
Abstract
Background
Elevated nighttime blood pressure (BP) predicts hypertension and its complications in adulthood.
Purpose
This study aimed to assess the independent effects of race and family income on night/day BP among adolescents and to examine whether negative emotions, low positive resources, and unpleasant interactions during the day are also related.
Methods
Healthy African American and Caucasian high school students (N = 239) wore an ambulatory BP monitor for 48 h, recorded quality of ongoing interpersonal interactions, and completed questionnaires.
Results
African Americans and those with lower family income had higher night/day BP ratios. African Americans reporting greater negative emotions, lower positive resources, and more unpleasant interactions had higher night/day BP ratios.
Conclusions
Racial differences in night BP emerge by adolescence, independent of family income. African Americans, especially those high in negative emotions and low in positive resources, may be at higher relative risk for hypertension later in life in part due to elevated night BP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Normal circadian rhythm of blood pressure (BP) is characterized by a higher BP during the day and comparatively lower BP at night during sleep. Accumulating evidence shows that the absence of or a limited decline in nighttime BP relative to daytime BP, which is called BP nondipping, is an independent predictor of cardiovascular events and mortality [1–4]. Furthermore, BP nondipping has been implicated in the development of hypertension [5, 6] and is associated with complications, including target organ damage [5–7]. It has been postulated that a failure of nighttime BP to fall contributes to an overload on the cardiovascular system, and, thereby, inhibits the restorative processes of the body at night [8].
Research consistently shows that African American adults are more likely to exhibit BP nondipping, relative to Caucasians [9–11]. It is not established when in the life span these racial disparities emerge. Only three studies have examined racial differences in nocturnal BP decline among children and adolescents, two of which reported a higher prevalence of BP nondipping among African American youth [12–14]. Because elevated BP during childhood persists into adulthood and predicts adult hypertension [15], adolescence is a critical period during which trajectories to cardiovascular risk are established. Thus, investigating race and other factors related to BP nondipping during this period of biological, social, and psychological maturation could shed light on inequalities in cardiovascular morbidity and mortality in adulthood.
To fully comprehend race differences in BP nondipping, it is essential to consider socioeconomic status (SES). Research indicates that lower SES individuals are at greater risk for nondipping compared to higher SES individuals [16–20]. Because African Americans are overrepresented in lower SES positions [21], racial differences in BP nondipping may be attributed in part to racial disparities in SES. Consistent with this notion are findings that years of education largely attenuated the effect of race on BP nondipping among normotensive and hypertensive adults [19]. Moreover, being African American and low SES may interact to confer increased risk for nondipping and subsequent hypertension, as African Americans may be more vulnerable to the negative impact of lower SES environments. Indeed, only among African American adolescents from lower SES neighborhoods were perceptions of unfair treatment from others associated with higher night/day BP ratios [14]. A primary objective of this study was to test the independent and combined effects of race and SES on night/day BP ratios in healthy African American and Caucasian adolescents.
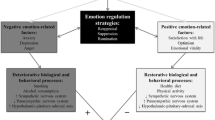
Understanding the pathways by which SES and race influence cardiovascular health is of great public health and clinical significance [22–24]. From a psychosocial perspective, both lower SES and minority status are thought to lead to greater exposure to stressful circumstances and their emotional sequelae, which, in turn, may lead to elevated cardiovascular risk [24, 25]. However, it is also recognized that psychosocial resources—including intrapersonal, interpersonal, and cultural resources—may be important in reducing the likelihood of adverse cardiovascular consequences [26, 27]. These factors may be especially applicable to understanding nondipping because stressful circumstances and negative emotions are known to disturb circadian rhythms [28–30].
Consistent with this perspective, a burgeoning literature finds that adults who exhibit BP nondipping have elevated scores on measures of anger, hostility, and depression [31–33], and there is preliminary evidence that suggests that African Americans may be particularly vulnerable to the toxic effects of negative emotions on the diurnal pattern of BP [34]. Less is known about positive resources in relation to nondipping. The few available studies report that high social support and high life purpose are associated with dipping in middle-aged adults [32, 35, 36]. A second aim of this study was to examine whether nondipping was associated with high levels of negative emotions and low levels of psychosocial resources among adolescents and whether accounting for these psychological factors attenuated the impact of race and SES.
