
Abstract
Arthrometry and stress imaging are useful clinical tools for the objective assessment of anterior cruciate ligament (ACL) integrity. They are most frequently used for the diagnosis of a complete ACL tear when other workup is equivocal, in conjunction with history and clinical exam findings. Other applications include the diagnosis of partial ACL tears, injury prognosis, and post-operative monitoring. However, further studies are needed to validate these uses. Many different devices and techniques exist for objective examination, which have been compared in recent literature. Reliability and validity measures of these methods vary, and often depend upon examiner familiarity and skill. The KT series of devices is the current gold standard for arthrometry, although the newer robotic GNRB device shows promising early results. Newer methods of data interpretation have been developed for stress imaging, and portable technology may impact this field further.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Accurate assessment of knee laxity is critical for many steps in the management of anterior cruciate ligament (ACL) injury. Classic physical exam maneuvers, while essential, depend on subjective factors such as clinician experience, muscle relaxation, and inherent knee variability. Advanced imaging such as MRI is expensive and cannot directly evaluate instability. Therefore, objective assessment of joint laxity, or “laximetry,” is often desired to supplement physical exam findings. Broadly, the two types of laximetry are stress imaging and arthrometry, both of which quantify the knee displacement resulting from an applied force.
Both techniques have evolved since their introduction 30–40 years ago. Clinically, laximetry is best defined as a dichotomous tool for diagnostic purposes, used in combination with physical exam maneuvers. In addition, many groups have sought to harness laximetry’s quantitative properties for prognostic purposes or to monitor post-operative laxity. These applications currently have less clear support in the literature, although a recent study suggests that objective evaluation of the uninjured knee can aid in the prognosis of ACL reconstructive surgery. Laximetry is also useful in research, since its quantitative properties allow objective evaluation and comparison of different factors such as surgical techniques or rehabilitation regimens.
Major recent developments include the introduction of a robotic arthrometer, designed to improve the objectivity of arthrometry. There are also ongoing attempts to validate laximetry results in the clinical setting and to systematically compare the many existing techniques and protocols.
Stress radiography
Stress radiography is a non-invasive method of visual observation and quantification of knee joint laxity in response to an applied stress. For ACL injury, this is typically measured in the anteroposterior plane, although techniques do exist for evaluating rotational and varus/valgus laxity [1••]. Generally, a “baseline” resting lateral knee X-ray (XR) is obtained and compared to an analogous image obtained with force applied to the knee. The level of anteroposterior knee laxity is inferred from the changing tibiofemoral relationship.
The diagnostic value of stress imaging as compared to clinical exam or MRI is unclear, and it is therefore recommended as a diagnostic adjunct rather than a stand-alone tool [2–4]. The highest diagnostic ability is obtained by combining stress imaging with these methods [5].
Several imaging protocols exist, with a recent article reviewing 12 techniques described in the literature [1••]. The Telos device (Austin & Associates, Fallston, Maryland) is a highly reproducible means of producing knee stress for imaging and has achieved widespread use. Clinicians should adopt a consistent testing regimen and should not assume that the results of different protocols are comparable.
Choice of landmarks
Multiple landmarks can be used to define the tibial and femoral position. Ideally, landmarks should be easily and unequivocally identifiable, and should not be highly dependent on subtle changes in knee rotation or flexion. Theoretically, posterior landmarks are the least dependent on knee flexion, since the center of knee flexion lies posterior to the midshaft axis [6–8]. Central landmarks are the least dependent on axial knee rotation, since they again are nearest to the center of rotational motion. Some investigators choose landmarks which evaluate translation in one knee compartment (i.e., medial or lateral), while others select midline landmarks which represent overall tibial translation. The lateral knee compartment has consistently shown higher anterior laxity in both normal and injured knees, and investigators have found better reliability in measuring the medial compartment [9–12].
Landmarks for defining femoral position include the posterior-most aspect of the lateral femoral condyle (LFC), the posterior-most medial femoral condyle (MFC), or the midpoint between the two as seen on lateral XR. Other studies have used central landmarks, such as the posterior-most aspect of Blumensaat’s line, or the central femoral axis. Studies which position the knee in 90° of flexion will often use the anterior-most aspect of the respective femoral condyle. After a femoral landmark is chosen, typically a line is drawn tangential to the landmark and extended distally in a direction perpendicular to the tibial plateau, to allow for comparison to the tibial landmark.
Landmarks for defining tibial position on lateral XR include the posterior-most aspect of the lateral tibial plateau, the posterior-most medial tibial plateau, or the midpoint between the two. Other alternatives include the posterior fibular head, the medial intracondylar eminence, central tibial axis, or the anterior-most aspect of the tibial plateau.
Several studies have compared different landmarks used in stress imaging. In a study by Lee et al., a method using the posterior Blumensaat’s line and the anterior tibial plateau showed the best inter-rater and intra-rater reliability, with an intraclass correlation coefficient between 0.891 and 0.963 [6]. Wirz et al. also compared multiple measurement protocols, specifically examining the effect of rotation and flexion on landmark position and reliability, as these represent common positioning errors [7]. They found that a “central-peripheral” method was most consistent despite rotation or flexion—this method used the central tibial axis, compared to a parallel line positioned midway between the posterior aspects of both femoral condyles. The tibial eminence was a relatively inconsistent landmark and was not recommended for use.
Patient positioning
Knee laxity is dependent on positioning, as the degree of flexion influences the activity of different anatomical restraints. An ideal position should isolate the ACL; this is typically found at roughly 20° of flexion, similar to the position used to perform a Lachman’s test. In the majority of studies that describe passive stress imaging, the knee is positioned in 20° of flexion, typically with the patient in a decubitus position lying on the affected side. However, studies have described using knee flexion ranging from 0° to 90°.
