
Abstract
Background
Most research on adjustment of women undergoing genetic testing for breast cancer susceptibility has not followed women for more than 6 months after result receipt and has not evaluated curvilinear patterns in general and cancer-specific adjustment.
Purpose
This study’s primary goal was to examine the trajectory of psychological status in women at risk for breast and ovarian cancer prior to undergoing genetic testing through 1 year after BRCA1/2 result receipt.
Methods
Women in the UCLA Familial Cancer Registry completed questionnaires assessing psychological status (i.e., depressive symptoms, negative and positive mood, anxiety, and cancer-related distress) prior to testing and at 1, 6, and 12 months after result receipt.
Results
Of 155 women tested, 117 were BRCA1/2− (96 uninformative negative and 21 true negative) and 38 were BRCA1/2+. Linear mixed model analyses revealed a consistent pattern in adjustment indicators, such that the groups did not differ at baseline, but mutation carriers endorsed significantly more depressive symptoms, negative mood, and cancer-specific distress relative to non-mutation carriers at 1 and 6 months after test result receipt (and less positive mood at 6 months only). At 12 months, negative and positive mood returned to baseline levels for mutation carriers, and depressive symptoms approached baseline. At 12 months, the groups differed significantly only on cancer-specific distress, owing to declining distress in non-carriers. Neither having a previous cancer diagnosis nor receiving a true negative versus uninformative negative result predicted reactions to genetic testing.
Conclusions
Genetic testing prompted an increase in general and cancer-specific distress for BRCA1/2+ women, which remitted by 1 year after result receipt.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Mutations in genes BRCA1 and BRCA2 [1, 2] have been linked to a lifetime risk of 35% to 85% for breast cancer and 16% to 60% for ovarian cancer [3–6]. Found in less than 0.5% of the population [6], these mutations are believed to account for approximately 5% [7] of breast cancer cases. The primary goal of this study was to investigate prospectively the psychological impact of BRCA1/2 genetic testing and result receipt in a cohort of women over a year’s period.
Concerns that women informed of their status as BRCA1/2 carriers (i.e., BRCA1/2+) would experience anxiety and depression [8] prompted research to assess the psychological impact of testing. The majority of research suggests that most women do not experience sharp elevations in general distress after being informed that they are mutation carriers [8–18]. When the psychological status of carriers and non-carriers diverges after test receipt, this change often is driven by a decrease in the distress reported by non-carriers and stable or somewhat increased distress in carriers [12–14, 17, 18]. Accordingly, Croyle et al. [8] suggested that undergoing genetic testing can represent an effective means of coping with a familial cancer history by reducing uncertainty about risk and providing health information.
Research on change in cancer-specific distress suggests a somewhat different pattern than that on change in general distress, with more indication of cancer-related psychological disruption upon BRCA1/2+ notification [8, 14, 19–22]. For example, Watson et al. [21] reported that cancer-related worry and intrusive thoughts increased significantly in BRCA1/2 carriers 1 month after testing, whereas cancer-related worry decreased significantly in non-carriers. Furthermore, women display an increase in stress appraisals related to medical and family decision making [20] and an increase in distress and uncertainty specific to their carrier status [19] upon BRCA1/2+ result receipt. Accordingly, we hypothesized that cancer-related distress would increase in women who tested BRCA1/2+ and would decrease in non-carriers and that general distress would increase or remain stable in carriers and would decrease in non-carriers after result receipt. We were also interested in the effects of genetic testing on positive affect, given accumulating evidence for its role in psychological and physical health outcomes [23]. Cella et al. [19], the only known group to assess positive affect during BRCA1/2 testing, found that mutation carriers were less likely to report “positive experiences” (e.g., feeling happy about test results) than non-carriers 1 month after result receipt.