Poor social relationships, including the level of conflict experienced in relationships, have also been associated with BP nondipping [37–39]. Conflictual interpersonal interactions with family and friends are a typical feature of adolescent life and are associated with negative emotions [40]. Ecological momentary assessment of ongoing conflictual and unpleasant encounters throughout the day may provide a more valid representation of social relationships than global self-report measure [41]. To date, only two ambulatory BP studies have examined interpersonal conflict by ecological momentary assessment, with conflict exhibiting positive associations with within-person fluctuations in systolic (S) BP and diastolic (D) BP in one study [42] and masked hypertension in the other [43]; these studies did not evaluate the effects on nighttime BP or night/day ratios. A third purpose of this study was to test the associations between cumulative exposure to conflictual and unpleasant interactions throughout the day and BP nondipping.
To meet study objectives, we measured ambulatory BP for two full days and nights during the school week in a sample of healthy African American and Caucasian high school students. The measures of nondipping were the ratios of night/day SBP and DBP measured during sleep and awake periods verified by actigraphy. At the time of BP assessment, students recorded the quality of their concurrent social interactions. Thus, our study was able to test the following hypotheses: Night/day BP ratios would be elevated among African American and low SES adolescents. Night/day ratios would be elevated among adolescents with high negative emotions and low positive resources scores, with statistical adjustment for emotions and resources attenuating any observed associations of night/day ratios and ethnicity and SES. Night/day ratios would be elevated among those who experienced conflictual, unpleasant encounters throughout the day. Furthermore, the study examined whether associations between psychosocial factors and night/day BP ratios would be stronger in African Americans, who may be more vulnerable because of their established risk for nondipping and hypertension in adulthood.
Method
Participants were 250 adolescents between the ages of 14 and 19 from an urban, integrated, public high school near Pittsburgh, PA, USA. Participants were recruited from health classes between 2008 and 2011 for an adolescent health project designed to measure risk factors for cardiovascular disease and sleep. Exclusionary criteria for study participation included parental report of children’s cardiovascular or kidney disease, usage of medication for emotional problems, diabetes or high blood pressure, as well as medication known to affect the cardiovascular system or sleep. Sixteen participants who expressed an interest in the study were ineligible to participate based on the exclusionary criteria, and seven students who signed consent forms did not actively enroll in the study. Of the 250 adolescents who enrolled in the study, two adolescents had body mass index (BMI) values that fell over four standard deviations from the sample mean (54.6 and 58.2) and were excluded from analyses. Also excluded were one adolescent who did not complete the ambulatory BP monitoring procedures and two participants who removed the BP cuff on at least one night of data collection. Six participants had missing data for family size, which precluded calculation of an imputed score for income, and four participants were missing questionnaire data. The final sample consisted of 239 adolescents.
Measures and Procedures
Overview
Participants were recruited during physical education classes in which trained staff presented the study objectives and protocol. Subsequently, parents/guardians of students who expressed an interest in the study were contacted for a screening phone interview. After obtaining signed informed consent from the parent/guardian and student, parents/guardians were interviewed regarding household SES and family history. Students were then scheduled to complete a 7-day study protocol, which included two school days and two nights of ambulatory BP monitoring, completion of a battery of psychosocial questionnaires via protected web access, a blood draw, and actigraphy. Upon completion of the study protocol, participants were compensated $100 for successful participation in the research project.
Ambulatory Blood Pressure Assessment
A Spacelabs Monitor 90217 was used to measure ambulatory BP for two days and two nights. This monitor uses the auscultatory method of BP assessment. A BP reading was taken every 30 min from 7:00 a.m. to 10:00 p.m. and hourly thereafter. Measurements were averaged across the night, starting when participants went to sleep and stopping when they reported awakening in daily diaries (verified by actigraphy) and across the remaining wake period. At least five readings across each night were required in order to calculate this average. Blood pressures that fell within the participant’s self-reported sleep window were used to calculate average nighttime BP; BP readings that were ±3 standard deviations from a participant’s individual mean were treated as outliers and excluded. Night/day ratio was defined as the ratio of average nighttime BP to average daytime BP for SBP and DBP separately. Accordingly, a higher score represents a smaller nocturnal decline relative to daytime BP or more BP nondipping. We chose the night/day SBP and DBP ratios as our primary measures because they provide continuous measures and maximize statistical power.