Active stress imaging can also be performed using a number of different techniques. The quadriceps contraction technique was first described by DeJour et al. in 1988, and involves positioning the patient supine with the knee initially placed over a triangle [13]. For the image, the patient then fires the quadriceps and extends the leg fully, lifting it into the air. The extensor mechanism, in addition to extending the leg, will translate the tibia anteriorly, and this translation is compared between the two limbs. Another active technique is the lateral monopedal stance, also described by DeJour et al. [14]. The patient stands only on the leg to be imaged, with the knee flexed 20°. In this position, the tibia will translate anteriorly, the degree to which was found to be dependent on the tibial plateau posterior slope. Although this method was initially thought to be desirable due to the physiologically relevant position, it was found to be less sensitive than stress imaging using a manual Lachman maneuver in diagnosing ACL rupture.
Force application
The force used in stress imaging should be reproducible, gentle to the patient, and adequate to produce maximal translation. This can be performed using passive means, in which an extrinsic force is applied to the patient, or active means, in which the patient produces the translating force through muscle contraction. While active means are attractive due to their physiological mechanism, they generally are more patient-dependent and are less reproducible.
Several passive techniques have been described. Most simply, some authors perform a manual Lachman test during imaging. Another simple technique involves placing a sandbag onto the patient’s leg in an appropriate position, typically weighing anywhere from 3 to 9 kg [9, 11, 15]. The Telos apparatus is also commonly used [2, 5, 16–19]. This is a device which holds the femur and tibia in a fixed position, and then applies a reproducible force to the posterior tibia, producing anterior tibial translation. Most authors use 150 N of force, roughly equivalent to 15 kg, but different protocols use anywhere from 50 to 250 N [2, 6, 7, 16].
The baseline for measurement should also be consistent. Some groups simply use the resting knee position, whereas others initially apply a posterior force, thus obtaining the full anteroposterior laxity. PCL integrity obviously can impact this measurement and should always be considered.
Active techniques, as previously mentioned, use the patient’s own musculature to produce tibial translation. Typically, this involves a full quadriceps contraction, or enough contraction to position the knee in 20° flexion in a standing position [12, 14]. Obviously these forces cannot be standardized between patients and may be less useful for research purposes. However, they may be more functionally relevant in the clinical setting as they involve the patient’s own musculature. Comparative studies have found easier testing protocols and higher diagnostic value using passive methods [18].
Methods of quantification
Most investigators prefer comparing the affected knee to the unaffected knee, obtaining a “side-to-side difference” (SSD) measurement of increased laxity. Normal SSD is near zero [20]. Different diagnostic thresholds have been reported in the literature ranging from SSD of 2 to 5 mm [14, 17, 21]. In patients with complete ACL tear, Panisset et al. found average SSD to be 7.4 ± 4.3 mm and used SSD >5 mm as their diagnostic threshold using Telos stress imaging (Sn 80.9 %, sp 81.8 %) [5]. Beldame et al. instead used a diagnostic threshold of 4 mm with Telos stress imaging (Son 59 %, Sp 90 %) [2]. Most investigators have found higher diagnostic reliability and validity with medial compartment laxity, as opposed to the lateral compartment [9, 14].
Single-knee absolute translation is the simplest measurement to obtain, and limits overall radiation exposure. However, inherent knee laxity differs between patients, making these results less accurate. A study of normal patients with the Telos device found an average normal knee anterior laxity of 1.76 ± 0.33 mm [22•]. Lerat et al. suggested a 6-mm diagnostic threshold for absolute laxity measurements of the medial compartment using Telos stress imaging [9].
Rotational stress imaging
Classic stress imaging cannot evaluate rotational instability, a significant criticism of this technique. Although some groups have described rotational stress imaging techniques, this has not yet been well-validated and is not widespread in clinical practice or research [23, 24].
Arthrometry
Arthrometers are devices designed to apply a reproducible force across the knee and mechanically measure the resulting displacement. Advantages include a relatively simple and quick clinical technique, increased objectivity compared to simple clinical exam, and a lack of radiation exposure. Many devices have been developed, although only a few have entered widespread clinical practice. Testing techniques differ somewhat for each device, and there are also several described methods of data interpretation.
Devices
KT-1000/KT-2000
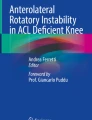
The KT series of arthrometers are the most highly studied and widely used arthrometers in orthopedic practice, and are largely considered a gold standard for laximetry. The original KT-1000 Knee Ligament Arthrometer (MEDmetric Corp, San Diego, CA, USA) was introduced in 1982 and first reported in 1985 [25, 26]. The patient is positioned supine with the knee flexed, and the KT-1000 is attached to the patient’s leg as shown in Fig. 1. Forces can be applied to the tibia either manually or by using a force-quantifying handle. The examiner first “zeroes” the probe at the maximal posterior displacement, and then applies anterior force to the tibia, recording the maximal anterior translation. The KT-2000 adds a two-dimensional display which can produce a force-displacement curve [25].

The KT-1000 arthrometer as positioned on a subject. The device is centered over the patella, with two straps around the tibia providing stability. Two probes extend to the anterior patella and proximal tibia, recording the tibial position relative to the patella
The diagnostic validity of KT arthrometry has been the focus of much scrutiny and some criticism, although the literature is generally supportive [25, 27–30]. It is important to note that diagnostic sensitivity and specificity vary with the testing protocol, the method of data interpretation, and the diagnostic threshold used. Several groups have found that higher applied forces improve diagnostic ability [31••, 32]. In their comparative meta-analysis, Van Eck et al. found generally good validity measures, with improvement as the applied forces increased from 69 N (Avg Sn 54 % [range 0.24–0.84]), to 89 N (Sn 73 % [60–100 %], Sp 92 % [67–100 %]), to maximum manual force (Sn 93 % [88–100 %], Sp 91 % [87–100 %]) [31••].
