
Abstract
Background
Everyday discrimination scale scores are associated with increased ambulatory blood pressure (BP) and reduced nocturnal dipping, and the endothelin-1 (ET-1)/Lys198Asn polymorphism is associated with increased resting BP and exaggerated BP reactivity among African Americans compared to European Americans. Combined influences of these factors on BP control are unknown.
Purpose
This study tested the hypothesis of a three-way interaction between ethnicity, ET-1 carrier status, and everyday discrimination upon ambulatory BP and nocturnal dipping.
Methods
Baseline laboratory anthropometrics and the everyday discrimination scale were completed by 352 (175 African American) young adult normotensives, followed by 24-h ambulatory BP monitoring.
Results
For nocturnal dipping, multiple regression models controlling for age, sex, ethnicity, and body mass index revealed significant three-way ET-1 × everyday discrimination × ethnicity interactions. Specifically, among African American ET-1 T-allele carriers, increases in everyday discrimination led to reduced nocturnal dipping.
Conclusions
African Americans that carry the ET-1/Lys198Asn T-allele and report higher everyday discrimination scores may be at particular risk for reduced nocturnal dipping.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the USA, cardiovascular diseases including heart disease and stroke is the leading cause of mortality, accounting for more than one third (33.6 %) of all deaths [1]. Although a myriad of comorbid factors contribute to cardiovascular disease development, epidemiologic studies have shown that blood pressure (BP) levels are monotonically associated with future cardiovascular disease development [2]. Multiple studies have shown that ambulatory BP is a better predictor of hypertensive organ damage than clinically assessed BP [3–6]. In addition, lack of nocturnal dipping (i.e., typically considered a nocturnal decline of 10 % or more [7]) has been found to independently predict mortality and cardiovascular events in hypertensive patients without previous cardiovascular disease history, even after adjustment for 24-h ambulatory BP [8].
Increased resting and ambulatory BP and reduced nocturnal dipping among African American adolescents and adults compared to European Americans are well-documented. Concomitant life stressors (e.g., lower socioeconomic status, exposure to discrimination) have been shown to further augment these ethnic group differences [9–12]. Specific to African Americans and nocturnal BP, increased report of unfair treatment has been significantly related to reduced nocturnal dipping [13–16]. Interestingly, two of these studies [15, 16] found that everyday discrimination mediated dipping among both European Americans and African Americans. Why these differences are more often associated for African Americans compared to European Americans in some studies is not well-understood.
In a review paper, Brondolo [17] describes the work of Broman [18] and reported there was no effect of coping as a response to perceived discrimination or an impact of self-reported discrimination on clinician-diagnosed hypertension and/or heart disease. However, in a later community study with African Americans and Latin Americans, she concluded that perceived discrimination was positively associated to nocturnal dipping even when personality factors and socioeconomic status were controlled [13]. In a recent epidemiological study, researchers examined active coping (i.e., John Henryism) and hypertension status among 4,567 African Americans; their results concluded that, while John Henryism is correlated with age, it does not significantly correlate with hypertension status [19]. Finally, although coping style was not directly assessed, Cooper et al. [20] examined the effects of perceived discrimination and socioeconomic status upon nocturnal dipping and plasma endothelin-1 (ET-1) between European Americans and African Americans. The results from their study showed that African Americans with higher levels of perceived discrimination also had significantly higher levels of ET-1 even after controlling for socioeconomic status; their results suggest that the interactive relationship between ET-1 and increased stress via perceived discrimination upon BP control affects African Americans and European Americans differently.
ET-1, a potent vasoconstrictor, and endothelium-derived relaxing factor (primarily nitric oxide) are produced by vascular smooth muscle cells and must maintain a delicate balance for BP to remained controlled. Differences between circulating concentrations and/or receptor sensitivity may be partially responsible for exacerbations of BP among African Americans. Previous reactivity studies that examined hypertensive adults and normotensive adolescents and adults have found that African Americans exhibit higher plasma ET-1 increases compared to European Americans when behaviorally stressed [21–24].
