
Abstract
Background
Anxiety, depression, insomnia, fatigue, and pain are frequently reported by cancer patients. These symptoms are highly interrelated. However, few prospective studies have documented the sequence with which symptoms occur during cancer care.
Purpose
This longitudinal study explored the temporal relationships between anxiety, depression, insomnia, fatigue, and pain over an 18-month period in a large population-based sample of nonmetastatic cancer patients (N = 828), using structural equation modeling.
Methods
The patients completed a battery of self-report scales at baseline and 2, 6, 10, 14, and 18 months later.
Results
The relationships between the same symptom at two consecutive assessments showed the highest coefficients (β = 0.29 to 0.78; all ps ≤ 0.05). Cross-loading parameters (β = 0.06 to 0.19; ps ≤ 0.05) revealed that fatigue frequently predicted subsequent depression, insomnia, and pain, whereas anxiety predicted insomnia.
Conclusions
Fatigue and anxiety appear to constitute important risk factors of other cancer-related symptoms and should be managed appropriately early during the cancer care trajectory.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer patients are likely to experience a variety of psychological and somatic symptoms, such as anxiety, depression, insomnia, fatigue, and pain, from the time of their diagnosis to months and sometimes years after the end of their treatment [1, 2]. These symptoms rarely occur alone and can influence each other during the cancer care trajectory. Indeed, many longitudinal studies have shown that the severity level of one symptom (e.g., depression) can predict that of the same symptom at a subsequent time assessment [3–11]. For example, results from a study conducted in 144 colorectal cancer patients showed that their baseline level of anxiety and depressive symptoms significantly predicted the increase of the same symptoms in the following year [7].
Other findings have revealed that temporal relationships also exist between different symptoms (e.g., anxiety symptoms at one time assessment predicting the level of fatigue found at a subsequent time assessment; [9, 11–19]). In a recent study, 82 men undergoing radiation therapy for prostate cancer completed questionnaires at several time points over a 6-month period [18]. Results showed that trait anxiety and depression symptoms, but not fatigue and pain, at baseline predicted sleep difficulties throughout the duration of the study. Conversely, previous reviews have underlined that fatigue and pain may be major risk factors for the development or increase of insomnia symptoms in cancer patients [20–23]. Further research is needed to resolve these inconsistent findings and address the limitations of prior research. For example, most of the studies were conducted using a small sample (i.e., mainly from 41 to 223 participants), which limits the statistical power and therefore the complexity of the analyses that can be computed. Some statistical procedures such as structural equation modeling are more appropriate to study temporal associations between symptoms [12], but these analyses generally require a large number of participants [24–26]. Furthermore, their study design often comprised two or three time points only, which limits the capacity of investigating the consistency of the pattern of temporal relationships over time. Indeed, stronger inferences about cause and effect relationships can be made from results obtained with several time assessments [27]. Getting a clearer picture of the temporal relationship between cancer-related symptoms appears to be very relevant from a clinical standpoint. By better understanding the sequence with which symptoms occur, interventions targeting symptoms that seem to appear first in the cancer care trajectory could be developed in order to prevent the incidence of other symptoms.
The main goal of this study was to explore temporal relationships between anxiety, depression, insomnia, fatigue, and pain, over an 18-month period in a large population-based sample of nonmetastatic cancer patients, using structural equation modeling. More precisely, this research aimed at examining to what extent the severity level of one specific symptom can uniquely and significantly predict the severity level of the same symptom and each of the other symptoms at the subsequent time point. It was postulated that the severity level of one specific symptom would significantly predict scores of the same symptom at the subsequent time point, consistently throughout the cancer care trajectory. No specific hypothesis was stated on associations between different symptoms because of the inconsistent results obtained thus far.
Method
Participants
Inclusion criteria were: (a) confirmed first diagnosis of nonmetastatic cancer, (b) scheduled to receive curative surgery, (c) between 18 and 80 years of age, and (d) able to read and understand French. Exclusion criteria were: (a) administration of neoadjuvant cancer treatment; (b) upcoming surgery as part of brachytherapy for prostate cancer, because of its very distinct side effects profile; (c) severe cognitive impairments (e.g., Alzheimer's disease) or severe psychiatric disorder (e.g., psychosis) as noted in the medical chart, observed at recruitment, or reported by the patients; d) having been diagnosed by a physician or being treated for a sleep disorder other than insomnia (e.g., sleep apnea) as reported by the patient; and (e) severe visual, hearing, or language defects impairing the capacity to complete the measures. Surgery that is done with a curative intent, in nonmetastatic cancer patients, is usually scheduled early in the cancer care trajectory. We chose to recruit patients scheduled to receive surgery in order to be able to follow them from the beginning of their treatment path.