The reliability of KT-1000 measurement has also been questioned, and the literature overall is more inconclusive. However, in subjects with an intact ACL, the reliability is generally good, with intra-rater correlations ranging from 0.83 to 0.97 [33–38] and inter-tester correlations ranging from 0.41 to 0.92 [33, 34, 37–40].
In ACL-deficient patients, the literature is more limited and equivocal. Forster et al. initially warned of significant test-retest discrepancies, inter- and intra-surgeon variation, as well as significant differences depending on anesthesia [29]. Measurements are often only reproducible within a few millimeters, which can skew results given that diagnostic thresholds are typically 2–3 mm [41]. Developers of the International Knee Documentation Committee (IKDC) form, designed to be a comprehensive evaluation of knee function, recognized this fact [42]. While their new form required data such as subjective symptoms, manual examination, and functional testing, it only included objective laxity assessment as an optional supplement. The developers cited measurement error, cost, time, and limitation to the anteroposterior plane in their reasoning. Wiertsema et al. were also critical, finding the KT-1000 inferior to the Lachman test in both intra-rater (ICC = 1.0 vs. 0.47) and inter-rater (ICC = 0.77 vs. 0.14) reliability, even with experienced KT-1000 users [43]. The few other published reliability measures vary, with intra-rater reliability ranging from 0.67 to 0.99 and inter-rater reliability ranging from 0.65 to 0.92 [37, 40, 44]. Many factors influence test reliability, including examiner experience, device over-tightening, improper positioning, inconsistent force application, leg external/internal rotation, examiner hand dominance, and knee effusions [34, 39, 40, 44–49]. Although only explicitly studied with the KT system, several of these factors could conceivably affect other devices as well.
GNRB
The GNRB (Genourob, Laval, France) was first described in 2009 and has been a major focus of arthrometry literature in the past 3 years. It is a robotic arthrometer designed to avoid operator-dependent and relaxation-dependent error. The patient’s leg is placed in 20° knee flexion with restraints at the patella and ankle. Pre-defined force is applied to the posterior proximal calf by a mechanical jack, and a probe measures the resulting displacement of the proximal anterior tibia. Electrodes over the posterior thigh are designed to account for the effects of incomplete hamstring relaxation [50].
Several groups have found GNRB reliability to be superior to other arthrometers, which they attributed to the higher-precision translation probe and the automated force application [22•, 50, 51]. However, the literature is not unequivocal, with Vauhnik et al. finding lower intra-rater and inter-rater reliability [52, 53].
Diagnostic validity measures are comparable to other devices, and again depend on the test protocol used. Robert et al. found moderate test sensitivity (Sn 70 %, Sp 99 %) using 134 N force at 20° of knee flexion and a 3-mm SSD diagnostic threshold [50]. Klouche et al. found better sensitivity (Sn 92 %, Sp 98 %) using 200 N force with a 1.9-mm SSD diagnostic threshold. Other groups found more moderate results (Sn 62 %, Sp 76 % at 1.5 mm SSD threshold) [18]. One group also found the GNRB useful for partial tears (Sn 84 %, Sp 81 % at 2.5 mm SSD threshold) [54•].
Rolimeter
The Rolimeter (Aircast Europa, Neubeuern, Germany) is another common device used to quantify anteroposterior knee laxity. The device similarly attaches to the patella and the distal tibia, with a probe that rests on the tibial tuberosity. The clinician then performs a manual Lachman test, and the maximal displacement of this probe is recorded [55]. The skill and consistency of the examiner are crucial, as there is no means of standardizing the force or technique applied.
Reliability measures have been moderately high, but possibly dependent on examiner skill. Hatcher et al. found inter-rater reliability of 0.91–0.95 by a range of skill levels [56]. Muellner found reliability of 0.71–0.90 in experienced testers, but worse in novices [57]. Papandreou found varying inter-rater reliability of 0.55–0.96, which they attributed to the inherent subjectivity of the testing method [58].
Intra-rater reliability is also moderately good but variable. Several groups have published their results, ranging from 0.24, 0.55–0.72, to 0.49–1.0 [57–59]. Again, investigators cited inherent subjectivity in explaining this variability.
The little evidence that exists for the Rolimeter’s validity is promising. In a study of 50 normal and 46 ACL-deficient knees, sensitivity was 93 % and specificity 87 % in detecting ACL tears [60].
Other devices
Several additional arthrometers have been previously developed, but have not maintained widespread adoption.
The Genucom Knee Analysis system (FARO Medical Technologies Inc, Montreal, Canada) is a sophisticated, highly studied arthrometer designed to measure knee laxity in multiple planes [61]. However, reliability and validity were generally inferior, and prohibitively high costs have limited its clinical use [31••, 35–37, 62–68].
The Stryker Knee Laxity Tester (Stryker, Kalamazoo, MI, USA) is an arthrometer conceptually similar to the KT and Rolimeter [69]. Van Eck et al. performed a meta-analysis of studies examining the Stryker device and on average found 81 % sensitivity (range 71–94 %) and 96 % specificity (range 82–100 %) [31••].
The UCLA instrumented clinical knee testing apparatus is also conceptually similar to the KT-1000, with the added ability to evaluate endpoint firmness. Its use is largely limited to that institution; while important in previous research, it has not been featured in recent studies and is not commercially available [46, 70, 71].