The health belief model [24] posits that one’s perception of the benefits of a health-related behavior predicts engagement in that behavior. A similar causal relationship between beliefs and engagement is inherent in self-regulation theory [25], which suggests that confidence in a situation’s positive outcomes spurs actions to pursue these outcomes. According to these theories, women who pursue genetic testing are more likely to believe that they will gain benefits from knowing their BRCA1/2 status than are women who do not pursue testing. Such appraisals of benefits (e.g., information gained), and perhaps concomitant increased perceived control over preventive decisions, might assist women in returning to their baseline psychological status after testing. This psychological adaptation may not be immediate, however. Theories of well-being (e.g., hedonic treadmill, [26]) and supporting research [27] suggest that threatening events can perturb psychological homeostasis for several months, but that habituation to the stressful event eventually will occur. Most studies of reactions to genetic testing follow women after result receipt for no longer than 6 months [8, 11, 13, 14, 16–20, 28, 29] and may not capture this habituation process. The above theories point to the importance of examining quadratic trends in adjustment over longer time spans and lead to the hypothesis in this study that adjustment would evidence a curvilinear pattern in mutation carriers, with evidence of a return to baseline by 1 year after genetic testing.
Return to baseline adaptation after a stressor can be conditioned by personal and contextual factors (for a review, see [30]). One such factor might be personal history of cancer. Existing studies often include either women with a personal history of breast/ovarian cancer (i.e., affected) [20] or women with no such history (i.e., unaffected) [9, 10, 14, 15, 21, 22]. To date, the direction of association between personal cancer history and distress during genetic testing has not been consistent [8, 11, 28, 29, 31]. Becoming aware of one’s status as a mutation carrier might exacerbate distress for affected women owing to the accumulation of stressful events, concern for the future health of oneself or one’s children, or the stress of associated medical decision making (e.g., prophylactic surgery). The unaffected mutation carrier, however, also faces future health threat and potentially stressful decision making.
The nature of the specific BRCA1/2 result also might affect adjustment. Previous studies often have included only women from families with a known BRCA1/2 mutation [8, 11, 12, 14, 15, 22, 28, 29]. The implications of a “true negative” result, which can only occur in families with an already identified BRCA1/2 mutation, are different from an “uninformative negative” result, which might be more likely to engender appraisals of ambiguity and threat and hence more prolonged distress [32]. Few studies have attempted to assess differences in adjustment as a function of women’s specific negative result [17, 33, 34], and their findings are disparate. The current study includes both affected and unaffected women as well as women who receive true negative and uninformative negative results to examine potential between-group differences.
Methods
Patients
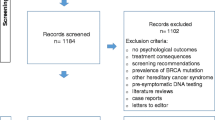
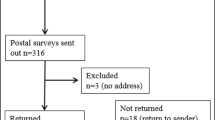
Participants were 155 women enrolled in the UCLA Genetic Evaluation Program who sought BRCA1/2 testing. They were part of a larger UCLA Familial Cancer Registry composed of individuals at high risk for breast, ovarian, or colon cancer. To be eligible for BRCA1/2 testing, patients were required to meet the following criteria: (1) age 18 or older and (2) personal or family history of breast, ovarian, or other cancer consistent with BRCA1/2 heredity and/or 10% prior probability of carrying a BRCA1/2 deleterious mutation based on published risk assessment data. Of 291 women who were eligible for genetic testing, 213 elected it. Participants underwent BRCA1/2 testing from April of 1999 through March of 2004 and were deemed eligible for analysis if they completed at least the 6-month follow-up (in order to ensure at least one assessment of longer-term adjustment). Women who tested positive for a variant of unknown significance (n = 11) were excluded from analyses because too few underwent testing to allow reliable analyses. Of the 202 women, 146 completed the 1-month follow-up assessment after genetic result receipt, 155 (77%) completed the 6-month assessment, and 130 completed the 12-month assessment. Attrition was due to death (n = 2) or noncompletion/late return of questionnaires. Preliminary analyses revealed that women who completed the 12-month assessment (n = 130) did not differ significantly from those who did not (n = 25) on any demographic or psychological variable, with the exception of positive mood (M = 38.5 for completers and 34.9 for noncompleters, p = .019).
