
Abstract
Reconstruction of finger contractures is a challenge for the plastic surgeon. It is important to restore the length, function, along with providing a good quality skin cover (Sridhar and Hariharan in Int J Sci Stud 5(2):55-58, 2017). This study is aimed to show use of square flap in finger contractures along with determining its functional outcome. Three cases of finger contractures were reconstructed between May 2020 and December 2020 in a tertiary care hospital in north India. Departmental clearance was done. Written informed consent was taken. Results were analyzed as per successful reconstruction, type of reconstruction and stages, complications, and functional outcome. The surgical outcome has shown improvement in overall function. Square flap has proven to be a useful flap in post-burn/trauma finger reconstruction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hands are a mirror image of mental health of a person. Hands are involved in more than 80% of severe burns/trauma. Each hand is < 2–3% of the total body surface area. Hand burns are considered as major burns [1].
In the treatment of burned hand, along with a multidisciplinary approach, early excision and grafting followed by early initiation of physical therapy, splinting, and exercises are indicated to minimize finger contractures [2].
Post-burn deformities occur even in a well-managed case and remain the most common cause of finger contractures [3]. Reconstruction of finger contractures is a challenge for the plastic surgeon. It is important to restore the length, function, along with providing a good quality skin cover [4].
Numerous methods have been suggested by various authors for surgical management of contractures at axilla, elbow, and fingers: skin grafting; Z-plasty, Y-V plasty, and their modifications; other local-flap plasty’s; fasciocutaneous and musculocutaneous pedicled, and free flaps.
This study is aimed to show use of square flap in finger contracture along with determining its functional outcome.
Patients and Methods
Three cases of finger contractures were reconstructed between May 2020 and December 2020 in a tertiary care hospital in north India. Departmental clearance was done. Written informed consent was taken. Patients with either post-burns of traumatic contractures involving single digit were chosen.
All the flaps were done under tourniquet guidance and local anesthesia/brachial block by resident surgeons. Average time taken was 40–50 min.
Along the line of contracture, the square is designed on the side from where the tissue is pliable and can be advanced with ease. On the other side, two triangular flaps are marked. Angles are kept 45° for the 1st one and 90° for the second one. All the limb lengths of square and triangular flaps kept equal (Fig. 1).

Line diagram
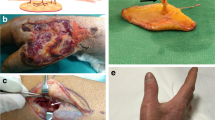
Incisions made along the marked line and the contracture are released up to permissible limit. Three flaps are elevated. Tourniquets are released where applied. Square flap is then advanced across the previous contracture line; the two triangular flaps are transposed and sutured on either side of the square flap, where the raw area was more additional split thickness skin graft used to cover the defect. Dressing of the wound done according to our hospital protocol (Image 1).

Case 1
Sutures were removed after complete healing at 10–14 days. Postoperative splint was given for 14–21 days. Pressure garments advised for 3–6 months to soften the scar and to reduce possibility of scar hypertrophy. Any postoperative complications were noted and managed accordingly. Regular physiotherapy was started postoperatively. Follow up visits were scheduled for minimum period of 6 months and range of motion and pre- and postoperative photographs were taken. Patient and surgeon satisfaction was recorded (Image 2).

Follow up picture of case 1
Results
There were total three cases of contracture of finger. There were two gentlemen and one lady. Two of the patients were below 20 years of age. Two cases were post traumatic and one case was post-burn finger contracture.
All patients underwent release with square flap. Two patients required Split Skin grafting. There were no complications.
There was an overall improvement in range of motion in postoperative follow up. The patients were followed up for 6 months (Table 1).
Discussion
The square flap is a type of local flap that is appropriate for the surgical release of a single linear band contracture at various locations that have adjacent healthy tissue [5]. The original design of the square flap had a square and two adjacent triangular flaps that are at an acute angle. This design was later modified in 1987. The author made one of the triangular flaps to a right angle flap which resulted in better lengthening [6].
In our study, we have used the square flap technique to release finger contractures. There were total three cases of contracture of fingers. There were two gentlemen and one lady patient. Two of the patients were below 20 years of age. Two cases were post traumatic and one case was post-burn finger contracture.
All the designed square flaps gave adequate lengthening of the contracture bands. Many local flap methods have been described previously in the literature for release of scar contractures of the finger. Z-plasty gives a good overall lengthening but large flaps are susceptible to more transverse tension. Modifications such as multiple Z-plasty in series, four-flap, five-flap, and seven flap Z-plasties provide suitable lengthening with lesser transverse tension [7].
Advantages of using the square flap in contracture release are that it creates a larger flap area to interpose a normal skin flap between the scarred burn flaps for optimal length gain. It is associated with the less physiological tension, which means that the deformity and the dependence on the laxity of the adjacent skin are minimal [8].
The square flap technique is a simple, easy technique which provides good lengthening, effective release of the contracture band with overall good cosmetic outcome [5]. It can be used in fingers, axilla, elbow, knee, etc.
The limitation of this study is the small number of patients and short follow up period. More cases and an extended follow up interval are required to confirm the efficacy of the square flap technique for the release of finger scar contractures.
Conclusions
The square flap technique is a simple, easy technique which provides good lengthening, effective release of the contracture band.
References
Hanumadass M, Kagan R, Matsuda T (1984) Early coverage of deep hand burns with groin flaps. J Trauma 27:109–114
Harnar T, Engrav L, Heimbach D, Marvin JA (1985) Experience with skeletal immobilization after excision and grafting of severely burned hands. J Trauma 25:299–302
Beasley RW (1990) Secondary repair of burned hands 1981. Hand Clin 6:319–341
Sridhar R, Hariharan NC (2017) Reconstruction of post-burn contracture of fingers. Int J Sci Stud 5(2):55–58
Hifny MA (2018) The square flap technique for burn contractures: clinical experience and analysis of length gain. Ann Burns Fire Disasters 31(4):306–312
Hyakusoku H, Fumiiri M (1987) The square flap method. Br J Plast Surg 40:40–46
Sison-Williamson M, Bagley A, Palmieri T (2012) Long-term postoperative outcomes after axillary contracture release in children with burns. J Burn Care Res 33:228–234
Huang C, Ogawa R (2014) Three-dimensional reconstruction of scar contracture-bearing axilla and digital webs using the square flap method. Plas Reconstr Surg Glob Open 2:e149
Author information
Authors and Affiliations
Contributions
All authors contributed equally to the case.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bharat, S.S., Jain, A., Mishra, A. et al. Role of Square Flaps in Finger Contractures. Indian J Surg 84, 345–348 (2022). https://doi.org/10.1007/s12262-021-02898-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-021-02898-9