Research supports that sympathetic nervous system activity may also contribute to ethnic BP control differences, with previous research findings revealing diurnal pressure variation between African Americans and European Americans [25–27]. It remains unknown if these ethnic variations are truly environmentally driven, but some literature examining geographical influence and ethnic variation is supportive of this view. Fumo [28] examined European Americans, African Americans, and West Africans matching for age, sex, and daytime BP; nonsignificant differences between European Americans and West Africans and significant differences in African Americans when compared to both European Americans and West Africans in nocturnal dipping suggested that previously found racial differences between European Americans and African Americans were likely environmental in origin. In addition, African Americans and West Africans had similar cation excretion rates (i.e., sodium, potassium) but differed in BP patterns and cardiac masses, thus ruling out divergence in sodium or potassium intake as explanations for ethnic group differences in the USA.
In addition to environmental differences, the unexplained heterogeneity between European Americans and African Americans may be at least partially due to genetic differences in the ability for the endothelium to maintain vascular tone. When environmental stressors heighten sympathetic nervous system activity, vasoconstricting factors are released from sympathetic nerve terminals; to maintain tonic balance, vasodilating factors from the endothelium are released. Harris and Matthews [29] provide an extensive review of the dynamic interplay between the autonomic nervous system and the endothelium, suggesting that endothelial α2-adrenoreceptors release nitric oxide to counteract vasoconstriction caused by the α1-adrenergic receptor stimulation of the vascular smooth cell; they also report that less is known about β-adrenoreceptors, but nitric oxide-mediated vasorelaxation has been speculated. The interplay of mechanistic pathways from previously published stress-induced biobehavioral cardiovascular disease models (i.e., the renin–angiotensin–aldosterone system, the sympathetic nervous system, and the endothelial system) corroborates with their interpretation that an abnormality in either the autonomic nervous system or endothelial system may negatively affect vascular tone, leading to essential hypertension development and eventually cardiovascular disease [30–32].
Previous findings support a gene × environment model of stress-induced essential hypertension [30, 33], suggesting that individuals with genetic susceptibility for essential hypertension who are exposed to frequent environmental stress and/or other stress-related potentiating factors (e.g., ineffective coping skills) will be most likely to exhibit the greatest BP stress reactivity, higher resting BP levels, and eventually develop essential hypertension and cardiovascular disease. The model has not been examined with nocturnal dipping, but evidence is pertinent to the previously described balance between the autonomic nervous system and the endothelium system (see bold pathways in Fig. 1).

Gene × environment (G × E) model of stress-induced essential hypertension endothelial and autonomic nervous system imbalance. HPA hypothalamic–pituitary–adrenal axis, SNS sympathetic nervous system, ES endothelial system, RAAS renin–angiotensin–aldosterone system, SES socioeconomic status
The ET-1 gene is localized on chromosome 6, spans 5.5 kb, and contains 5 exons and 4 introns and has been identified as one candidate gene for essential hypertension and cardiovascular disease [34]. A G-to-T transversion predicting a lysine–asparagine change at amino acid 198 (Lys198Asn, i.e., rs5370) single-nucleotide polymorphism has been associated with increased BP levels from adolescence to middle age in Japanese, European Americans, and African Americans [35–37]. Exaggerated BP reactivity to laboratory stressors among those exposed to background stress-related factors has been reported. For example, T-allele carriers from lower socioeconomic status backgrounds exhibited greater BP increases to a video-game challenge compared the other subgroups [21]. Rabineau et al. [38] found vasoconstrictive reactivity to behavioral stress was the highest among T-allele carriers with poor anger management skills. No previous studies have examined the combined effects of everyday discrimination and the Lys198Asn single-nucleotide polymorphism upon nocturnal BP between European Americans and African Americans. However, this relationship has been shown to modulate ambulatory BP improvements as a result of 12-week behavioral stress reduction interventions among African American adolescents. In a recent study, Gregoski et al. [39] found that, even when beneficial coping strategies were used, participants who were ET-1/Lys198Asn carriers and reported high everyday discrimination had no improvements in BP control compared to noncarriers or carriers who reported lower levels of discrimination.
The previous study did not include European American participants and everyday discrimination is potentially more salient among African American participants [40]. However, the purpose of the current study was to further explore this gene × environment relationship (i.e., everyday discrimination/unfair treatment × Lys198Asn carrier status) as a collective source of autonomic nervous system and endothelial imbalance and determine if this interaction significantly differentiates nocturnal ambulatory BP levels indicative of dipping status between African Americans and European Americans. No previous studies have examined the interactive influence of everyday discrimination and Lys198Asn carrier status on ambulatory BP and nocturnal BP dipping despite the potent effects upon BP control found independently among these factors.
