
Abstract
The effects of family structure on children’s health behaviour have already been explored in the literature. However, few studies have considered also sets of some of the more important family characteristics, so that doubt as to exactly whether family structure influences children’s health behaviour still remains. In this study, we examined the effects of family structure on adolescents’ health behaviour in Italy by also taking into account other family factors such as parental behaviour, economic well-being, and family satisfaction. Data were drawn from the survey “Aspects of Daily Life” carried out by the Italian Statistical Institute (ISTAT). In this work, we use data from the 2005–2009 rounds of this survey, focusing on the sub-sample of adolescents aged 14–17. Four types of health behaviour were considered: cigarette smoking, consumption of alcohol, sports and physical activity, and consumption of fruit and vegetables. Results show the effect of family structure, but for some types of health behaviour this effect is confounded by other family characteristics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Adolescence is a critical period for the onset or formation of various types of health behaviour, and most of the decisions about them are made within the family, since the family unit is one of the main environmental factors in children’s growth and development. However, higher rates of divorce (González-Val and Marcén 2012) and having children outside marriage (Klüsener et al. 2012) have considerably increased the diversity of children’s and adolescents’ families in recent years. In particular, decreasing numbers of adolescents reside in two-parent households with their married, biological parents, and growing numbers live in different types of families (e.g., unmarried biological parents, step-families, single-parent families) in many European countries (OECD 2009; Eurostat 2010; Iacovu and Skew 2011; van Poppel et al. 2013). This is also true of a country like Italy, which has only recently been undergoing a transition from traditional to new family forms. For example, according to the survey “Health Behaviour in School-aged Children” (HBSC, 2005/2006), 87 % of young adolescents (aged 11, 13 or 15) live with both their parents, but 9 % live with a single parent and 3 % with one biological parent and one step-parent (1 % reside with neither) (OECD 2009). Thus, if family structure affects children’s health behaviour, these recent trends may have several consequences in terms of adolescents’ health. Several studies have already examined the relationship between family structure and adolescents’ health-related behaviour, but our understanding of the reasons for this association is not completely clear (see the discussion in Broman et al. 2008).
In this paper, using data from a nation-wide representative Italian survey, we examined the effect of family structure, controlling for economic conditions, parental behaviour, and the quality of family relationships, in several types of children’s health behaviour. In particular, we examined the effects of family structure on four types of health behaviour in adolescents aged 14–17. Two represent at risk behaviour and are connected with substance use (cigarette smoking and alcohol consumption) and two healthy lifestyle behaviour (sports and physical activity and consumption of fruit and vegetables). Information on multiple types of health behaviour can lead to better understanding of the broad health consequences of the family structure.
We therefore aimed to answer to what extent the associations between family structure and adolescents’ health behaviour in Italy are confounded by other factors such as parental behaviour, household economic well-being, and family satisfaction.
2 Literature Review
2.1 Children’s Health Status vs Children’s Behaviour
In studying children’s well-being, it is difficult to decide precisely on what we should focus. Our choice lay between children’s health status, or their health behaviour (i.e., behaviour positively or negatively affecting their present and/or future health), and we chose the latter, for two main reasons. First, these types of behaviour are risk factors for many chronic illnesses later in life and may thus be considered precursors of disease (Sanchez et al. 2007; Tercyak and Tyc 2006). There is no doubt about the negative effects of adolescent smoking and alcohol consumption, but the relationship between physical activity and various aspects of health are also clearly established. Active lifestyles are often associated with better health and a higher quality of life in children (Hallal et al. 2006). Similarly, a large body of evidence indicates that the daily consumption of fruit and vegetables helps to promote health and prevent chronic disease (Reddy and Katan 2004). Second, risky health behaviour, such as cigarette smoking and alcohol abuse, often begins during adolescence (Green and Palfrey 2000) and continues into adulthood (Jefferis et al. 2004; Hu et al. 2006). The same is true of a healthy or unhealthy lifestyle (Lien et al. 2001; Mikkilä et al. 2004; Telama et al. 2005): sedentary behaviour and poor dietary habits which developed during adolescence often form the basis for the same habits in adulthood.
2.2 How Family Structure Affects Children’s Well-Being
The family has been identified as a crucial context for the development of children’s and adolescents’ well-being, as it is the primary environment during children’s growth and development (Tinsley 2003).
The effect of family structure on children’s well-being has been extensively studied, and the association appears to be strong (McLanahan 2009). For example, it has been shown that children who live with both their biological parents are less likely to experiment with at risk behaviour, such as substance use (including smoking, alcohol, and drug-taking) than children from single-parent families (Blum et al. 2000; Brown and Rinelli 2010; Duncan et al. 2002). Compared with those from both biological parent families, a significantly higher risk of substance use has also been observed in adolescents in step-families (Griesbach et al. 2003). Instead, results regarding healthy behaviour are less conclusive: for instance, adolescents in single-parent families are more likely to have unhealthy eating habits than those from two-parent families (Roos et al. 2001; Rasmussen et al. 2006; Stewart and Menning 2009), but studies on physical activity show mixed results (Gustafson and Rhodes 2006).
