
Abstract
Background
Symptoms of posttraumatic stress disorder (PTSD) after acute coronary syndrome (ACS) are associated with recurrent ACS events and mortality. Poor sleep may be a mechanism, but the association between PTSD and sleep after ACS is unknown.
Purpose
This study aims to estimate the association between ACS-induced PTSD symptoms and self-reported sleep.
Methods
ACS-induced PTSD symptoms were assessed 1-month post-ACS in 188 adults using the Impact of Events Scale-Revised. Sleep was assessed using the Pittsburgh Sleep Quality Index. Linear and logistic regression models were used to determine whether PTSD symptoms were associated with self-reported sleep, independent of sociodemographic and clinical covariates.
Results
In adjusted models, ACS-induced PTSD symptoms were associated with worse overall sleep (β = 0.22, p = 0.003) and greater impairment in six of seven components of sleep (all p values <0.05).
Conclusions
ACS-induced PTSD symptoms may be associated with poor sleep, which may explain why PTSD confers increased cardiovascular risk after ACS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Acute coronary syndrome (ACS)-induced symptoms of posttraumatic stress disorder (PTSD) are prevalent among patients with ACS and are associated with adverse clinical outcomes. A recent meta-analysis of ACS patients found an aggregate prevalence estimate for PTSD of 12 % across 24 studies and a doubling of risk for a combined outcome of mortality and ACS recurrence in patients with clinically significant PTSD symptoms compared to those without PTSD symptoms [1]. It is well known that exposure to a traumatic event can interfere with sleep and that PTSD contributes to the development of sleep problems [2]. Indeed, approximately 70 % of people with clinician-diagnosed PTSD have co-occurring sleep problems [2, 3]. Additional research has shown that disrupted sleep is also common among ACS patients [4], and disrupted sleep has been shown to predict cardiovascular outcomes [5]. Understanding and modifying risk factors for disrupted sleep in patients after ACS may ultimately reduce morbidity and mortality. Although risk factors for disrupted sleep have been examined in patients with chronic diseases, including those with stable coronary heart disease [6], few studies have examined predictors of sleep in post-ACS patients.
Notwithstanding the wealth of data linking PTSD to sleep problems in the general populations and psychiatric samples, no studies to our knowledge have examined the specific association of ACS-induced PTSD symptoms with sleep in patients with an ACS. Given that medically induced forms of trauma such as an ACS have been differentiated from other forms of trauma both conceptually and clinically [7], it is possible that the associations of PTSD symptoms and sleep differ based on type of trauma. In addition, little is known about the mechanisms linking PTSD to outcomes, and poor sleep may be a candidate mechanism by which PTSD confers increased risk of ACS recurrence and mortality. We thus examined the associations of ACS-induced PTSD symptoms with overall self-reported sleep in a cross-sectional study of 188 patients with ACS. Given the well-characterized association between PTSD and sleep reported in community samples and other patient populations, we hypothesized that greater ACS-induced PTSD symptoms would be associated with worse self-reported sleep. We secondarily tested whether pre-ACS history of PTSD was also associated with overall self-reported sleep in this sample. Finally, we examined whether specific components of self-reported sleep, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction, were associated with greater ACS-induced PTSD symptoms.
Methods
Participants
Participants were consecutively hospitalized patients with ACS who were enrolled in the Prescription Use, Lifestyle, and Stress Evaluation study, an ongoing, single-site, prospective, observational cohort study of the prognostic risk conferred by psychosocial factors at the time of an ACS. Patients with unstable angina pectoris or acute ST and non-ST segment elevation myocardial infarction were recruited from Columbia University Medical Center within one week of hospitalization for their ACS. Patients completed a structured psychiatric interview 3–7 days postdischarge and a follow-up interview 1 month later. The current analyses include 188 participants who completed self-report measures of ACS-induced PTSD symptoms and sleep approximately 1 month after their index ACS event. Excluded from analyses were 507 participants who were enrolled prior to initiation of PTSD data collection (n = 362), were missing data on sleep (n = 4), were missing data on both PTSD symptoms and sleep (n = 94), or whose PTSD and sleep data were obtained beyond the window of the 1-month follow-up visit (n = 47). Compared to the 188 participants included in this study, the 507 participants not included did not differ on any sociodemographic, behavioral, or clinical factors included in these analyses. Data collection occurred between February 2009 and June 2010. The Institutional Review Board of Columbia University approved this study, and all participants provided informed consent.