Methods
Subjects
The present study comprised subjects from a longitudinal cohort, which was established in 1989, to study the development of biobehavioral risk factors for cardiovascular disease and is fully described elsewhere [41]. It included almost equal numbers of European Americans and African American participants with evaluations conducted annually. The Institutional Review Board at the Medical University of South Carolina and Georgia Regents University had given approval for the study. Informed consent was obtained on all subjects and by parents if subjects were <18 years of age. All participants were screened and included for participation in the study if they had no history of congenital heart defect, diabetes, sickle cell anemia, asthma, or any chronic illness or psychological/health problem that required regular pharmacological treatment.
The original sample included 587 participants. However, of these 587, 15 classified themselves as an ethnicity other than European American or African American, 177 refused to complete ambulatory BP measurements, 12 refused or did not receive genotyping, 30 did not fully complete everyday discrimination measures, and 1 was omitted for missing anthropometric data. As a result, the current sample comprised 352 participants (190 female, 175 African American), with an average age of 18.32 ± 2.7 years, and utilized information from the first visit that participants completed everyday discrimination measures. As described, participants were included if they had completed genotyping, everyday discrimination measures, anthropometrics, and wore the ambulatory BP monitor for a 24-h period.
Measurements
Anthropometric Measures
Height and weight were measured as described elsewhere [41]. Body mass index (BMI) was calculated as a measure of general adiposity, BMI z-scores (BMI-Z) adjusted for gender and age were created based on the Center for Disease Control growth charts.
Genotyping
Genomic DNA was extracted from buccal cells using QiaAmp DNA Blood Mini Kits (Qiagen). The extracted DNA was stored at −80 °C until analyzed. The Lyn/Asn amino acid change at codon 198 of the ET-1 gene was detected by polymerase chain reaction followed by direct sequence analysis, as previously described elsewhere [35].
Ambulatory BP Evaluation
Ambulatory systolic blood pressure (SBP) and diastolic blood pressure (DBP) were recorded for 24 h using Spacelabs 90207 monitors (Spacelabs, Inc., Issaquah, WA, USA). Measurements were preset to record every 30 min for sleep hours and every 20 min otherwise, based on each participant’s self-reported sleep schedule. Ambulatory BP monitoring has been shown to be a better predictor of essential hypertension than casual BP [42]. The instrument has been validated [43] and acceptability of ambulatory readings was based on established criteria [44]. Hourly averages were obtained by averaging all readings for each clock hour across daytime (8 a.m. to 10 p.m.) and nighttime (12 a.m. to 6 a.m.) periods, as suggested by the European Society of Hypertension Working Group on Blood Pressure Monitoring [45]. Transitional periods from 6 a.m. to 8 a.m. and from 10 p.m. to midnight were not included in the analyses [46]. To be included in the analyses, hourly averages for SBP and DBP required a minimum of 50 % of total possible evaluations for the respective time period.
In some studies, nocturnal dipping has been dichotomously defined as a reduction of at least 10 % compared to daytime values. However, continuous nocturnal BP dipping variables calculated using average daytime BP minus average nighttime BP have been reported to have greater stability [47] and were used in this study. The established protocol for the longitudinal study was to conduct a single 24-h recording as preliminary work indicated low acceptance by participants in wearing the monitor for longer durations.
Everyday Discrimination
The everyday discrimination scale was used to assess chronic psychosocial stress through the form of everyday discrimination [48, 49]. The everyday discrimination scale is purposed to capture more subtle experiences than overt forms of discrimination (e.g., nonrandom police stops based on racial profiling) and is framed in the context of unfairness so it can be administered to a variety of ethnic groups [16, 49]. It was administered to each participant via paper and pencil as part of a battery of psychosocial questionnaires. The everyday discrimination scale is comprised of nine items with a six-point response format: almost every day, at least once a week, a few times a month, a few times a year, less than once a year, and never. There is some evidence that it may have slightly more salience with certain ethnic groups [40], but it has been found to have good internal consistency with α = 0.88 [50] and previous principal component analysis supported it being a unidimensional construct [48]. Cronbach’s α was 0.85 in the current study.
Results
Only six European Americans and six African Americans were homozygous for the T-allele. As a result, genotypes were defined as carriers (GT and TT) and noncarriers (GG) of the T-allele. Genotyping frequencies were in Hardy–Weinberg equilibrium χ 2(1, 351) = 1.97, p = 0.16. There were no statistical differences in allele frequency by ethnicity χ 2(2, 351) = 1.89, p = 0.17. As shown in Table 1, there were some initial significant baseline differences between European Americans and African Americans for age and BMI-Z with African Americans being approximately 6 months older on average than European Americans and having a slightly higher BMI-Z.