What is the mechanism that leads adolescents from two-biological-parent families to have healthier lifestyles than their peers living in other family structures? Different theories have been suggested by literature.
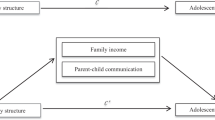
The first mechanism is connected with the fact that, from a resource perspective, living in some family forms is disadvantageous. Parental death or separation might, indeed, reduce financial, social, and time resources devoted to the child. These resources have an impact on children behaviours. For example, as regard socio-economic status (SES), single parents often have limited financial resources and live in more economically disadvantaged communities, where their children are more frequently exposed to negative social distractions (Manning and Brown 2006; Millar and Ridge 2001). Adolescents in families of low SES are found to be at greater risk of cigarette smoking (Sweeting and West 2001; Wardle et al. 2003), to have poorer nutritional habits (Xie et al. 2003) and to take less exercise (La Torre et al. 2006) than high-SES teenagers; results for alcohol consumption are mixed, as reported by Hanson and Chen (2007). Thus, changes in the economic resources connected with a transition to a new family form imply lower behavioural outcomes for children. A similar remark might hold for the level of supervision provided by family structure: the level of parental monitoring may be lower in single-parent families than in two-parent ones (Ledoux et al. 2002; Otten et al. 2007), and this, in turn, may have effects on children behaviours. In the case of step-families, the addition of an adult to the household can provide extra financial resources and time for monitoring, but the presence of a step-parent can also introduce more complex family relationships, conflicts, and stress. These aspects are connected with a second mechanism: according to the stress-adjustment perspective, a change in family structure might induce stress which leads to negative outcomes for children (Amato 2000). A related mechanism is the level of parent–child conflict (Cavanagh 2008), which may increase in the case of separation. For example, Mak et al. (2010) reported that adolescents from single-parent and no-parent families of Hong Kong Chinese had higher substance use, and hypothesised that this relationship is mediated by poorer communication with the absent father. In this perspective, children who have experienced the separation or the death of a parent are more vulnerable compared to those who are born in never-married single-parent families, but less vulnerable than those living in step-families (who have to spend an additional period of adjustment). In other words, as suggested by literature, it would be the number of family transitions that matters (Cavanagh 2008; Cavanagh and Huston 2008; Magnuson and Berger 2009; Hofferth and Goldscheider 2010). Biblarz and Gottainer (2000) suggest that there might be a difference also between children who underwent parental separation and those who underwent a parents’ death. These differences are in terms of conflicts (i.e. divorce might lead to hostile feelings toward the the father, while orphans might develop a positive inner construction of fathers), parental behaviour (i.e. widowed parents have more traditional life styles than divorced ones), and economic (widows have a greater financial support after husband’s death, than what divorced mothers have after separation).
Research has also emphasised the role of parental behaviours. Parents who are not married or become divorced/widowed generally exhibit less healthy behaviour than parents in married couples (see Lee et al. 2005, for a discussion) and this, in turn, may have an influence on their children. According to social learning theory (Bandura 1977, 1986), indeed, parents’ actions may be emulated by children: thus, for example, the children of parents who are smokers are more likely to smoke than those of non-smoking parents (Hill et al. 2005; Rainio et al. 2008; Brown and Rinelli 2010) and similarly for other risky and healthy types of behaviour (Bere and Klepp 2004; Gross et al. 2010). Research also shows some contradictory findings: in their review of researches assessing the association between adolescent smoking and parent smoking, Avenevoli and Merikangas (2003) cited reports regarding the non-significant effects of current parental smoking; similarly, in their review of studies on parental correlates of children’s physical activity level, Gustafson and Rhodes (2006) found that some researchers reported weak or no correlation between the physical activity patterns of parents and children.
Lastly, what is commonly called family functioning - the quality of interactions and relationships between family members – may be an important mechanism in the connection between family structure and children behavioural outcomes. Limited parental contacts are widely acknowledged disadvantages of separated parents families (Kelly 2003) and the patterns of parent–child interaction may confound the relationship between specific types of families and adolescents’ “outcomes” since it has an effect on children’s behaviour (Shek 1997). For example, it has been shown that greater perceived support protects against substance use (Wills et al. 2004; Brown and Rinelli 2010), whereas negative relationships, such as family conflicts, predict greater use (Aquilino and Supple 2001). Similarly, a positive environment, in which the family has meals together, has been found to reduce the risks of disordered eating behaviour (Neumark-Sztainer et al. 2004) and parental support promotes children’s physical activity (Sallis et al. 2000). In fact, family functioning is not necessarily connected with family structure, since in several cases, children whose parents were still together experience more conflicts than those whose parents broke up but still had good contacts.