Measures
Self-reported Sleep Problems
One-month following their discharge from the hospital, participants attended a follow-up visit during which they completed the Pittsburgh Sleep Quality Index (PSQI), a widely used self-report measure of sleep over the past month on which higher total scores indicate worse overall sleep [8]. Probable sleep disorder was defined categorically as a global PSQI score of >5, a cutoff with diagnostic sensitivity of 89.6 %, and specificity of 86.5 % in distinguishing groups of “good” and “poor” sleepers compared to gold standard clinical and laboratory measures [8].
In addition to a total sleep score, which has a possible range of 0 to 21, the PSQI also provides information regarding seven components of sleep. The first component, subjective sleep quality, is measured by a single item that asks participants to rate their overall sleep quality using a 4-point response scale ranging from 1 (“very good”) to 4 (“very bad”). The second component, sleep latency, is assessed with two items, including how many minutes it usually takes the participant to fall asleep and how often participants are unable to fall asleep within 30 min. For the second item, participants use a 4-point response scale ranging from 1 (“not during the past month”) to 4 (“three or more times per week”). This 4-point response scale is used for all other frequency items on the PSQI. The third component, sleep duration, is based on the number of hours of sleep during a typical night reported by participants. The fourth component, habitual sleep efficiency, is assessed using participants’ reports of when they typically went to bed, when they typically awoke, and how many hours they typically slept. This information is used to compute the proportion of sleep time relative to the number of hours in bed. The fifth component, sleep disturbance, is assessed using nine items such as frequency of waking during the night or frequency of having pain. The sixth component, use of sleep medications, is assessed based on participants’ reports of how often they took prescription or over-the-counter medication to help them sleep. The seventh component, daytime dysfunction, is assessed using two items that ask participants about the frequency with which they were not able to “keep up enthusiasm to get things done” and had “trouble staying awake while driving, eating meals, or engaging in social activity.”
Consistent with the PSQI scoring instructions [7], responses to items for each PSQI component were recoded such that scores ranged from 0 to 3, with higher scores indicating poorer sleep on that component. Correlations (Spearman’s rho) among the individual sleep components ranged from ρ = 0.11 (sleep duration and use of sleep medications) to ρ = 0.65 (sleep duration and habitual sleep efficiency). All correlations—except the associations of use of sleep medications with sleep duration, daytime dysfunction, and habitual sleep efficiency—were significant (all p values ≤0.008). The mean correlation was ρ = 0.31.
Scores across the seven PSQI component scores were aggregated into a global score of self-reported sleep with a range from 0 to 21. As global scores above 5 are considered indicative of probable sleep disorder [8], any participant with a global score above 5 was given a score of 1 on probable sleep disorder, and all other respondents were coded 0.
ACS-Induced PTSD Symptoms
ACS-induced PTSD symptoms were assessed at the 1-month follow-up visit with the Impact of Events Scale-Revised (IES-R) [9]. Participants used a 5-point scale ranging from 0 (“not at all”) to 4 (“extremely”) to report the extent to which they had been bothered by each of 22 PTSD symptoms in the past week with reference to their hospitalization for ACS. Specifically, they were told, “Think about when you were hospitalized on (date), and we enrolled you in this study. In the past 7 days have you been bothered by any of the following in reference to that hospitalization?” The IES-R yields a total score with a range from 0 to 88, and the internal validity of this score in the current study was acceptable (Cronbach’s α = 0.94).