Procedures
After women were determined eligible for the registry, they were invited to a risk assessment and genetic counseling visit with a genetic counselor, in which they also completed written informed consent and a measure of depressive symptoms [35]. Women attended a second appointment to have blood drawn for genetic testing and complete other baseline measures. Women received one of three test results (no woman declined to receive her result), given at a third meeting with the genetic counselor: (1) Women who tested positive for a known familial mutation were classified as BRCA1/2+ (positive), (2) women who tested negative for a known familial mutation were classified as BRCA1/2 true negative, and (3) women with no previously identified familial mutation who tested negative for BRCA1/2 mutations were classified as BRCA1/2 uninformative negative. Model probabilities of breast/ovarian cancer were generated for all women using the Gail and Claus models [36, 37]. BRCA1/2+ women were reminded of the benefits and limitations of BRCA1/2 genetic testing and informed of the risk for breast, ovarian, and other known associated cancers. BRCA1/2+ women with a cancer history were informed of risk for multiple primary cancers. Risks to family members such as children and siblings were discussed. Women were extensively informed of current consensus guidelines regarding cancer risk management in BRCA1/2 carriers: surveillance, prophylactic surgery, chemoprevention, and risk avoidance/lifestyle modification. Women who received a true negative result were told that their relevant family history no longer contributed to their total percentage risk of breast/ovarian cancer and that they were at the same risk as the general population or that of their own personal/reproductive risk factors. Risk calculations for women who received uninformative negative results included familial and personal risks, but these women were told that they were at no additional risk due to a known deleterious mutation. Recommendations for future surveillance and preventive options also were addressed. Women were mailed questionnaires 1, 6, and 12 months following result receipt, which they returned by mail.
Measures
Demographics
Age, race, religion, marital status, education, income, and parity were assessed by self-report questionnaire.
Cancer History
We assessed whether the participant had a personal history of cancer and whether she had undergone prophylactic mastectomy or oophorectomy, total number of first-degree female relatives who had been affected with or who had died from breast or ovarian cancer, and whether the participant had a first-degree BRCA1/2+ relative.
General Psychological Adjustment
The Center for Epidemiologic Studies—Depression Scale (CES-D) is a 20-item questionnaire with higher scores indicating more depressive symptoms [35]. The 20-item Positive and Negative Affect Scales (PANAS) were used to assess positive and negative mood during the past four weeks [38]. Higher scores indicate greater positive and negative mood, respectively. The State–Trait Anxiety Inventory (SAI) was used to evaluate state anxiety [39].
Cancer-Specific Distress
The total score on the 22-item Impact of Events Scale—Revised (IES-R) was used to evaluate cancer-specific distress [40]. The scale assesses intrusive thoughts, avoidant thoughts, and hyperarousal in relation to a specific stressful event, in this case “your genetic testing and counseling.” Because IES-R responses were skewed toward lower scores, a logarithmic transformation [log(IES-R + 1)] was applied, resulting in a more normal distribution.
At baseline, correlations between psychological adjustment variables ranged in absolute magnitude from 0.35 to 0.61, p < .0001.
Data Analysis
Data from women who completed questionnaires through the 6-month follow-up (n = 155) were included in analyses, and data were analyzed through the 12-month assessment. Given that multilevel modeling estimates missing data, women who did not complete the 12-month assessment (n = 25) were eligible for study inclusion.
Psychological adjustment across time was assessed as a function of the genetic test result. Preliminary analyses, which examined previous breast/ovarian cancer history (i.e., affected status) and the specific negative result, revealed no significant difference on outcomes as a function of affected status or BRCA1/2 true negative versus BRCA1/2 uninformative negative status; therefore, these variables were not included in the final models. General linear mixed modeling was conducted to assess differences in change over time between BRCA+ and BRCA− participants in depressive symptoms (CES-D), positive and negative affect (PANAS+ and PANAS−), state anxiety (SAI), and cancer-specific distress (IES-R). Random effects of both intercept and time were tested for each outcome measure and included in the model based upon the model fit statistics (Akaike Information Criterion and −2 Log Likelihoods). Each model used an unstructured covariance structure, which allowed for varying correlations between the random coefficients of intercept and time.
Each dependent variable was tested using the models with the main effects for time and BRCA1/2 status and the interaction of time × BRCA1/2 status. We tested non-linear trends by including the quadratic term time2, as well as an interaction of time2 × BRCA1/2 status to test for differences in the non-linear trend as a function of BRCA status. Analyses were performed using the PROC MIXED procedure in SAS v 9.1 (SAS Institute, Cary, NC, USA).
Results
Sample Characteristics
Sample characteristics are shown in Table 1. The majority of patients were white (91%) and in a committed relationship (81%). Approximately half the sample had an annual household income greater than $100,000 and had education beyond college.