Daytime and Nighttime ABP
To determine the unique contribution of carrier status × everyday discrimination on ambulatory daytime and nighttime SBP and DBP, multiple linear regression analyses were performed with ethnicity, age, sex, everyday discrimination scores, BMI-Z, and ET-1/Lys198Asn entered as covariates on the first block. The interaction terms of ethnicity × everyday discrimination score, carrier status × ethnicity, and ethnicity × ET-1/Lys198Ans were entered in the second block. Finally, the three-way interaction of ethnicity × ET-1 × everyday discrimination score was added in the third block of the regression model. Continuous variables represented age, everyday discrimination scores, and BMI-Z. Ethnicity, sex, and ET-1/Lys198Asn were dummy coded. Tolerance and variance inflation factors did not detect redundancy among predictors or multicollinearity. The results of these analyses are shown in Table 2.
For daytime SBP, the first block of the model containing ethnicity, age, sex, BMI-Z, everyday discrimination scale, and ET-1/Lys198Asn was significant F(6, 334) = 20.32, p < 0.001 and accounted for 26.7 % of the variance in the model. The terms in the second and third blocks did not significantly account for additional variance in the model. Significant terms in the first block of the model included a significant main effect for age and sex. Being male was associated with higher daytime SBP, and increases in age were associated with increased SBP.
For nighttime SBP, the first block of the model was significant F(6, 344) = 27.48, p < 0.001 and accounted for 32.4 % of the variance in the model. The terms in the second and third blocks did not significantly account for additional variance in the model. Significant terms in the first block of the model included a significant main effect for sex, age, and BMI-Z. As with daytime SBP, male gender was associated with higher nighttime SBP, and increases in age and BMI-Z were associated with increased SBP.
For daytime DBP, the first block of the model was significant F(6, 334) = 7.813, p < 0.001 and accounted for 12.3 % of the variance in the model. The terms in the second and third blocks did not significantly account for additional variance in the model. Significant terms in the first block of the model included a main effect for age and BMI-Z. Increases in age were associated with increased DBP, and increases in BMI-Z were associated with decreased DBP.
For nighttime DBP, the first block of the model was significant F(6, 344) = 27.48, p < 0.001 and accounted for 21.4 % of the variance in the model. The terms in the second block did not significantly account for additional variance in the model. However, the third block that included the three-way term ethnicity × ET-1 × everyday discrimination scores significantly accounted for an additional 2.8 % of variance in the model. Similar to daytime DBP, significant terms in the first block of the model included a significant main effect for age and BMI-Z. Increases in age were associated with increased DBP, and increases in BMI-Z were associated with decreased DBP. The significant three-way interaction for ethnicity × ET-1 × everyday discrimination revealed that increases in discrimination significantly increased DBP for African American T-allele carriers compared to other subgroups in the model.
SBP and DBP Dipping
Analyses for SBP and DBP dipping were conducted in a similar fashion to daytime and nighttime SBP and DBP models using continuous nocturnal BP dipping (i.e., average daytime BP minus average nighttime BP) as the dependent measure. For SBP dipping, the first block of the model was significant F(6, 334) = 3.857, p = 0.001 and accounted for 6.5 % of the variance in the model. The interactive terms of ethnicity × everyday discrimination scores, carrier status × ethnicity, and ethnicity × ET-1/Lys198Ans entered in the second block accounted for an additional 0.1 % of variance in the model and was not significantly different from the model in the first step. However, the model including the third block which added the three-factor interaction of carrier status × everyday discrimination scores × ethnicity and subsumed two-way interactions and main effect terms was a significant change from the original model F ∆(1, 330) = 6.586, p = 0.01, accounting for an additional 1.8 % of the variance. Significant terms in the final model included the three-way ET-1 × everyday discrimination scores × ethnicity interaction (p = 0.011) and a significant main effect for ethnicity (p = 0.007). As shown in Table 3, being African American corresponded with decreased dipping and being African American and a T-allele carrier of ET-1 corresponded to an additional significant reduction in nocturnal dipping when discrimination increases compared to other subgroups and controlling for other variables.