Pre-ACS History of PTSD
Within 3–7 days of their discharge from the hospital, participants were screened for PTSD in the 3 months preceding hospitalization for their index ACS event using the Structured Clinical Interview for DSM-IV [10]. They reported whether they had [1] experienced a traumatic event (“such as a major disaster, very serious accident or fire, being physically assaulted or raped, seeing another person killed, or dead, or badly hurt, or hearing about something horrible that has just happened to someone close to you”) [2], whether the event recurred “in nightmares, flashbacks, or thoughts you cannot get rid of,” and [3] whether the experience of “thoughts or feelings coming back” had happened in the past 3 months. Participants who responded “yes” to all three items were categorized as having a pre-ACS history of PTSD. Responses to these questions correctly identified 97 % of PTSD cases in previous studies [11]. All analyses that included pre-ACS history of PTSD were limited to the 158 participants who were not missing data on this variable.
Sociodemographic and Clinical Covariates
During their hospitalization, participants identified their ethnicity (Hispanic versus non-Hispanic), race (Black versus non-Black), high school education (yes/no), and partner status (has a partner or spouse/does not have a partner or spouse). Medical chart review was used to ascertain body mass index (BMI), prior cardiovascular disease and cardiac procedures (unstable angina, myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, New York Heart Association heart failure class), prior cerebrovascular disease (stroke and transient ischemic attack), and other chronic conditions (e.g., respiratory diseases, liver diseases, and rheumatologic diseases). Age and sex were recorded for each participant. Measures of disease severity included the Global Registry of Acute Coronary Events risk score as an estimate of 6-month post-ACS mortality risk [12], and the Charlson comorbidity index as a measure of medical comorbidities [13].
Psychological and Behavioral Covariates
During the 1-month follow-up, participants also completed the 21-item Beck Depression Inventory [14] and the Paffenbarger Physical Activity Questionnaire [15]. The Beck Depression Inventory is a self-report instrument that assesses severity of depressive symptoms experienced during the past week, with possible scores for each question ranging from 0 to 3 and a possible total score ranging from 0 to 63. It has excellent psychometric properties, as shown with multiple community and medical samples [16]. In the current study, the internal consistency of the Beck Depression Inventory as measured by Cronbach’s α was 0.88. The Paffenbarger Physical Activity Questionnaire was used to calculate weekly energy expended through leisure time physical activity using the scoring system described by Paffenbarger and colleagues [17].
Analytic Strategy
Baseline sociodemographic, behavioral, and clinical characteristics were calculated separately for those with and without probable sleep disorder, and participants in these two groups were compared using independent-samples t tests and Pearson’s chi-square tests for continuous and categorical variables, respectively. The association between ACS-induced PTSD symptoms and self-reported sleep was examined in an unadjusted and an adjusted linear regression model with total IES-R score as the primary predictor and total continuous PSQI score as the primary dependent variable. Given that the total PSQI score was positively skewed, a square-root transformation was applied to this variable. The adjusted linear regression model included sociodemographic, behavioral, and clinical predictors of self-reported sleep [18] as covariates, including age, sex, partner status, high school education, BMI, Paffenbarger physical activity score, Global Registry of Acute Coronary Events risk score, Charlson comorbidity index, and Beck Depression Inventory score. All covariates were entered with the primary predictor variable in a single block. Similar unadjusted and adjusted binary logistic regression models were conducted with probable sleep disorder (i.e., global PSQI score of >5) as the outcome measure. To secondarily examine possible differential associations between self-reported sleep and pre-ACS history of PTSD versus ACS-induced PTSD symptoms, all aforementioned linear and logistic regression models were repeated substituting pre-ACS history of PTSD for IES-R scores.