Measures
Socioeconomic Status
We utilized parental education and family income as indicators of SES. These two indicators are distinct in that income is often characterized as a resource measure and education as a prestige index of SES [21]. Parental education was the higher level of educational attainment of either mother or father or head of household, with 1 = grade school, 2 = high school diploma, 3 = associate degree, and 4 = college degree, and then summarized as lower than or equal to high school, or associate degree or higher. Family income was reported as gross annual family income in the categories of <$5,000, <$12,000, <$16,000, <$25,000, <$35,000, <$50,000, <$75,000, <$100,000, and >$100,000. To create a family size adjusted income, we first derived midpoints for the income categories, with the open ended top category being assigned a value of 50 % above its lower boundary. Thereafter, income was adjusted for the square root of the household size (i.e., the number of adults and children) and a log transformation was applied to reduce skewness of the distribution. Additionally, because the parents of 15 participants declined to provide information about their family income, we imputed income data by identifying families with similar structure (i.e., number of adults and children in the same household) and using the midpoint of the average income category for the comparable family constellations [17]. The results presented below were identical to those results based on excluding those with the imputed scores.
Assessments of Psychological Factors: Negative Emotions and Positive Resources
Four measures of negative emotions were included. The Positive and Negative Affect Schedule [44] consisted of 10 items each measuring global positive and negative dispositional affect. Participants were asked to indicate how much they feel each affect in general ranging from 1 (not at all) to 5 (extremely). Cronbach’s alpha coefficient for negative affect was 0.85. Depressive symptoms were assessed using the 20-item Center for Epidemiological Studies Depression (CES-D) scale [45]. Participants rated the frequency of experiencing each symptom in the past week, ranging from 1 (less than 1 day) to 4 (5–7 days). A sample item was “I was bothered by things that usually don’t bother me.” Higher scores indicated greater depressive symptoms. Cronbach’s alpha coefficient for the CES-D in this sample was 0.85. Anger was measured using the Spielberger Trait Anger Scale [46], which consists of 10 items related to the frequency with which the emotion of anger is generally experienced in relation to situations and interactions with others. Participants characterized how they generally felt, ranging from a 1 (almost never) to 4 (almost always). Sample items were, “I have a fiery temper” and “When I get frustrated, I feel like hitting someone.” Higher scores indicate greater trait anger. Cronbach’s alpha for trait anger was 0.87. Cynicism was assessed by 12 items from the Cook-Medley Hostility Scale [47]. Participants designated if they believed a statement to be true or false about the ways people behave. Sample items include, “It is safer to trust nobody” and “I think most people would lie to get ahead.” Higher scores indicate greater cynicism and the Cronbach’s alpha in this sample was 0.55.
Four measures of positive resources were included. Positive affect was derived from the Positive and Negative Affect Scale, described above; Cronbach’s alpha for positive affect was 0.82. Self-esteem was measured with 10 items from the Rosenberg Self-Esteem Scale [48]. Students characterized their agreement with statements regarding perceptions of self-worth using a scale ranging from 1 (strongly disagree) to 4 (strongly agree). A sample item is, “I feel that I am a person of worth, at least on an equal basis with others.” Higher scores are indicative of higher self-esteem. In our sample, the Cronbach’s alpha was 0.84. Optimism was measured using the six-item Life Orientation Test—Revised (LOT-R) [49]. Participants characterized their agreement with each item using a scale ranging from 0 (strongly disagree) to 4 (strongly agree), with 2 being a neutral response. A sample optimism item is, “In uncertain times, I usually expect the best.” The LOT-R overall score ranges from 0 to 24, and higher scores indicate greater optimism. The LOT-R showed moderate reliability; the Cronbach’s alpha coefficient was 0.60. Subjective social standing was measured using the MacArthur Scale of Subjective Social Standing (modified for adolescents) that was developed as a measure of people’s perceptions of their placement in the social hierarchy [50]. Using a picture of a ladder with nine rungs, adolescents indicated where they rank relative to other students in the school based on popularity, grades, respect, etc. The youth version of the MacArthur Scale is appropriate for those grades 7 and above or children aged 12 and older. This measure was considered to be a positive sense of self, relative to other students.
Principal components analysis with orthogonal varimax rotation was conducted on the scale scores from the above questionnaires. The Kaiser–Meyer–Olkin measure verified the sampling adequacy for the analysis, KMO = 0.72. Barlett’s test of sphericity χ 2(28) = 499.45, p < .01, indicated that correlations between measures were sufficiently large. Two components had eigenvalues over Kaiser’s criterion of 1 and in combination explained 55.5 % of the variance. Four measures (CES-D, PANAS Negative Affect, Spielberger Trait Anger, and Cook–Medley Cynicism) loaded > .55 on the first factor, labeled Negative Emotions, and four measures (PANAS Positive Affect, Rosenburg Self-Esteem, Optimism, and the Subjective Social Standing ladder) loaded > .61 on the second factor, labeled Positive Resources. Each score was standardized and added together to form composites.
