
Abstract
Purpose of Review
Injury to the ulnar collateral ligament is the most common, significant injury affecting the medial elbow of the overhead athlete. However, there are many other significant sources of pathology that should be considered. This review seeks to present a broad range of conditions that providers should consider when evaluating the overhead athlete with medial elbow pain.
Recent Findings
Recent biomechanical studies have deepened understanding of the anatomy and function of the anterior bundle of the ulnar collateral ligament germane to the overhead athlete. Orthobiologics hold potential for expanding the role of non-operative treatment for ulnar collateral ligament injuries.
Summary
In addition to injury to the ulnar collateral ligament, providers should be prepared to diagnose and treat valgus extension overload, proximal olecranon stress fracture, ulnar nerve pathology, common flexor - pronator mass injury, and, in adolescents, medial epicondylar avulsion, when managing medial elbow pain in the overhead athlete.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rupture of the ulnar collateral ligament continues to be the most feared of medial elbow injuries. Less appreciated, but equally significant pathologies affecting the thrower’s elbow include valgus extension overload, ulnar nerve pathology, common flexor - pronator mass injury, and proximal ulnar shaft stress reaction. Furthermore, in a skeletally immature population, medial epicondylar apophysitis can produce substantial pain and dysfunction, and potentially lead to avulsion of the epicondyle.
Overhead throwing imparts tremendous load to the medial elbow, both from acute and chronic—repetitive perspectives, resulting in significant potential for injury in the overhead athlete. According to some authors, up to 22% of days on the disabled list (DL) and up to 16.4% of documented injuries in Major League Baseball (MLB) result from elbow pathology [1, 2]. Other data would suggest more conservative, but nonetheless significant, estimates of 7.8% and 9.8% in MLB and Minor League Baseball (MiLB) respectively [3•]. In a recent epidemiologic analysis of MLB and MiLB taken over a 5-year period from the MLB Health and Injury Tracking System, a significant number of documented elbow injuries (> 40%) involved medial elbow anatomy [3•]. Interestingly, only a small percentage (< 3%) were attributed directly to lateral structures, outside of traumatic contusions arising from collisions or errant pitches.
Anatomy and Biomechanics of the Medial Elbow
Osseous Anatomy of the Medial Elbow
The general osseous anatomy of the elbow joint possesses some inherent complexity, consisting of three functionally separate articulations: the proximal radioulnar, the radiocapitellar, and the ulnohumeral. These articulations permit a constrained range-of-motion in flexion and extension between the humerus and radioulnar forearm unit generally ranging between − 5° and 140°, as well as rotational motion within the radioulnar forearm unit ranging between 90° of pronation and 90° of supination [4, 5]. Most relevant to medial elbow pathology, the humeral trochlea articulates with the sigmoid notch of the proximal ulna, with the olecranon process constituting the most proximal aspect of the notch and the coronoid process the most distal. The medial epicondyle arises from an apophysis positioned slightly medial and posterior to the central axis of the humerus. The medial epicondylar apophysis is the last of the six physes at the elbow to close during skeletal maturity with implications for medial-sided elbow injury in adolescent throwers [6, 7].
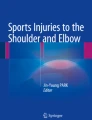
The medial epicondyle provides a proximal attachment for the ulnar collateral ligament complex (UCL), as well as a point of origin for the common flexor-pronator mass (Fig. 1) and a ceiling for the trajectory of the ulnar nerve as it traverses the elbow [4]. Additional soft tissue structures in relative proximity to the medial epicondyle include the median nerve and the brachial artery, resting in that order from medial to lateral and generally uninvolved in medial-sided elbow pain in the thrower [4].

Basic ligamentous and muscular anatomy of medial elbow (reprinted from [8•], copyright © 2017 by SAGE Publications, Inc. Reprinted by Permission of SAGE Publications, Inc.)
Ligamentous Anatomy of the Medial Elbow
The UCL includes anterior, posterior, and transverse bundles as distinct thickenings of the medial elbow joint capsule. The anterior bundle can be further divided into anterior and posterior bands with distinct functions as the elbow flexes and extends. A recent study detailed the osteoligamentous anatomic footprint of the UCL and challenged historical notions [9]. The anterior bundle arises from the anterior-inferior aspect of the medial epicondyle with a roughly circular origin footprint of 32 mm2 and possesses an elongated and distally tapered ulnar attachment measuring 188 mm2 and 2.6 cm in length. Although historically the distal attachment of the anterior bundle was described as involving the sublime tubercle of the proximal medial ulna, more current quantitative analysis of the ulnar attachment has identified the actual attachment as including the medial ulnar collateral ridge, which extends an average of 22 mm beyond the tubercle (Fig. 2) [10]. The posterior and transverse (oblique) bundles have significantly smaller dimensions, with proximal/distal attachments being roughly circular and measuring 26 mm2/16 mm2 and 21 mm2/17 mm2 respectively. The posterior bundle has a proximal attachment positioned on the direct inferior surface of the medial epicondyle and a distal attachment along the posterior aspect of the semilunar notch. The transverse bundle has both attachment sites along the semilunar notch, with the one arising immediately posterior to the distal attachment of the anterior bundle and the other immediately anterior to that of the posterior bundle [9].

a, b Extended distal attachment of the anterior bundle of the medial collateral ligament along the medial collateral ligament ridge (reprinted from [10], copyright © 2011 by SAGE Publications, Inc. Reprinted by Permission of SAGE Publications, Inc.)