To test whether specific components of self-reported sleep were associated with ACS-induced PTSD symptoms, we conducted exploratory unadjusted and adjusted ordered logistic regression models for each of the seven PSQI sleep components. The assumption of proportional odds, which specifies homogeneity of the effect of each predictor variable across all levels of the outcome, was evaluated for each model. This assumption was violated for models with sleep duration, sleep efficiency, and sleep disturbances. Because these three components of the PSQI are calculated using a continuous, interval scale before being recoded to the continuous, ordinal scale used by the other PSQI components, we conducted a median split of these variables and analyzed them using binary logistic regression.
We additionally performed exploratory analyses to characterize the unique and common variance contributions of ACS-induced PTSD symptoms and depressive symptoms with overall self-reported sleep. To do so, we conducted a hierarchical linear regression model with three blocks of variables. Block 1 included age, sex, and all demographic and clinical covariates except the Beck Depression Inventory; block 2 added the Beck Depression Inventory; and block 3 added the IES-R. Using this approach, we report the change in the variance explained in overall self-reported sleep associated with the addition of ACS-induced PTSD symptoms to a model already including depressive symptoms. We additionally report the partial correlations of ACS-induced PTSD symptoms with overall self-reported sleep first controlling for all demographic and clinical covariates except depressive symptoms and then additionally controlling for depressive symptoms.
The percentage of missing data on covariates ranged from 1.0 % (for partner status) to 1.6 % (for Paffenbarger physical activity score). We conducted multiple imputation to generate five imputed datasets. All variables except the primary independent variables (i.e., ACS-induced PTSD symptoms and pre-ACS history of PTSD) and dependent variables (i.e., all PSQI scores) were included. All analyses were conducted using SPSS 20.0 (IBM, Armonk, NY).
Results
Participants in this sample were predominantly male (65.4 %) and non-Hispanic (63.8 %) with a mean age of 63.2 ± 11.3 years. Other descriptive characteristics of this sample are shown in Table 1.
Association of ACS-Induced PTSD Symptoms with Overall Self-reported Sleep
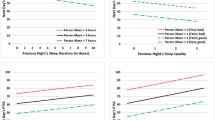
The mean IES-R score for the sample of 188 participants was 6.3 ± 11.0 (range, 0–55.0), and the mean PSQI total score was 5.2 ± 4.0 (range, 0–17.0). Greater ACS-induced PTSD symptoms were independently associated with worse overall self-reported sleep in unadjusted and adjusted linear regression models. In the adjusted model, which included as covariates age, sex, ethnicity, partner status, high school education, BMI, Paffenbarger physical activity score, Global Registry of Acute Coronary Events risk score, Charlson comorbidity index, and depressive symptom score, each standard deviation increase on the IES-R measure of ACS-induced PTSD symptoms was associated with a 0.22 standard deviation worsening in overall self-reported sleep (β = 0.22, p = 0.003; Table 2). Hispanic ethnicity, greater BMI, and higher depressive symptom scores were also independent, significant correlates of overall self-reported sleep in this adjusted linear regression model.
Of note, the unadjusted association of ACS-induced PTSD symptoms with overall self-reported sleep was attenuated when depressive symptoms were added to the regression model but not when other demographic and clinical characteristics were added. Specifically, the zero-order correlation of ACS-induced PTSD symptoms with overall self-reported sleep was 0.38; the partial correlation of ACS-induced PTSD symptoms with overall self-reported sleep independent of all covariates except depressive symptoms was 0.39; and the partial correlation of ACS-induced PTSD symptoms with overall self-reported sleep independent of all covariates including depressive symptoms was 0.26 (all p values <0.001). Notwithstanding this attenuated effect, the addition of ACS-induced PTSD symptoms to a fully adjusted model that included depressive symptoms contributed to a significant increase of 5 % in the variance explained in overall self-reported sleep (F change (1, 172) = 12.5, p = 0.001).