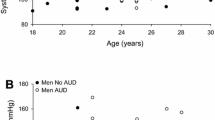
For DBP dipping, the first block of the model was significant F(6, 334) = 2.602, p = 0.018, accounting for 4.5 % of the variance in the model. The terms in the second block of the model did not significantly account for additional variance. However, the third block including the three-factor interaction of carrier status × everyday discrimination scores × ethnicity was significantly different from the original model F ∆(1, 330) = 7.11, p = 0.008 and accounted for an additional 2.0 % of the variance. Significant terms in the final model included the three-way ET-1 × everyday discrimination scores × ethnicity interaction and a subsumed two-way interaction between ET-1 × ethnicity as well as a significant main effect for ethnicity. Results were similar to SBP dipping such that being African American corresponded with decreased dipping and being African American and a T-allele carrier of ET-1 corresponded with an additional significant reduction in nocturnal dipping when discrimination increases compared to other subgroups and controlling for other variables. Figure 2a, b provides a graphical demonstration of reduced SBP dipping across ethnicity, Lys198Asn carrier status, and levels of everyday discrimination (i.e., below and on/above the median).

a, b Continuous nocturnal dipping as a function of ethnicity, Lys198Asn T-allele carrier status by participant’s reported everyday discrimination. EA European Americans, AA African Americans, LowEDS (a left) everyday discrimination below median, HighEDS (b right) everyday discrimination on/above median. Lower scores indicate less dipping. Bars represent the subgroup mean ± SEM
Discussion
The current study investigated the hypothesis that the interaction of everyday discrimination exposure levels and Lys198Asn carrier status would significantly differentiate ambulatory BP levels and dipping status between African American and European American participants. The hypothesis was partially supported. As shown in Table 2 and described in the “Results” section, a significant interaction between ET-1 carrier status, everyday discrimination scores, and ethnicity emerged for nighttime DBP and dipping SBP and DBP even after controlling for ethnicity, age, gender, discrimination, and ET-1 carrier status. The general pattern of results showed that, for African Americans, being a Lys198Asn T-allele carrier combined with higher everyday discrimination levels led to increases in nighttime DBP and reduced nocturnal SBP and DBP dipping.
For daytime SBP and DBP, the three-way interaction between carrier status, EDS, and ethnicity was not significant. For daytime SBP, age and gender emerged as significant main effects. As expected, males had higher BP than females regardless of ethnicity or carrier status and increases in age were associated with increased SBP. For daytime DBP, age was associated with increased DBP and BMI-Z were associated with lower DBP. The association between DBP and BMI-Z was not anticipated; however, Settler et al. [51] reported similar results from data observed in the 1999–2002 National Health and Examination Survey.
For nighttime SBP, the three-way interaction between carrier status, EDS, and ethnicity was not significant. The model including the first block was significant and significant main effects emerged for age, gender, and BMI-Z. Increases in age, being male, and increases in BMI-Z all significantly predicted increases in nighttime SBP. For nighttime DBP, the three-way interaction between carrier status, everyday discrimination scores, and ethnicity was significant.
Previous researchers have speculated that the everyday discrimination scale may not be as salient of a measure among European Americans as it is among African Americans. It is impossible to determine whether the saliency of the measure or the actual experiences of African Americans in terms of everyday discrimination exceed those of European Americans in a given sample. Cooper et al. found that everyday discrimination affected plasma ET-1 among African Americans, but not European Americans, and that socioeconomic status affected plasma ET-1 among European Americans, but not African Americans [20]. Irrespective of whether the everyday discrimination scale is more salient for African Americans and socioeconomic status is more salient for European Americans, significant interactions between ET-1/Lys198Asn carrier status and everyday discrimination scores emerged and may lend some support to the review of Harris and Matthews [29] which suggested that autonomic nervous system regulation could be linked with cardiovascular disease development through impairments in the endothelial system.
Although interesting, these findings are speculations. Our assumptions align with those of Harris and Matthews and we purport that the increased sympathetic nervous system activity combined with the ET-1 T-allele carrier status results in higher prevalence of autonomic nervous system imbalance and leads to decreased nocturnal BP. In this study, we did not examine socioeconomic status, sympathetic nervous system activity, or plasma ET-1/nitric oxide activity, but the differential results on nocturnal BP dipping among African American T-allele carriers with higher everyday discrimination scores and nocturnal BP when compared to European Americans lend some additional support that everyday discrimination makes a unique contribution on African American BP regulatory mechanisms.