Muscular Anatomy of the Medial Elbow
The flexor carpi ulnaris (FCU), flexor digitorum superficialis, and a portion of the pronator teres originate from a conjoined tendon at the medial epicondyle. The FCU has additional origin along the medial aspect of the coronoid process and proximal medial ulna, essentially giving rise to two “heads” between which the ulnar nerve passes. It has been hypothesized that the FCU, which overlaps approximately 21% of the anterior bundle of the UCL and exerts a line of action slightly posterior to the elbow’s axis of rotation, plays the most significant role in valgus stability of the elbow, functioning as a secondary dynamic restraint [4, 8•, 11]. Nevertheless, EMG investigation failed to demonstrate significant activation of this musculature during application of valgus force across the elbow, leaving this idea somewhat controversial [12].
Nervous Anatomy of the Medial Elbow
The ulnar nerve represents a continuation of the medial cord of the brachial plexus and contains fibers from C8 and T1. Its course takes it along the medial border of the distal triceps, posterior to the medial intermuscular septum and medial epicondyle, and passes into the body of the FCU between its two “heads.” Although a rare branch to the triceps has been described, the ulnar nerve most commonly has no brachial branches and has as its first motor branches those to the FCU [4]. As it passes into the FCU, it lies directly superficial to the ulnar attachment of the posterior bundle of the UCL. Immediately after entering the FCU, the nerve lies along the elongated ulnar attachment of the anterior bundle. An awareness of this anatomic proximity is essential to safe execution of ulnar collateral ligament repair or reconstruction. A final consideration is the medial antebrachial cutaneous nerve (MACN), which is a direct branch of the medial cord of the brachial plexus. The MACN traverses the brachium in a position medial to the brachial artery, dividing into volar and ulnar branches in the distal brachium. The ulnar branch crosses anterior to the medial epicondyle, continuing to the dorsal antebrachium at times as far distal as the wrist [13]. Clinically relevant instability of the MACN has been described and must also be considered, most commonly as a diagnosis of exclusion, during evaluation of medial elbow pain in the thrower [14•].
Biomechanics of the Medial Elbow
Valgus stability of the elbow arises from a variety of static and dynamic elements. Static elements functioning as primary restraints to valgus strain include the ulnar collateral ligament, ulnohumeral articulation of the trochlea within the sigmoid notch. Secondary restraints include the anterior elbow joint capsule, common flexor-pronator mass, and radiohumeral articulation [5]. Primary restraints can be defined as those structures that if sectioned will generate laxity, whereas a secondary restraint is defined as a structure whose release in isolation is insufficient to cause laxity, but whose release in addition to the release of a primary restraint will increase laxity [15,16,17]. The relative contributions of soft tissue versus osseous restraints vary with degree of elbow flexion. Soft tissue restraints—in particular the UCL—making increasingly significant contributions to valgus stability as the elbow moves in flexion [5]. The proximal aspect of the sigmoid notch and associated olecranon process can up to 85% of the osseous contribution to valgus stability.
With respect to the biomechanical function of the distinct elements of the UCL, the anterior bundle functions as the principle restraint to valgus stress [16,17,18]. Furthermore, the anterior bundle of the UCL can be divided into functional anterior and posterior bands of equal widths that tighten and relax in reciprocal fashion, making their most significant contribution to valgus stability as the elbow moves through a range of flexion and extension from 30° to 120° [18, 19]. The anterior band remains taut from 30° to 90°, and the posterior band from approximately 90° to 120°. This range corresponds to the typical range of flexion angles experienced by the elbow during the throwing cycle, making it arguably the single most important valgus stabilizer during the throwing motion. The posterior bundle can be considered a secondary valgus restraint throughout functional elbow range-of-motion and constitutes the floor of the cubital tunnel, potentially playing a role in ulnar nerve compression as the elbow flexes [18, 20]. The transverse bundle does not traverse the ulnohumeral articulation and therefore does not contribute to valgus stability.
Ulnar Collateral Ligament Pathology
History and Physical Exam
In the author’s experience, it is rare that UCL injuries present with a classic “pop” and acute pain following a single pitch or throw. More commonly, throwers experience a prodromal phase of forearm or medial elbow “tightness” or “discomfort” associated with varying degrees of loss of location and/or velocity over a period of time. Ultimately, the athlete is unable to throw and presents for evaluation. To that end, any throwing athlete presenting with vague symptoms of medial forearm tightness should be taken seriously and injury to the UCL should be considered rather than dismissing the episode as “flexor tendonitis.”
Physical exam follows a systematic assessment of elbow range-of-motion and tenderness. Subtle loss of terminal extension is common in elite throwers, but can also indicate presence of problematic posterior olecranon osteophytes or medial soft tissue edema. Palpation along the medial epicondyle and proximal medial ulna, extending along the medial ulnar collateral ridge, should be performed as precisely as possible and separate from palpation of the common flexor pronator mass origin. In the author’s experience, particularly in the subacute setting, throwers with a significant injury to the UCL will exhibit marked tenderness at the site of injury—either proximally or distally.
The moving valgus stress test, which has been shown to have 100% sensitivity and 75% specificity, should be performed [21]. Static valgus stress testing (e.g., the “milking maneuver”), in contrast, has been shown to have a sensitivity of only 65% and specificity of 50% [21]. With the former, the examiner stands behind or to the affected side of the athlete and positions the athlete’s shoulder in maximal external rotation with the elbow flexed to at least 120°. Applying valgus stress, the examiner then extends the elbow. Pain in the arc from 120° to 70°—reflective of the most common degree of elbow flexion during the late cocking and early acceleration phases of throwing—is indicative of UCL injury (Fig. 3).