Unpleasant Social Interactions
In conjunction with the daytime ambulatory BP recordings, participants reported via electronic diaries whether or not they had been engaged in a social interaction (via text, phone, internet, or in person) in the 10 minutes preceding each daytime BP recording. If “Yes” was indicated, participants answered two questions: “Did you have a conflict or disagreement with someone? Did you have a pleasant interaction with someone?” The responses ranged from 1 (not at all) to 6 (a lot). The responses for pleasantness and conflict averaged across the total number of responses provided across the measurement period were inversely related, r = −.42. The ratings of pleasantness were reverse coded and added to the ratings of conflict to make a total combined score, labeled unpleasant interaction score, across the total number of responses provided across the measurement period; eight participants with fewer than five recorded interactions were not included in the analysis of this variable.
Covariates
The covariates were age, sex, and BMI. Age and sex were determined by self-report. BMI was derived from weight and height measured on a calibrated scale nearest 0.1 kg and 0.1 cm, respectively; because of its distribution, a square root transformation was performed.
Statistical Analyses
Race and gender differences in SES, BP, negative emotions, positive resources, and unpleasant interaction scores were examined by 2 (race) × 2 (sex) ANOVAS. To test our hypotheses, we used linear regression, with covariates of age, sex, and BMI. To meet the first aim, in separate analyses for household income and parental education, the covariates, race, and the SES variable were entered at step 1, and the interaction of race and SES at step 2. To meet the second and third aims, after entering covariates plus race and household income, negative emotions, positive resources, and unpleasant interaction scores were entered separately in the second step. The change in the betas for race and SES were evaluated as to whether they were attenuated by the introduction of the psychosocial scores. Finally, the interactions between race and each of the psychosocial scores were calculated. Significant interactions with race were further examined by conducting race-stratified regressions. For illustration only, figures show the estimated means at one standard deviation above and below sample mean for continuous SES and psychosocial variables. Statistical significance was set at p < .05 (two-tailed) and was conducted with SPSS, Version 18 (SPSS Inc., Chicago, IL, USA).
Results
Sample Characteristics
The study sample included 239 participants, about half of whom were female, with a mean age of approximately 16 years. One hundred thirty-five participants self- reported their race as African American and 104 as Caucasian; two Hispanic participants were grouped with Caucasians. Results reported below were similar when the two Hispanic participants were removed from analyses. Approximately 22 % of the adolescents were obese (BMI ≥ 30). Using the criterion of <10 % decline in BP during sleep relative to daytime BP, 26 % of the adolescents would be categorized as nondippers for SBP and 4 % for DBP.
Table 1 shows the full sample characteristics as well as race differences in characteristics. African American adolescents had higher SBP ratios and nighttime SBP and lower household income than Caucasians. African Americans had lower negative emotions and higher positive resources scores than Caucasians, each of the scales contributing to the overall factor scores differed by race as well (data not shown). Only one significant interaction between race and sex emerged for BMI [F (1, 235) = 5.23, p = .02], with Caucasian males exhibiting the highest BMI (data not shown).
Table 2 shows the simple correlations among variables. Household income and parental education were modestly associated. Lower income was associated with higher SBP and DBP ratios. Negative emotion scores were positively correlated with SBP and DBP ratios. Additionally, negative emotions were inversely correlated with positive resources. As might be expected, adolescents who had higher negative emotion and lower positive resource scores reported more unpleasant social interactions throughout the two days of monitoring.
Influence of Race and Socioeconomic Status on Night/Day BP ratios
The results of linear regression models testing the independent associations of race and income with BP ratios are displayed in Table 3. Larger SBP ratios were observed among African Americans than among Caucasians, whereas larger DBP ratios were associated with lower household income (base models). Moreover, income interacted with race to predict SBP ratio. Race-stratified analyses revealed that among African American adolescents, lower income was associated with higher night/day SBP ratio (β = −.16, p = .05), but not among Caucasians (β = .12 p = .25; for illustration, see Fig. 1 for means of participants 1 SD above and below sample mean). There were no significant effects involving parental education, p’s > .25.