Association of ACS-Induced PTSD Symptoms with Probable Sleep Disorder
Of the 188 participants, 76 (40.4 %) had a PSQI total score of >5, which is indicative of probable sleep disorder. Compared with participants who did not have probable sleep disorder, those who did have a probable sleep disorder had lower scores on the total PSQI score and all seven sleep components, which is indicative of poorer self-reported sleep. They were also significantly more likely to be female and Hispanic, had a significantly higher BMI, and reported significantly more depressive symptoms and ACS-induced PTSD symptoms. In the unadjusted logistic regression model, greater ACS-induced PTSD symptoms were significantly associated with elevated odds of having probable sleep disorder (i.e., PSQI total score of >5). Each point increase on the IES-R measure of ACS-induced PTSD symptoms was significantly associated with approximately 6 % increased odds of having probable sleep disorder. ACS-induced PTSD symptoms were not significantly associated with odds of probable sleep disorder in the adjusted model, although greater BMI and greater depressive symptoms were significantly associated with increased odds of probable sleep disorder in this model. Hispanic ethnicity was associated with significantly lower odds of probable sleep disorder.
Association of Pre-ACS History of PTSD with Overall Self-reported Sleep and Probable Sleep Disorder
Pre-ACS history of PTSD was not associated with either overall self-reported sleep or probable sleep disorder in unadjusted or adjusted regression models (all p values >0.11).
Association of ACS-Induced PTSD Symptoms with Individual Components of Self-reported Sleep
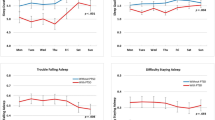
Greater ACS-induced PTSD symptoms were significantly associated with six of seven PSQI sleep components in unadjusted and adjusted logistic regression models (Table 3). The association of ACS-induced PTSD symptoms with sleep latency was only significant in an unadjusted model. The magnitude of the significantly increased odds of poor self-reported sleep associated with each 1-point increase on the IES-R measure of ACS-induced PTSD symptoms ranged from 2 % for sleep quality and daytime dysfunction to 9 % for sleep disturbances. Female sex, Hispanic ethnicity, BMI, partner status, Charlson comorbidity index, and depressive symptoms were also significantly associated with various self-reported sleep components.
Discussion
We found that greater ACS-induced symptoms of PTSD were associated with worse overall self-reported sleep and poorer scores on six of seven individual components of sleep as measured by the PSQI in 188 patients with recent hospitalization for ACS. These associations remained significant after adjusting for sociodemographic covariates, medical comorbidities (Charlson), cardiac disease severity (Global Registry of Acute Coronary Events risk score), and depressive symptoms (Beck Depression Inventory). We also observed a trend for an association between ACS-induced PTSD symptoms and probable sleep disorder, although this association did not remain significant after multivariable adjustment. In contrast, pre-ACS history of PTSD was not associated with overall self-reported sleep or probable sleep disorder in either unadjusted or adjusted models.
Our findings are consistent with those from studies of PTSD and sleep among individuals with PTSD induced by nonmedical events. Indeed, previous studies have indicated that as many as 70 % of those with PTSD report sleep disturbances [3]. Furthermore, polysomnography assessments have shown that compared to those without exposure to childhood trauma, those with exposure have greater trouble initiating and maintaining sleep, poorer sleep quality, greater sleep disturbances and nighttime awakenings, lower sleep efficiency, shorter duration of rapid eye movement sleep, and longer latency to enter rapid eye movement sleep [2]. Another study of outpatients with a primary diagnosis of PTSD found positive correlations between severity of PTSD, the PSQI global score and five of the seven PSQI components (sleep efficiency and use of sleep medications did not vary with PTSD severity) [19]. The strong association between ACS-induced PTSD and sleep may be due to the fact that disturbed sleep is embedded in the PTSD phenotype and its diagnosis. However, results of recent treatment studies for PTSD and sleep disturbance suggest that the two conditions may be most usefully conceptualized as comorbid, rather than one being merely a symptom of the other [20, 21]. In addition, autonomic dysregulation, which is associated with both PTSD [22] and disrupted sleep [23], may represent a common mechanism underlying their association.