Unfortunately, one weakness of this study is the protocol implemented in the original longitudinal study, which did not collect cation excretion rates (e.g., sodium) or markers of hypothalamus–pituitary–adrenal axis (e.g., cortisol) during this initial visit when everyday discrimination was obtained. The lack of these measures makes it impossible to ascertain whether the influence of everyday discrimination is on the sympathetic nervous system, endothelial system function, or alternative biological mechanisms that were affecting nocturnal BP. Future studies should include these and other biomarkers to help elucidate the specific mechanistic pathways that are affected.
A second weakness is the small amount of variance accounted for by these three-way interactions. Some researchers have suggested that the use of multiple nights of ambulatory BP measurement may increase the ability to detect psychosocial and environmental influences. When investigating a gene × environment interaction of this nature, one could argue that the environmental factor of interest may not be stable and so the use of multiple nights of monitoring for detection are only valuable if the repeated measurement occurs on nights the psychosocial and environmental factors are reported as heightened. The use of ambulatory diaries measuring affective status combined with multiple nights of BP monitoring may help determine the stability of these influences. However, the established protocol for this longitudinal study was to conduct a single 24-h recording and this study data was collected prior to the development of easy-to-use electronic BP diaries. Preliminary work indicated low acceptance by participants when handwritten BP diaries and multiple nights of BP monitoring were implemented so they were omitted. Now that electronic easy-to-use BP diaries are widely available, we encourage their use in future studies.
Despite its limitations, the results from this study help to demonstrate that, even though gene × environment models are in their infancy, there are some important utilities of their use. As mentioned in the “Introduction” section, during a previous randomized controlled trial among adolescent African Americans who were prehypertensive, we found that T-allele carriers of the ET-1/Lys198Asn single-nucleotide polymorphism who reported higher levels of everyday discrimination were much less responsive to behavioral interventions compared to other subgroup combinations (i.e., noncarriers and carriers reporting low discrimination, noncarriers reporting high discrimination) [39]. The collective findings from this and the previous studies warrant the need for additional research into the relationship between ET-1 and autonomic nervous system balance as well as the exploration of potential interventions to maintain homeostasis between these systems.
Finally, future studies should continue to focus on other potential gene × environment models and cardiovascular-related mechanisms. Additional systems and personalized interventions may help to further eradicate risk factors for EH which target specific subgroups of the population (e.g., genetic predisposition for sodium sensitivity and dietary approaches to stopping hypertension). The potential benefit of personalized medicine, allowing the implementation of low-cost maximally effective treatments with minimal side effects, could greatly enhance the current prescription-based system.
References
CDC National Center for Chronic Disease Prevention and Health Promotion. Heart disease and stroke prevention: Addressing the nation’s leadings killers. Atlanta: Center for Disease Control; 2011.
Kannel WB. Progression of uncontrolled hypertension and implications for managing its sequelae. Manag Care. 2003;12:26-33.
Staessen JA, Thijs L, Fagard R, et al. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. Systolic hypertension in Europe trial investigators. JAMA. 1999;282:539-546.
Mancia G, Zanchetti A, Agabiti-Rosei E, et al. Ambulatory blood pressure is superior to clinic blood pressure in predicting treatment-induced regression of left ventricular hypertrophy. Sample study group. Study on ambulatory monitoring of blood pressure and lisinopril evaluation. Circulation. 1997;95:1464-1470.
Fagard RH, Staessen JA, Thijs L. Relationships between changes in left ventricular mass and in clinic and ambulatory blood pressure in response to antihypertensive therapy. J Hypertens. 1997;15:1493-1502.
Perloff D, Sokolow M. Ambulatory blood pressure measurements, prognostic implications. Arch Mal Coeur Vaiss. 1991;84(3):21-27.
Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure. An independent predictor of prognosis in essential hypertension. Hypertension. 1994;24:793-801.
Fagard RH, Thijs L, Staessen JA, et al. Night–day blood pressure ratio and dipping pattern as predictors of death and cardiovascular events in hypertension. J Hum Hypertens. 2009;23:645-653.
Barnes VA, Treiber FA, Musante L, et al. Ethnicity and socioeconomic status: Impact on cardiovascular activity at rest and during stress in youth with a family history of hypertension. Ethn Dis. 2000;10:4-16.
Pletcher MJ, Bibbins-Domingo K, Lewis CE, et al. Prehypertension during young adulthood and coronary calcium later in life. Ann Intern Med. 2008;149:91-99.