The Vermont Knee Laxity Device (VKLD) was designed to evaluate knee laxity under variable levels of lower extremity weight-bearing. Reliability is generally comparable to other devices [72]. This device was useful for literature comparing the knee under variable weight-bearing loads, but is too large and impractical for routine clinical use.
The Edixhoven Mechanic Lachman Device was first described in 1987 and featured a vector-controlled manual handle for force application [73]. Although this theoretically improves reproducibility, the device is quite large and impractical for routine clinical use.
The Acufex Knee Signature System (KSS) consists of a tibial frame and a manual force-applying handle, mounted with transducers to accurately record force and displacement in three dimensions [74]. Limited reports show moderate reliability in injured patients and somewhat inferior reliability in uninjured patients [37].
Data interpretation
Arthrometry results can be interpreted in a number of ways. The most common data interpretation measure is SSD, using the patient’s uninjured knee as a reference. Multiple groups have shown better consistency in SSD measurements as opposed to single-knee measurements, both among different patients, as well as in test-retest analysis of individual knees [25, 29, 38, 68, 75]. Appropriate SSD thresholds vary by device, but are generally 2–3 mm. Some groups do advocate higher or lower values, but this typically comes at a cost of decreased sensitivity or specificity [18, 30, 54•, 69, 71, 76, 77•].
Absolute single-knee translation is a simpler outcome measure, but is confounded by the natural variance in inherent laxity [25]. Daniel et al. showed that average absolute knee laxity increases from 5.8 mm in normal knees to 13.0 mm in ACL-deficient knees using the KT-1000. Subsequent studies have yielded similar results [25, 69, 78].
Another indicator of ACL integrity is the differential laxity produced by increasing forces, visualized by a force-displacement curve. This broad concept has been expressed in several forms, including “stiffness,” “compliance index,” and “elastic modulus.” Daniel et al. recommended their “compliance index,” originally defined as the difference in absolute laxity from an applied force of 67 vs. 89 N [25]. They found this to be most sensitive measure of ACL laxity, and other literature has also supported this measurement technique [78]. Alternatively, the “elastic modulus” can be calculated by calculating the slope of the force-displacement curve, which increases in ACL-deficient knees [78, 79]. Wordeman et al. described a “modified compliance index” designed to evaluate the force-displacement slope at relatively higher forces, eliminating the effects of secondary knee stabilizers [79]. Other groups have recommended the use of second-order mathematical derivatives of the force-displacement curve in detecting ACL laxity [80].
Comparative studies
Stress radiography and arthrometry have distinct advantages and disadvantages when compared to each other. Both are relatively quick with most devices and can be performed in the clinical setting. Stress imaging has the advantages of avoiding measurement error related to soft-tissue effects and the ability to visualize laxity in each knee compartment if desired. Disadvantages include added radiation and cost related to the imaging portion.
Studies comparing diagnostic ability have been mixed, with most finding similar results with both techniques [18, 21, 81•, 82]. Isolated studies have suggested that arthrometry has superior validity to stress imaging when using the KT-1000 or GNRB, but inferior when performed with the Rolimeter [5, 54•, 83]. One group found a higher level of test-retest variability over time with stress imaging, which could impair diagnostic ability [22•]. These findings should be interpreted cautiously as they have not been consistently reproduced and may depend on clinician familiarity. Overall, stress radiography and arthrometry have comparable diagnostic ability, and both appear appropriate in the clinical setting.
Recent comparative studies among arthrometers have shown superior reliability and less operator-dependent error with the GNRB device, likely due to its highly consistent robotic technique [50, 51]. Studies have found comparable results with the KT-1000, Rolimeter, and Stryker devices, and consistently inferior validity and reliability with the Genucom system [36, 55, 59, 60, 64, 84, 85]. It is important to note that each device’s results will fundamentally differ, and clinicians must therefore not assume comparability between measurements from different devices [59, 60, 85].
Clinical application
At this time, laximetry is best-indicated for the diagnostic assessment of complete ACL rupture, alongside a thorough history and clinical exam. Alone, the diagnostic value of laximetry appears comparable to classic exam maneuvers such as the Lachman’s or pivot-shift tests, but the combination of both measures is superior [5, 28, 43, 86, 87]. Some literature suggests that this combination exceeds the diagnostic abilities of MRI, thus potentially obviating the need for the added time and cost of advanced imaging [5, 28].
There is limited evidence for laximetry’s value in managing partial ACL tears, which can be subtle and challenging to clinicians. Some literature suggests that the majority of partial tears have laxity increases of <3 mm and are undetectable with laximetry [78, 88–92]. However, one group using the GNRB arthrometer found 80 % sensitivity and 87 % specificity with their protocol [50]. Other groups have found good diagnostic ability for laximetry when combined with the pivot-shift test, and there is also suggestion that force-displacement curve analysis could be promising for diagnosis severity [19, 78]. Arthrometry may also be useful for monitoring of conservatively treated partial ACL tears, with some evidence that increasing laxity can predict poorer outcomes and therefore guide treatment [93, 94].
Investigation continues regarding other uses for laximetry. Most recently, it was suggested that increased pre-operative laxity of the uninvolved knee may predict increased involved knee laxity and poorer subjective outcomes following ACL reconstruction [95••]. This could represent an important prognostic marker with which to counsel patients pre-operatively. Other groups have recently attempted to correlate laximetry measurements with functional knee stresses, finding a significant positive correlation between arthrometry results and ACL strain during landing exercises [96•].
Previously, there was much speculation that post-operative laxity of the involved knee could predict outcomes. However, prior research shows poor correlation between involved limb laxity and post-operative subjective or functional outcomes [95••, 97–99]. It is our experience as well that post-operative laxity is not strongly linked to negative outcomes such as re-injury rates. Interestingly, there is limited evidence suggesting that increased laxity following ACL reconstruction may indicate injury to other ipsilateral knee ligaments [100]. However, given the scarcity of data, no conclusive recommendation can be made at this time regarding laximetry for prognosis or post-operative monitoring.
