E., & Davies, P. F. (2005). Spatial heterogeneity of endothelial phenotypes correlates with side-specific vulnerability to calcification in normal porcine aortic valves. Circulation Research, 96, 792–799.
Butcher, J. T., Tressel, S., Johnson, T., Turner, D., Sorescu, G., Jo, H., et al. (2006). Transcriptional profiles of valvular and vascular endothelial cells reveal phenotypic differences: influence of shear stress. Arteriosclerosis, Thrombosis, and Vascular Biology, 26, 69–77.
Guerraty, M. A., Grant, G. R., Karanian, J. W., Chiesa, O. A., Pritchard, W. F., & Davies, P. F. (2010). Hypercholesterolemia induces side-specific phenotypic changes and peroxisome proliferator-activated receptor-gamma pathway activation in swine aortic valve endothelium. Arteriosclerosis, Thrombosis, and Vascular Biology, 30, 225–231.
Sucosky, P., Balachandran, K., Elhammali, A., Jo, H., & Yoganathan, A. P. (2009). Altered shear stress stimulates upregulation of endothelial vcam-1 and icam-1 in a bmp-4- and tgf-beta1-dependent pathway. Arteriosclerosis, Thrombosis, and Vascular Biology, 29, 254–260.
Aikawa, E., Whittaker, P., Farber, M., Mendelson, K., Padera, R. F., Aikawa, M., et al. (2006). Human semilunar cardiac valve remodeling by activated cells from fetus to adult: Implications for postnatal adaptation, pathology, and tissue engineering. Circulation, 113, 1344–1352.
Chi, J. T., Chang, H. Y., Haraldsen, G., Jahnsen, F. L., Troyanskaya, O. G., Chang, D. S., et al. (2003). Endothelial cell diversity revealed by global expression profiling. Proceedings of the National Academy of Sciences of the United States of America, 100, 10623–10628.
Johnson, C. M., & Fass, D. N. (1983). Porcine cardiac valvular endothelial cells in culture. A relative deficiency of fibronectin synthesis in vitro. Laboratory Investigation, 49, 589–598.
Johnson, C. M., & Helgeson, S. C. (1993). Fibronectin biosynthesis and cell-surface expression by cardiac and non-cardiac endothelial cells. American Journal of Pathology, 142, 1401–1408.
Simon, A., Zavazava, N., Sievers, H. H., & Muller-Ruchholtz, W. (1993). In vitro cultivation and immunogenicity of human cardiac valve endothelium. Journal of Cardiac Surgery, 8, 656–665.
Markwald, R. R., Fitzharris, T. P., & Manasek, F. J. (1977). Structural development of endocardial cushions. The American Journal of Anatomy, 148, 85–119.
Markwald, R. R., Fitzharris, T. P., & Smith, W. N. (1975). Structural analysis of endocardial cytodifferentiation. Developmental Biology, 42, 160–180.
Krug, E. L., Runyan, R. B., & Markwald, R. R. (1985). Protein extracts from early embryonic hearts initiate cardiac endothelial cytodifferentiation. Developmental Biology, 112, 414–426.
Markwald, R., Eisenberg, C., Eisenberg, L., Trusk, T., & Sugi, Y. (1996). Epithelial-mesenchymal transformations in early avian heart development. Acta Anatomica, 156, 173–186.
Sugi, Y., Yamamura, H., Okagawa, H., & Markwald, R. R. (2004). Bone morphogenetic protein-2 can mediate myocardial regulation of atrioventricular cushion mesenchymal cell formation in mice. Developmental Biology, 269, 505–518.
Ma, L., Lu, M. F., Schwartz, R. J., & Martin, J. F. (2005). Bmp2 is essential for cardiac cushion epithelial-mesenchymal transition and myocardial patterning. Development, 132, 5601–5611.
Rivera-Feliciano, J., & Tabin, C. J. (2006). Bmp2 instructs cardiac progenitors to form the heart-valve-inducing field. Developmental Biology, 295, 580–588.
Brown, C. B., Boyer, A. S., Runyan, R. B., & Barnett, J. V. (1996). Antibodies to the type ii tgfbeta receptor block cell activation and migration during atrioventricular cushion transformation in the heart. Developmental Biology, 174, 248–257.
Person, A. D., Klewer, S. E., & Runyan, R. B. (2005). Cell biology of cardiac cushion development. International Review of Cytology, 243, 287–335.
Liebner, S., Cattelino, A., Gallini, R., Rudini, N., Iurlaro, M., Piccolo, S., et al. (2004). Beta-catenin is required for endothelial-mesenchymal transformation during heart cushion development in the mouse. The Journal of Cell Biology, 166, 359–367.
Timmerman, L. A., Grego-Bessa, J., Raya, A., Bertran, E., Perez-Pomares, J. M., Diez, J., et al. (2004). Notch promotes epithelial-mesenchymal transition during cardiac development and oncogenic transformation. Genes & Development, 18, 99–115.
Combs, M. D., & Yutzey, K. E. (2009). Heart valve development: regulatory networks in development and disease. Circulation Research, 105, 408–421.
Lincoln, J., & Yutzey, K. E. (2011). Molecular and developmental mechanisms of congenital heart valve disease. Birth Defects Research. Part A, Clinical and Molecular Teratology, 91, 526–534.
Paranya, G., Vineberg, S., Dvorin, E., Kaushal, S., Roth, S. J., Rabkin, E., et al. (2001). Aortic valve endothelial cells undergo transforming growth factor-beta-mediated and non-transforming growth factor-beta-mediated transdifferentiation in vitro. American Journal of Pathology, 159, 1335–1343.
