
Abstract
Background
There has been limited research addressing changes in subjective well-being as a result of quitting smoking.
Purpose
The purpose of this study was to use longitudinal data to determine the relation between smoking cessation and subjective measures of well-being, including global quality of life (QOL), health-related QOL (HR-QOL), affect, relationship satisfaction, and stressor occurrence.
Methods
As part of a randomized, placebo-controlled smoking cessation trial, 1,504 participants (58.2% women, 83.9% white) completed assessments and had their smoking status biochemically confirmed at baseline and years 1 and 3 post-quit.
Results
Compared with continuing smokers, quitters showed improved global QOL, HR-QOL, and affect at years 1 and 3 and fewer stressors by year 3. Smoking status did not influence marital relationship satisfaction.
Conclusions
Successful quitters, in contrast to continuing smokers, reported improved subjective well-being, which could be used to motivate quit attempts by individuals with concerns about what life will be like without cigarettes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The dangers of smoking and the beneficial effects of smoking cessation on health are well established [1]. However, less is known about how quitting smoking affects quality of life (QOL). Smokers report various reasons for wanting to smoke, such as coping with stress and cravings, social facilitation, and improving mood [2, 3]. Furthermore, smokers report concerns about the effects of quitting smoking such as gaining weight, decreased ability to cope with stressors and negative affects, social ostracism, loss of pleasure, and intense cravings [4, 5]. Such findings raise questions about how quitting vs. continued smoking actually affects general mood, perceived health status, life satisfaction, and quality of life in the long term—once the effects of withdrawal have dissipated. Increases in subjective well-being may be as important or relevant to smokers as quitting to reduce disease risk [6]. More compelling evidence on this issue could be used to quell smokers’ fears and might actually be used to encourage more quit attempts.
QOL measures can be divided into instruments that focus on health-related outcomes and functionality (i.e., health-related QOL) and ones that also include dimensions in addition to health, e.g., social, recreational, affective/mental health, and life circumstances (i.e., global QOL). Some cross-sectional studies have focused on the differences in health-related quality of life (HR-QOL) amongst smokers, never smokers, and former smokers. Such studies have shown that active smoking is associated with lower levels of self-reported functioning in all health-related domains as compared with never smokers [7–10]. In fact, smoking has also been associated with decreased HR-QOL over and above other chronic or severe medical conditions [11]. Cross-sectional studies have also shown that HR-QOL ratings of ex-smokers more closely approximate never smokers than they do smokers, suggesting that quitting may improve HR-QOL [7, 9, 12]. However, only a few longitudinal studies have focused on the relation between cessation and changes in HR-QOL [13, 14]. For example, Sarna et al. [14] used data from women smokers who participated in the Nurses’ Health Study [15] and tracked changes in HR-QOL over 8 years. In that research, continuing smokers reported lower physical and mental health status compared with never smokers and smokers who quit at some point during the 8 years of the study. While this study is consistent with the cross-sectional data, the generalizability and robustness of the findings are limited as it is restricted to women and does not have very close temporal resolution since assessments were at 4-year intervals and were not timed to quitting. Furthermore, the few extant longitudinal studies are not treatment studies; rather, smokers quit throughout the study (e.g., [13, 15]). Thus, later differences between quitters and continuing smokers may strongly reflect differences that spurred quit attempts (e.g., illness concerns, dissatisfaction with smoking). In the current study, all participants were motivated to quit smoking and engaged in a quit attempt at the study’s inception. This produces some consistency in the timing of the quit attempt and initial motivational status of the participants.
In sum, while studies have shown that physical health is an important element of QOL, it does not, by itself, accurately capture overall QOL [16, 17], and even less is known about how smoking affects global QOL than HR-QOL. Cross-sectional studies show that smokers report significantly worse mental health functioning than either never smokers or former smokers [7, 8, 10]. In addition, retrospective data suggest that ex-smokers report being happier after quitting than they were while they were smoking [18]. These results support the hypothesis that quitting smoking may improve affect and life satisfaction. However, very few longitudinal studies have addressed changes in global QOL, and these have limitations such as poor temporal resolution, unusual populations of smokers, and quitting that may be highly driven by changes in disease status [13, 15]. Thus, there is considerable uncertainty as to how global QOL changes over the long term in successful quitters vs. those continuing smoking.