Conclusions
Laximetry is a useful technique in clinical practice, especially for aiding in the diagnosis of complete ACL tears. It is most strongly proven as a dichotomous diagnostic tool, although there is limited evidence that quantitative results from the involved or uninvolved knee could be useful prognostically. Perhaps the largest recent development in the field is the introduction of the robotic GNRB arthrometer. While the KT series is the existing arthrometry gold standard, the GNRB has received increased attention owing to its automated testing protocol and promising reliability measures.
Stress imaging and arthrometry have comparable diagnostic value and can be chosen according to clinician preference. A consistent regimen should be adopted, and laximetry should always be combined with a thorough history and physical exam for maximal utility. Laximetry devices and methodology are still evolving, and the diagnostic and prognostic power of these methods will improve with further development. Additional research is needed to better define the indications for objective ACL assessment, to cost-effectively integrate it within routine clinical practice, and ultimately improve outcomes for patients.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
James EW, Williams BT, LaPrade RF. Stress radiography for the diagnosis of knee ligament injuries: a systematic review. Clin Orthop Relat Res. 2014;472(9):2644–57. A comprehensive review of the various techniques of stress imaging for ACL laxity.
Beldame J, Bertiaux S, Roussignol X, et al. Laxity measurements using stress radiography to assess anterior cruciate ligament tears. Orthop Traumatol Surg Res. 2011;97(1):34–43.
Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sport Phys Ther. 2006;36(5):267–88.
Oei EHG, Nikken JJ, Verstijnen ACM, Ginai AZ, Myriam Hunink MG. MR imaging of the menisci and cruciate ligaments: a systematic review. Radiology. 2003;226(3):837–48.
Panisset JC, Ntagiopoulos PG, Saggin PR, Dejour D. A comparison of Telos stress radiography versus Rolimeter in the diagnosis of different patterns of anterior cruciate ligament tears. Orthop Traumatol Surg Res. 2012;98(7):751–8.
Lee YS, Han SH, Jo J, Kwak K-S, Nha KW, Kim JH. Comparison of 5 different methods for measuring stress radiographs to improve reproducibility during the evaluation of knee instability. Am J Sports Med. 2011;39(6):1275–81.
Wirz P, von Stokar P, Jakob RP. The effect of knee position on the reproducibility of measurements taken from stress films: a comparison of four measurement methods. Knee Surg Sports Traumatol Arthrosc. 2000;8(3):143–8.
McPhee IB, Fraser JG. Stress radiography in acute ligamentous injuries of the knee. Injury. 1981;12(5):383–8.
Lerat JL, Moyen BL, Cladière F, Besse JL, Abidi H. Quantification of the Lachman test. J Bone Joint Surg (Br). 2000;82(1):42–7.
Staubli H-U, Noesberger B, Jakob RP. Stressradiography of the knee. Acta Orthop Scand. 1992;63(249):1–27.
Hooper G. Radiological assessment of anterior cruciate ligament deficiency: a new technique. J Bone Joint Surg (Br). 1986;68(2):292–6.
Franklin J, Rosenberg T, Paulos L, France EP. Radiographic assessment of instability of the knee due to rupture of the anterior cruciate ligament. J Bone Joint Surg Am. 1991;73(3):365–72.
Dejour H, Walch G, Chambat P, Ranger P. Active subluxation in extension: a new concept of study of the ACL deficient knee. Am J Knee Surg. 1988;1:204–11.
Dejour H, Bonnin M. Tibial translation after anterior cruciate ligament rupture: two radiological tests compared. J Bone Joint Surg (Br). 1994;76(5):745–9.
Jacobsen K. Stress radiographical measurement of the anteroposterior, medial and lateral stability of the knee joint. Acta Orthop Scand. 1976;47(3):335–4.
Rijke AM, Goitz HT, Mccue FC, Delp JL, Lam D, Southall EP. Graded stress radiography of injured anterior cruciate ligaments. Invest Radiol. 1991;26(11):926–33.
Garcés GL, Perdomo E, Guerra A, Cabrera-Bonilla R. Stress radiography in the diagnosis of anterior cruciate ligament deficiency. Int Orthop. 1995;19(2):86–8.
Beldame J, Mouchel S, Bertiaux S, et al. Anterior knee laxity measurement: comparison of passive stress radiographs Telos and “Lerat”, and GNRB arthrometer. Orthop Traumatol Surg Res. 2012;98(7):744–50.
Dejour D, Ntagiopoulos PG, Saggin PR, Panisset JC. The diagnostic value of clinical tests, magnetic resonance imaging, and instrumented laxity in the differentiation of complete versus partial anterior cruciate ligament tears. Arthroscopy. 2013;29(3):491–9.
Shino K, Inoue M, Horibe S, Nakamura H, Ono K. Measurement of the anterior instability of the knee. J Bone Joint Surg (Br). 1987;69(4):608–13.
Lerat JL, Moyen B, Jenny JY, Perrier JP. A comparison of pre-operative evaluation of anterior knee laxity by dynamic X-rays and by the arthrometer KT 1000. Knee Surg Sports Traumatol Arthrosc. 1993;1(1):54–9.
Bouguennec N, Odri GA, Graveleau N, Colombet P. Comparative reproducibility of TELOS and GNRB for instrumental measurement of anterior tibial translation in normal knees. Orthop Traumatol Surg Res. 2015;101(3):301–5. The largest recent study investigating the reliability of GNRB measurements.