Of note, the adjusted association of ACS-induced PTSD symptoms with probable sleep disorder was not significant, although the magnitude of the unadjusted and adjusted associations was comparable. Although it is possible that ACS-induced PTSD symptoms are indeed not associated with probable sleep disorder, there are other explanations for the observed null finding. First, we may have had limited statistical power to detect this association given that our total sample size was small relative to the number of covariates in our adjusted regression model. Second, it is possible that the cutpoint used to define probable sleep disorder (i.e., PSQI total score > 5) is not optimal for participants with PTSD or ACS-induced PTSD. Although the diagnostic accuracy of the PSQI has not been investigated exclusively for individuals with PTSD to our knowledge, studies of other measures have found different estimates of diagnostic accuracy for subgroups of patients with different clinical characteristics [24]. Interestingly, in post hoc analyses of this study, we found that ACS-induced PTSD symptoms were significantly associated with an 8 % increased odds of probable sleep disorder in an adjusted model with probable sleep disorder defined as having a PSQI total score greater than the median (>4).
Our analyses identified several additional independent correlates of self-reported sleep and sleep components including female sex, Hispanic ethnicity, partner status, BMI, Charlson comorbidity index, and depressive symptoms. Consistent with several other studies, we found that depressive symptoms were significantly associated with overall self-reported sleep quality, probable sleep disorder, and some components of self-reported sleep [25, 26]. Although the association of ACS-induced PTSD symptoms with overall self-reported sleep was attenuated when controlling for depressive symptoms but not when controlling for other demographic and clinical covariates, the addition of ACS-induced PTSD symptoms to a fully adjusted model with depressive symptoms contributed to a significant increase in the variance explained in overall self-reported sleep. Future studies should further consider reasons for the differential associations of depressive symptoms with various components of self-reported sleep and disentangle the possibly complex associations among depression, PTSD, and self-reported sleep in patients with ACS. We additionally observed that female sex and greater BMI were associated with worse overall self-reported sleep, while Hispanic ethnicity was protective against various components of poor sleep. Although the BMI finding is consistent with previous findings [27], other studies have reported no gender differences in objective and subjective sleep measures [28] and have suggested that Hispanic ethnicity might confer increased risk for sleep problems [29]. Future studies may pursue a more detailed investigation of the association between sociodemographic factors and sleep specifically in patients with ACS and other cardiovascular diseases.
Notwithstanding the strong and consistent associations observed between ACS-induced PTSD symptoms and both overall self-reported sleep and specific sleep components, our study is limited by several factors that deserve mention. First, it is cross-sectional, precluding us from considering the directionality of the association between ACS-induced PTSD and sleep. Although research in other populations suggests that exposure to a traumatic event can interfere with sleep and that PTSD is related to the development of sleep problems [2], other research has shown that poor sleep may contribute to the development of PTSD [30]. Future research with repeat assessments of sleep and PTSD are needed to disentangle the possibly complex associations among these two factors in patients with ACS. Secondly, our assessment of sleep was obtained by self-report at a single point in time. Although the PSQI has been widely used in other studies, additional studies are needed with assessments of objectively measured sleep via gold-standard methods such as polysomnography. Future research should additionally consider whether sleep problems that precede an ACS event or sleep problems at other time points following an ACS contribute to the associations observed in the current study. Third, our assessment of ACS-induced PTSD symptoms did not include a diagnostic interview. Although the IES-R has been widely featured in studies of PTSD, has favorable psychometric properties [31], and has been linked to prognosis in ACS patients [32], additional studies of the association between clinician-diagnosed PTSD and sleep are needed. Fourth, we did not control for participants’ overall medication use or a general measure of anxiety, which may confound the observed associations of ACS-induced PTSD symptoms and self-reported sleep. Finally, very few participants in our sample had a pre-ACS history of PTSD, which may have limited our power to detect an association of this variable with self-reported sleep. Nonetheless, the association of pre-ACS history of PTSD with each of the self-reported sleep outcomes was uniformly nonsignificant, and we did not observe any signals of an association.