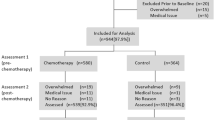
This study was part of a larger longitudinal study on the epidemiology of insomnia in the context of cancer [28, 29]. Potential participants were recruited at L’Hôtel-Dieu de Québec (Centre Hospitalier Universitaire de Québec; CHUQ) and Hôpital du St-Sacrement (Centre Hospitalier Affilié Universitaire de Québec; CHA), in Quebec City, Canada, from 2005 to 2007. The study was approved by the research ethics committees of the CHUQ, the CHA, and of the Université Laval. All patients meeting the initial inclusion criteria were approached by a research assistant on the day of their preoperative visit to explain the study goals and further assess their eligibility. Of the 3,196 patients solicited to take part in the larger study, 1,677 (52.5 %) were eligible and 962 agreed to participate (57.4 %). Differences between these patients and the ones who refused to participate are described elsewhere [28]. From the original sample of 962 participants, 86.1 % completed at least 50 % of this study's variables for at least 50 % of the assessment points (N = 828), which formed the sample for the current study. This decision was supported by evidence that patients who were excluded on this basis (N = 134) had a much larger amount of missing data (77.3 %) on the symptom variables, compared to 6.4 % only for participants included in the final sample. Patients who were excluded due to this criterion were more likely to be widowed, χ 2(1, N = 134) = 18.16, p < 0.0001; to receive chemotherapy, χ 2(1, N = 134) = 39.4, p < 0.0001; to have a gynecological, χ 2(1, N = 134) = 3.90, p = 0.05 or a urinary and gastrointestinal cancer, χ 2(1, N = 134) = 7.43, p = 0.006; and less likely to be married, χ 2(1, N = 134) = 5.78, p = 0.02 and to receive a combination of chemotherapy, radiation, and hormone therapy as adjuvant treatments, χ 2(1, N = 134) = 5.27, p = 0.02. However, they were not significantly different at baseline on any of the main dependent (symptoms) variables.
Procedure
The study used a prospective longitudinal design comprising six time assessments: baseline (T1), 2 (T2), 6 (T3), 10 (T4), 14 (T5), and 18 months (T6). At T1, participants were given a battery of self-report scales which they had to complete and mail back within the following week. Then, a phone interview was conducted to obtain missing data and review the most challenging items to fill out in order to increase the reliability of the data. Although patients were recruited before surgery, the majority (79.7 %) chose to complete the baseline measures after being operated. The same procedure was used from T2 to T6, except that the questionnaires were mailed. Participants received a compensation of 20$ CAD for each time assessment completed.
Measures
Hospital Anxiety and Depression Scale [30]
This questionnaire includes 14 items divided into two subscales: depression and anxiety (seven items each). The Hospital Anxiety and Depression Scale (HADS) contains no somatic items which could be confounded with symptoms of the medical condition. The 4-point Likert scale ranges from “0” to “3.” The total for each subscale ranges from 0 to 21 [31, 32]. The French–Canadian version has psychometric qualities equivalent to those of the original English version [32].
Insomnia Severity Index [33]
The Insomnia Severity Index (ISI) includes seven items which evaluate the perceived severity of: (a) difficulties falling asleep, (b) difficulties maintaining sleep, (c) early morning awakenings, (d) the degree of dissatisfaction with current sleep, (e) the degree to which sleep difficulties interfere with daytime functioning, (f) the degree to which others notice the deterioration of functioning related to the sleep problem, and (g) the level of distress or worry caused by the sleep difficulties. The 5-point Likert scale ranges from “0” (not at all) to “4” (extremely), for a total score ranging from 0 to 28 [34]. The French–Canadian version of the ISI was empirically validated among cancer patients [35, 36], with psychometric properties similar to those found in the general population [33].
Multidimensional Fatigue Inventory [37]
The French–Canadian version used is a short form of the original Multidimensional Fatigue Inventory (MFI) [38]. It contains 15 items divided into four subscales, but only the general and physical fatigue subscale was used for this study (seven items), in order to avoid the potential overlap between other dimensions of fatigue and depression (e.g., loss of motivation). The items are evaluated on a Likert scale ranging from “0” (not at all) to “4” (extremely). The French–Canadian version of the MFI has excellent psychometric qualities [37].
Physical Symptoms Questionnaire
An adaptation of the Memorial Symptom Assessment Scale [39] was developed to assess the frequency of 19 somatic symptoms often reported by cancer patients. Each item is scored on a Likert scale, ranging from “0” (never) to “4” (often). Only the pain item was used in the current study.
Demographic and Cancer Characteristics
Participant's age, education level, marital, employment, and socioeconomic status were collected using a questionnaire. Cancer-related data (e.g., cancer site and stage, and adjuvant treatments received) were taken from the patient's medical record.