Paruchuri, S., Yang, J. H., Aikawa, E., Melero-Martin, J. M., Khan, Z. A., Loukogeorgakis, S., et al. (2006). Human pulmonary valve progenitor cells exhibit endothelial/mesenchymal plasticity in response to vascular endothelial growth factor-a and transforming growth factor-beta2. Circulation Research, 99, 861–869.
Yang, J. H., Wylie-Sears, J., & Bischoff, J. (2008). Opposing actions of notch1 and vegf in post-natal cardiac valve endothelial cells. Biochemical and Biophysical Research Communications, 374, 512–516.
Chaput, M., Handschumacher, M. D., Tournoux, F., Hua, L., Guerrero, J. L., Vlahakes, G. J., et al. (2008). Mitral leaflet adaptation to ventricular remodeling: occurrence and adequacy in patients with functional mitral regurgitation. Circulation, 118, 845–852.
Dal-Bianco, J. P., Aikawa, E., Bischoff, J., Guerrero, J. L., Handschumacher, M. D., Sullivan, S., et al. (2009). Active adaptation of the tethered mitral valve: Insights into a compensatory mechanism for functional mitral regurgitation. Circulation, 120, 334–342.
Lincoln, J., Lange, A. W., & Yutzey, K. E. (2006). Hearts and bones: shared regulatory mechanisms in heart valve, cartilage, tendon, and bone development. Developmental Biology, 294, 292–302.
Pittenger, M. F., Mackay, A. M., Beck, S. C., Jaiswal, R. K., Douglas, R., Mosca, J. D., et al. (1999). Multilineage potential of adult human mesenchymal stem cells. Science, 284, 143–147.
Wylie-Sears, J., Aikawa, E., Levine, R. A., Yang, J. H., & Bischoff, J. (2011). Mitral valve endothelial cells with osteogenic differentiation potential. Arteriosclerosis, Thrombosis, and Vascular Biology, 31, 598–607.
Melero-Martin, J. M., Khan, Z. A., Picard, A., Wu, X., Paruchuri, S., & Bischoff, J. (2007). In vivo vasculogenic potential of human blood-derived endothelial progenitor cells. Blood, 109, 4761–4768.
Ingram, D. A., Mead, L. E., Tanaka, H., Meade, V., Fenoglio, A., Mortell, K., et al. (2004). Identification of a novel hierarchy of endothelial progenitor cells using human peripheral and umbilical cord blood. Blood, 104, 2752–2760.
Kraling, B. M., & Bischoff, J. (1998). A simplified method for growth of human microvascular endothelial cells results in decreased senescence and continued responsiveness to cytokines and growth factors. In Vitro Cellular & Developmental Biology–Animal, 34, 308–315.
Rajamannan, N. M., Subramaniam, M., Rickard, D., Stock, S. R., Donovan, J., Springett, M., et al. (2003). Human aortic valve calcification is associated with an osteoblast phenotype. Circulation, 107, 2181–2184.
Chen, J. H., Yip, C. Y., Sone, E. D., & Simmons, C. A. (2009). Identification and characterization of aortic valve mesenchymal progenitor cells with robust osteogenic calcification potential. American Journal of Pathology, 174, 1109–1119.
Osman, L., Yacoub, M. H., Latif, N., Amrani, M., & Chester, A. H. (2006). Role of human valve interstitial cells in valve calcification and their response to atorvastatin. Circulation, 114, I547–552.
Bouchard-Martel, J., Roussel, E., Drolet, M. C., Arsenault, M., & Couet, J. (2009). Interstitial cells from left-sided heart valves display more calcification potential than from right-sided valves: an in-vitro study of porcine valves. The Journal of Heart Valve Disease, 18, 421–428.
Aikawa, E., Nahrendorf, M., Sosnovik, D., Lok, V. M., Jaffer, F. A., Aikawa, M., et al. (2007). Multimodality molecular imaging identifies proteolytic and osteogenic activities in early aortic valve disease. Circulation, 115, 377–386.
Arciniegas, E., Sutton, A. B., Allen, T. D., & Schor, A. M. (1992). Transforming growth factor beta 1 promotes the differentiation of endothelial cells into smooth muscle-like cells in vitro. Journal of Cell Science, 103(Pt 2), 521–529.
Frid, M. G., Kale, V. A., & Stenmark, K. R. (2002). Mature vascular endothelium can give rise to smooth muscle cells via endothelial-mesenchymal transdifferentiation: in vitro analysis. Circulation Research, 90, 1189–1196.
Ishisaki, A., Hayashi, H., Li, A. J., & Imamura, T. (2003). Human umbilical vein endothelium-derived cells retain potential to differentiate into smooth muscle-like cells. Journal of Biological Chemistry, 278, 1303–1309.
Dudley, A. C., Khan, Z. A., Shih, S. C., Kang, S. Y., Zwaans, B. M., Bischoff, J., et al. (2008). Calcification of multipotent prostate tumor endothelium. Cancer Cell, 14, 201–211.
Zeisberg, E. M., Tarnavski, O., Zeisberg, M., Dorfman, A. L., McMullen, J. R., Gustafsson, E., et al. (2007). Endothelial-to-mesenchymal transition contributes to cardiac fibrosis. Nature Medicine, 13, 952–961.
Zeisberg, E. M., & Kalluri, R. (2010). Origins of cardiac fibroblasts. Circulation Research, 107, 1304–1312.
Medici, D., Shore, E. M., Lounev, V. Y., Kaplan, F. S., Kalluri, R., & Olsen, B. R. (2010). Conversion of vascular endothelial cells into multipotent stem-like cells. Nature Medicine, 16, 1400–1406.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bischoff, J., Aikawa, E. Progenitor Cells Confer Plasticity to Cardiac Valve Endothelium. J. of Cardiovasc. Trans. Res. 4, 710–719 (2011). https://doi.org/10.1007/s12265-011-9312-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-011-9312-0