As Barrett and Turner (2006) emphasised, most previous studies focus on a single aspect of these possible mechanisms. Thus, it is not clear whether differences across family types really mean that family structure affects children’s health behaviour, or whether it is simply the spurious effect of the changing socio-economic circumstances and relationship characteristics (e.g. family functioning) of single-parent families and step-families compared with those typical of families formed by both married biological parents. Some researches considering family structure together with socio-economic status and parental behaviour (Griesbach et al. 2003) and other factors, such as the quality of the parent–child interaction (Barrett and Turner 2006; Brown and Rinelli 2010), have shown that the different characteristics of different families do not always explain the higher percentage of at risk behaviour among adolescents in some families.
3 Data and Methods
3.1 Measures
We use data from the Multipurpose survey “Aspects of Daily Life,” conducted in Italy by the Italian Statistical Institute (ISTAT). This survey has been conducted yearly since 1993 on nationally representative cross-sectional samples of about 20,000 households per year. It uses the paper-and-pencil interview technique and is based on face-to-face interviews and self-administered questionnaires. A complex sampling pattern based on stratification of municipalities according to their demographic size is used (for details on stratification and selection of sample units, see methodological notes, available at: http://en.istat.it/salastampa/comunicati/non_calendario/20100512_00/methodology.pdf ). Besides socio-demographic characteristics, several items covering health, lifestyle, and social behaviour for each household member (aged over 11) are recorded, together with information on the family’s socio-economic status and structure, and satisfaction within family relationships. In the present work, we use data from the 2005–2009 rounds.Footnote 1 Adolescents’ health behaviour, family structure and family characteristics were measured in the following ways.
Smoking Status
Current smoking behaviour was assessed by the question “Do you smoke at present?” Three response alternatives were offered: “Yes,” “I used to smoke,” and “I have never smoked.” Adolescents’ smoking status was defined through three categories in descriptive analyses: smokers, ex-smokers, and non-smokers; in all subsequent analyses, “never-smokers” were compared with “ever-smokers” (including both ex-smokers and current smokers).
Alcohol Use
Drinking behaviour was investigated by various questions aimed at assessing lifetime drinking habits, drinking in the past 12 months, and current use of wine, beer, and spirits. The survey also recorded whether respondents had ever experienced “binge drinking”. This was measured by a question which asked whether, during the past 12 months, the interviewee had drunk six or more alcoholic drinks one after the other. We chose to focus on this behaviour, since it is more risky than the general consumption of alcohol.
Physical Activity
The survey provides separate items for playing sports and engaging in some kind of other physical activity. In particular, whether individuals play sports habitually or only occasionally is examined; for those who do not engage in sports either habitually or occasionally, questions cover how often (never/less than once a month/at least once a month/at least once a week) some types of physical activity are practiced (such as walks of about two kilometres, swimming or cycling). For our descriptive analysis, we constructed a categorical variable distinguishing individuals who habitually play sports, play sports only occasionally, engage only in some kinds of physical activity, and sedentary individuals. In the multivariate analyses, adolescents were distinguished according to whether they were sedentary or not.Footnote 2
Consumption of Fruit and Vegetables
Respondents were asked the frequency with which they consumed several items of food, including fruit and vegetables, and how many days (in a week) they usually consumed different kinds of food. The five response categories were “not at all,” “less than once a week,” “several times a week,” “once a day,” and “more than once a day.” A dichotomous variable defined daily consumers of fruit and vegetablesFootnote 3 as those who answered that they ate fruit and vegetables at least once a day.
Family Structure
This was defined according to the family ties between young children and adults in the household, and parents’ marital status. In this way, seven categories of families were distinguished:
-
Both married biological parents, married: adolescents lived with both their married biological parents.
-
Both unmarried biological parents, cohabiting: adolescents lived with both their unmarried biological parents.
-
Step-families: adolescents lived with their father and his partner or with their mother and her partner.
-
Widowed single-parent families: adolescents lived with either their father or their mother but not with both, and did not live with a step-parent after the death of a parent.
-
SeparatedFootnote 4 single-parent families: adolescents lived with either their father or their mother but not with both, and did not live with a step-parent after their parents’ marital dissolution.
-
Never-married single-parent families: adolescents lived with either their father or their mother, who had never been married to each other and who did not have a live-in partner.