Statistical Analyses
Raw data were entered twice by independent assistants and were cross-validated to ensure maximal integrity. They were examined for distribution and missing data using standard procedures [25]. As already explained, participants who had significant missing data (N = 134) were excluded from the sample. A direct maximum-likelihood imputation was then performed, using the expectation maximization algorithm [40], which yielded a sample of 828 participants with complete data (all five symptoms for all six assessments). Since structural equation modeling techniques assume multivariate normality [41], multivariate outliers (N = 38) were first identified with the Mahalanobis' distance computed on the five symptoms at the six time assessments (df = 30, alpha = 0.001) and then dropped, leaving a sample of 790 participants for the structural equation model. These statistical procedures were completed using SAS 9.1.3 [42] and a standard alpha level of 5 %.
Structural equation modeling (EQS software, version 6.1; [43]) was used in order to explore the directional temporal relationships between anxiety, depression, insomnia, fatigue, and pain. More specifically, a path analysis based on these observed variables (symptoms) examined to what extent the severity level of one specific symptom uniquely and significantly predicted the severity level of the same symptom and other symptoms at the subsequent time point. This statistical analysis was chosen over multivariate regressions because: (a) it makes it possible to test multiple temporal relationships simultaneously; (b) it provides model fit indices on the model adequacy; and (c) it enables comparisons between different models [24, 27, 41].
Except for temporal relationships between the same symptom at two different time points, no consistent pattern emerged from previous studies regarding temporal relationships between different symptoms. Thus, a saturated model was favored as a starting point to explore these relationships between the five symptoms across the six time points, as recommended by Byrne [24]. More precisely, all possible temporal relationships (parameters) between two consecutive time points (temporal intervals) were tested, in addition to the correlations between the five independent variables (symptoms at T1) and between all error terms associated with the dependent variables (symptoms from T2 to T6), respectively. With the aim of keeping the model as parsimonious as possible, parameters between nonconsecutive time points (e.g., between T2 and T4) or predicting symptoms in an opposite direction (e.g., T4 predicting T3) were not investigated. Then, following an iterative procedure based on the Lagrange and Wald tests, parameters were dropped or added until the most parsimonious model with the most adequate fit indices (i.e., χ 2/df ratio, Consistent Akaike Information Criteria (CAIC), Root Mean–Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Bentler–Bonett Non-Normed Fit Index (NNFI)) was obtained.
Afterwards, a second model was tested, in order to verify to what extent the more stable relationships observed could be generalized to all time points. More precisely, parameters that were found to be significant for the majority of the temporal intervals (more than or equal to three out of five intervals) were then generalized to the complete model (all five temporal intervals). The fit indices of this second model were compared to the first model, and a chi-square test on the fit difference was computed to determine whether these models differed significantly.
Results
Demographic and Medical Characteristics
Table 1 presents the main characteristics of the study sample at baseline (N = 828). The French–Canadian participants were 56.9 years old on average, and most of them were women (68.8 %). The most frequent cancer sites were breast (49.4 %) and prostate (28.3 %), and most commonly, patients had localized disease (i.e., stage I or II, 73.7 %). Surgery only (40.8 %) and the combination of chemotherapy, radiation, and hormone therapies (18.0 %) were the most common treatment regimens received.
Temporal Relationships from T1 to T6 (Model 1)
Mean scores obtained for each symptom are reported elsewhere [44]. Model 1 is shown in Fig. 1. The correlations obtained between each independent variable (symptoms at T1) were all significant (ps ≤ 0.01; r = 0.11 to 0.61), as were the correlations observed between the error terms of each dependent variable (symptoms from T2 to T6; ps ≤ 0.05; r = 0.07 to 0.56), except one (E4 with E28). Nearly half of the parameters (62 out of 125) were significant (ps ≤ 0.05) and remained in the model after completing the iterative selection procedures. Among these significant associations, all parameters representing the temporal relationship for a given symptom between two consecutive time points were significant (β from 0.29 to 0.78). Several cross-loading parameters (i.e., a symptom predicting another symptom) were significant, but they exhibited smaller coefficients (β from 0.06 to 0.19). Between 13 and 61 % of the variance of each symptom was explained by this final model.