The final sample included 155 women who completed the 6-month assessment; of these, 130 provided 12-month data. Thirty-eight (24.5%) were BRCA1/2+ and 117 (75.5%) were BRCA1/2− (96 uninformative negatives and 21 true negative). Women who had been diagnosed with stages 1–4 breast cancer or ductal carcinoma in situ were considered affected; 84 (54%) women were affected and 71 (46%) women were unaffected. Of BRCA1/2+ women, 25 were affected and 13 were not. Of BRCA1/2− women, 59 were affected and 58 were not. Seventeen of the affected women were diagnosed in the same year that they underwent testing. Fifteen women had received prophylactic surgeries prior to baseline.
Baseline Group Differences and Selection of Covariates
Women with a positive test result were significantly younger and more likely to have a BRCA1/2+ relative than were BRCA− women (Table 1). No other significant difference on any baseline variable emerged as a function of test result. Three significant relations of potential demographic and cancer-related covariates with dependent variables emerged. Women with annual household incomes lower than $100,000 reported more depressive symptoms than more affluent women, F(1,147) = 9.94, p = 0.002. White women reported more positive mood than other women, F(1,150) = 7.05, p = 0.009. Women who were not in a committed relationship reported less cancer-related distress than women in a committed relationship, F(1,150) = 4.99, p = 0.027. These variables were controlled in analyses of the relevant dependent variable.
Descriptive Statistics on Psychological Variables
Table 2 displays means on outcome measures stratified by BRCA1/2 status over time. The range of observed scores on each measure was CES-D = 0–57, PANAS+ = 13–50, PANAS− = 10–50, SAI = 20–78, and logIES-R = 0–1.45.
Effects of BRCA1/2 Status on Dependent Variables
Table 3 displays results of the mixed model analyses. As displayed in Fig. 1, analyses revealed significant time × BRCA1/2 status interactions for the CES-D, PANAS+, PANAS−, and IES-R.

Adjusted means on outcomes for significant time × BRCA1/2 status interactions plotted from baseline through 12-month follow-up, controlling for all other significant covariates in mixed models
Depressive Symptoms
A significant interaction of time × BRCA1/2 status emerged for the CES-D, which indicates that the slope of CES-D, F(1,415) = 4.16, p = 0.042, differed significantly between BRCA1/2+ and BRCA1/2− women. BRCA1/2+ women’s report of depressive symptoms rose from baseline to 1 month and decreased from 6 to 12 months. BRCA1/2− women’s CES-D scores were stable over time.
To examine group differences in the CES-D further, adjusted mean scores were compared between groups at each assessment point, and percentages who reached the cutoff of 16 suggestive of a clinically meaningful level of depressive symptoms were examined. Depressive symptoms were significantly higher in BRCA1/2+ women than BRCA1/2− women at 1 month (p = .018) and 6 months after adjusting for income (p = 0.006; comparison of unadjusted CES-D means yielded the same findings). In addition, 24%, 36%, 34%, and 22% of BRCA+ women had CES-D scores of 16 or above at each sequential assessment, whereas 22%, 20%, 20%, and 23% of BRCA1/2− women had scores suggestive of clinical depression (Χ 2 results: p = 0.190, p = 0.005, p = 0.025 and p = 0.311, respectively).
Positive Mood
A significant time × BRCA1/2 status interaction indicates that the slope of PANAS+, F(1,425) = 7.02, p = 0.008, differed significantly between BRCA1/2+ and BRCA1/2− women. The significant time2 × BRCA1/2 status interaction indicates a quadratic slope in PANAS+, F(1,425) = 5.90, p = 0.015, for BRCA1/2+ women only. Positive mood decreased from baseline to 1 month and increased from 6 to 12 months in BRCA1/2+ women. BRCA1/2− women’s PANAS+ scores were stable over time. Adjusting for race, PANAS+ scores were significantly higher for BRCA1/2− women than BRCA1/2+ women at the 6-month assessment point (p = 0.033).