-
Non-parental families: adolescents did not live with their father, mother, or a step-parent. Since less than 1 % (41 observations, or 0.4 %) of the adolescents aged 14–17 of our sample lived in non-parental families, these cases were removed from the following analyses. No meaningful analyses could be carried out on such a small group.
In addition, the number of siblings was controlled for, but not the presence of other family members, since very few adolescents in our sample lived with family members other than their siblings and parents. Nor do we distinguish between adolescents living with their biological parents and those living with adoptive parents, as this information was not available in our data. However, as the number of adoptive parents is very low in Italy,Footnote 5 even if this information had been available, it could not have been used, due to its low prevalence.
Family Socio-Economic Status
Several of the survey questions can be used as measures of a family’s socio-economic status. Families were asked about the quality of the neighbourhood in which they lived, the quality of their accommodation, and which durable goods they possessed, and three indices were constructed for each of these aspects. They were built as weighted averages of items (see Table 3, Appendix), in which the weights were inversely proportional to the coefficient of variation of each item. For example, if we examine the last index (possession of durable goods), in this way we give greater weight to goods which are owned by a large percentage of families, and a lower weight to ones which are owned by only a small percentage of families. Each index value ranges from 0 to 1 (higher values indicating higher socio-economic status) and is considered as continuous variable. This approach is similar to that used by Aassve et al. (2007) with European Community Household Panel data. In addition, the highest educational level obtained by at least one parent was considered as a measure of family socio-economic status. We also controlled for parents’ employment status, distinguishing families with both co-resident parents unemployed or inactive from those in which at least one parent was employed or retired. Lastly, parental age was controlled for by averaging parents’ age if adolescents lived with two parents. This serves as a proxy of parents’ cohort, and our expectation was that different cohorts would have different parenting standards (e.g., younger cohorts would on average have a lower level of monitoring than older cohorts).
Parental Behaviour
In order to take into account the possible influence of parental behaviour, health behaviour reported by both (co-resident) fathers and mothers were considered. For parental smoking status, families were divided in two groups: those without a smoking parent, and those with one or both smoking parents. A similar categorisation was used to identify parents who were ex-smokers. Parental alcohol use was considered through the daily consumption of wine and beer. Excessive drinkers were defined as men consuming more than three alcoholic unitsFootnote 6 per day and as women consuming more than two units per day.Footnote 7 Children with parents who were not excessive drinkers were distinguished from those who had at least one parent who drank to excess. As regards physical activity, parents who did not engage in sports either habitually or occasionally and who did not practise any other form of physical activity were defined as sedentary. In this way, families were distinguished according to whether they had at least one sedentary parent. Parental diet behaviour was measured by the daily consumption of fruit and vegetables, and parents who were daily consumers were distinguished from those who reported the opposite. Families were grouped into two categories according to whether they contained no parents who did not consumed fruit or vegetables daily, and those with one or two parents who did.
Adolescents’ Satisfaction with Family Relationships
We did not have an accurate measure of family functioning, but a question asking children to evaluate their satisfaction with family relationships was taken as a proxy of this aspect. In particular, all household members aged over 14 were asked whether they were satisfied with their family relationships, with reference to the past 12 months. Four responses were possible: “a lot”, “quite”, “so-so”, and “not at all”. In the following analyses, adolescents who were a lot or quite satisfied were distinguished from the other two response groups.
3.2 Descriptive Analyses
Table 1 lists the percentages of types of health behaviour among adolescents aged 14–17, by family structure. The findings are in line with previous literature showing that health behaviour during adolescence varies according to family structure. In particular, adolescents living in families other than those with both married biological parents are significantly more likely to smoke. Teenagers in step-families have particularly high levels of smokers. As regards binge drinking, the differences according to family structure were less strong (and are not significant), but they did depend on the number of parents: adolescents living with only one parent had higher levels of this at risk behaviour than those living with two parents. Sports and physical activities were more common among adolescents living with both married biological parents (even if differences are not strongly significant); conversely, the percentage of sedentary adolescents was highest among those living in step-families. Among teenagers living with only one parent, those who had suffered the death of a parent had the highest level of sedentary lifestyle. Adolescents living with unmarried biological parents were also more frequently sedentary than those with married parents. Lastly, the daily consumption of fruit and vegetables was slightly lower among adolescents living with separated or widowed single parents than those living with both married biological parents. Teenagers living with unmarried biological parents showed the lowest consumption of fruit and vegetables. Surprisingly, those living in step-families or never-married single-parent families more frequently had better diets than those in traditional families with both married biological parents.