Significant parameters obtained from T1 to T6 in the final model (model 1). Note. In order to keep the figure readable, only the correlations obtained between independent variables (symptoms at T1) and the parameters found to be significant between each time assessment are represented
Mean coefficients for the complete model were computed and are presented in Table 2. No significant parameter was found for the relationship “depression → fatigue” and for “depression → pain,” across the six time points, as is also shown in Fig. 1. The total number of significant parameters reported in Table 2 suggests that fatigue was the most contributive predictor over the course of the study (as is also exhibited in Fig. 1). More precisely, this variable had a significant relationship with subsequent symptoms 72 % of the time (18 significant parameters out of 25). Specifically, fatigue significantly predicted depression (i.e., T1 to T2, T2 to T3, T4 to T5, T5 to T6), insomnia (i.e., T1 to T2, T3 to T4, T5 to T6), and pain (i.e., T1 to T2, T3 to T4, T4 to T5, T5 to T6) at least for three temporal intervals out of five. Anxiety was another important predictor (15 out of 25 parameters), especially of insomnia scores at the subsequent time point (i.e., T1 to T2, T2 to T3, T4 to T5, T5 to T6). The variable that was most consistently predicted by other symptoms at the previous time point was insomnia (14 out of 25), although depression and pain were also significantly predicted by other symptoms assessed priorly in 13 out of 25 possible relationships.
Generalization of the Stable Temporal Relationships (Model 2)
Since the results revealed a number of relationships that were fairly stable over time, namely fatigue predicting depression, insomnia and pain, and anxiety predicting insomnia, another model (model 2) was tested to examine to what extent these relationships could be generalized to all temporal intervals. Specifically, in model 2, these parameters were entered for each temporal interval (i.e., T1 to T2, T2 to T3, T3 to T4, T4 to T5, and T5 to T6), in addition to the parameters already found to be significant between some symptoms at two consecutive time points. The comparison of global fit indices for model 2 (the generalized model) and for model 1 (the final model) is presented in Table 3 and reveals better indices for model 1. More precisely, lower χ 2/df ratio, CAIC, and RMSEA values, and higher CFI and NNFI indices were found with model 1. Finally, the chi-square test computed between models 1 and 2 was statistically significant, χ 2(16, N = 790) = 253.68, p = 0.01. Thus, the generalization of the more stable parameters to the whole model significantly decreased the data fit, which suggests that these temporal relationships were not present for all time points in this study. Model 1 was therefore retained.
Discussion
The goal of this study was to examine temporal relationships between anxiety, depression, insomnia, fatigue, and pain, over an 18-month period in a large sample of cancer patients, using structural equation modeling. More precisely, this research aimed at evaluating to what extent the severity level of a specific symptom can uniquely and significantly predict the severity level of the same symptom and other symptoms at the subsequent time point. As hypothesized, and consistent with previous studies, the severity level of a specific symptom significantly predicted that of the same symptom at the subsequent time point, for all symptoms and for all temporal intervals. Moreover, these relationships yielded the strongest coefficients.
Despite their lower magnitude, several cross-loading parameters were found to be significant. The findings revealed that fatigue was the most important predictor of other symptoms at the subsequent time point. One of the more constant relationships of fatigue over time was with future levels of insomnia, which might appear counterintuitive at first sight. Fatigue is the most common complaint of patients with sleep disturbances; hence, it is more frequently perceived as a consequence rather than a risk factor of insomnia [e.g., 21, 45]. However, in order to cope with the fatigue related to treatment, cancer patients often adopt maladaptive sleep behaviors, such as day napping and spending more time awake in their bed, which may disrupt circadian rhythms in the long run and increase the risk of insomnia [19, 21, 22, 29]. Besides insomnia, fatigue also frequently predicted pain and depression. The influence of fatigue on future levels of pain may take place through a deconditioning process [46–48]. By reducing their level of activity, a strategy commonly used by cancer patients to preserve their energy, they become vulnerable to a muscle deconditioning that can lead to increased pain when more vigorous activities are resumed. Carrying out fewer daily activities may also precipitate depressed mood. Indeed, the reduction of positive reinforcements normally resulting from personal and social activities may significantly contribute to the development of depression [49]. Although behavioral mechanisms of relationships between fatigue and other symptoms are plausible, the possibility of biological mechanisms should not be overlooked. Indeed, fatigue can reflect the presence of increased neoplastic activity which may better explain the occurrence of other symptoms (e.g., pain).
It is noteworthy that the fatigue level reported at the 14-month assessment (T5), when less than 5 % of the patients were still receiving chemotherapy or radiation therapy, significantly predicted all other symptoms at the following time point. This finding suggests that the severity of fatigue at the end of adjuvant treatments remains a relevant treatment target to help relieve general psychological distress often reported during this transition to the “survivorship” phase [50, 51].
Anxiety appeared as another important predictor of other variables, especially of insomnia, a result that is consistent with numerous longitudinal studies conducted in cancer patients [e.g., 14, 18, 29]. Psychophysiological arousal and catastrophic thoughts (e.g., “I'll never be able to do everything I have to do at work tomorrow if I don't sleep well.”) are characteristics commonly found in anxious individuals that could contribute to triggering sleep difficulties [52, 53]. In addition, the level of anxiety at the 2-month assessment (T2) significantly predicted the level of all other symptoms at the 6-month evaluation (T3). Given that the highest proportion of patients receiving adjuvant treatments was at 2 months (T2; 52.9 %), these results suggest that interventions focusing on anxiety symptoms early in the cancer care trajectory might prevent the aggravation of other symptoms during the next few months.