Conclusions
Our study is the first to examine the association of ACS-induced symptoms of PTSD with self-reported sleep. The implications of the PTSD-sleep association in the context of the post-ACS recovery period is thus important to consider with respect to gaining a better understanding of the associations between PTSD, sleep, and cardiac prognosis as well as treatment strategies for patients recovering from an ACS. Both poor sleep [5] and PTSD symptoms [1] have been linked to adverse cardiovascular outcomes, and our findings suggest that either sleep or PTSD may mediate or modify the impact of the other on cardiac prognosis in ACS patients. If future research supports this mediation or moderation hypothesis, then additional research might consider whether interventions that address either PTSD symptoms or sleep among ACS patients offset the risk of adverse cardiovascular events in this population. Still other research might consider the feasibility and efficacy of routine screening for PTSD and sleep problems in patients with ACS to improve cardiovascular outcomes—a policy that has recently been adopted with respect to other psychosocial risk factors such depression in ACS [33].
References
Edmondson D, Richardson S, Falzon L, Davidson KW, Mills MA, Neria Y. Posttraumatic stress disorder prevalence and risk of recurrence in acute coronary syndrome patients: A meta-analytic review. PLoS One. 2012;7:e38915.
Babson KA, Feldner MT. Temporal relations between sleep problems and both traumatic event exposure and PTSD: A critical review of the empirical literature. J Anxiety Disord. 2010;24:1-15.
Ohayon MM, Shapiro CM. Sleep disturbances and psychiatric disorders associated with posttraumatic stress disorder in the general population. Compr Psychiatry. 2000;41:469-478.
Schiza SE, Simantirakis E, Bouloukaki I, et al. Sleep patterns in patients with acute coronary syndromes. Sleep Med. 2010;11:149-153.
Schwartz SW, Cornoni-Huntley J, Cole S, Hays J, Blazer DG, Schocken DD. Are sleep complaints an independent risk factor for myocardial infarction? Ann Epidemiol. 1998;8:384-392.
Caska CM, Hendrickson BE, Wong MH, Ali S, Neylan T, Whooley MA. Anger expression and sleep quality in patients with coronary heart disease: Findings from the Heart and Soul Study. Psychosom Med. 2009;71:280-285.
Mundy E, Baum A. Medical disorders as a cause of psychological trauma and posttraumatic stress disorder. Curr Opin Psychiatry. 2004;17:123-127.
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193-213.
Weiss D. The impact of event scale: Revised. In: Wilson JP, Tang CS, eds. Cross-cultural assessment of psychological trauma and PTSD. New York: Springer; 2007:219-238.
First M, Spitzer R, Gibbon M, Williams J. Structured clinical interview for DSM-IV Axis I Disorders. Washington, DC: American Psychiatric Press; 1997.
Franklin CL, Sheeran T, Zimmerman M. Screening for trauma histories, posttraumatic stress disorders (PTSD) and subthreshold PTSD in psychiatric outpatients. Psychol Assess. 2002;14:467-471.
Goldberg RJ, Currie K, White K, et al. Six-month outcomes in a multinational registry of patients hospitalized with an acute coronary syndrome (the Global Registry of Acute Coronary Events [GRACE]). Am J Cardiol. 2004;93:288-293.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245-1251.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-571.
Paffenbarger RS Jr, Blair SN, Lee IM, Hyde RT. Measurement of physical activity to assess health effects in free-living populations. Med Sci Sports Exerc. 1993;25:60-70.
Beck A, Steer R, Garbin M. Psychometric properties of the Beck Depression Inventory: 25 years of evaluation. Clin Psychiatry Rev. 1988;8:77-100.