3.3 Multivariate Analyses
As previously noted, results showing associations between family structure and adolescent health behaviour may depend on factors such as family satisfaction, parental behaviour, and economic resources. In order to assess whether family structure had an independent effect on adolescents’ health behaviour, separate multivariate analyses were carried out for each one, entered as a dependent variable; other variables, such as family structure, family satisfaction, family socio-economic status, and parental behaviour were considered as covariates. Each year of the survey (from 2005 to 2009) was also controlled for.Footnote 8 Other background factors of adolescents, such as their gender, age, region of residence, and number of siblings, were considered as control covariates.
Dependent dichotomous variables (smoking status, binge drinking, sedentary lifestyle, daily fruit and vegetable consumption) were analysed with logistic regression models.
Table 2 lists the coefficients of the finalFootnote 9 models describing adolescents’ health behaviour: a positive coefficient indicates an higher risk of unhealthy behaviour with respect the baseline category, while a negative value indicates a lower risk. In order to assess which family characteristics potentially alter the effect of family structure on adolescents’ health behaviour, additional models were fitted to include groups of explanatory variables, one at a time: the first model contains only family structure, and family economic well-being indicators, family satisfaction, and parental behaviour were then added. The results are listed in the Appendix for clarity.
4 Results
Our results show that male adolescents are more likely to engage in at risk behaviour like smoking and binge drinking, and to have a worse diet than female adolescents, who are more prone to sedentary behaviour. For example, the odds of smoking for boys are 1.66 (= exp(0.51)) times the odds for girls. Teenagers aged 14–15 have a lower risk of smoking, binge drinking and sedentary behaviour than those aged 16–17. Adolescents living in the northern regions of Italy are more likely to engage in at risk behaviour but less likely to be sedentary.
As regards family characteristics, parental behaviour appears to have a very strong effect on children’s behaviour, particularly as regards at risk behaviour. Family satisfaction has strong effects on at risk behaviour but not on physical activity. Socio-economic status is only significant for binge drinking and physical activity. After having controlled for these factors, the effect of family structure turns out to be significant only for smoking and, partially, for the other at risk behaviour (binge drinking). Single parenthood has a positive effect on the probability of smoking: for example, the odds of smoking for adolescents living in separated single-parent families are 1.81 (= exp(0.59)) times the odds for those living with both married biological parents; adolescents living in step-families have 1.92 (= exp(0.65)) times the odds of smoking than the reference group. Adolescents in separated single-parent families are also more likely to have experienced binge drinking, having an odds of 1.42 times the odds of other adolescents. Instead, the effect of living with both unmarried biological parents is never significant.
Table 4 in the Appendix shows that the association between some family types and adolescent smoking is not confounded by lower economic status, higher parental smoking, or lower family satisfaction among some family types. Instead, the effect of living with both unmarried biological parents disappears once family satisfaction is controlled for. Similarly, as regards physical activity, the effects of widowed and separated single-parent families, of unmarried biological parents, and of step-families disappeared once family economic status and parental behaviour, respectively, were controlled for (Table 6).
5 Discussion
Our study extends the literature on variations according to family structure in the propensity towards healthy versus at risk behaviour among adolescents by examining explanations for these differences.
In contrast with many previous studies, which did not always analyse the effect of family structure controlling for various family characteristic, we simultaneously examined the influence of family structure, family socio-economic status, parental behaviour, and family satisfaction on children’s health behaviour. In addition, the definition of family structure was more detailed than usual: in most studies, single-parent families whose status is due to widowhood are not distinguished from those due to separation/divorce or those made up of a never-married parent. These single-parent variations in family structure may give rise to non-identical family environments; thus, making a distinction between them may be important when examining the effect of family structure (as suggested, for example, by Biblarz and Gottainer 2000). Single-parent families are distinguished across widowed, never married, and separated parents. Two-parent families are distinguished across unmarried biological parents, married biological parents, and step-families.
Some other potentially important factors are not considered in this study, although including them in future extension to this field of research would be interesting. First of all, we did not control for the critical role played by peer group (Hussong 2002). In addition, since children living in single-parent families may be exposed not only to the behaviour of the custodial parent but also to that of the non-resident parent, the latter is an important factor which should be included. Unfortunately, both information on peer group and on non-resident parent was not available for the present analysis. Lastly, we did not control for other family members (aunts, uncles, grandparents) which might influence child behaviour, but their prevalence was too low for us to be able to create an additional category with the available data.
The overall findings of our study are that family structure has a significant effect on adolescents’ behaviour but, once family characteristics are controlled for, in some cases this effect becomes non-significant. In particular, for lifestyle behaviour such as physical activity and diet, the negative effect of some family types (living with unmarried biological parents, or in separated or widowed single-parent families as regards physical activity, and living with unmarried biological parents as regards diet) is confounded by family socio-economic status, as these family types are of poorer socio-economic status.