The strong beliefs smokers hold that quitting smoking will reduce quality of life (e.g., [5]) constitute a significant barrier to cessation for some smokers. Knowledge regarding improved long-term satisfaction with life, and QOL after quitting smoking, could offer clinicians important information for intervening with smokers who are worried about the effects of quitting and could be used to motivate and educate smokers on a broader scale (e.g., via media resources).
The goal of the current research was to assess prospectively changes in global QOL and HR-QOL, along with other subjective well-being dimensions (e.g., [16]), amongst smokers making a quit attempt as part of a clinical trial. This work was guided by the a priori expectations that successful smoking cessation would lead to both improved global QOL and improved HR-QOL. The current research examined the relations between successful vs. unsuccessful smoking cessation and a broad measure of life satisfaction (global QOL) that tapped individuals’ evaluations of their satisfaction with respect to not only their health but also to their self-regard, philosophy of life, standard of living, work, recreation, learning, creativity, social service, civic action, love relationship, friendships, relationships with children, relatives, home, neighborhood, and community (i.e., the Quality of Life Inventory, QOLI) [19]. This broad assessment of QOL was supplemented by additional assessments of positive and negative affect, the occurrence of stressors, and marital/partner relationship satisfaction since affect, stress, and supportive interpersonal relations are so core to subjective well-being. Understanding relatively short-term (i.e., 1 year) and long-term (i.e., 3 years) changes in QOL measures may help clinicians motivate smokers to make quit attempts and help researchers to understand better the relations of smoking with other life factors.
Methods
Participants
Participants were 1,504 smokers (58% female, 83% Caucasian) initially enrolled in a long-term smoking cessation trial conducted in Madison and Milwaukee, WI [20]. Adult smokers were recruited via media advertisements and earned media (e.g., newspaper articles) from January 2005 to June 2007. The inclusion criteria included smoking more than nine cigarettes per day on average for at least the past 6 months, having an alveolar carbon monoxide level >9, and being motivated to quit smoking (scoring 7 or higher on a 10-point scale). The exclusion criteria included using any form of tobacco other than cigarettes, currently taking bupropion, or having a current psychosis or schizophrenia diagnosis. In addition, participants were excluded if they had medical contraindications for any of the study medications, including high alcohol consumption (six drinks per day on 6 or 7 days of the week), a history of seizure, high blood pressure (>160/100), bipolar disorder, an eating disorder, a recent cardiac event, or allergies to any of the medications. All participants provided written informed consent, and the study was approved by the University of Wisconsin Health Sciences Institutional Review Board (see [20] for additional details).
Procedures
Interested smokers phoned a central research office where they completed a telephone screen to determine eligibility. Participants who passed the telephone screen were invited to an informational session where they provided written informed consent. Next, participants completed three in-person baseline sessions where they underwent further screening and completed demographic, smoking history, tobacco dependence, and quality of life questionnaires.
Participants were randomized in a double-blind manner to one of six treatment conditions: (1) bupropion SR; (2) nicotine lozenge; (3) nicotine patch; (4) nicotine patch + nicotine lozenge; (5) bupropion SR + nicotine lozenge; or (6) placebo. In addition to pharmacotherapy, all participants received six one-on-one counseling sessions based upon the Public Health Service Guideline [21]. Participants had study visits on their quit day and at 1, 2, 4, 8, and 52 weeks post-quit. At the 52-week study visits, vital signs, adverse events, and smoking status were all recorded and participants completed a similar battery of questionnaires to those administered at baseline, including quality of life assessments.
Measures
Demographics and Smoking
Baseline questionnaires assessed demographics, smoking history, and nicotine dependence. The demographics questionnaire tapped characteristics such as gender, race (smokers were asked which race they most strongly identified with), Hispanic ethnicity (i.e., reporting at least one parent of Hispanic origin), income, education level, and age. A smoking history questionnaire provided information about smoking behavior, smoking restrictions at home and work, self-efficacy to quit smoking, spouse smoking patterns, and motivation to quit smoking. Nicotine dependence questionnaires included the Fagerström Test of Nicotine Dependence [22], the Nicotine Dependence Syndrome Scale [23], the Tobacco Dependence Screener [24], and the Wisconsin Inventory of Smoking Dependence Motives [25].