SBP night/day ratios according to family income scores (1 SD above and below mean)
Influence of Negative Emotions and Positive Resources on Night/day BP Ratios
Table 4 shows the results of the relations between negative emotions, positive resources, and each BP ratio, independent of variables in the base models (see Step 2). Only the summed negative emotions were related to SBP ratio and marginally to DBP ratio. Furthermore, the standardized beta for the association between race and SBP ratio (β = 0.147, p = .023) was not attenuated with the inclusion of negative emotions (β = 0.171, p = .01) in the model, and the relationship between family income and DBP ratio (β = −0.175, p = .009) was not attenuated with the inclusion of negative emotions (β = −0.179, p = .008) in the model.
Significant interactions emerged between race and negative emotions for both SBP and DBP ratios, and race and positive resources for DBP ratio (Table 4, Step 3). Race-stratified analyses revealed that among African Americans, higher scores on negative emotions were associated with higher night/day SBP (β = .30, p < .01; r 2 change = .08) and DBP ratios (β = .29, p = .001, r 2 change = .08), but not among Caucasians (β = −.04 p = .69) and (β = −.06 p = .57), respectively. Similarly, lower scores on positive resources were associated with higher DBP ratio only among African Americans (β = −.20, p < .02; r 2 change = .04), but not Caucasians (β = .06 p = .59). The above interactions are illustrated in Figs. 2 and 3 that depict the analyses of the simple slopes at one standard deviation above and below the mean. Of note, the effects of positive resources (β = −.16 p = .05) on DBP ratios among African Americans were independent of negative emotions when both were introduced into the model (β = .27, p < .01). Stratified analyses for African Americans showed that the inclusion of negative emotions along with the covariates of age, sex, and BMI accounted for 22 and 21 % percent of the variance in SBP and DBP ratio, respectively. With the addition of positive resources in the same model as negative emotions, 23 % variance in DBP ratios was explained.

SBP night/day ratios according to negative emotion scores (1 SD above and below mean)

DBP night/day ratios according to positive resources scores (1 SD above and below mean)
Influence of Unpleasant Social Interactions on Night/Day BP Ratios
Unpleasant interactions were not associated with DBP and SBP ratios. However, a significant interaction between race and unpleasant interactions was observed (Table 4, step 3), with higher unpleasant interactions associated with higher SBP ratio among African Americans (β = −.19, p = .03, r 2 change = .02), but not Caucasians (β = .09, p = .40) in race-stratified analyses. Figure 4 plots the regression of race by unpleasant interaction (at one standard deviation above and below the mean) on SBP ratio.

SBP night/day ratios according to unpleasant interactions scores averaged across days (1 SD above and below mean)
Discussion
The first aim of this study was to evaluate racial differences in BP nondipping in adolescents and to extend the findings by examining whether expected racial differences were independent of SES. We found that African American adolescents showed higher SBP night/day ratio than Caucasians, independent of both parental education and family income. Lower family income was associated with higher SBP ratio for African Americans only and was associated with higher DBP ratio in both African Americans and Caucasians. The blunted BP decline observed among African Americans and low income adolescents in this study is consistent with the considerable evidence on the prevalence of BP nondipping in African American and low SES adults [9–11, 16–20]. Taken together, the current study replicates the extant findings in the literature regarding the independent association between SES and BP dipping and demonstrates that the association between race and night/day BP ratio in adolescents cannot be explained by racial disparities in family income.
The second aim of this study was to examine whether negative emotions and positive resources would be related to BP nondipping and would attenuate the associations of race and SES. We hypothesized that adolescents who reported high negative emotions and low positive resources would exhibit higher night/day ratios. Our results showed that higher scores on the composite measure of negative emotions (anger, depressive symptoms, negative affect, and cynicism) were associated with SBP night/day ratios. On the other hand, neither negative emotions nor positive resources explained race and SES effects on BP dipping. This relationship between negative emotions and BP dipping is in line with previous findings in adults [28–32]. The finding that negative emotions did not account for demographic differences in BP is also consistent with previous research, as only one study found that hostility and anger expression explained racial differences in nocturnal decreases [31], whereas three additional studies [19, 51, 52] did not observe that individual negative emotions explained race differences in BP nondipping.