Negative Mood
Both time × BRCA1/2 status and time2 × BRCA1/2 status interactions were significant. The interaction of time × BRCA1/2 status indicates that the slope of PANAS−, F(1,425) = 6.71, p = 0.010, over time differed significantly between BRCA1/2+ and BRCA1/2− women. The significant interaction of time2 × BRCA1/2 status coupled with a non-significant time2 term indicates a quadratic slope in PANAS−, F(1,425) = 7.45, p = 0.007, for BRCA1/2+ women only. Specifically, BRCA1/2+ women’s report of negative mood rose from baseline to 1 month and decreased from 6 to 12 months. BRCA1/2− women’s PANAS− scores were stable over time. Negative mood was significantly higher in BRCA1/2+ women than in BRCA1/2− women at 1 month (p = 0.010) and 6 months (p = 0.002).
State Anxiety
The main effect of time on the SAI, F(1,425) = 4.45, p = .036 was significant. State anxiety increased over time for both BRCA1/2+ and BRCA1/2− women. No interaction term was significant.
Cancer-Related Distress
Analyses revealed a significant time × BRCA1/2 status interaction, F(1,424) = 5.20, p = 0.023. Cancer-specific distress decreased steadily over time for BRCA1/2− women, whereas it increased from baseline to 1 month and decreased from 6 to 12 months in BRCA1/2+ women. Adjusted cancer-related distress was higher in BRCA1/2+ than BRCA1/2− women at 1 month (p = 0.001), 6 months (p = 0.001), and 12 months (p = 0.005).
Discussion
The current study prospectively examined psychological concomitants of BRCA1/2 mutation testing in a sample of women through 1 year after result receipt. In contrast to some prior research suggesting that psychological adjustment remains unchanged in mutation carriers [12, 13, 16, 17], results revealed that BRCA1/2+ women experienced heightened general and cancer-related distress for several months after test result receipt relative to BRCA1/2− women. General distress in the form of depressive symptoms and negative mood were heightened and positive mood declined at 1 and 6 months after result receipt for mutation carriers relative to non-carriers. Although group means were within normal limits, it is notable that CES-D scores exceeded the clinical cut-off of 16 for more than one third of the BRCA1/2 mutation carriers at 1 and 6 months following result receipt. At 12 months, positive and negative mood returned to baseline levels and depressive symptoms approached baseline for carriers, and scores did not differ significantly between mutation carriers and non-carriers. As hypothesized, cancer-specific distress evidenced a similar pattern for mutation carriers and a “relief” effect for non-carriers, diminishing over the 12 months. Thus, although cancer-specific distress was low in general and returned to baseline for carriers, it continued to exceed distress in non-carriers at 12 months. Declining cancer-specific distress in non-carriers is consistent with findings in other studies [10, 14, 17] and with the suggestion that genetic testing may benefit BRCA1/2− women by relieving distress related to cancer.
For mutation carriers, the immediate months after test receipt often involve decisions about prophylactic options and communication of results to family and friends; these activities, accompanied by one’s own emotional and cognitive processing of the result, may explain the heightened distress observed during this period. That elevated distress diminished by 12 months following genetic test receipt is consistent with theories regarding the time-limited effects of stressful life events on well-being [26, 27]. Overall, this pattern of diminished positive mood and heightened distress that eventually remits for BRCA1/2+ women was evident across dependent variables and suggests that there is a psychological adjustment period after discovering that one carries a BRCA1/2 mutation.
It is important to consider the impact that cancer-related distress may have on the health behaviors of both BRCA1/2+ and BRCA1/2− women. The majority of research on the relationship between cancer-related anxiety/worry and breast cancer screening practices suggests that higher cancer-related anxiety predicts greater likelihood of screening [41–44]; therefore, it is possible that the elevated 12-month cancer-related distress in BRCA1/2+ women relative to BRCA1/2− women serves a positive function. For BRCA1/2− women, whose cancer-related distress is significantly reduced, reminders that cancer screening is still vital may aid in ensuring optimal surveillance.