Quality of Life Measures
All quality of life measures were administered at baseline, year 1, and year 3. Overall quality of life was measured using the QOLI [19], which comprises 17 QOLI subscales: health, self-regard, philosophy of life, standard of living, work, recreation, learning, creativity, social service, civic action, love relationship, friendships, relationships with children, relationships with relatives, home, neighborhood, and community (see Table 1 for content of these subscales). We did not use the civic action item because of seeming irrelevance to quitting smoking. We used the QOLI health item as the HR-QOL assessment which asked individuals to rate a single statement (“Health is being physically fit, not sick and without pain or disability”) on two dimensions: “How important is Health to your happiness?” and “How satisfied are you with your Health?” The QOLI has demonstrated good test–retest reliability and internal consistency ranging from 0.77 to 0.89 across three clinical and three non-clinical samples [19]. The QOLI is correlated with other measures of quality of life and life satisfaction (e.g., the Satisfaction with Life Scale) at levels ranging from 0.35 to 0.65 [19], is related to psychiatric symptoms at about r = 0.40–0.60 [19, 26], and shows predictive validity with regard to later adjustment (e.g., academic retention and future grades in college students) [27]. QOLI total scores correlate positively with other measures of well-being and correlate negatively with general psychopathology, anxiety, and depression. We also assessed positive and negative affect in the last 24 h using the Positive and Negative Affect Scale [28]. Life stressors were assessed using the Social Readjustment Rating Scale [29], a 34-item measure of stressful life events that typically entail adaptive or coping behavior. The stressful items endorsed were summed to create a total score indicative of the total number of stressors a person encountered in the prior year. Finally, participants who were married or living with a domestic partner were asked to complete the Kansas Marital Satisfaction Scale, a three-item scale that has been shown to be internally consistent and have adequate test–retest reliability and construct, concurrent, discriminative, and criterion validity [30–33]. We also asked whether the participant’s spouse/partner smoked and whether the spouse/partner supported the participant’s efforts to quit smoking on a five-point Likert scale from 1 = strongly agree to 5 = strongly disagree.
Smoking Status
Smoking status was assessed using 7-day point prevalence abstinence (“Have you smoked at all, even a puff, in the last seven days?”). All of participants’ self-reports of smoking status during study visits were confirmed by an expired carbon monoxide level of <10 ppm measured using a Micro-3 Smokerlyzer (Bedfont Scientific, USA, Williamsburg, VA). Quitters were defined as having carbon monoxide-confirmed 7-day point prevalence abstinence; all others were considered smokers. In-person smoking status assessments were conducted at baseline and years 1 and 3 post-quit.
Statistical Analyses
All analyses were conducted using SPSS 15.0 software (SPSS, Inc.). To address the issue of changes in QOL and its various components following a successful vs. unsuccessful quit attempt, we compared participants who were carbon monoxide-verified abstinent at years 1 and 3 post-quit from those who were not. To assess change, we created a difference score (Year 1 or 3 − Baseline) for each of the QOL subscales, which renders the directionality and magnitude of change patent. We then compared quitters and smokers using independent samples t tests and chi-square analyses as appropriate for the various QOL measures. It should be noted that we obtained a similar pattern of results when we analyzed the data using a repeated measures analysis of variance (ANOVA). A priori, we hypothesized that relative to continuing smokers, quitters would have better overall QOL, better HR-QOL, more positive affect, and less negative affect. Therefore, for these analyses, we used a p < 0.05 two-tailed cutoff to indicate a significant finding. However, we set a more conservative Bonferroni-corrected alpha of ≤0.003 (the Bonferroni p value cutoff for 16 comparisons) for the exploratory analyses of the other specific 15 QOLI subscales and the other QOL measures such as stressors and relationship satisfaction. We used t tests to assess group differences in gender and race (white vs. non-white) and ANOVA to examine interactions amongst smoking status and gender, race, education, age, and nicotine dependence for the overall QOL and the HR-QOL analyses.