We also found that race moderated the association between both negative emotions and positive resources and BP dipping. Specifically, among African Americans only, higher negative emotion scores were associated with higher SBP and DBP ratios, with each component of the negative emotions factor related (data not shown). Furthermore, low positive resources, especially low positive affect and low optimism (data not shown), were associated with higher DBP ratio. In contrast, negative emotions and positive resources were unrelated to nocturnal decline among Caucasian adolescents. These findings coincide with findings by Shapiro et al. [34] and Steffen et al. [33] observed in African American adults and suggest that African American adolescents may be particularly vulnerable to the effects of high levels of negative emotions and low positive resources.
The third goal of this study was to evaluate the role of daily interpersonal stress in BP nondipping. We found no evidence that level of unpleasant interactions reported over two days via ecological momentary assessment mitigated the effects of either race or SES on night/day ratio. However, parallel to our findings on the moderating effects of negative emotions and positive resources, we did find that more unpleasant interactions were associated with higher SBP ratios among African American adolescents, but not among Caucasians.
Taken together, these findings highlight the significance of negative emotions, positive resources, and unpleasant interactions for understanding BP nondipping among African American adolescents. One plausible explanation of race differences in the influence of these psychosocial variables could be different patterns of cardiovascular reactivity among African Americans and Caucasians, with African Americans exhibiting more alpha-adrenergic (vascular) response to laboratory stressors and Caucasians more beta-adrenergic (cardiac), reactivity [53]. Greater vascular reactivity may accelerate stiffening of the vasculature, leading to eventual hypertension, in contrast to beta-adrenergic reactivity that may have more direct effects on atherosclerosis. Indeed, in a different sample of adolescents than the present, among African Americans, increasing negative mood states (assessed by ecological momentary assessment) predicted greater increases in ambulatory heart rate and DBP measured across two schools [54]. Relatedly, African Americans’ greater sensitivity to the effects of psychosocial factors on nocturnal BP decline could reflect diathesis stress processes [55], such that physiological vulnerabilities conferred by race and exposure to negative psychosocial factors interact to place African Americans on trajectories for disruptions in circadian BP regulation and later hypertension.
There are several strengths of this study, including the examination of BP dipping in an adolescent sample with representation of African American and Caucasian participants, which permitted the examination of race differences. Additionally, we assessed BP over two nights, which increased the reliability of our nondipping measure compared to most studies that have examined dipping over a single 24-h period, and we utilized self-reported sleep and wake times confirmed by objective actigraphy data rather than imposing arbitrary night and day periods. Finally, we considered positive as well as negative psychosocial factors in our explorations of potential pathways leading to BP nondipping.
Notwithstanding the aforementioned strengths, the findings should be interpreted in light of several limitations. First, our study did not have a broad range of SES as participants were from families of a low to middle class background from a single urban high school. Thus, the restricted family income and homogenous sample limit the generalizablity of our findings. The excellent health of the adolescent sample also limited the range of ambulatory BP. Finally, the cross-sectional design of the study does not permit inferences about causality.
In summary, our findings suggest both African American and lower SES adolescents may be at risk for elevated night/day BP ratios. Furthermore, African American adolescents who report greater negative emotions, lower positive resources, and more unpleasant social interactions may be particularly vulnerable to having elevated night/day BP ratios. Given that the sample consisted of healthy, normotensive adolescents, it is striking that elevated night/day BP ratios were associated with race, SES, and negative emotions. Should these associations persist into adulthood, such adolescents may be at high risk for later hypertension and its complications. Interventions focused on enhancing the psychological resources of African American adolescents may reduce their risk for later hypertension.
References
Ohkubo T, Hozawa A, Yamaguchi J, et al. Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: The Ohasama study. J Hypertens. 2002;20:2183-2189.
Routledge F, McFetridge-Durdle J. Nondipping blood pressure patterns among individuals with essential hypertension: A review of the literature. Eur J Cardiovasc Nurs. 2007;6:9-26.
Staessen JA, Thijs L, Fagard R, et al. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. Systolic Hypertension in Europe Trial Investigators JAMA. 1999;282:539-546.
Fagard RH, Thijs L, Staessen JA, et al. Night–day blood pressure ratio and dipping pattern as predictors of death and cardiovascular events in hypertension. J Hum Hypertens. 2009;23:645-653.
Timio M, Venanzi S, Lolli S, et al. “Non-dipper” hypertensive patients and progressive renal insufficiency: a 3-year longitudinal study. Clin Nephrol. 1995;43:382-387.