The final model showed that levels of depression never significantly predicted fatigue levels at the subsequent time point. Hence, the relationship between depression and fatigue does not seem to be bidirectional, as is generally believed. The majority of previous studies that have found a significant association between these two symptoms looked at the relationship in only one direction [e.g., 16, 17, 54, 55]. One of the few studies that have investigated this relationship bidirectionally [56] showed that fatigue predicted depressive mood better than depressive mood predicted fatigue, as in the current results.
The absence of significant associations between depression and pain, in both directions (except pain at T3 → depression at T4), is also worth discussing. This somewhat surprising result is probably due to our study sample composed of patients with localized cancer, who are less likely to experience chronic pain [57–59]. It should also be underlined that our measure of pain, which encompasses both cancer- and noncancer-related pain, was perhaps not specific enough.
Lastly, the second model tested failed to show a constant pattern of temporal relationships in the current sample. In fact, the statistical analyses rejected the generalization of the four stable relationships found in model 1 (i.e., anxiety → insomnia; fatigue → depression; fatigue → insomnia; fatigue → pain) to all time points and favored model 1. These results suggest that changes occurring during the cancer care trajectory, such as cancer treatments received and the side effects they induced, alter the nature and strength of the relationships found between the symptoms.
Although one could argue that the current fit indices did not reach the recommended cutoffs usually found in the literature, the final model offers relatively good fit indices given the constraints initially set. It is indeed desirable to have: (a) a low value on the following indices: between 5.00 and 2.00 for the χ 2/df ratio, under 0.08 (more desirably under 0.05) for the RMSEA and between 0.00 and 0.08 for its confidence interval, and (b) a high value on the following indices: over 0.90 (more desirably over 0.95) for the CFI and the NNFI [24, 26, 41, 60, 61]. However, in order to keep the model as parsimonious as possible, some constraints were initially set (i.e., no parameter was tested between two nonconsecutive time points or in the opposite direction), which consequently limited the capacity to reproduce the observed variance/covariance matrix, and explained the lower, but still acceptable, fit indices of the final model.
Many strengths of this study should be emphasized. First, the large population-based sample size, composed of patients with diverse cancer characteristics, contributed to maximizing the generalization of the findings and offered enough statistical power to compute more complex statistical analyses, while the use of specific, reliable, and valid questionnaires enhanced the study's internal validity. Second, numerous prospective, repeated measurements at specific time points over an 18-month period allowed us to examine the stability of temporal relationships throughout the cancer care trajectory. Nonetheless, this study has some limitations that should be underlined. First, the analyses were exploratory, since no clear pattern of findings or theoretical model was available in the literature. Replication of these results is therefore strongly warranted. Second, time points were separated by a relatively long period of time, which was 4 months in most of the cases. It is possible that other temporal relationships would have been observed with shorter intervals that were not captured in this study. Third, the temporal relationships obtained between cancer-related symptoms do not imply causality. Other psychological and biological factors, which were not measured in this study, might better explain the occurrence of these symptoms. Fourth, the potential influence of patients' sociodemographic characteristics and clinical variables (e.g., cancer site, adjuvant treatments) on the evolution of cancer-related symptoms were not controlled for in the analysis.
Besides the necessity of replicating the current results, including in studies with shorter time intervals, future studies should investigate other symptoms that may be interrelated with those assessed in this study. For instance, hot flashes may mediate the relationship between anxiety and insomnia, as these symptoms have been shown to be positively associated with both anxiety [e.g., 62] and sleep difficulties [e.g., 63]. Cognitive disturbances, which may be a consequence of sleep impairments [64], could also lead to depressive symptoms. More studies are also warranted on the possible role of other side effects of treatments, such as urinary incontinence or sexual dysfunctions [65–68] and on potential biological mechanisms.
This exploratory study also points to suggestions for interventions. The level of a specific symptom was the strongest predictor of the same symptom afterwards, but could also significantly predict the subsequent level of other symptoms. For instance, it would appear that providing patients with cognitive and behavioral strategies targeting dysfunctional thoughts and maladaptive behaviors associated with anxiety could be offered in order to decrease anxiety levels, but also to prevent the development of insomnia symptoms. Fatigue was a significant predictor of many other symptoms throughout the cancer care trajectory, especially after completion of adjuvant treatments. It seems therefore relevant to specifically treat fatigue per se, but also to prevent the development or the aggravation of other symptoms over time. For example, cognitive–behavioral strategies, such as behavioral activation and physical activity, as well as cognitive restructuring and pacing, have been found to be efficacious for reducing fatigue symptoms in cancer patients [45, 69–71] and could be used as preventive interventions.