Results
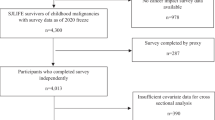
Of the 1,504 participants who enrolled in this study, 1,025 provided QOL data at the 1-year follow-up (63.3% smoking) and 999 provided QOL data at the 3-year follow-up (64.1% smoking; see Table 2 for demographic and smoking data). Participants in this study were similar in gender, race, and marital status to daily smokers who participated in a population-based survey of smoking in Wisconsin [34], although participants in the current study were somewhat more educated (70.8% with some college or technical school education vs. 44.0% in the population-based sample).
All participants showed decreased global QOL over the 1- and 3-year follow-up endpoints. However, compared with smokers, quitters at year 1 and year 3 had smaller decreases in overall QOL from baseline to year 1 and from baseline to year 3 (p = 0.045 and p = 0.02, respectively; see Table 3), indicating a relative maintenance of QOL with the passage of time. It should be noted that smokers and quitters did not differ in change in global QOL at year 1 if HR-QOL was removed from the total score; however, at year 3, quitters showed a significantly smaller decrease in global QOL even with the HR-QOL removed relative to continuing smokers (p = 0.04).
As hypothesized, at years 1 and 3, quitters reported higher levels of HR-QOL than they did at baseline, while smokers reported lower HR-QOL scores at years 1 and 3. Analyses showed significant differences between smokers and quitters in the degree of change in HR-QOL from baseline to years 1 and 3 (p = 0.005 and p = 0.002, respectively). There were no significant main effects of gender, race, age, education, or Fagerström Test of Nicotine Dependence total score, nor were there any significant interactions between smoking status and gender, race, age, education, or Fagerström Test of Nicotine Dependence total score for change in QOL-Total or HR-QOL at year 1 or at year 3.
Smokers and successful quitters also showed differences in degree of change for QOL subscales in addition to HR-QOL. For instance, relative to continuing smokers, at year 3, quitters showed smaller decreases in Self-Regard, Philosophy of Life, Standard of Living, Recreation, and Home (see Table 3). However, these comparisons were not significant when the Bonferroni-corrected p value of ≤0.003 was applied (only the difference in Philosophy of Life at Year 1 remained significant, p = 0.002).
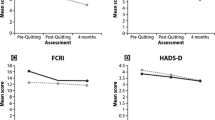
Significant differences between quitters and smokers were found in change in negative and positive affect from baseline to years 1 and 3 (see Table 4). Quitters at year 1, relative to smokers, reported a decrease in negative affect over the course of the follow-up year, while continuing smokers showed a slight increase. In addition, quitters showed stable positive affect over this time period, while continuing smokers showed declines. The effects for change in negative affect were similar at year 3, with quitters showing decreases and continuing smokers showing increases, but there was no significant difference in change in positive affect between smokers and quitters at year 3.
Chi-square analyses revealed no significant change from baseline to year 1 between smokers and quitters in overall stressors, as measured by the Social Readjustment Rating Scale total score (see Table 4). However, by year 3, there was a significant difference such that smokers reported an increase in stressor occurrence while quitters reported a decrease (see Table 4).
The final analyses addressed changes in relationship satisfaction amongst participants who were either married or living with a domestic partner. Of the 809 participants who reported being married or living with a domestic partner, 793 completed the KMSS at baseline, 542 completed it at year 1, and 509 completed it at year 3. There were no significant differences in marital satisfaction between smokers and year 1 quitters at baseline (see Table 4). We conducted an analysis of variance to determine whether partner smoking status moderated the relation between marital satisfaction and smoking status, but we did not find any significant effects for baseline spouse/partner smoking, smoking status at year 1, or the interaction between baseline spouse/partner smoking and smoking status at year 1. The results were similar at year 3. We did find that spouse support of quitting increased more in smokers than quitters at both years 1 and 3 (see Table 4).