a, b Evaluation of valgus stability of the elbow via the moving valgus stress test with application of valgus stress while moving the athlete’s elbow through an arc from approximately 50° to 120° of flexion
Imaging
Magnetic resonance arthrography (MRA) remains the gold standard for evaluation of the UCL, demonstrating sensitivity as high as 92% and specificity as high as 100%, versus standard MR imaging (MRI), which demonstrates sensitivity of only 57% [22]. One particular finding to note is the “T-sign,” a finding on MRA in which arthrography dye is noted to extravasate distally between the sublime tubercle, proximal medial ulnar collateral ridge, and the overlying anterior bundle of the UCL (Fig. 4) [23]. This finding has been shown to have a sensitivity of up to 57% and specificity of up to 100%. Furthermore, to facilitate detection of partial thickness UCL tears, the elbow should be maintained in as full extension as possible during MR evaluation to tension the anterior bundle of the UCL [24].

Coronal T2 FS magnetic resonance arthrographic image of elbow demonstrating infiltration of dye between the sublime tubercle/medial collateral ligament ridge and the distal attachment of the anterior bundle of the medial collateral ligament (asterisk)
The addition of dynamic ultrasound, particularly in cases of partial thickness injury to the UCL, can add valuable information regarding the functional status of the ligament to help the treating physician accurately decide which injuries can be treated non-operatively and which may require repair or reconstruction [25]. In a dynamic ultrasound study using a cadaveric model, sectioning of the anterior band of the anterior bundle produced an average of 2.0 mm of medial gapping with valgus force, of the posterior band of the anterior bundle 1.4 mm, and of the entire anterior bundle 3.4 mm [26]. Sectioning of the remaining portion of the ligament (posterior and transverse bundles) produced a net increase of only 0.8 mm in valgus gapping. However, dynamic ultrasound findings should be interpreted in the context of history, physical exam, and MRA—particularly in the case of elite (collegiate and professional) overhead athletes—as a 10-year follow-up study of professional baseball players demonstrated a statistically significant increase in medial joint space gapping over time, even in asymptomatic pitchers [27]. One should note that when utilizing stress ultrasonography to evaluate the functional competency of the UCL, the elbow should be maintained at a flexion angle of 30° in order to mitigate the stabilizing effect of osteoarticular congruency [26].
As a final “imaging” modality, the treating surgeon can consider arthroscopic evaluation of medial ulnohumeral gapping while viewing from a lateral arthroscopic portal. However, given the necessity of maintain an elbow flexion angle of 30° during stress evaluation of the UCL, in the author’s experience, caring for a Major League Baseball team for over a decade, this has minimal practical value.
Treatment
Ulnar collateral ligament reconstruction (UCLR) remains the gold standard for treatment of acute full-thickness disruption of the anterior bundle of the UCL, as well as for chronic injuries that do not respond to non-operative treatment, with reported return-to-play (RTP) ranging from 80 to 94% depending on technique, graft choice, and a number of other factors [28,29,30]. A full discussion of UCLR techniques and outcomes is beyond the scope of this review article. However, for partial thickness injuries to the anterior bundle of the UCL, one may consider other options, including rehabilitation, orthobiologics, and potentially operative repair.
Historically, reported RTP rates for non-operatively treated UCL injuries have been extremely poor. Rettig et al. reported only 42% of athletes with UCL injuries were able to return to play after 3 months of rest followed by 3 months of rehabilitation [31]. More recently, however, Ford et al. reported on a large cohort of professional baseball players with UCL injuries ranging from partial to complete, and found among 31 players with partial injuries who completed a non-operative rehabilitation program, 84% returned to the same level of play or higher [32•]. In this study, one should note that careful attention was given to new versus chronic partial tears (chronic tears were weighted more towards UCLR) and rate of response to initial rehabilitation efforts. If a player did not respond to an initial 6–8 weeks of rehabilitation, then UCLR was considered.
The expanding body of data around and indications for orthobiologics such as platelet-rich plasma (PRP) and mesenchymal stem cell (MSC) therapy either via bone marrow aspirate concentrate (BMAC) or adipose-derived offers yet another adjunct tool for non-operative treatment of UCL injuries. Multiple authors have now reported RTP rates that exceed historical norms for partial thickness UCL injuries treated with a single PRP injection and structured rehabilitation followed by an interval throwing program [33•, 34, 35•]. Currently, there is no published clinical data to guide decision-making regarding the use of MSC’s in the context of UCL injuries, although studies are underway.
Non-augmented operative repair of partial or complete injuries to the anterior bundle of the UCL has been a controversial topic, with reported results ranging from 50 to 97% [36, 37]. More recently, synthetic augmentation during repair using a woven, high-strength, collagen-coated tape has been advocated with promising reported biomechanical results [38].
Medial Epicondylar Apophysitis and Avulsion Fractures
Avulsion of the medial epicondyle accounts for up to 12% of pediatric elbow fractures and typically occurs between the ages of 9 and 15 years when either a significant valgus force is applied to the adolescent elbow or as the result of chronic, repetitive stress that results from activities such as overhead throwing [6, 39]. The medial epicondyle represents a vital structure for valgus stability of the medial elbow, as both dynamic and static stabilizers attach to it.