References
Esther Kim JE, Dodd MJ, Aouizerat BE, Jahan T, Miaskowski C. A review of the prevalence and impact of multiple symptoms in oncology patients. J Pain Symptom Manage. 2009 Apr; 37(4).
National Institutes of Health. NIH State-of-the-Science Statement on symptom management in cancer: Pain, depression, and fatigue. NIH Consens State Sci Statements. 2002 Jul; 19(4): 1-29.
Ahlberg K, Ekman T, Gaston-Johansson F. The experience of fatigue, other symptoms and global quality of life during radiotherapy for uterine cancer. Int J Nurs Stud. 2005 May; 42(4): 377-386.
Couper JW, Love AW, Duchesne GM, et al. Predictors of psychosocial distress 12 months after diagnosis with early and advanced prostate cancer. Med J Aust. 2010 Sep 6; 193(5 Suppl): S58-S61.
Dahl AA, Nesvold IL, Reinertsen KV, Fossa SD. Arm/shoulder problems and insomnia symptoms in breast cancer survivors: Cross-sectional, controlled and longitudinal observations. Sleep Medicine. 2011 Jun; 12(6): 584-590.
Hill J, Holcombe C, Clark L, et al. Predictors of onset of depression and anxiety in the year after diagnosis of breast cancer. Psychol Med. 2011 Jul; 41(7): 1429-1436.
Hyphantis T, Paika V, Almyroudi A, Kampletsas EO, Pavlidis N. Personality variables as predictors of early non-metastatic colorectal cancer patients' psychological distress and health-related quality of life: A one-year prospective study. J Psychosom Res. 2010 May; 70(5): 411-421.
Miaskowski C, Paul SM, Cooper BA, et al. Trajectories of fatigue in men with prostate cancer before, during, and after radiation therapy. J Pain Symptom Manage. 2008 Jun; 35(6): 632-643.
Servaes P, Gielissen MF, Verhagen S, Bleijenberg G. The course of severe fatigue in disease-free breast cancer patients: A longitudinal study. Psychooncology. 2007 Sep; 16(9): 787-795.
Sharma A, Sharp DM, Walker LG, Monson JR. Predictors of early postoperative quality of life after elective resection for colorectal cancer. Ann Surg Oncol. 2007 Dec; 14(12): 3435-3442.
Stone P, Richards M, A'Hern R, Hardy J. Fatigue in patients with cancers of the breast or prostate undergoing radical radiotherapy. J Pain Symptom Manage. 2001 Dec; 22(6): 1007-1015.
Brown LF, Kroenke K. Cancer-related fatigue and its associations with depression and anxiety: A systematic review. Psychosomatics. 2009 Sep-Oct; 50: 440-447.
Chen SC, Liao CT, Chang JT. Orofacial pain and predictors in oral squamous cell carcinoma patients receiving treatment. Oral Oncol. 2011 Feb; 47(2): 131-135.
Colagiuri B, Christensen S, Jensen AB, et al. Prevalence and predictors of sleep difficulty in a national cohort of women with primary breast cancer three to four months postsurgery. J Pain Symptom Manage. 2011 Nov; 42(5): 710-720.
Den Oudsten BL, Van Heck GL, Van der Steeg AF, Roukema JA, De Vries J. Predictors of depressive symptoms 12 months after surgical treatment of early-stage breast cancer. Psychooncology. 2009 Nov; 18(11): 1230-1237.
De Vries J, Van der Steeg AF, Roukema JA. Determinants of fatigue 6 and 12 months after surgery in women with early-stage breast cancer: A comparison with women with benign breast problems. J Psychosom Res. 2009 Jun; 66(6): 495-502.
Geinitz H, Zimmermann FB, Thamm R, et al. Fatigue in patients with adjuvant radiation therapy for breast cancer: Long-term follow-up. J Cancer Res Clin Oncol. 2004 Jun; 130(6): 327-333.
Miaskowski C, Paul SM, Cooper BA, et al. Predictors of the trajectories of self-reported sleep disturbance in men with prostate cancer during and following radiation therapy. Sleep. 2011 Feb; 34(2): 171-179.
Liu L, Rissling M, Natarajan L, et al. The longitudinal relationship between fatigue and sleep in breast cancer patients undergoing chemotherapy. Sleep. 2012; 35(2): 237-245.
Roscoe JA, Kaufman ME, Matteson-Rusby SE, et al. Cancer-related fatigue and sleep disorders. Oncologist. 2007; 12(Suppl 1): 35-42.
Savard J, Morin CM. Insomnia in the context of cancer: A review of a neglected problem. J Clin Oncol. 2001 Feb 1; 19(3): 895-908.