Spruill TM, Gerin W, Ogedegbe G, et al. Socioeconomic and psychosocial factors mediate race differences in nocturnal blood pressure dipping. Am J Hypertens. 2009;22:637-642.
Hickson DA, Diez Roux AV, Wyatt SB, et al. Socioeconomic position is positively associated with blood pressure dipping among African-American adults: The Jackson Heart Study. Am J Hypertens. 2011;24:1015-1021.
Brondolo E, Libby DJ, Denton EG, et al. Racism and ambulatory blood pressure in a community sample. Psychosom Med. 2008;70:49-56.
Hill LK, Kobayashi I, Hughes JW. Perceived racism and ambulatory blood pressure in African American college students. J Black Psychol. 2007;33:404-421.
Smart Richman L, Pek J, Pascoe E, Bauer DJ. The effects of perceived discrimination on ambulatory blood pressure and affective responses to interpersonal stress modeled over 24 hours. Health Psychol: Off J Div Health Psychol Am Psychol Assoc. 2010;29:403-411.
Tomfohr L, Cooper DC, Mills PJ, Nelesen RA, Dimsdale JE. Everyday discrimination and nocturnal blood pressure dipping in Black and White Americans. Psychosom Med. 2010;72:266-272.
Brondolo E, Rieppi R, Kelly KP, Gerin W. Perceived racism and blood pressure: A review of the literature and conceptual and methodological critique. Ann Behav Med. 2003;25:55-65.
Broman CL. The health consequences of racial discrimination: A study of African Americans. Ethn Dis. 1996;6:148-153.
Buxbaum SG, Goel P, White W, Gregoski M, Dunn SH. Heritability of John Henryism, and correlation between John Henryism and hypertension in the Jackson Heart Study. International Genetics Epidemiology Society (IGES) 21st Annual Meeting (vol. under review), Portland, Oregon; 2012.
Cooper DC, Mills PJ, Bardwell WA, Ziegler MG, Dimsdale JE. The effects of ethnic discrimination and socioeconomic status on endothelin-1 among Blacks and Whites. Am J Hypertens. 2009;22:698-704.
Treiber FA, Jackson RW, Davis H, et al. Racial differences in endothelin-1 at rest and in response to acute stress in adolescent males. Hypertension. 2000;35:722-725.
Treiber FA, Kapuku GK, Davis H, Pollock JS, Pollock DM. Plasma endothelin-1 release during acute stress: Role of ethnicity and sex. Psychosom Med. 2002;64:707-713.
Ergul S, Parish DC, Puett D, Ergul A. Racial differences in plasma endothelin-1 concentrations in individuals with essential hypertension. Hypertension. 1996;28:652-655.
Evans RR, Phillips BG, Singh G, Bauman JL, Gulati A. Racial and gender differences in endothelin-1. Am J Cardiol. 1996;78:486-488.
Harshfield GA, Alpert BS, Willey ES, et al. Race and gender influence ambulatory blood pressure patterns of adolescents. Hypertension. 1989;14:598-603.
Harshfield GA, Hwang C, Grim CE. Circadian variation of blood pressure in blacks: Influence of age, gender and activity. J Hum Hypertens. 1990;4:43-47.
James GD. Race and perceived stress independently affect the diurnal variation of blood pressure in women. Am J Hypertens. 1991;4:382-384.
Fumo MT, Teeger S, Lang RM, et al. Diurnal blood pressure variation and cardiac mass in American Blacks and Whites and South African Blacks. Am J Hypertens. 1992;5:111-116.
Harris KF, Matthews KA. Interactions between autonomic nervous system activity and endothelial function: A model for the development of cardiovascular disease. Psychosom Med. 2004;66:153-164.
Imumorin IG, Dong Y, Zhu H, et al. A gene–environment interaction model of stress-induced hypertension. Cardiovasc Toxicol. 2005;5:109-132.
Ge D, Dong Y, Wang X, Treiber FA, Snieder H. The Georgia cardiovascular twin study: Influence of genetic predisposition and chronic stress on risk for cardiovascular disease and type 2 diabetes. Twin Res Hum Genet: Off J Int Soc Twin Stud. 2006;9:965-970.
Snieder H, Harshfield GA, Barbeau P, et al. Dissecting the genetic architecture of the cardiovascular and renal stress response. Biol Psychol. 2002;61:73-95.
Light KC. Hypertension and the reactivity hypothesis: The next generation. Psychosom Med. 2001;63:744-746.