History and Physical Exam
In cases of acute avulsion, the adolescent throwing athlete invariably presents with pain and swelling over the medial elbow along with a history recounting a distinct “pop” during a throwing motion. Examination will reveal tenderness of the medial epicondyle with a palpably mobile mass in acute cases with significant displacement. Secondary to the line of force of the common flexor pronator mass, the direction of displacement is slightly anterior and distal. In some cases, however, the adolescent throwing athlete may present with a more prolonged history of progressive medial-sided elbow pain. One should not dismiss this as “flexor tendonitis,” but rather assume until proven otherwise that the athlete is experiencing medial epicondylar apophysitis, commonly known as “Little Leaguer’s Elbow.”
Imaging
Plain radiographs suffice to characterize the presence of the fracture and degree of displacement for cases of acute avulsion. Four views, including two oblique radiographs, can assist with characterizing degree of displacement more accurately than a simple AP and lateral, given the position of the medial epicondyle slightly posterior to midline with respect to the humeral shaft and elbow axis of rotation [6]. For cases in which there is question about degree of displacement, advanced imaging such as MRI or computed tomography (CT) with 3-D reconstruction can be helpful, although the author tends to avoid CT in this young population when possible given long-term risks associated with radiation exposure. More advanced imaging may also be helpful with more chronic cases to detect edema in the region of the medial epicondylar apophysis. “Widening” of the apophysis may not be easily visualized on plain radiographs in more chronic cases.
Treatment
Broad consensus exists with respect to treatment of chronic cases of medial epicondylar apophysitis without avulsion. The athlete is restricted from throwing and any other activities that generate pain, typically for a period of 3 months. This may be a time during which a structured rehabilitation program focusing on correcting core strength and flexibility deficits, as well as glenohumeral internal rotation deficit (GIRD) and periscapular muscle activation may be of benefit. Following this period of rest, the athlete follows an interval return to throw program.
Furthermore, non-displaced fractures (< 2 mm) can be treated either with immobilization in a long-arm cast for 3 weeks for younger patients or in a hinged elbow brace for 4–6 weeks for older patients [6, 39]. For displaced fractures (> 5 mm), open reduction and internal fixation, typically using a single, partially threaded screw, may be considered to restore valgus stability to the medial elbow [40, 41].
Controversy exists, however, regarding treatment of minimally to moderately displaced, acute avulsions of the medial epicondyle with low-energy mechanisms, such as throwing. Nevertheless, for low-energy mechanisms, excellent results have been reported for fractures displaced an average of 5.3 mm with non-operative treatment. All patients in this study achieved bony union [42]. In the author’s practice, for low-energy mechanisms such as throwing, fractures displaced ≤ 5 mm typically are treated non-operatively and those displaced > 5 mm are treated with ORIF using a single cannulated, partially threaded screw and washer, followed by early, active range-of-motion (Fig. 5).

a Medial epicondylar avulsion with significant displacement in a skeletally immature athlete. b After fixation with single, partially threaded, cannulated screw
Valgus Extension Overload
First described in 1983 by Wilson et al., valgus extension overload (VEO) refers to a pathologic increase in mechanical load experienced by the posteriormedial aspect of the elbow joint during the late acceleration and follow-through phases of throwing (Fig. 6) [43]. The phrase, “valgus extension overload,” arose from the historical conceptualization that it was only at lower flexion angles during the late acceleration phase of throwing, i.e., extension, that valgus overload occurred. However, more recent data suggest that in the context of valgus laxity, mechanical overload can occur throughout a more extensive range-of-motion, giving rise to the possibly more accurate phrase of “ulnohumeral chondral and ligamentous overload” (UCLO). Furthermore, given the increasing contact pressure experienced by the posteromedial olecranon in biomechanical studies as the anterior bundle is sectioned, one must have a high degree of suspicion for clinically significant UCL injury when evaluating throwers with VEO [44, 45]. Although typically observed in adult throwers, VEO has also been reported in an adolescent population, albeit with perhaps a slightly different etiology than adult counterparts [46].

a, b Classic depiction of valgus extension overload (reprinted from [43], copyright © 1983 by SAGE Publications, Inc. Reprinted by Permission of SAGE Publications, Inc.)
History and Physical Exam
Throwers commonly present with a history of posterior or posteromedial elbow pain most prominent in the late acceleration and follow-through phases of throwing. If there is significant pain in late cocking phase as well, then one should suspect clinically significant injury to the UCL. The athlete often has a mild flexion contracture, direct tenderness to palpation over the posterior olecranon process, and may have a positive “bounce” test in which the elbow is rapidly brought from flexion to full extension with a snapping motion, reproducing the thrower’s symptoms [43].
Imaging
Plain radiographs may reveal a posterior osteophyte at the distal tip of the olecranon process. More detailed evaluation via CT may demonstrate that the osteophyte is fractured or bound to the olecranon by a fibrous bridge and may reveal additional osteocartilaginous loose bodies in the posterior joint space.
Treatment
A trial of activity restriction and rehabilitation may be attempted. However, with radiographic confirmation of the presence of a posteromedial osteophyte, often surgical treatment is required. With current arthroscopic techniques, good-to-excellent results have been reported with osteophyte excision [43, 46,47,48]. One must take care to resect only the osteophytic portion of the posterior olecranon and avoid resection of native bone to avoid increasing stress on the anterior bundle of the UCL [44, 45].
Olecranon Stress Fracture
Olecranon stress fracture (OSF) was first reported by Waris in a javelin thrower in 1946 [49]. The repetitive valgus load experienced by the olecranon process throughout the throwing motion is hypothesized to generate this rare injury [48, 50]. A high percentage of these cases may have concomitant, clinically relevant injury to the UCL, so as with evaluation of VEO, the clinician should maintain a high degree of suspicion [51].