Instead, the effect of family structure on adolescents’ smoking habits persists when all other household characteristics are controlled for. A similar result has been obtained also in some other countries, particularly for adolescents living in step-families (Griesbach et al. 2003). One natural explanation for this is poorer parental monitoring and less provision of supervision in single-parent families and step-families than that provided in two-biological-parent families (see Otten et al. 2007). However, this explanation is not completely consistent with findings on binge drinking, which is only partially affected by family structure. We may therefore hypothesise that the prevalence of binge drinking among adolescents does not really depend on the level of parental monitoring, but is also affected by other factors: the family satisfaction effect is very strong, so intergenerational conflict may be much more important than the level of supervision (as found in some European studies, see, for example, Breivik et al. 2009; Mak et al. 2010). This was not measured in our study, but it is probably associated with the measure of family functioning which we used. Smoking is affected by both intergenerational conflict and the level of parental monitoring, and this is why the family structure effect is significant for this behaviour. Hence, this analysis could be extended by using better measures of conflict and monitoring levels, in order to test this hypothesis.
Notes
Using several rounds of the same survey allows us to have a sufficient number of cases for robust results, even for the smaller groups, e.g., those living in step-families.
Keeping the physical activity variable as four ordinal categories does not provide different results than those obtained with a binary variable.
The World Health Organization recommends eating at least five portions of fruit and vegetables every day, but few children reach this target. In Italy, as a consequence, we use a less restrictive measure of a good diet.
This category also includes single-parent families with divorced parents. It should be noted indeed that, according to Italian law, couples may be divorced only after 3 years of legal separation and that many couples do not even try to go through divorce procedures and remain “separated”. For this reason, in this work, the term “separated” is used with reference to parents having undergone marital dissolution, and includes both separated and divorced persons.
Analyses based on data from another survey (the nation-wide representative survey “Families and Social Subjects”) conducted in Italy in 2009 showed that, of women aged 15 and over, only 0.4 % had at least one adopted child.
One alcoholic unit is the quantity of alcohol contained in a small glass (125 ml) of wine, a can (330 ml) of beer, or a small glass (40 ml) of spirits.
These thresholds were used following Italian Ministry of Health guidelines.
We actually have also implemented analyses with random intercept and/or random slope taking into account the fact that data come from several rounds of a survey. However, these models did not increase the goodness of fit, while they are far less efficient than the model used in the paper.
The interactions were not statistically significant.
References
Aassve, A., Betti, G., Mazzuco, S., & Mencarini, L. (2007). Marital disruption and economic well-being: a comparative analysis. Journal of the Royal Statistical Society, Series A, 170(3), 781–799.
Amato, P. R. (2000). The consequences of divorce for adults and children. Journal of Marriage and the Family, 62, 1269–1287.
Aquilino, W. S., & Supple, A. J. (2001). Long-term effects of parenting practices during adolescence on well-being outcomes in young adulthood. Journal of Family Issues, 22(3), 289–308.
Avenevoli, S., & Merikangas, K. R. (2003). Familial influences on adolescent smoking. Addiction, 98, 1–20.
Bandura, A. (1977). Social learning theory. New York: Prentice Hall, Englewood Cliffs.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. New York: Prentice-Hall, Upper Saddle River.
Barrett, A. E., & Turner, J. (2006). Family structure and substance use problems in adolescence and early adulthood: examining explanations for the relationship. Addiction, 101, 109–120.
Bere, E., & Klepp, K. I. (2004). Correlates of fruit and vegetable intake among Norwegian schoolchildren: parental and self-reports. Public Health Nutrition, 7(8), 991–998.
Biblarz, T., & Gottainer, G. (2000). Family structure and children’s success: a comparison of widowed and divorced single-mother families. Journal of Marriage and the Family, 62(2), 533–548.
Blum, R. W., Beuhring, T., Shew, M. L., Bearinger, L. H., Sieving, R. E., & Resnick, M. D. (2000). The effects of race/ethnicity, income, and family structure on adolescent risk behaviors. American Journal of Public Health, 90(12), 1879–1884.
Breivik, K., Olweus, D., & Endresen, I. (2009). Does the quality of parent–child relationships mediate the increased risk for antisocial behaviour and substance use among adolescents in single-mother and single-father families? Journal of Divorce & Remarriage, 50, 400–426.
Broman, C. L., Li, X., & Reckase, M. (2008). Family structure and mediators of adolescent drug use. Journal of Family Issues, 29(12), 1625–1649.
Brown, S. L., & Rinelli, L. N. (2010). Family structure, family processes, and adolescent smoking and drinking. Journal of Research on Adolescence, 20(2), 259–273.
Cavanagh, S. E. (2008). Family structure history and adolescent adjustment. Journal of Family Issues, 29(7), 944–980.