Hoshino Y, Araujo P, Ahldén M, et al. Quantitative evaluation of the pivot shift by image analysis using the iPad. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):975–80.
Espregueira-Mendes J, Pereira H, Sevivas N, et al. Assessment of rotatory laxity in anterior cruciate ligament-deficient knees using magnetic resonance imaging with Porto-knee testing device. Knee Surg Sports Traumatol Arthrosc. 2012;20(4):671–8.
Daniel D, Malcom L, Losse G, Stone ML, Sachs R, Burks R. Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg Am. 1985;67(5):720–6.
Malcom L, Daniel D, Stone ML, Sachs R. The measurement of anterior knee laxity after ACL reconstructive surgery. Clin Orthop Relat Res. 1985;196:35–41.
Arneja S, Leith J. Review article: validity of the KT-1000 knee ligament arthrometer. J Orthop Surg. 2009;17(1):77–9.
Liu S, Osti L, Henry M, Bocchi L. The diagnosis of acute complete tears of the anterior cruciate ligament. J Bone Joint Surg (Br). 1995;77(4):586–8.
Forster IW, Warren-Smith CD, Tew M. Is the KT1000 knee ligament arthrometer reliable? J Bone Joint Surg (Br). 1989;71(5):843–7.
Bach BR, Warren RF, Flynn WM, Kroll M, Wickiewiecz TL. Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg Am. 1990;72(9):1299–306.
Van Eck CF, Loopik M, van den Bekerom MP, Fu FH, Kerkhoffs GMMJ. Methods to diagnose acute anterior cruciate ligament rupture: a meta-analysis of instrumented knee laxity tests. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):1989–97. A very comprehensive comparison of the reliability and validity of a wide range of arthrometers.
Highgenboten CL, Jackson AW, Jansson KA, Meske NB. KT-1000 arthrometer: conscious and unconscious test results using 15, 20, and 30 pounds of force. Am J Sports Med. 1992;20(4):450–4.
Hanten WP, Pace MB. Reliability of measuring anterior laxity of the knee joint using a knee ligament arthrometer. Phys Ther. 1987;67(3):357–9.
Fiebert I, Gresley J, Hoffman S, Kunkel K. Comparative measurements of anterior tibial translation using the KT-1000 knee arthrometer with the leg in neutral, internal rotation, and external rotation. J Orthop Sport Phys Ther. 1994;19(6):331–4.
Highgenboten C, Jackson A, Meske NB. Genucom, KT-1000, and Stryker knee laxity measuring device comparisons. Am J Sports Med. 1989;17(6):743–6.
Torzilli P, Panariello R, Forbes A, Santner T, Warren R. Measurement reproducibility of two commercial knee test devices. J Orthop Res. 1991;9(5):730–7.
Queale WS, Snyder-Mackler L, Handling K, Richards JG. Instrumented examination of knee laxity in patients with anterior cruciate deficiency: a comparison of the KT-2000, Knee Signature System, and Genucom. J Orthop Sport Phys Ther. 1994;19(6):345–51.
Myrer JW, Schulthies SS, Fellingham GW. Relative and absolute reliability of the KT-2000 arthrometer for uninjured knees. Am J Sports Med. 1996;24(1):104–8.
Sernert N, Kartus JTJ, Ejerhed L, Karlsson J. Right and left knee laxity measurements: a prospective study of patients with anterior cruciate ligament injuries and normal control subjects. Arthroscopy. 2004;20(6):564–71.
Ballantyne BT, French AK, Heimsoth SL, Kachingwe AF, Lee JB, Soderberg GL. Influence of examiner experience and gender on interrater reliability of KT-1000 arthrometer measurements. Phys Ther. 1995;75(10):898–906.
Wroble R, Van Ginkel L, Grood E, Noyes F, Shaffer B. Repeatability of the KT-1000 arthrometer in a normal population. Am J Sports Med. 1990;18(4):396–9.
Hefti F, Muller W, Jakob R, Staubli H. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993;1(3–4):226–34.
Wiertsema SH, van Hooff HJA, Migchelsen LAA, Steultjens MPM. Reliability of the KT1000 arthrometer and the Lachman test in patients with an ACL rupture. Knee. 2008;15(2):107–10.
Robnett NJ, Riddle DL, Kues JM. Intertester reliability of measurements obtained with the KT-1000 on patients with reconstructed anterior cruciate ligaments. J Orthop Sport Phys Ther. 1995;21(2):113–9.
Berry J, Kramer K, Binkley J, et al. Error estimates in novice and expert raters for the KT-1000 arthrometer. J Orthop Sport Phys Ther. 1999;29(1):49–55.
Markolf KL, Graff-Radford A, Amstutz HC. In vivo knee stability: a quantitative assessment using an instrumented clinical testing apparatus. J Bone Joint Surg Am. 1978;60(5):664–74.
Kowalk DL, Wojtys EM, Disher J, Loubert P. Quantitative analysis of the measuring capabilities of the KT-1000 knee ligament arthrometer. Am J Sports Med. 1993;21(5):744–7.
Sernert N, Helmers J, Kartus C, Ejerhed L, Kartus J. Knee-laxity measurements examined by a left-hand- and a right-hand-dominant physiotherapist, in patients with anterior cruciate ligament injuries and healthy controls. Knee Surg Sports Traumatol Arthrosc. 2007;15(10):1181–6.
Wright RW, Luhmann SJ. The effect of knee effusions on KT-1000 arthrometry: a cadaver study. Am J Sports Med. 1998;26(4):571–4.
Robert H, Nouveau S, Gageot S, Gagnière B. A new knee arthrometer, the GNRB: experience in ACL complete and partial tears. Orthop Traumatol Surg Res. 2009;95(3):171–6.