History and Physical Exam
Not surprisingly given the similar mechanical etiology, athletes often present in a fashion similar to those with VEO, complaining of posteromedial pain during the late acceleration and follow-through phases of throwing [52].
Physical exam often reveals tenderness to palpation and percussion along the proximal ulna and olecranon process. Similar to VEO, a mild flexion contracture and a positive “bounce” test may be present.
Imaging
In the early phases of this process, when there is no overt fracture, plain radiographs are often unremarkable with the exception of the possible presence of a posterior olecranon osteophyte. Late in the evolution of OSF, one may be able to identify a lucency within the proximal ulna or olecranon consistent with a stress fracture rather than a stress reaction. MRI is essential to making this diagnosis early in the process.
Furushima et al. proposed classifying OSF into five categories: physeal, classic, transitional, sclerotic, and distal, with the physeal type being the most common in their series at 50.5% of those presenting with this injury, which included a number of skeletally immature athletes [53]. In another study looking only at adult baseball players, the most common fracture pattern observed was oblique, running from proximal-medial to distal-lateral [51].
Treatment
Particularly when caught early (in the stress reaction phase of this injury), one can expect non-operative treatment to be successful. Schickendantz et al. reported on seven professional baseball players with MRI-detected stress reactions—without changes on plain radiographs—six of whom returned to their previous level of play following a period of activity restriction followed by an interval throwing program [52].
Once a fracture line is visible on plain radiographs or CT, operative fixation may be required, which can typically be accomplished using a cannulated screw placed perpendicular to the fracture plane [51]. In the author’s experience, autogenous local bone grafting may be beneficial in larger, more chronic, stress fractures in order to optimize the biologic as well as the mechanical milieu (Fig. 7).

a Olecranon stress fracture (asterisk) demonstrated on coronal T2 FS magnetic resonance image of elbow. b After fixation with axial compression screw and tension band construct
Ulnar Nerve
Pathology of the ulnar nerve has been reported in conjunction with valgus instability of the elbow in the throwing athlete, as well as secondary to intrinsic nerve instability, impingement via extrinsic osteophytes, flexor muscle hypertrophy, snapping medial head of the triceps, and presence of an accessory anconeus epitrochlearis [20, 54,55,56]. As it can lead to loss of “touch” and dexterity in the affected hand, ulnar nerve pathology can have significant adverse effects on performance in the throwing athlete.
History and Physical Exam
Throwing athletes with pathology affecting the ulnar nerve may present with complaints of numbness, tingling, or burning along the medial elbow and forearm, extending in to the small and ring fingers, often exacerbated by repetitive throwing [57]. In advanced cases, with motor involvement, athletes may describe weakness in grip strength, loss of manual dexterity, and a decrease in ability to control movement in their pitches. Throwers with mechanical subluxation of the ulnar nerve frequently report a “popping” or “snapping” sensation along the medial elbow as they move from flexion to extension with valgus stress (e.g., throwing).
Physical exam should include evaluation of the cervical spine to rule out a “double crush syndrome” in which there is proximal compression of the C8 and or T1 nerve roots along with distal compression of the ulnar nerve. A Tinel’s sign should be sought along the course of the ulnar nerve from the mid-medial brachium through the medial proximal forearm. Subluxation of the ulnar nerve from the cubital tunnel across the medial epicondyle as the elbow is brought from full flexion to extension while applying a valgus force, which can be present in up to 16% of individuals, should be evaluated [58]. A flexion-supination test should be performed in which the athlete’s elbow is hyperflexed while supinating the forearm and flexing the wrist. Exacerbation of the patient’s symptoms in this position indicates a positive test. Finally, in more advanced cases, a Froment’s sign may be present, in which the athlete demonstrates intrinsic weakness relative to the contralateral extremity when attempting to prevent the examiner from pulling free a piece of paper held between the thumb and index finger.
Imaging
Plain radiographs may reveal impinging osteophytes along the medial elbow and MRI can be helpful for identifying concomitant pathology of the UCL, as well as identifying extrinsic causes of compression such as an accessory medial head of the triceps (Fig. 8) or an anconeus epitrochlearis, which can be present in up to 25% of patients with ulnar nerve symptoms [20]. Dynamic ultrasound may also be useful when evaluating stability of the nerve, as well as fusiform swelling, which may indicate compression at a specific site.

Accessory medial head of the triceps (arrow) generating medial elbow “snapping” and compression of the ulnar nerve (asterisk)
EMG should be obtained, but can have a high false-negative rate in the throwing athlete, up to 10% [59]. Nevertheless, EMG can prove useful for localizing the site of compression when surgical intervention is contemplated.
Treatment
Early-stage ulnar nerve pathology may respond favorably to activity modification and physical therapy that targets nerve mobility, as well as the pectoralis minor and thoracic outlet as potential additional, more proximal sources of nerve compression. Modalities such as iontophoresis may also be effective in early stages by reducing inflammation.
In cases of mechanical instability or in compressive cases refractory to non-operative measures, operative treatment in the form of decompression or transposition may be indicated. Transposition in which the course of the ulnar nerve is altered to run anterior (rather than posterior) to the medial epicondyle may be performed in one of the three manners: subcutaneous, submuscular, and intramuscular. The intramuscular technique is largely of historical interest and reported results for RTP in throwers have been poor for the submuscular technique [60]. However, rates of 88–100% RTP have been reported following subcutaneous nerve transposition [61].