Cavanagh, S. E., & Huston, A. C. (2008). The timing of family instability and children’s social development. Journal of Marriage and the Family, 70, 1258–1269.
Duncan, S. C., Duncan, T. E., Strycker, L. A., & Chaumeton, N. R. (2002). Relations between youth antisocial and prosocial activities. Journal of Behavioural Medicine, 25, 425–438.
Eurostat. (2010). Household structure in the EU. Eurostat Methodologies and working Papers.
González-Val, R., & Marcén, M. (2012). Breaks in the breaks: an analysis of divorce rates in Europe. International Review of Law and Economics, 32(2), 242–255.
Green, M., & Palfrey, J. S. (2000). Bright futures: Guidelines for health supervision of infants, children, and adolescents (2nd ed.). Arlington: National Center for Education in Maternal and Child Health.
Griesbach, D., Amos, A., & Currie, C. (2003). Adolescent smoking and family structure in Europe. Social Science & Medicine, 56(1), 41–52.
Gross, S. M., Pollock, E. D., & Braun, B. (2010). Family influence: key to fruit and vegetable consumption among fourth- and fifth-grade students. Journal of Nutrition Education and Behavior, 42(4), 235–241.
Gustafson, S. L., & Rhodes, R. E. (2006). Parental correlates of physical activity in children and early adolescents. Sports Medicine, 36(1), 79–97.
Hallal, P. C., Victora, C. G., Azevedo, M. R., & Ells, J. C. K. (2006). Adolescent physical activity and health: a systematic review. Sports Medicine, 36(12), 1019–1030.
Hanson, M. D., & Chen, E. (2007). Socioeconomic status and health behaviors in adolescence: a review of the literature. Journal of Behavioral Medicine, 30(3), 263–285.
Hill, K. G., Hawkins, J. D., Catalano, R. F., Abbott, R. D., & Guo, J. (2005). Family influences on the risk of daily smoking initiation. Journal of Adolescent Health, 37(3), 202–210
Hofferth, S. L., & Goldscheider, F. (2010). Family structure and the transition to early parenthood. Demography, 47, 415–437.
Hu, M. C., Davies, M., & Kandel, D. B. (2006). Epidemiology and correlates of daily smoking and nicotine dependence among young adults in the United States. American Journal of Public Health, 96(2), 299–308.
Hussong, A. M. (2002). Differentiating peer contexts and risk for adolescent substance abuse. Journal of Youth and Adolescence, 31, 207–220.
Iacovu, M., & Skew, A. J. (2011). Household composition across the new Europe: where do the new Member States fit in? Demographic Research, 25, 465–490.
Jefferis, B. J., Power, C., Graham, H., & Manor, O. (2004). Effects of childhood socioeconomic circumstances on persistent smoking. American Journal of Public Health, 94(2), 279–285.
Kelly, J. B. (2003). Changing perspectives on children’s adjustment following divorce: a view from the United States. Childhood, 10, 237–254.
Klüsener, S., Perrelli-Harris, B, & Sánchez Gassen, N. (2012). Spatial aspects of the rise of nonmarital fertility across Europe since 1960: the role of states and regions in shaping patterns of change. MPIDR Working Paper 2012–005.
La Torre, G., Masala, D., De Vito, E., Langiano, E., Capelli, G., & Ricciardi, W. (2006). Extra-curricular physical activity and socioeconomic status in Italian adolescents. BMC Public Health, 6, 1–9.
Ledoux, S., Miller, P., Choquet, M., & Plant, M. (2002). Family structure, parent–child relationships, and alcohol and other drug use among teenagers in France and the United Kingdom. Alcohol and Alcoholism, 37(1), 52–60.
Lee, S., Cho, E., Grodstein, F., Kawachi, I., Hu, F. B., & Colditz, G. A. (2005). Effects of marital transitions on changes in dietary and other health behaviours in US women. International Epidemiological Association, 34, 69–78.
Lien, N., Lytle, L. A., & Klepp, K. I. (2001). Stability in consumption of fruit, vegetables, and sugary foods in a cohort from age 14 to age 21. Preventive Medicine, 33, 217–226.
Magnuson, K., & Berger, L. M. (2009). Family structure states and transitions: associations with children’s well-being during middle childhood. Journal of Marriage and the Family, 71, 575–591.
Mak, K. K., Ho, S. Y., Thomas, G. N., Schooling, C. M., McGhee, S. M., & Lam, T. H. (2010). Family structure, parent–child conversation time and substance use among Chinese adolescents. BMC Public Health, 10, 503.
Manning, W. D., & Brown, S. (2006). Children’s economic well-being in married and cohabiting parent families. Journal of Marriage and the Family, 68(2), 345–362.
McLanahan, S. (2009). Children in fragile families. Mimeo: Princeton University.