Cuspidi C, Macca G, Sampieri L, et al. Target organ damage and non-dipping pattern defined by two sessions of ambulatory blood pressure monitoring in recently diagnosed essential hypertensive patients. J Hypertens. 2001;19:1539-1545.
Izzedine H, Launay-Vacher V, Deray G. Abnormal blood pressure circadian rhythm: A target organ damage? Int J Cardiol. 2006;107:343-349.
Stolarz K, Staessen JA, O’Brien ET. Night-time blood pressure: Dipping into the future? J Hypertens. 2002;20:2131-2133.
Agyemang C, Bhopal R, Bruijnzeels M, Redekop WK. Does nocturnal blood pressure fall in people of African and South Asian descent differ from that in European white populations? A systematic review and meta-analysis. J Hypertens. 2005;23:913-920.
Hyman DJ, Ogbonnaya K, Taylor AA, Ho K, Pavlik VN. Ethnic differences in nocturnal blood pressure decline in treated hypertensives. Am J Hypertens. 2000;13:884-891.
Profant J, Dimsdale JE. Race and diurnal blood pressure patterns. A review and meta-analysis Hypertension. 1999;33:1099-1104.
Belsha CW, Spencer HJ 3rd, Berry PL, Plummer JK, Wells TG. Diurnal blood pressure patterns in normotensive and hypertensive children and adolescents. J Hum Hypertens. 1997;11:801-806.
Harshfield GA, Wilson ME, Treiber FA, Alpert BS. A comparison of ambulatory blood pressure patterns across populations. Blood Press Monit. 2002;7:265-269.
Beatty DL, Matthews KA. Unfair treatment and trait anger in relation to nighttime ambulatory blood pressure in African American and white adolescents. Psychosom Med. 2009;71:813-820.
Chen X, Wang Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation. 2008;117:3171-3180.
Campbell TS, Key BL, Ireland AD, Bacon SL, Ditto B. Early socioeconomic status is associated with adult nighttime blood pressure dipping. Psychosom Med. 2008;70:276-281.
Hickson DA, Diez Roux AV, Wyatt SB, et al. Socioeconomic position is positively associated with blood pressure dipping among African-American adults: The Jackson Heart Study. Am J Hypertens. 2011;24:1015-1021.
Stepnowsky CJ Jr, Nelesen RA, DeJardin D, Dimsdale JE. Socioeconomic status is associated with nocturnal blood pressure dipping. Psychosom Med. 2004;66:651-655.
Spruill TM, Gerin W, Ogedegbe G, et al. Socioeconomic and psychosocial factors mediate race differences in nocturnal blood pressure dipping. Am J Hypertens. 2009;22:637-642.
Fortmann AL, Gallo LC, Roesch SC, et al. Socioeconomic status, nocturnal blood pressure dipping, and psychosocial factors: A cross-sectional investigation in Mexican-American women. Ann Behav Med. 2012;44:389-398. doi:10.1007/s12160-012-9387-0.
Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: Concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18:341-378.
Adler NE. Health disparities through a psychological lens. Am Psychol. 2009;64:663-673.
Adler NE, Boyce T, Chesney MA, et al. Socioeconomic status and health: The challenge of the gradient. Am Psychol. 1994;49:15-24.
Myers HF. Ethnicity- and socio-economic status-related stresses in context: An integrative review and conceptual model. J Behav Med. 2009;32:9-19.
Gallo LC, Matthews KA. Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychol Bull. 2003;129:10-51.
Matthews KA, Gallo LC. Psychological perspectives on pathways linking socioeconomic status and physical health. Annu Rev Psychol. 2011;62:501-530.
Hobfoll SE. Conservation of resources: A new attempt at conceptualizing stress. Am Psychol. 1989;44:337-370.
Kario K, Schwartz JE, Davidson KW, Pickering TG. Gender differences in associations of diurnal blood pressure variation, awake physical activity, and sleep quality with negative affect: The work site blood pressure study. Hypertension. 2001;38:997-1002.
Mellman TA, Brown DD, Jenifer ES, Hipolito MS, Randall OS. Posttraumatic stress disorder and nocturnal blood pressure dipping in young adult African Americans. Psychosom Med. 2009;71:627-630.
Tomfohr L, Cooper DC, Mills PJ, Nelesen RA. Everyday discrimination and nocturnal blood pressure dipping in black and white Americans. Psychosom Med. 2010;72:1-7.