Flexor-Pronator Mass Injury
The muscle group originating from the medial epicondyle, to which providers commonly refer as the “common flexor-pronator mass” (CFPM), comprises five distinct muscles: the pronator teres (PT), flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), flexor digitorum superficialis (FDS), and the palmaris longus (PL). Of these, from a biomechanical perspective, the FCU and FDS assume a vector of action that could theoretically provide support congruent with that supplied by the UCL during episodes of valgus force across the elbow. However, EMG studies—including one examining baseball pitchers with UCL deficiency—have failed to demonstrate increased FCU/FDS activation during periods of increased valgus force across the elbow, calling into question a significant supporting role for this musculature [12]. Nevertheless, overuse injuries and strains of the common flexor pronator mass can occur in the overhead population and produce clinically significant medial elbow pain. As an additional note, one should consider that CFPM pathology is exceedingly rare in a skeletally immature population, and one should instead suspect irritation of the medical epicondylar physis.
History and Physical Exam
Overhead athletes with injury to the CFPM may present with symptoms similar to those observed with injury to the UCL: medial-sided elbow pain predominantly during the late cocking and early acceleration phases of the throwing cycle. Unlike UCL injuries, however, in my experience with professional and other elite level overhead throwing athletes, those with CFPM pathology typically complain of medial elbow discomfort during a wider range of activities than those with UCL injuries. Those with CFPM pathology can experience pain with virtually any activity that activates this muscle group, including carrying an equipment bag, turning a doorknob, or opening a jar! Nevertheless, particularly with acute-onset cases, one must maintain a high degree of suspicion for UCL injury.
Physical exam, in my experience, can be useful in differentiating between cases of simple CFPM injury/irritation and UCL pathology. Athletes with simple CFPM injury commonly exhibit tenderness to palpation approximately 1 cm distal to the CFPM origin at the medial epicondyle along a line almost directly orthogonal to the anterior aspect of the epicondyle. Individuals with injury to the anterior band of the UCL typically exhibit tenderness posterior to this location and along the more inferior aspect of the epicondyle. Furthermore, muscle activation tests such as resisted pronation and wrist flexion will commonly reproduce symptoms in athletes with CFPM pathology whereas they provoke marginal reaction in those with UCL injury.
Imaging
In an elite overhead throwing population, I have a low threshold for obtaining advanced imaging, primarily to confirm that the UCL is not involved. Nevertheless, in a non-professional population without seasonal pressure for initiation of a return to throw program, I will often forego advanced imaging if the history and physical exam are classic for CFPM injury, proceed with rehabilitation, and obtain advanced imaging (e.g., MRA) only in those athletes who do not respond to appropriate therapy.
Treatment
For true, isolated CFPM injuries, a period of “active” rest (rest from throwing, but with implementation of rehabilitative exercises) ranging from 2 to 4 weeks, non-steroidal anti-inflammatory medication and eccentric strengthening, followed by a structured return-to-throwing program, is almost universally successful in allowing the athlete to return to play. Persistence of symptoms beyond 4 to 6 weeks or frequent recurrence of symptoms should prompt increased suspicion of underlying structural damage to the CFPM origin or UCL pathology, and advanced imaging should be obtained.
Conclusion
When evaluating the throwing athlete who presents with activity-related, medial-sided elbow pain, one must maintain a healthy suspicion for UCL pathology, but must also consider concomitant or alternate pathologies such as valgus extension overload, olecranon stress fracture, ulnar nerve compression or instability, medial epicondylar apophysitis in the skeletally immature, and injury to the common flexor pronator mass. With appropriate history, physical exam, and implementation of diagnostic imaging, accurate diagnosis can be achieved and effective treatment provided.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Conte S, Requa RK, Garrick JG. Disability days in major league baseball. Am J Sports Med. 2001;29(4):431–6.
Posner M, Cameron KL, Wolf JM, Belmont PJ, Owens BD. Epidemiology of major league baseball injuries. Am J Sports Med. 2011;39(8):1676–80.
• Ciccotti MG, Pollack KM, Ciccotti MC, et al. Elbow injuries in professional baseball: epidemiological findings from the major league baseball injury surveillance system. Am J Sports Med. 2017;45(10):2319–28 Excellent, up-to-date review of the epidemiology of elbow injuries in Major League Baseball.
Morrey BF. Anatomy of the elbow joint. In: Morrey BF, Sanchez-Sotelo J, editors. The elbow and its disorders. Philadelphia, PA: Saunders Elsevier; 2009. p. 11–38.
An KN, Zobitz ME, Morrey BF. Biomechanics of the elbow. In: Morrey BF, Sanchez-Sotelo J, editors. The elbow and its disorders. Philadelphia, PA: Saunders Elsevier; 2009. p. 39–63.
Peterson H. Physeal fractures of the elbow. In: Morrey BF, Sanchez-Sotelo J, editors. The elbow and it’s disorders. Philadelphia, PA: Saunders Elsevier; 2009. p. 246–67.
Silberstein MJ, Brodeur AE, Graviss ER, Luisiri A. Some vagaries of the medial epicondyle. J Bone Joint Surg Am. 1981;63(4):524–8.
• Frangiamore SJ, Moatshe G, Kruckeberg BM, et al. Qualitative and quantitative analyses of the dynamic and static stabilizers of the medial elbow: an anatomic study. Am J Sports Med. 2018;46(3):687–694. Precise, biomechanical analysis of the anterior bundle of the UCLUCL, looking at the clinical significant of injuries to different parts of the complex.
Camp CL, Jahandar H, Sinatro AM, Imhauser CW, Altchek DW, Dines JS. Paper #15—quantitative anatomic analysis of the medial ulnar collateral ligament complex of the elbow with implications for reconstructive surgery. J Shoulder Elb Surg. 2018;27(4):e127.