Discussion
This research provides substantial evidence that quitting smoking benefits subjective well-being relative to continuing smoking. As other researchers have reported (e.g., [14]), health-related QOL improved following cessation, but decreased with continued smoking. The present study shows that this effect occurs relatively quickly as significant differences in the fates of quitters and continuing smokers are found within the first year after a quit attempt and are sustained for at least 3 years. The HR-QOL item asked individuals to rate a single statement about the importance of health to their happiness and how satisfied they were with their health. Therefore, the results showed that compared with continuing smokers, after 1 year, quitters were more satisfied with their health and saw a stronger health–happiness link. However, because smokers were not assigned randomly to quitting vs. continuing smoking groups, causal inferences are uncertain.
Because of the many physically harmful effects of smoking, it makes sense that quitting would enhance HR-QOL. The present study shows that cessation also benefits global or total QOL in addition to HR-QOL. While global QOL decreased significantly over the 3-year follow-up for both quitters and continuing smokers, consistent with previous research [14], the decrease was less for quitters at both years 1 and 3. This suggests that continued smoking may accelerate a decline in QOL and that quitting mitigates this effect.
The different trajectories in global QOL appear to be due to the cumulative effects of modest changes in multiple QOL dimensions (Table 3). Relative benefits of cessation occurred in many of the QOLI subscales, but the effects tended to be modest for each one, with effect sizes ranging from 0.25 downward. This is consistent with other findings showing that smoking cessation exerts reliable but modest effects on change in QOL [14]. It does appear that of the various QOL subscales, HR-QOL registered the biggest effects due to cessation vs. continued smoking. However, differences due to smoking status were found at year 3 in global QOL even when HR-QOL was removed from the total score, indicating that important changes, independent of health effects, are conferred by cessation.
The results also showed that over the 3-year study period, continuing smokers reported increased negative affect and decreased positive affect; conversely, successful quitters reported decreased negative affect and increased positive affect, although the year 3 positive affect findings did not reach statistical significance. Thus, while high levels of negative affect might constitute a barrier to quitting smoking (e.g., [35, 36]), these findings suggest that long-term cessation actually benefits affect, supporting the idea that smoking may serve to exacerbate psychological distress [37]. The notion that quitting ameliorates negative affect is consistent with both cross-sectional [8, 10] and longitudinal data [38, 39] showing that smokers have worse affect or mental health QOL than ex-smokers. Moreover, a recent retrospective survey showed that the great majority of ex-smokers reported that they are “happier” as ex-smokers than they were as smokers [18]. An improvement in affect due to cessation may be related to a reduction in repeated withdrawal experiences that smokers go through daily, in between cigarettes (e.g., [35, 40]), or perhaps due to a decrease in anxious arousal or restlessness that had been caused by the psychomotor stimulant effects of nicotine (cf. [37, 41]). Such an improvement is also consistent with previous research that suggests that smoking, itself, is a stressor and that quitting smoking removes this stressor [42–46]. However, it is important to note that increases in negative affect and decreases in positive affect may be causes of relapse rather than, or in addition to, consequences of continued smoking.
There was no difference between quitters and continuing smokers in the number of stressors reported at year 1, but by year 3 a significant difference was found, with continuing smokers reporting an increase and quitters a decrease. Again, causal inferences are uncertain. It may be that individuals with fewer stressors are able to maintain abstinence for years following a quit attempt or it may be that sustained, long-term abstinence causes a reduction of stressors. The latter could occur for several reasons. For instance, the expense, time requirements, and health effects of smoking may increase the likelihood of stressor occurrence. Recurrent illness and frequent smoking breaks might interfere with a person’s work or other performance, and the costs of smoking might increase vulnerability to economic challenges. In addition, the worsening negative affect of continuing smokers may make them more sensitive to, and aware of, stressors in their lives.
Quitting smoking was not related to overall marital satisfaction regardless of whether or not the participant’s spouse/partner was a smoker. This suggests that if a smoker quits but has a smoking spouse/partner, the cessation attempt does not damage the partner relationship. It was also interesting to note that participants reported an increase in spouse/partner support for quitting at years 1 and 3, and this increase was even larger for smokers. This difference may reflect, in part, that support for quitting is increasingly viewed as irrelevant when a spouse has achieved long-term abstinence.