Reactions to genetic test results did not differ significantly as a function of affected status or the specific negative result, and these factors are associated inconsistently with adjustment in the existing literature. It is possible that personal cancer history and the specific genetic result interact in complex ways over time; however, with only 21 women who received a true negative result, the current research likely did not have the statistical power to reveal such differences. Another possibility is that the particular genetic counseling context prompts differences in findings. For example, at UCLA, counseling is individualized for each woman, but true negative women are counseled differently from uninformative negative women in that true negative women are told that relevant family history (i.e., affected individuals in their family who are BRCA1/2+) no longer factors into their overall risk for breast/ovarian cancer. Women with true negative results are informed that they have the general population risk for breast/ovarian cancer or the risk associated with their own personal or reproductive risk factors. Women with uninformative negative results are counseled that their risks are not increased due to a known BRCA1/2 deleterious mutation; however, they still have increased risk for breast/ovarian cancer due to their family history and their own personal/reproductive risk factors. Genetic counselors in other settings may place more emphasis on the possibility of a medically relevant unidentified mutation in uninformative negative women and thereby increase uncertainty, which is linked to distress in the genetic testing context [45]. The framing of medical information is influential for patients, and it is important for researchers to describe the counseling provided to women in order to clarify disparate findings.
A potentially important explanation for the literature’s somewhat inconsistent findings regarding effects of personal cancer history and the specific negative result on reactions to genetic testing is that other parameters associated with the individual and their interpersonal environment condition reactions to genetic testing. In a theoretical synthesis regarding dissemination of cancer genomics, Hay et al. [46] posit that genetic information becomes “cognitively and affectively personalized” (p. 277), influenced by lay and familial explanations for disease [47], perceptions of control, and other personal meanings. These factors might moderate or exceed the influence of other variables, such as personal cancer history, on reactions to genetic testing. Similarly, revisions [30] of extant theories of well-being suggest that, rather than automatic habituation to stressors prompting a return to baseline well-being, individual differences such as personality attributes and coping strategies explain how the trajectory of adaptation varies after stressful events. Such constructs deserve greater study in the genetic testing context.
Although our findings suggest that professionals can reassure women who receive a BRCA1/2+ result that their distress is likely to diminish with time, approaches to accelerate psychological recovery deserve study, particularly for women who report elevated depressive symptoms. Furthermore, the unanticipated finding that women who were in a committed relationship experienced more cancer-related distress while undergoing genetic testing than did non-partnered women is notable. This relationship existed in the absence of any relationship between having children and psychological adjustment, suggesting that the finding may be due to women’s concerns over how their BRCA1/2 status might influence their partner and relationship. Further examination of the impact of relationship status and related constructs warrants attention. In addition, follow-up beyond 1 year would be informative. One study [48] of 65 women revealed that anxiety and depressive symptoms increased significantly in BRCA1/2− and BRCA1/2+ women from 1 year to approximately 5 years after testing, predicted by cancer-specific distress, having lost a relative to breast/ovarian cancer, less open communication about the test result, and other factors. Future research also is necessary to assess the generalizability of findings and implications for intervention in groups beyond this relatively highly educated and affluent sample, as women of lower socioeconomic status might have fewer resources to cope with genetic testing-related stress. Finally, future studies focusing on women’s medical decision making and processing of cancer-related material in tandem with psychosocial assessment will promote understanding of how changing distress levels influence women’s behaviors related to cancer surveillance and prevention within the genetic testing context.
References
Miki Y, Swensen J, Shattuck-Eidens D, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994; 266: 66–71.
Wooster R, Bignell G, Lancaster J, et al. Identification of the breast cancer susceptibility gene BRCA2. Nature. 1995; 378: 789–792.
Antoniou A, Pharoah PD, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. Am J Hum Genet. 2003; 72: 1117–1130.
Easton DF, Ford D, Bishop DT. Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am J Hum Genet. 1995; 56: 265–271.
Ford D, Easton DF, Bishop DT, Narod SA, Goldgar DE. Risks of cancer in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Lancet. 1994; 343: 692–695.
Struewing JP, Hartge P, Wacholder S, et al. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997; 336: 1401–1408.
Szabo CI, King MC. Inherited breast and ovarian cancer. Hum Mol Genet. 1995; 4: 1811–1817.
Croyle RT, Smith KR, Botkin JR, Baty B, Nash J. Psychological responses to BRCA1 mutation testing: Preliminary findings. Health Psychol. 1997; 16: 63–72.