Collette M, Courville J, Forton M, Gagnière B. Objective evaluation of anterior knee laxity; comparison of the KT-1000 and GNRB arthrometers. Knee Surg Sports Traumatol Arthrosc. 2012;20(11):2233–8.
Vauhnik R, Morrissey MC, Perme MP, Sevsek F, Rugelj D. Inter-rater reliability of the GNRB knee arthrometer. Knee. 2014;21(2):541–3.
Vauhnik R, Perme MP, Barcellona MG, Rugelj D, Morrissey MC, Sevsek F. Robotic knee laxity testing: reliability and normative data. Knee. 2013;20(4):250–5.
Lefevre N, Bohu Y, Naouri JF, Klouche S, Herman S. Validity of GNRB arthrometer compared to Telos in the assessment of partial anterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 2014;22(2):285–90. The largest recent study comparing GNRB to stress imaging and establishing its utility in diagnosis of partial ACL tears.
Balasch H, Schiller M, Friebel H, Hoffmann F. Evaluation of anterior knee joint instability with the Rolimeter: a test in comparison with manual assessment and measuring with the KT-1000 arthrometer. Knee Surg Sports Traumatol Arthrosc. 1999;7:204–8.
Hatcher J, Hatcher A, Arbuthnot J, McNicholas M. An investigation to examine the inter-tester and intra-tester reliability of the Rolimeter knee tester, and its sensitivity in identifying knee joint laxity. J Orthop Res. 2005;23(6):1399–403.
Muellner T, Bugge W, Johansen S, Holtan C, Engebretsen L. Inter- and intratester comparison of the Rolimeter knee tester: effect of tester’s experience and the examination technique. Knee Surg Sports Traumatol Arthrosc. 2001;9(5):302–6.
Papandreou MG, Antonogiannakis E, Karabalis C, Karliaftis K. Inter-rater reliability of Rolimeter measurements between anterior cruciate ligament injured and normal contralateral knees. Knee Surg Sports Traumatol Arthrosc. 2005;13:592–7.
Schuster AJ, Mcnicholas MJ, Wachtl SW, Mcgurty DW, Jakob RP. A new mechanical testing device for measuring anteroposterior knee laxity. Am J Sports Med. 2004;32(7):1731–5.
Passler H, Ververidis A, Monauni F. Beweglichkeitswertung an knien mit VKB-schaden mit hilfe des KT 1000 und Aircast Rolimeter. Hefte zur Zeitschrift der Unfallchirurg. 1998;272:731–2.
Oliver JH, Coughlin LP. Objective knee evaluation using the Genucom Knee Analysis System: clinical implications. Am J Sports Med. 1987;15(6):571–8.
Highgenboten C, Jackson A, Meske N. Genucom knee analysis system: reproducibility and database development. Med Sci Sports Exerc. 1990;22(5):713–7.
McQuade KJ, Sidles JA, Larson RV. Reliability of the Genucom Knee Analysis System: a pilot study. Clin Orthop Relat Res. 1989;245:216–9.
Steiner M, Brown C, Zarins B, Brownstein B, Koval P, Stone P. Measurement of anterior-posterior displacement of the knee. J Bone Joint Surg Am. 1990;72(9):1307–15.
Andersen HN, Frandsen PA. Assessment of anterior cruciate laxity using the Genucom System. Int Orthop. 1993;17(6):375–83.
Draganich L, Sathy M, Reider B. The effect of thigh and goniometer restraints on the reproducibility of the genucom knee analysis system. Am J Sports Med. 1994;22(5):627–31.
Granberry W, Noble P, Woods W. Evaluation of an electrogoniometric instrument for measurement of laxity of the knee. J Bone Joint Surg Am. 1990;72(9):1316–22.
Wroble RR, Grood ES, Noyes FR, Schmitt DJ. Reproducibility of Genucom knee analysis system testing. Am J Sports Med. 1990;18(4):387–95.
Boniface RJ, Fu FH, Ilkhanipour K. Objective anterior cruciate ligament testing. Orthopedics. 1986;9(3):391–3.
Sherman OH, Markolf KL, Ferkel RD. Measurements of anterior laxity in normal and anterior cruciate absent knees with two instrumented test devices. Clin Orthop Relat Res. 1987;215:156–61.
Pugh L, Mascarenhas R, Arneja S, Chin PYK, Leith JM. Current concepts in instrumented knee-laxity testing. Am J Sports Med. 2009;37(1):199–210.
Un BS, Beynnon BD, Churchill DL, Haugh LD, Risberg MA, Fleming BC. A new device to measure knee laxity during weightbearing and non-weightbearing conditions. J Orthop Res. 2001;19(6):1185–91.
Edixhoven P, Huiskes R, de Graaf R, van Rens TJG, Slooff TJ. Accuracy and reproducibility of instrumented knee-drawer tests. J Orthop Res. 1987;5(3):378–87.
Fruensgaard S, Krøner K, Riis J. Suture of the torn anterior cruciate ligament. Acta Orthop Scand. 1992;63(3):323–5.
Daniel DM, Stone ML, Sachs R, Malcom L. Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med. 1985;13(6):401–7.
Ramski DE, Kanj WW, Franklin CC, Baldwin KD, Ganley TJ. Anterior cruciate ligament tears in children and adolescents: a meta-analysis of nonoperative versus operative treatment. Am J Sports Med. 2014;42(11):2769–76.
Klouche S, Lefevre N, Cascua S, Herman S, Gerometta A, Bohu Y. Diagnostic value of the GNRB in relation to pressure load for complete ACL tears : a prospective case–control study of 118 subjects. Orthop Traumatol Surg Res. 2015;101(3):297–300. The largest case–control study evaluating the diagnostic capabilities of the GNRB arthrometer.