These results should be interpreted in the context of the limitations of this research. First, participants were not randomly assigned to quit or continue smoking (quitters and non-quitters were self-selected), and therefore we are unable to make strong inferences about the directionality of causal effects. For instance, it is possible that some third variable promoted both quitting and later improvements in QOL, e.g., the belief that quitting smoking would benefit health did not arise from cessation per se but rather reflected other influences that motivated continued abstinence. Second, some of the reported effects depend upon only a small number of self-report items (e.g., HR-QOL), raising questions about the reliability of the reported effects and the extent to which the content domain was adequately sampled. Third, while the changes in total and HR-QOL were statistically significant, it is unclear what clinical benefit they might represent. However, it may be that the findings have clinical significance despite the modest effect sizes. Clearly, some smokers have concerns that their quality of life may deteriorate if they stop smoking [4, 5]. The results reported here suggest that smokers who quit successfully, long-term, experience no such deterioration due to quitting and, if anything, see reliable improvements. To that end, while QOL has intrinsic importance, it is not known what implications the reported QOL effects have for other important life outcomes and future adjustment.
In conclusion, this research suggests that in addition to improvements in objective, physiologic health indices such as HDL-cholesterol and endothelial function [47–50], over the 3 years after a quit attempt, successful quitters, in contrast to continuing smokers, reported better global quality of life, improved health-related quality of life, improved affect, and fewer stressors. These findings could be used to motivate quit attempts by individuals who are low in motivation to quit or who are daunted by concerns about what life will be like without cigarettes. Smokers might believe that quitting will decrease life satisfaction or quality of life—because they believe it disrupts routines, interferes with relationships, produces a loss of reinforcement (loss of smoking related pleasure), or because cessation deprives them of a coping strategy. The current findings suggest that over the long term, individuals will be happier and more satisfied with their lives if they quit smoking than if they do not.
References
U.S. Department of Health and Human Services. HHS announces National Smoking Cessation Quitline Network. 2004. www.dhhsgov/news/press/2004pres/20040203html.
Brandon TH, Baker TB. The Smoking Consequences Questionnaire: The subjective expected utility of smoking in college students. Psychol Assess. 1991, 3:484–491.
Copeland AL, Martin PD, Geiselman PJ, Rash CJ, Kendzor DE. Smoking cessation for weight-concerned women: Group vs. individually tailored, dietary, and weight-control follow-up sessions. Addict Behav. 2006, 31:115–127.
Sorensen G, Pechacek TF. Attitudes toward smoking cessation among men and women. J Behav Med. 1987, 10:129–37.
McKee SA, O’Malley SS, Salovey P, Krishnan-Sarin S, Mazure CM. Perceived risks and benefits of smoking cessation: Gender-specific predictors of motivation and treatment outcome. Addict Behav. 2005, 30:423–435.
Chapman S, Wong WL, Smith W. Self-exempting beliefs about smoking and health: Differences between smokers and ex-smokers. Am J Public Health. 1993, 83:215–219.
Mody RR, Smith MJ. Smoking status and health-related quality of life: As findings from the 2001 Behavioral Risk Factor Surveillance System data. Am J Health Promot. 2006, 20:251–258.
Strine TW, Okoro CA, Chapman DP, Balluz LS, Ford ES, Ajani UA, et al. Health-related quality of life and health risk behaviors among smokers. Am J Prev Med. 2005, 28:182- 187.
Tillmann M, Silcock J. A comparison of smokers’ and ex-smokers’ health-related quality of life. J Public Health Med. 1997, 19:268–273.
Wilson D, Parsons J, Wakefield M. The health-related quality-of-life of never smokers, ex-smokers, and light, moderate, and heavy smokers. Prev Med. 1999, 29:139–144.
Turner J, Page-Shafer K, Chin DP, Osmond D, Mossar M, Markstein L, et al. Adverse impact of cigarette smoking on dimensions of health-related quality of life in persons with HIV infection. Aids Patient Care STDS. 2001, 15:615–624.
Mulder I, Tijhuis M, Smit HA, Kromhout D. Smoking cessation and quality of life: The effect of amount of smoking and time since quitting. Prev Med. 2001, 33:653–660.