Theobald DE. Cancer pain, fatigue, distress, and insomnia in cancer patients. Clin Cornerstone. 2004; 6(Suppl 1D): S15-S21.
Vena C, Parker K, Cunningham M, Clark J, McMillan S. Sleep-wake disturbances in people with cancer part I: An overview of sleep, sleep regulation, and effects of disease and treatment. Oncol Nurs Forum. 2004 Jul; 31(4): 735-746.
Byrne BM. Structural Equation Modeling with EQS: Basic Concepts, Applications, and Programming. 2nd ed. New York: Routledge; 2008.
Tabachnik B, Fidell L. Using Multivariate Statistics. 5th ed. Boston, MA: Allyn & Bacon; 2006.
Thompson B. Ten commandments of structural equation modeling. In: Grimm LG, Yarnold PR, eds. Reading and Understanding More Multivariate Statistics. 1st ed. Washington DC: American Psychological Association; 2000: 261-284.
Klem L. Structural equation modeling. In: Grimm LG, Yarnold PR, eds. Reading and Understanding More Multivariate Statistics. 1st ed. Washington DC: American Psychological Association; 2000: 227-260.
Savard J, Ivers H, Villa J, Caplette-Gingras A, Morin CM. Natural course of insomnia comorbid with cancer: An 18-month longitudinal study. J Clin Oncol. 2011 Sep 10; 29(26): 3580-3586.
Savard J, Villa J, Ivers H, Simard S, Morin CM. Prevalence, natural course, and risk factors of insomnia comorbid with cancer over a 2-month period. J Clin Oncol. 2009 Nov 1; 27(31): 5233-5239.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983 Jun; 67(6): 361-370.
Roth AJ, Kornblith AB, Batel-Copel L, et al. Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer. 1998 May 15; 82(10): 1904-1908.
Savard J, Laberge B, Gauthier JG, Ivers H, Bergeron MG. Evaluating anxiety and depression in HIV-infected patients. J Pers Assess. 1998 Dec; 71(3): 349-367.
Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine. 2001 Jul; 2(4): 297-307.
Blais FC, Gendron L, Mimeault V, Morin CM. Évaluation de l'insomnie: Validation de trois questionnaires. L'Encéphale. 1997 Nov-Dec; 23((6): 447-453.
Savard MH, Savard J, Simard S, Ivers H. Empirical validation of the Insomnia Severity Index in cancer patients. Psychooncology. 2005 Jun; 14(6): 429-441.
Smith S, Trinder J. Detecting insomnia: Comparison of four self-report measures of sleep in a young adult population. J Sleep Res. 2001 Sep; 10(3): 229-235.
Fillion L, Gélinas C, Simard S, Savard J, Gagnon P. Validation evidence for the French Canadian adaptation of the Multidimensional Fatigue Inventory as a measure of cancer-related fatigue. Cancer Nurs. 2003 Apr; 26(2): 143-154.
Smets EM, Garssen B, Bonke B, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995 Apr; 39(3): 315-325.
Portenoy RK, Thaler HT, Kornblith AB, et al. The Memorial Symptom Assessment Scale: An instrument for the evaluation of symptom prevalence, characteristics and distress. Eur J Cancer. 1994; 30A(9): 1326-1336.
Roth PL. Missing data: A conceptual review for applied psychologists. Personnel Psychology. 1994; 47(3): 537-560.
Ullman JB. Structural equation modeling. In: Tabachnik B, Fidell L, eds. Using Multivariate Statistics. 5th ed. Boston, MA: Allyn & Bacon; 2006: 676-780.
Institute SAS. SAS/STAT 9.1 User's Guide. Cary, NC: SAS Institute; 2004.
Bentler PM, Wu EJC. EQS for Windows User's Guide. Encino, CA: Multivariate Software; 1995.
Trudel-Fitzgerald C, Savard J, Ivers H. Evolution of cancer-related symptoms over an 18-month period. J Pain Symptom Manage; 2012. In press.
Wagner LI, Cella D. Fatigue and cancer: Causes, prevalence and treatment approaches. Br J Cancer. 2004 Aug 31; 91(5): 822-828.
Fishbain DA, Cole B, Cutler RB, et al. Is pain fatiguing? A structured evidence-based review. Pain Medicine. 2003 Mar; 4(1): 51-62.
Gatzounis R, Schrooten MG, Crombez G, Vlaeyen JW. Operant learning theory in pain and chronic pain rehabilitation. Curr Pain Headache Rep. 2012 Apr; 16(2): 117-126.
Stone PC, Minton O. Cancer-related fatigue. Eur J Cancer. 2008 May; 44(8): 1097-1104.