Popov AF, Schulz EG, Hinz J, et al. Impact of endothelin-1 Lys198Asn polymorphism on coronary artery disease and endorgan damage in hypertensives. Coron Artery Dis. 2008;19:429-434.
Tiret L, Poirier O, Hallet V, et al. The Lys198Asn polymorphism in the endothelin-1 gene is associated with blood pressure in overweight people. Hypertension. 1999;33:1169-1174.
Asai T, Ohkubo T, Katsuya T, et al. Endothelin-1 gene variant associates with blood pressure in obese Japanese subjects: The Ohasama Study. Hypertension. 2001;38:1321-1324.
Barath A, Endreffy E, Bereczki C, et al. Endothelin-1 gene and endothelial nitric oxide synthase gene polymorphisms in adolescents with juvenile and obesity-associated hypertension. Acta Physiol Hung. 2007;94:49-66.
Rabineau KM, Treiber FA, Poole J, Ludwig D. Interactive effects of anger expression and ET-1 Lys198Asn polymorphism on vasoconstriction reactivity to behavioral stress. Ann Behav Med. 2005;30:85-89.
Gregoski MJ, Barnes VA, Tingen MS, et al. Differential impact of stress reduction programs upon ambulatory blood pressure among African American adolescents: Influences of endothelin-1 gene and chronic stress exposure. Int J Hypertens. 2012;2012:510291.
Lewis TT, Yang FM, Jacobs EA, Fitchett G. Racial/ethnic differences in responses to the everyday discrimination scale: A differential item functioning analysis. Am J Epidemiol. 2012;175:391-401.
Dekkers C, Treiber FA, Kapuku G, Van Den Oord EJ, Snieder H. Growth of left ventricular mass in African American and European American youth. Hypertension. 2002;39:943-951.
O’Brien E, Atkins N, Staessen J. State of the market. A review of ambulatory blood pressure monitoring devices. Hypertension. 1995;26:835-842.
O’Brien E, Mee F, Atkins N, O’Malley K. Accuracy of the SpaceLabs 90207 determined by the British hypertension society protocol. J Hypertens. 1991;9:573-574.
Harshfield GA, Wilson ME, Treiber FA, Alpert BS. A comparison of ambulatory blood pressure patterns across populations. Blood Press Monit. 2002;7:265-269.
O’Brien E, Asmar R, Beilin L, et al. European society of hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003;21:821-848.
Wang X, Poole JC, Treiber FA, et al. Ethnic and gender differences in ambulatory blood pressure trajectories: Results from a 15-year longitudinal study in youth and young adults. Circulation. 2006;114:2780-2787.
Parati G, Staessen JA. Day–night blood pressure variations: Mechanisms, reproducibility and clinical relevance. J Hypertens. 2007;25:2377-2380.
Clark R, Coleman AP, Novak JD. Brief report: Initial psychometric properties of the everyday discrimination scale in Black adolescents. J Adolesc. 2004;27:363-368.
Williams DR, Yan Y, Jackson JS, Anderson NB. Racial differences in physical and mental health: Socio-economic status. Stress and discrimination. J Health Psychol. 1997;2:335-351.
Banks KH, Kohn-Wood LP, Spencer M. An examination of the African American experience of everyday discrimination and symptoms of psychological distress. Community Ment Health J. 2006;42:555-570.
Abstracts from the 46th Annual Conference on Cardiovascular Disease Epidemiology and Prevention. Circulation. 2006;113:e301–e381.
Acknowledgments
This publication was supported by grants from NIH/NHLBI (HL05662, HL069999) and the South Carolina Clinical and Translational Research Institute, with an academic home at the Medical University of South Carolina, NIH/NCRR, Grant #UL1RR029882. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH or NCRR. We acknowledge the following research assistants who assisted with data collection and other aspects of the study: Shawntel Parker and Greg Slavens assisted with data management and system analysis and Brenda Jackson, Sandra Young-Mayes, Tracy Miller, Pam Shields, and Bridgett Wells assisted with data collection.
Conflict of Interest
The authors have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Gregoski, M.J., Buxbaum, S.G., Kapuku, G. et al. Interactive Influences of Ethnicity, Endothelin-1 Gene, and Everyday Discrimination Upon Nocturnal Ambulatory Blood Pressure. ann. behav. med. 45, 377–386 (2013). https://doi.org/10.1007/s12160-013-9472-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-013-9472-z