Mitra M, Chung MC, Wilber N, Klein Walker D. Smoking status and quality of life: A longitudinal study among adults with disabilities. Am J Prev Med. 2004, 27:258–260.
Sarna L, Bialous SA, Cooley ME, Jun HJ, Feskanich D. Impact of smoking and smoking cessation on health-related quality of life in women in the Nurses’ Health Study. Qual Life Res. 2008, 17:1217–1227.
Colditz GA. The nurses’ health study: A cohort of US women followed since 1976. J Am Med Women’s Assoc. 1995, 50:40–44.
Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: Three decades of progress. Psychol Bull. 1999, 125:276–302.
Krause JS, Sternberg M. Aging and adjustment after spinal cord injury: The roles of chronologic age, time since injury, and environmental change. Rehab Psychol. 1997, 42:287–302.
Shahab L, West R. Do ex-smokers report feeling happier following cessation? Evidence from a cross-sectional survey. Nicotine Tob Res. 2009 11:553–557.
Frisch MB, Cornell J, Villanueva M, Retzlaff PJ. Clinical validation of the Quality of Life Inventory: A measure of life satisfaction for use in treatment planning and outcome assessments. Psychol Assess. 1992, 4:92–101.
Piper ME, Smith SS, Schlam TR, Fiore MC, Jorenby DE, Fraser D, et al. A randomized placebo-controlled clinical trial of 5 smoking cessation pharmacotherapies. Arch Gen Psychiatry. 2009, 66:1253–1262.
Fiore MC, Jaen CR, Baker TB, Bailey WC, Benowitz N, Curry SJ, et al. Treating tobacco use and dependence: 2008 update. Rockville, MD: U.S. Department of Health and Human Services, U.S. Public Health Service; 2008.
Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991, 86:1119–1127.
Shiffman S, Waters A, Hickcox M. The Nicotine Dependence Syndrome scale: A multidimensional measure of nicotine dependence. Nicotine Tob Res. 2004, 6:327–348.
Kawakami N, Takatsuka N, Inaba S, Shimizu H. Development of a screening questionnaire for tobacco/nicotine dependence according to ICD-10, DSM-III-R, and DSM-IV. Addict Behav. 1999, 24:155–166.
Piper ME, Piasecki TM, Federman EB, Bolt DM, Smith SS, Fiore MC, et al. A multiple motives approach to tobacco dependence: The Wisconsin Inventory of Smoking Dependence Motives (WISDM-68). J Consult Clin Psychol. 2004, 72:139–154.
Crits-Christoph P, Gibbons MBC, Ring-Kurtz S, Gallop R, Stirman S, Present J, et al. Changes in positive quality of life over the course of psychotherapy. Psychotherapy. 2008, 45:419–430.
Frisch MB, Clark MP, Rouse SV, Rudd MD, Paweleck JK, Greenstone A, et al. Predictive and treatment validity of life satisfaction and the quality of life inventory. Assessment. 2005, 12:66–78.
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Pers Soc Psychol. 1988, 54:1063- 1070.
Holmes TH, Rahe RH. The Social Readjustment Rating Scale. J Psychosom Res. 1967 11:213–218.
Mitchell SE, Newell GK, Schumm WR. Test–retest reliability of the Kansas Marital Satisfaction Scale. Psychol Rep. 1983, 53:545–546.
Schumm WR, Nichols CW, Schectman KL, Grigsby CC. Characteristics of responses to the Kansas Marital Satisfaction Scale by a sample of 84 married mothers. Psychol Rep. 1983, 53:567–572.
Schumm WR, Paff-Bergen LA, Hatch RC, Obiorah FC. Concurrent and discriminant validity of the Kansas Marital Satisfaction Scale. J Marriage Fam. 1986, 48:381–387.
Schumm WR, Anderson SA, Benigas JE, McCutchen MB, Griffin CL, Morris JE, et al. Criterion-related validity of the Kansas Marital Satisfaction Scale. Psychol Rep. 1985, 56:718.