Farrow LD, Mahoney AJ, Stefancin JJ, Taljanovic MS, Sheppard JE, Schickendantz MS. Quantitative analysis of the medial ulnar collateral ligament ulnar footprint and its relationship to the ulnar sublime tubercle. Am J Sports Med. 1936;2011(39):1941.
Lin F, Kohli N, Perlmutter S, Lim D, Nuber GW, Makhsous M. Muscle contribution to elbow joint valgus stability. J Shoulder Elb Surg. 2007;16(6):795–802.
Hamilton CD, Glousman RE, Jobe FW, Brault J, Pink M, Perry J. Dynamic stability of the elbow: electromyographic analysis of the flexor pronator group and the extensor group in pitchers with valgus instability. J Shoulder Elb Surg. 1996;5(5):347–54.
Masear VR, Meyer RD, Pichora DR. Surgical anatomy of the medial antebrachial cutaneous nerve. J Hand Surg Am. 1989;14(2 Pt 1):267–71.
• Cesmebasi A, O’driscoll SW, Smith J, Skinner JA, Spinner RJ. The snapping medial antebrachial cutaneous nerve. Clin Anat. 2015;28(7):872–7 Interesting report on a novel neurologic source of medial elbow pain.
Pribyl CR, Kester MA, Cook SD, Edmunds JO, Brunet ME. The effect of the radial head and prosthetic radial head replacement on resisting valgus stress at the elbow. Orthopedics. 1986;9(5):723–6.
Morrey BF, An KN. Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med. 1983;11(5):315–9.
Sojbjerg JO, Ovesen J, Nielsen S. Experimental elbow instability after transection of the medial collateral ligament. Clin Orthop Relat Res. 1987;218:186–90.
Callaway GH, Field LD, Deng XH, et al. Biomechanical evaluation of the medial collateral ligament of the elbow. J Bone Joint Surg Am. 1997;79(8):1223–31.
Schwab GH, Bennett JB, Woods GW, Tullos HS. Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop Relat Res. 1980;146:42–52.
O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br. 1991;73(4):613–7.
O’Driscoll SW, Lawton RL, Smith AM. The “moving valgus stress test” for medial collateral ligament tears of the elbow. Am J Sports Med. 2005;33(2):231–9.
Magee T. Accuracy of 3-T MR arthrography versus conventional 3-T MRI of elbow tendons and ligaments compared with surgery. AJR Am J Roentgenol. 2015;204(1):70.
Timmerman LA, Schwartz ML, Andrews JR. Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography. Evaluation in 25 baseball players with surgical confirmation. Am J Sports Med. 1994;22(1):31 discussion 32, 26.
Schreiber JJ, Potter HG, Warren RF, Hotchkiss RN, Daluiski A. Magnetic resonance imaging findings in acute elbow dislocation: insight into mechanism. J Hand Surg Am. 2014;39(2):199–205.
Kim NR, Moon SG, Park J, Choi JW, Oh K. Stress ultrasound in baseball players with ulnar collateral ligament injuries: additional value for predicting rehabilitation outcome. J Shoulder Elb Surg. 2017;26(5):815–23.
Ciccotti MC, Hammoud S, Dodson CC, Cohen SB, Nazarian LN, Ciccotti MG. Stress ultrasound evaluation of medial elbow instability in a cadaveric model. Am J Sports Med. 2014;42(10):2463–9.
Ciccotti MG, Atanda A, Nazarian LN, Dodson CC, Holmes L, Cohen SB. Stress sonography of the ulnar collateral ligament of the elbow in professional baseball pitchers: a 10-year study. Am J Sports Med. 2014;42(3):544–51.
Erickson BJ, Bach BR, Cohen MS, et al. Ulnar collateral ligament reconstruction: the rush experience. Orthop J Sports Med. 2016;4(1):2325967115626876 232596711562687.
Savoie FH, Morgan C, Yaste J, Hurt J, Field L. Medial ulnar collateral ligament reconstruction using hamstring allograft in overhead throwing athletes. J Bone Joint Surg Am. 2013;95(12):1062–6.
Cain EL, Andrews JR, Dugas JR, Wilk KE, McMichael CS, Walter JC II, et al. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010;38(12):2426–34.
Rettig AC, Sherrill C, Snead DS, Mendler JC, Mieling P. Nonoperative treatment of ulnar collateral ligament injuries in throwing athletes. Am J Sports Med. 2001;29(1):15–7.
• Ford GM, Genuario J, Kinkartz J, Githens T, Noonan T. Return-to-play outcomes in professional baseball players after medial ulnar collateral ligament injuries: comparison of operative versus nonoperative treatment based on magnetic resonance imaging findings. Am J Sports Med. 2016;44(3):723–8 Interesting look at the success/failure of non-operative treatment of varying degrees of UCLUCL injury in professional baseball players.
• Dines JS, Williams PN, ElAttrache N, et al. Platelet-rich plasma can be used to successfully treat elbow ulnar collateral ligament insufficiency in high-level throwers. Am J Orthop (Belle Mead NJ). 2016;45(5):296–300 Early data supporting use of orthobiologics in the setting of non-operative treatment of UCLUCL injuries in overhead throwers.
Deal JB, Smith E, Heard W, O’Brien MJ, Savoie FH. Platelet-rich plasma for primary treatment of partial ulnar collateral ligament tears: MRI correlation with results. Orthop J Sports Med. 2017;5(11):2325967117738238 Accessed Sep 29, 2018.