Liu W, Maitland ME, Bell GD. A modeling study of partial ACL injury: simulated KT-2000 arthrometer tests. J Biomech Eng. 2002;124(3):294–301.
Wordeman SC, Paterno MV, Quatman CE, Bates NA, Hewett TE. Arthrometric curve-shape variables to assess anterior cruciate ligament deficiency. Clin Biomech. 2012;27(8):830–6.
Maitland ME, Bell GD, Mohtadi NGH, Herzog W. Quantitative analysis of anterior cruciate ligament instability. Clin Biomech. 1995;10(2):93–7.
Jenny J, Arndt J, Computer Assisted OrthoPaedic Surgery-France (CAOS). Anterior knee laxity measurement using stress radiographs and the GNRB system versus intraoperative navigation. Orthop Traumatol Surg Res. 2013;99(6):S297–300. Compares GNRB arthrometry to stress imaging and finds comparable results, supporting its clinical value.
Staubli H-U, Jakob RP. Anterior knee motion analysis—measurement and simultaneous radiography. Am J Sports Med. 1991;19(2):172–7.
Fleming BC, Brattbakk B, Peura GD, Badger GJ, Beynnon BD. Measurement of anterior-posterior knee laxity: a comparison of three techniques. J Orthop Res. 2002;20(3):421–6.
Anderson AF, Snyder RB, Federspiel CF, Lipscomb AB. Instrumented evaluation of knee laxity: a comparison of five arthrometers. Am J Sports Med. 1992;20(2):135–40.
Ganko A, Engebretsen L, Ozer H. The Rolimeter a new arthrometer compared with the KT-1000. Knee Surg Sports Traumatol Arthrosc. 2000;8(1):36–9.
Anderson AF, Lipscomb AB. Preoperative instrumented testing of anterior and posterior knee laxity. Am J Sports Med. 1989;17(3):387–92.
Graham G, Johnson S, Dent C, Fairclough J. Comparison of clinical tests and the KT1000 in the diagnosis of anterior cruciate ligament rupture. Br J Sports Med. 1991;25(2):96–7.
DeFranco M, Bach B. A comprehensive review of partial anterior cruciate ligament tears. J Bone Joint Surg Am. 2009;91(1):198–208.
Fritschy D, Panoussopoulos A, Wallensten R, Peter R. Can we predict the outcome of a partial rupture of the anterior cruciate ligament? A prospective study of 43 cases. Knee Surg Sports Traumatol Arthrosc. 1997;5(1):2–5.
Bak K, Scavenius M, Hansen S, Nørring K, Jensen KH, Jorgensen U. Isolated partial rupture of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 1997;5(2):66–71.
Messner K, Maletius W. Eighteen- to twenty-five-year follow-up after acute partial anterior cruciate ligament rupture. Am J Sports Med. 1999;27(4):455–9.
Lintner DM, Kamaric E, Moseley JB, Noble PC. Partial tears of the anterior cruciate ligament: are they clinically detectable? Am J Sports Med. 1995;23(1):111–8.
Noyes FR, Mooar LA, Moorman III CT, McGinniss GH. Partial tears of the anterior cruciate ligament. J Bone Joint Surg (Br). 1989;71(5):825–33.
Fruensgaard S, Johannsen HV. Incomplete ruptures of the anterior cruciate ligament. J Bone Joint Surg (Br). 1989;71(3):526–30.
Kim S, Lee S, Kim S, Kim S, Kim J, Jung M. Does anterior laxity of the uninjured knee influence clinical outcomes of ACL reconstruction? J Bone Joint Surg Am. 2014;96(7):543–8. Suggests that uninvolved knee laximetry can help predict the outcome of contralateral knee ACL reconstruction. Validates arthrometry as a quantitative tool, as opposed to simply a dichotomous tool.
Kiapour A, Wordeman S, Paterno M, et al. Diagnostic value of knee arthrometry in the prediction of anterior cruciate ligament strain during landing. Am J Sports Med. 2014;42(2):312–9. Validates knee laximetry as correlated with in-vivo ACL stress during functional athletic maneuvers.
Hyder N, Bollen S, Sefton G, Swann A. Correlation between arthrometric evaluation of knees using KT 1000 and Telos stress radiography and functional outcome following ACL reconstruction. Knee. 1997;4(3):121–4.
Pollet V, Barrat D, Meirhaeghe E, Vaes P, Handelberg F. The role of the Rolimeter in quantifying knee instability compared to the functional outcome of ACL-reconstructed versus conservatively-treated knees. Knee Surg Sports Traumatol Arthrosc. 2005;13(1):12–8.
Giannotti BF, Fanelli GC, Barrett TA, Edson C. The predictive value of intraoperative KT-1000 arthrometer measurements in single incision anterior cruciate ligament reconstruction. Arthroscopy. 1996;12(6):660–6.
O’Brien S, Warren R, Pavlov H, Panariello R, Wickiewicz T. Reconstruction of the chronically insufficient anterior cruciate ligament with the central third of the patellar ligament. J Bone Joint Surg Am. 1991;73(2):278–86.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Eric M. Rohman declares that he has no conflict of interest.
Jeffrey A. Macalena has served as a consultant for Vericel, Smith and Nephew, and Arthrex within the past 36 months, outside of the submitted work.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on ACL Update: Objective Measures on Knee Instability
Rights and permissions
About this article

Cite this article
Rohman, E.M., Macalena, J.A. Anterior cruciate ligament assessment using arthrometry and stress imaging. Curr Rev Musculoskelet Med 9, 130–138 (2016). https://doi.org/10.1007/s12178-016-9331-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12178-016-9331-1