Ahrens D, Bandi P, Ullsvik J, Moberg DP. Who smokes? A demographic analysis of Wisconsin smokers. WMJ. 2005, 104:18–22.
Baker TB, Piper ME, McCarthy DE, Majeskie MR, Fiore MC. Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychol Rev. 2004, 111:33–51.
Kenford SL, Smith SS, Wetter DW, Jorenby DE, Fiore MC, Baker TB. Predicting relapse back to smoking: Contrasting affective and physical models of dependence. J Consult Clin Psychol. 2002, 70:216–227.
Parrott AC. Acute pharmacodynamic tolerance to the subjective effects of cigarette smoking. Psychopharmacology (Berl). 1994, 116:93–97.
Mino Y, Shigemi J, Otsu T, Tsuda T, Babazono A. Does smoking cessation improve mental health? Psychiatry Clin Neurosci. 2000, 54:169–172.
Stewart AL, King AC, Killen JD, Ritter PL. Does smoking cessation improve health- related quality-of-life. Ann Behav Med. 1995, 17:331–338.
Hendricks PS, Ditre JW, Drobes DJ, Brandon TH. The early time course of smoking withdrawal effects. Psychopharmacology (Berl). 2006, 187:385–396.
Commons KG. Neuronal pathways linking substance P to drug addiction and stress. Brain Res. 2010, 1314:175–182.
Parrott AC. Stress modulation over the day in cigarette smokers. Addiction. 1995, 90:233–244.
Parrott AC. Smoking cessation leads to reduced stress, but why? Int J Addict. 1995, 30:1509–1516.
Parrott AC. Does cigarette smoking cause stress? Am Psychol. 1999, 54:817–820.
Parrott AC. Cigarette-derived nicotine is not a medicine. World J Biol Psychiatry. 2003, 4:49–55.
Parrott AC. Nicotine psychobiology: How chronic-dose prospective studies can illuminate some of the theoretical issues from acute-dose research. Psychopharmacol. 2006, 184:567–576.
Gepner AD, Piper ME, Johnson HM, Fiore MC, Baker TB, Stein JH. Effects of smoking and smoking cessation on lipids and lipoproteins: Outcomes from a randomized clinical trial. Am Heart J. 2011, 161:145–151.
Asthana A, Johnson HM, Piper ME, Fiore MC, Baker TB, Stein JH. Effects of smoking intensity and cessation on inflammatory markers in a large cohort of active smokers. Am Heart J. 2010, 160:458–463.
Johnson HM, Gossett LK, Piper ME, Aeschlimann SE, Korcarz CE, Baker TB, et al. Effects of smoking and smoking cessation on endothelial function: 1-year outcomes from a randomized clinical trial. J Am Coll Cardiol. 2010, 55:1988–1995.
U.S. Department of Health and Human Services. The health benefits of smoking cessation: A report of the Surgeon General. Publication No. (CDC) 90-8416. Rockville, MD: U.S Department of Health and Human Services; 1990.
Acknowledgments
This research was conducted at the University of Wisconsin, Madison, and was supported by grant no. P50 DA019706 from NIH/NIDA and by grant no. M01 RR03186 from the General Clinical Research Centers Program of the National Center for Research Resources, NIH. Dr. Piper was supported by grant 1UL1RR025011 from the Clinical and Translational Science Award (CTSA) program of the National Center for Research Resources (NCRR), National Institutes of Health (NIH). Dr. Baker was supported via NCI 1K05CA139871.
Conflict of interest statement
Drs. Piper, Kenford, and Baker have no potential conflicts of interest to disclose. Over the last 3 years, Michael C. Fiore served as an investigator on research studies at the University of Wisconsin that were funded in part by Nabi Biopharmaceuticals and GlaxoSmithKline. From 1997 to 2010, Dr. Fiore held a University of Wisconsin (UW) named Chair, made possible by a gift to UW from GlaxoWellcome.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Piper, M.E., Kenford, S., Fiore, M.C. et al. Smoking Cessation and Quality of Life: Changes in Life Satisfaction Over 3 Years Following a Quit Attempt. ann. behav. med. 43, 262–270 (2012). https://doi.org/10.1007/s12160-011-9329-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-011-9329-2