Paffenbarger RS, Wing AL, Hyde RT. Physical activity as an index of heart attack risk in college alumni. Am J Epidemiol. 1978;108:161-175.
Kuppermann M, Lubeck DP, Mazonson PD, et al. Sleep problems and their correlates in a working population. J Gen Intern Med. 1995;10:25-32.
Germain A, Buysse DJ, Shear MK, Fayyad R, Austin C. Clinical correlates of poor sleep quality in posttraumatic stress disorder. J Trauma Stress. 2004;17:477-484.
Sanchez-Ortuno MM, Edinger JD. Cognitive-behavioral therapy for the management of insomnia comorbid with mental disorders. Curr Psychiatry Rep. 2012;14:519-528.
Lichstein KL. Secondary insomnia: A myth dismissed. Sleep Med Rev. 2006;10:3-5.
Blechert J, Michael T, Grossman P, Lajtman M, Wilhelm FH. Autonomic and respiratory characteristics of posttraumatic stress disorder and panic disorder. Psychosom Med. 2007;69:935-943.
Yang AC, Tsai S-J, Yang C-H, Kuo C-H, Chen T-J, Hong C-J. Reduced physiologic complexity is associated with poor sleep in patients with major depression and primary insomnia. J Affect Disord. 2011;131:179-185.
Lijmer JG, Bossuyt PMM, Heisterkamp SH. Exploring sources of heterogeneity in systematic reviews of diagnostic tests. Stat Med. 2002;21:1525-1537.
Dørheim SK, Bondevik GT, Eberhard-Gran M, Bjorvatn B. Sleep and depression in postpartum women: A population-based study. Sleep. 2009;32:847-855.
Tsuno N, Besset A, Ritchie K. Sleep and depression. J Clin Psychiatry. 2005;66:1254-1269.
Knutson KL, Spiegel K, Penev P, Cauter EV. The metabolic consequences of sleep deprivation. Sleep Med Rev. 2007;11:163-178.
Voderholzer U, Al-Shajlawi A, Weske G, Feige B, Riemann D. Are there gender differences in objective and subjective sleep measures? A study of insomniacs and healthy controls. Depress Anxiety. 2003;17:162-172.
Loredo JS, Soler X, Bardwell W, Ancoli-Israel S, Dimsdale JE, Palinkas LA. Sleep health in U.S. Hispanic population. Sleep. 2007;33:962-967.
Koren D, Arnon I, Lavie P, Klein E. Sleep complaints as early predictors of posttraumatic stress disorder: A 1-year prospective study of injured survivors of motor vehicle accidents. Am J Psychiatry. 2002;159:855-857.
Creamer M, Bell R, Failla S. Psychometric properties of the Impact of Event Scale—Revised. Behav Res Ther. 2003;41:1489-1496.
Shemesh E, Yehuda R, Milo O, et al. Posttraumatic stress, nonadherence, and adverse outcome in survivors of a myocardial infarction. Psychosom Med. 2004;66:521-526.
Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. Depression and coronary heart disease: Recommendations for screening, referral, and treatment: A science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation. 2008;118:1768-1775.
Acknowledgments
This work was supported by grants HL-088117, HL-076857, HL-080665, HL-101663, and HL-084034 from the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH). Dr. Shaffer is supported by grants 12CRP8870004 from the American Heart Association and K23-HL112850 from NHLBI/NIH. Dr. Kronish is supported by grant K23-HL098359 from NHLBI/NIH.
Conflict of Interest Statement
The authors have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Shaffer, J.A., Kronish, I.M., Burg, M. et al. Association of Acute Coronary Syndrome-Induced Posttraumatic Stress Disorder Symptoms with Self-Reported Sleep. ann. behav. med. 46, 349–357 (2013). https://doi.org/10.1007/s12160-013-9512-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-013-9512-8