• Podesta L, Crow SA, Volkmer D, Bert T, Yocum LA. Treatment of partial ulnar collateral ligament tears in the elbow with platelet-rich plasma. Am J Sports Med. 2013;41(7):1689–94 Accessed Sep 29, 2018. Early data supporting use of orthobiologics in the setting of non-operative treatment of UCLUCL injuries in overhead throwers.
Savoie FH, Trenhaile SW, Roberts J, Field LD, Ramsey JR. Primary repair of ulnar collateral ligament injuries of the elbow in young athletes: a case series of injuries to the proximal and distal ends of the ligament. Am J Sports Med. 2008;36(6):1066–72.
Conway JE, Jobe FW, Glousman RE, Pink M. Medial instability of the elbow in throwing athletes. Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am. 1992;74(1):67–83.
Dugas JR, Walters BL, Beason DP, Fleisig GS, Chronister JE. Biomechanical comparison of ulnar collateral ligament repair with internal bracing versus modified Jobe reconstruction. Am J Sports Med. 2016;44(3):735–41.
Wilkins K. Fractures involving the medial epicondylar apophysis. In: Rockwood CJ, Wilkins K, King R, editors. Fractures in children. Phladelphia, PA: JB Lippincott. p. 509–28.
Patel NM, Ganley TJ. Medial epicondyle fractures of the humerus: how to evaluate and when to operate. J Pediatr Orthop. 2012;32(Suppl 1):10.
Case SL, Hennrikus WL. Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med. 1997;25(5):682–6.
Lawrence JTR, Patel NM, Macknin J, Flynn JM, Cameron D, Wolfgruber HC, et al. Return to competitive sports after medial epicondyle fractures in adolescent athletes. Am J Sports Med. 2013;41(5):1152–7.
Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983;11(2):83–8.
Osbahr DC, Dines JS, Breazeale NM, Deng XH, Altchek DW. Ulnohumeral chondral and ligamentous overload: biomechanical correlation for posteromedial chondromalacia of the elbow in throwing athletes. Am J Sports Med. 2010;38(12):2535–41.
Ahmad CS, Park MC, Elattrache NS. Elbow medial ulnar collateral ligament insufficiency alters posteromedial olecranon contact. Am J Sports Med. 2004;32(7):1607–12.
Park JY, Yoo HY, Chung SW, Lee SJ, Kim NR, Ki SY, et al. Valgus extension overload syndrome in adolescent baseball players: clinical characteristics and surgical outcomes. J Shoulder Elb Surg. 2016;25(12):2048–56.
Cohen SB, Valko C, Zoga A, Dodson CC, Ciccotti MG. Posteromedial elbow impingement: magnetic resonance imaging findings in overhead throwing athletes and results of arthroscopic treatment. Arthroscopy. 2011;27(10):1364–70.
Ahmad CS, ElAttrache NS. Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med. 2004;23(4):76 x.
Waris W. Elbow injuries of javelin-throwers. Acta Chir Scand. 1946;93(6):563–75.
Suzuki K, Minami A, Suenaga N, Kondoh M. Oblique stress fracture of the olecranon in baseball pitchers. J Shoulder Elb Surg. 1997;6(5):491–4.
Paci JM, Dugas JR, Guy JA, Cain EL Jr, Fleisig GS, Hurst C, et al. Cannulated screw fixation of refractory olecranon stress fractures with and without associated injuries allows a return to baseball. Am J Sports Med. 2013;41(2):306–12.
Schickendantz MS, Ho CP, Koh J. Stress injury of the proximal ulna in professional baseball players. Am J Sports Med. 2002;30(5):737–41.
Furushima K, Itoh Y, Iwabu S, Yamamoto Y, Koga R, Shimizu M. Classification of olecranon stress fractures in baseball players. Am J Sports Med. 2014;42(6):1343–51.
Treihaft MM. Neurologic injuries in baseball players. Semin Neurol. 2000;20(2):187–93.
Keefe DT, Lintner DM. Nerve injuries in the throwing elbow. Clin Sports Med. 2004;23(4):42 xi.
Spinner RJ, O’Driscoll SW, Jupiter JB, Goldner RD. Unrecognized dislocation of the medial portion of the triceps: another cause of failed ulnar nerve transposition. J Neurosurg. 2000;92(1):52–7.
Conti MS, Camp CL, Elattrache NS, Altchek DW, Dines JS. Treatment of the ulnar nerve for overhead throwing athletes undergoing ulnar collateral ligament reconstruction. World J Orthop. 2016;7(10):650–6.
Childress HM. Recurrent ulnar-nerve dislocation at the elbow. Clin Orthop Relat Res. 1975;108:168–73.
Zemel NP. Ulnar neuropathy with and without elbow instability. Hand Clin. 2000;16(3):95 x.
Del Pizzo W, Jobe FW, Norwood L. Ulnar nerve entrapment syndrome in baseball players. Am J Sports Med. 1977;5(5):182–5.
Rettig AC, Ebben JR. Anterior subcutaneous transfer of the ulnar nerve in the athlete. Am J Sports Med. 1993;21(6):40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
L. Pearce McCarty has received consulting fees and speaker honorarium from Anthrex Inc. and is a principle investigator in an industry sponsored study funded by Biomet.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Injuries in Overhead Athletes
Rights and permissions
About this article

Cite this article
Pearce McCarty, L. Approach to Medial Elbow Pain in the Throwing Athlete. Curr Rev Musculoskelet Med 12, 30–40 (2019). https://doi.org/10.1007/s12178-019-09534-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12178-019-09534-w