Arver B, Haegermark A, Platten U, Lindblom A, Brandberg Y. Evaluation of psychosocial effects of pre-symptomatic testing for breast/ovarian and colon cancer pre-disposing genes: A 12-month follow-up. Fam Cancer. 2004; 3: 109–116.
Claes E, Evers-Kiebooms G, Denayer L, et al. Predictive genetic testing for hereditary breast and ovarian cancer: Psychological distress and illness representations 1 year following disclosure. J Genet Couns. 2005; 14: 349–363.
Dorval M, Patenaude AF, Schneider KA, et al. Anticipated versus actual emotional reactions to disclosure of results of genetic tests for cancer susceptibility: Findings from p53 and BRCA1 testing programs. J Clin Oncol. 2000; 18: 2135–2142.
Kinney AY, Bloor LE, Mandal D, et al. The impact of receiving genetic test results on general and cancer-specific psychologic distress among members of an African-American kindred with a BRCA1 mutation. Cancer. 2005; 104: 2508–2516.
Lerman C, Narod S, Schulman K, et al. BRCA1 testing in families with hereditary breast-ovarian cancer. A prospective study of patient decision making and outcomes. JAMA. 1996; 275: 1885–1892.
Lodder L, Frets PG, Trijsburg RW, et al. Psychological impact of receiving a BRCA1/BRCA2 test result. Am J Med Genet. 2001; 98: 15–24.
Lodder L, Frets PG, Trijsburg RW, et al. One year follow-up of women opting for presymptomatic testing for BRCA1 and BRCA2: Emotional impact of the test outcome and decisions on risk management (surveillance or prophylactic surgery). Breast Cancer Res Treat. 2002; 73: 97–112.
Reichelt JG, Heimdal K, Møller P, Dahl AA. BRCA1 testing with definitive results: A prospective study of psychological distress in a large clinic-based sample. Fam Cancer. 2004; 3: 21–28.
Schwartz M, Peshkin B, Hughes C, Main D, Isaacs C, Lerman C. Impact of BRCA1/BRCA2 mutation testing on psychological distress in a clinic-based sample. J Clin Oncol. 2002; 20: 514–520.
Tercyak K, Lerman C, Peshkin B, et al. Effects of coping style and BRCA1 and BRCA2 test results on anxiety among women participating in genetic counseling and testing for breast and ovarian cancer risk. Health Psychol. 2001; 20: 217–222.
Cella D, Hughes C, Peterman A, et al. A brief assessment of concerns associated with genetic testing for cancer: The multidimensional impact of cancer risk assessment (MICRA) questionnaire. Health Psychol. 2002; 21: 564–572.
Halbert CH, Schwartz MD, Wenzel L, et al. Predictors of cognitive appraisals following genetic testing for BRCA1 and BRCA2 mutations. J Behav Med. 2004; 27: 373–392.
Watson M, Foster C, Eeles R, et al. Psychosocial impact of breast/ovarian (BRCA1/2) cancer-predictive genetic testing in a UK multi-centre cohort. Br J Cancer. 2004; 91: 1787–1794.
Meiser B, Butow P, Friedlander M, et al. Psychological impact of genetic testing in women from high-risk breast cancer families. Eur J Cancer. 2002; 38: 2025–2031.
Fredrickson BL. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am Psychol. 2001; 56: 218–226.
Becker MH, Maiman LA. Sociobehavioral determinants of compliance with health and medical care recommendations. Med Care. 1975; 13: 10–24.
Carver CS, Scheier MF. Principles of self-regulation: Action and emotion. In: Higgins ET, Sorrentino RM, eds. Handbook of Motivation and Cognition: Foundations of Social Behavior. New York: Guilford; 1990: 3–52.
Brickman P, Campbell DT. Hedonic relativism and planning the good society. In: Appley MH, ed. Adaptation Level Theory: A Symposium. New York: Academic; 1971: 287–302.
Suh E, Diener E, Fujita F. Events and subjective well-being: Only recent events matter. J Pers Soc Psychol. 1996; 70: 1091–1102.
van Roosmalen MS, Stalmeier PF, Verhoef LC, et al. Impact of BRCA1/2 testing and disclosure of a positive result on women affected and unaffected with breast or ovarian cancer. Am J Med Genet. 2004; 124A: 346–355.