Dimidjian S, Martell CR, Addis ME, Herman-Dunn R. Behavioral activation for depression. In: Barlow DH, ed. Clinical Handbook of Psychological Disorders: A Step-by-Step Treatment Manual. 4th ed. New York: Guilford Press; 2008: 328-364.
Allen JD, Savadatti S, Levy AG. The transition from breast cancer 'patient' to 'survivor'. Psychooncology. 2009 Jan; 18(1): 71-78.
Molassiotis A, Wengstrom Y, Kearney N. Symptom cluster patterns during the first year after diagnosis with cancer. J Pain Symptom Manage. 2010 May; 39(5): 847-858.
Espie CA. Insomnia: Conceptual issues in the development, persistence, and treatment of sleep disorder in adults. Annu Rev Psychol. 2002; 53: 215-243.
Harvey AG, Tang NK, Browning L. Cognitive approaches to insomnia. Clin Psychol Rev. 2005 Jul; 25(5): 593-611.
Bower JE, Ganz PA, Desmond KA, et al. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer. 2006 Feb 15; 106(4): 751-758.
de Graeff A, de Leeuw JR, Ros WJ, et al. Long-term quality of life of patients with head and neck cancer. Laryngoscope. 2000 Jan; 110(1): 98-106.
Visser MR, Smets EM. Fatigue, depression and quality of life in cancer patients: How are they related? Support Care Cancer. 1998 Mar; 6(2): 101-108.
Burton AW, Fanciullo GJ, Beasley RD, Fisch MJ. Chronic pain in the cancer survivor: A new frontier. Pain Medicine. 2007 Mar; 8(2): 189-198.
Edrington J, Miaskowski C, Dodd M, Wong C, Padilla G. A review of the literature on the pain experience of Chinese patients with cancer. Cancer Nurs. 2007; 30(5): 335-346.
Potter J, Higginson IJ. Pain experienced by lung cancer patients: A review of prevalence, causes and pathophysiology. Lung Cancer. 2004 Mar; 43(3): 247-257.
Hooper D, Coughlan J, Mullen MR. Structural equation modelling: Guidelines for determining model fit. EJBRM. 2008; 6(1): 53-60.
Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999; 6: 1-55.
Freeman EW, Sammel MD, Lin H, et al. The role of anxiety and hormonal changes in menopausal hot flashes. Menopause. 2005 May-Jun; 12(3): 258-266.
Savard MH, Savard J, Trudel-Fitzgerald C, Ivers H, Quesnel C. Changes in self-reported hot flashes and their association with concurrent changes in insomnia symptoms among women with breast cancer. Menopause. 2011 Sep; 18(9): 985-993.
Caplette-Gingras A, Savard J, Savard MH, Ivers H. Is insomnia associated with cognitive impairments in breast cancer patients? Behav Sleep Med; 2012. In press.
Carter J, Penson R, Barakat R, Wenzel L. Contemporary quality of life issues affecting gynecologic cancer survivors. Hematol Oncol Clin North Am. 2012 Feb; 26(1): 169-194.
Mirza M, Griebling TL, Kazer MW. Erectile dysfunction and urinary incontinence after prostate cancer treatment. Semin Oncol Nurs. 2011 Nov; 27(4): 278-289.
Denlinger CS, Barsevick AM. The challenges of colorectal cancer survivorship. J Natl Compr Canc Netw. 2009; 7(8): 883-893. Quiz 94.
Sadovsky R, Basson R, Krychman M, et al. Cancer and sexual problems. J Sex Med. 2010 Jan; 7(1 Pt 2): 349-373.
Kangas M, Bovbjerg DH, Montgomery GH. Cancer-related fatigue: A systematic and meta-analytic review of non-pharmacological therapies for cancer patients. Psychol Bull. 2008 Sep;134(5):700-741.
Mustian KM, Morrow GR, Carroll JK, et al. Integrative nonpharmacologic behavioral interventions for the management of cancer-related fatigue. Oncologist. 2007; 12(Suppl 1): 52-67.
Servaes P, Verhagen C, Bleijenberg G. Fatigue in cancer patients during and after treatment: Prevalence, correlates and interventions. Eur J Cancer. 2002 Jan; 38(1): 27-43.
Acknowledgments
We sincerely thank the patients for their participation and Fred Sengmueller for revising the manuscript. This research was supported by a training award held by the first author from the Canadian Institutes of Health Research, a grant from the Canadian Institutes of Health Research (MOP-69073), and a research scientist award from the Fonds de la Recherche en Santé du Québec to the second author.
Conflict of Interest
The authors report no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Trudel-Fitzgerald, C., Savard, J. & Ivers, H. Which Symptoms Come First? Exploration of Temporal Relationships Between Cancer-Related Symptoms over an 18-Month Period. ann. behav. med. 45, 329–337 (2013). https://doi.org/10.1007/s12160-012-9459-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-012-9459-1