Thomas KS, Nelesen RA, Dimsdale JE. Relationships between hostility, anger expression, and blood pressure dipping in an ethnically diverse sample. Psychosom Med. 2004;66:298-304.
Mezick EJ, Matthews KA, Hall M, et al. Low life purpose and high hostility are related to an attenuated decline in nocturnal blood pressure. Health Psychol. 2010;29:196-204.
Steffen PR, McNeilly M, Anderson N, Sherwood A. Effects of perceived racism and anger inhibition on ambulatory blood pressure in African Americans. Psychosom Med. 2003;65:746-750.
Shapiro D, Goldstein IB, Jamner LD. Effects of cynical hostility, anger out, anxiety, and defensiveness on ambulatory blood pressure in black and white college students. Psychosom Med. 1996;58:354-364.
Cooper DC, Ziegler MG, Nelesen RA, Dimsdale JE. Racial differences in the impact of social support on nocturnal blood pressure. Psychosom Med. 2009;71:524-531.
Rodriguez JC, Burg MM, Meng J, et al. Effect of social support on nocturnal blood pressure dipping. Psychosom Med. 2008;70:7-12.
Troxel WM, Buysse DJ, Hall M, et al. Social integration, social contacts, and blood pressure dipping in African-Americans and whites. J Hypertens. 2010;28:265-271.
Holt-Lunstad J, Birmingham W, Jones BQ. Is there something unique about marriage? The relative impact of marital status, relationship quality, and network social support on ambulatory blood pressure and mental health. Ann Behav Med. 2008;35:239-244.
Holt-Lunstad J, Jones BQ, Birmingham W. The influence of close relationships on nocturnal blood pressure dipping. Int J Psychophysiol. 2009;71:211-217.
Steinberg L. Autonomy, conflict, and harmony in the family relationship. Cambridge: Harvard University Press; 1990.
Kamarck TW, Schwartz JE, Shiffman S, Muldoon MF, Tyrell-Sutton K, Janicki DL. Daily experience and cardiovascular disease risk. J Pers. 2005;73:1-23.
Kamarck TW, Janicki DL, Shiffman S, et al. Psychosocial demands and ambulatory blood pressure: A field assessment approach. Physiol Behav. 2002;77:699-704.
Schoenthaler AM, Schwartz J, Cassells A, Tobin JN, Brondolo E. Daily interpersonal conflict predicts masked hypertension in an urban sample. Am J Hypertens. 2010;23:1082-1088.
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54:1063-1070.
Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385-401.
Spielberger CD, Jacobs G, Russell S, Crane RS. Assessment of anger: The State-Trait Anger Scale. In: J. N. B. C. D. Spielberger, ed. Advances in personality assessment (Vol. 2). Hillsdale: Lawrence Erlbaum; 1983:159-187.
Cook WW, Medley DM. Proposed hostility and pharisaic-virtue scales for the MMPI. J Applied Psychol. 1954;38:414-418.
Rosenberg M. Society and adolescent self-image. Princeton: Princeton University Press; 1965.
Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J Pers Soc Psychol. 1994;67:1063-1078.
Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychol. 2000;19:586-592.
Ituarte PH, Kamarck TW, Thompson HS, Bacanu S. Psychosocial mediators of racial differences in nighttime blood pressure dipping among normotensive adults. Health Psychol. 1999;18:393-402.
Linden W, Klassen K, Phillips M. Can psychological factors account for a lack of nocturnal blood pressure dipping? Ann Behav Med. 2008;36:253-258.
Treiber FA, Musante L, Braden D, et al. Racial differences in hemodynamic responses to the cold face stimulus in children and adults. Psychosom Med. 1990;52:286-296.
McGrath JJ, Matthews KA, Brady SS. Individual versus neighborhood socioeconomic status and race as predictors of adolescent ambulatory blood pressure and heart rate. Soc Sci Med. 2006;63:1442-1453.
Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: Implications for the depressive disorders. Psychol Bull. 1991;110:406-425.
Acknowledgments
This work was supported by grants from the National Institutes of Health (HL07560 and HL025767).
Conflict of Interest Statement
The authors have no conflicts to disclose.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Burford, T.I., Low, C.A. & Matthews, K.A. Night/Day Ratios of Ambulatory Blood Pressure Among Healthy Adolescents: Roles of Race, Socioeconomic Status, and Psychosocial Factors. ann. behav. med. 46, 217–226 (2013). https://doi.org/10.1007/s12160-013-9487-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-013-9487-5