Lerman C, Hughes C, Lemon SJ, et al. What you don’t know can hurt you: Adverse psychologic effects in members of BRCA1-linked and BRCA2-linked families who decline genetic testing. J Clin Oncol. 1998; 16: 1650–1654.
Diener E, Lucas RE, Scollon CN. Beyond the hedonic treadmill: Revising the adaptation theory of well-being. Am Psychol. 2006; 61: 305–314.
Coyne JC, Kruus L, Racioppo M, Calzone KA, Armstrong K. What do ratings of cancer-specific distress mean among women at high risk of breast and ovarian cancer? Am J Hum Genet. 2003; 116: 222–228.
Baum A, Friedman AL, Zakowski SG. Stress and genetic testing for disease risk. Health Psychol. 1997; 16: 8–19.
Dorval M, Gauthier G, Maunsell E, et al. No evidence of false reassurance among women with an inconclusive BRCA1/2 genetic test result. Cancer Epidemiol Biomarkers Prev. 2005; 14: 2862–2867.
van Dijk S, Timmermans DR, Meijers-Heijboer H, Tibben A, van Asperen CJ, Otten W. Clinical characteristics affect the impact of an uninformative DNA test result: The course of worry and distress experienced by women who apply for genetic testing for breast cancer. J Clin Oncol. 2006; 24: 3672–3677.
Radloff L. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977; 1: 385–401.
Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer. Implications for risk prediction. Cancer. 1994; 73: 643–651.
Gail MH, Brinton LA, Byar DP, et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst. 1989; 81: 1879–1886.
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Pers Soc Psychol. 1988; 54: 1063–1070.
Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State—Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologist Press; 1970.
Weiss DS, Marmar CR. The impact of event scale-revised. In: Wilson JP, Deane TM, eds. Assessing Psychological Trauma and PTSD. New York, NY: Guilford; 1997: 399–411.
Brain K, Norman P, Gray J, Mansel R. Anxiety and adherence to breast self-examination in women with a family history of breast cancer. Psychosom Med. 1999; 61: 181–187.
Diefenbach MA, Miller SM, Daly MB. Specific worry about breast cancer predicts mammography use in women at risk for breast and ovarian cancer. Health Psychol. 1999; 18: 532–536.
McCaul KD, Mullens AB. Affect, thought, and self-protective health behavior: The case of worry and cancer screening. In: Suls J, Wallston K, eds. Social Psychological Foundations of Health and Illness. Malden, MA: Blackwell; 2003: 137–168.
Hay JL, McCaul KD, Magnan RE. Does worry about breast cancer predict screening behaviors? A meta-analysis of the prospective evidence. Prev Med. 2006; 42: 401–408.
O’Neill SC, DeMarco T, Peshkin BN, et al. Tolerance for uncertainty and perceived risk among women receiving uninformative BRCA1/2 test results. Am J Med Genet. 2006; 142C: 251–259.
Hay JL, Meischke HW, Bowen DJ, et al. Anticipating dissemination of cancer genomics in public health: A theoretical approach to psychosocial and behavioral challenges. Ann Behav Med. 2007; 34: 275–286.
McAllister M. Predictive genetic testing and beyond: A theory of engagement. J Health Psychol. 2002; 7: 491–508.
van Oostrom I, Meijers-Heijboer H, Lodder LN, et al. Long-term psychological impact of carrying a BRCA1/2 mutation and prophylactic surgery: A 5-year follow-up study. J Clin Oncol. 2003; 21: 3867–3874.
Acknowledgment
This research was supported by funding from the Breast Cancer Research Foundation to Dr. Stanton. Dr. Ganz was supported through an American Cancer Society Clinical Research Professorship and Dr. Vodermaier by a stipend from the Dr.-Werner-Jackstaedt-Stiftung of the Founder Association of the German Sciences (S134-10.021). The Cancer Center Core Grant (P30 CA 16042) and the Jonsson Cancer Center Foundation provided funding for the UCLA Familial Cancer Registry.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Beran, T.M., Stanton, A.L., Kwan, L. et al. The Trajectory of Psychological Impact in BRCA1/2 Genetic Testing: Does Time Heal?. ann. behav. med. 36, 107–116 (2008). https://doi.org/10.1007/s12160-008-9060-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-008-9060-9