Mikkilä, V., Räsänen, L., Raitakari, O. T., Pietinen, P., & Viikari, J. (2004). Longitudinal changes in diet from childhood into adulthood with respect to risk of cardiovascular diseases: the cardiovascular risk in young Finns study. European Journal of Clinical Nutrition, 58, 1038–1045.
Millar, J., & Ridge, T. (2001). Families, poverty, work and care: A review of literature on lone parents and low-income families, Leeds: department for work and pensions research report 153.
Neumark-Sztainer, D., Wall, M., Story, M., & Fulkerson, J. A. (2004). Are family meal patterns associated with disordered eating behaviors among adolescents? Journal of Adolescent Health, 35, 350–359.
OECD. (2009). Doing Better for Children. OECD. http://www.oecd.org/els/family/doingbetterforchildren.htm.
Otten, R., Engels, R. C. M. E., van de Ven, M. O. M., & Bricker, J. B. (2007). Parental smoking and adolescent smoking stages: the role of parents’ current and former smoking, and family structure. Journal of Behavioral Medicine, 30, 143–154.
Rainio, S. U., Rimpelä, A. H., Luukkaala, T. H., & Rimpelä, M. K. (2008). Evolution of the association between parental and child smoking in Finland between 1977 and 2005. Preventive Medicine, 46, 565–571.
Rasmussen, M., Krølner, R., Klepp, K., Lytle, L., Brug, J., Bere, E., & Due, P. (2006). Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. International Journal of Behavioral Nutrition and Physical Activity, 3, 22.
Reddy, W. S., & Katan, M. B. (2004). Diet, nutrition and the prevention of hypertension and cardiovascular diseases. Public Health Nutrition, 7, 167–186.
Roos, E. B., Hirvonen, T., Mikkilä, V., Karvonen, S., & Rimpelä, M. (2001). Household educational level as a determinant of consumption of raw vegetables among male and female adolescents. Preventive Medicine, 33, 282–291.
Sallis, J. F., Prochaska, J. J., & Taylor, W. C. (2000). A review of correlates of physical activity of children and adolescents. Medicine and Science in Sports and Exercise, 32, 963–973.
Sanchez, A., Norman, G. J., Sallis, J. F., Calfas, K. J., Cella, J., & Patrick, K. (2007). Patterns and correlates of physical activity and nutrition behaviors in adolescents. American Journal of Preventive Medicine, 32, 124–130.
Shek, D. T. L. (1997). The relation of family functioning to adolescent psychological well-being, school adjustment, and problem behavior. The Journal of Genetic Psychology, 158(4), 467–479.
Stewart, S. D., & Menning, C. L. (2009). Family structure, nonresident father involvement, and adolescent eating patterns. Journal of Adolescent Health, 45, 193–201.
Sweeting, H., & West, P. (2001). Social class and smoking at age 15: the effect of different definitions of smoking. Addiction, 96, 1357–1359.
Telama, R., Yang, X., Viikari, J., Valimaki, I., Wanne, O., & Raitakari, O. (2005). Physical activity from childhood to adulthood: a 21-year tracking study. American Journal of Preventive Medicine, 28, 267–273.
Tercyak, K. P., & Tyc, V. L. (2006). Opportunities and challenges in the prevention and control of cancer and other chronic diseases: children’s diet and nutrition and weight and physical activity. Journal of Pediatric Psychology, 31, 750–763.
Tinsley, B. J. (2003). How children learn to be healthy. Cambridge, England: Cambridge University Press.
van Poppel, F., Schenk, N., & van Gaalen, R. (2013). Demographic transitions and chahes in te living arrangements of children: the Netherlands 1850–2010. Population Research and Policy Review, 332, 243–260.
Wardle, J., Jarvis, M. J., Steggles, N., Sutton, S., Williamson, S., Farrimond, H., Cartwright, M., & Simon, A. E. (2003). Socioeconomic disparities in cancer-risk behaviors in adolescence: baseline results from the Health and Behaviour in Teenagers Study (HABITS). Preventive Medicine, 36, 721–730.
Wills, T. A., Resko, J. A., Ainette, M. G., & Mendoza, D. (2004). Role of parent support and peer support in adolescent substance use: a test of mediated effects. Psychology of Addictive Behaviors, 18, 122–134.
Xie, B., Gilliland, F. D., Li, Y. F., & Rockett, H. R. (2003). Effects of ethnicity, family income, and education on dietary intake among adolescents. Preventive Medicine, 36, 30–40.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Mazzuco, S., Meggiolaro, S. Family Structures and Health Behaviour in Adolescents. Child Ind Res 7, 155–175 (2014). https://doi.org/10.1007/s12187-013-9207-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12187-013-9207-5