
Abstract
Background
Tailored health communications to date have been based on a rather narrow set of theoretical constructs.
Purpose
This study was designed to test whether tailoring a print-based fruit and vegetable (F & V) intervention on relatively novel constructs from self-determination theory (SDT) and motivational interviewing (MI) increases intervention impact, perceived relevance, and program satisfaction. The study also aimed to explore possible user characteristics that may moderate intervention response.
Methods
African American adults were recruited from two integrated health care delivery systems, one based in the Detroit Metro area and the other in the Atlanta Metro area, and then randomized to receive three tailored newsletters over 3 months. One set of newsletters was tailored only on demographic and social cognitive variables (control condition), whereas the other (experimental condition) was tailored on SDT and MI principles and strategies. The primary focus of the newsletters and the primary outcome for the study was fruit and vegetable intake assessed with two brief self-report measures. Preference for autonomy support was assessed at baseline with a single item: “In general, when it comes to my health I would rather an expert just tell me what I should do”. Most between-group differences were examined using change scores.
Results
A total of 512 (31%) eligible participants, of 1,650 invited, were enrolled, of which 423 provided complete 3-month follow-up data. Considering the entire sample, there were no significant between-group differences in daily F & V intake at 3 month follow-up. Both groups showed similar increases of around one serving per day of F & V on the short form and half a serving per day on the long form. There were, however, significant interactions of intervention group with preference for autonomy-supportive communication as well as with age. Specifically, individuals in the experimental intervention who, at baseline, preferred an autonomy-supportive style of communication increased their F & V intake by 1.07 servings compared to 0.43 servings among controls. Among younger controls, there was a larger change in F & V intake, 0.59 servings, than their experimental group counterparts, 0.29 servings. Conversely, older experimental group participants showed a larger change in F & V, 1.09 servings, than older controls, 0.48.
Conclusion
Our study confirms the importance of assessing individual differences as potential moderators of tailored health interventions. For those who prefer an autonomy-supportive style of communication, tailoring on values and other motivational constructs can enhance message impact and perceived relevance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
For more than 15 years, individually tailored interventions have been used to modify a wide range of health behaviors, including a large number focusing on dietary change [1–17]. Although the precise mechanisms by which tailored interventions produce their desired affects have not been fully explicated, tailoring appears to increase recipient attention, processing effort, perceived message relevance, and perceived message salience [15, 18–20]. Due to their capacity for both high efficacy and high reach, tailored interventions hold particular promise for achieving significant public health impact.
Although there has been diversity in the types of health behaviors that have been addressed, the majority of tailored interventions to date have been grounded in a rather narrow set of theoretical constructs, most notably the transtheoretical model, social cognitive theory (SCT), and the health belief model [6, 15, 17, 20–30]. However, as suggested in a recent review by Noar et al. [30], inclusion of multiple psychologic constructs may enhance the effectiveness of tailored interventions.
This study was designed to test whether tailoring on theoretical approaches that have not heretofore been incorporated in tailored interventions can improve both process and outcome measures. Specifically, the study examined whether the inclusion of tailored messages based on principles and strategies drawn from self-determination theory and motivational interviewing (experimental group) can increase intervention impact, perceived relevance, and program satisfaction compared to an intervention based on “usual” SCT tailoring (control group).
Although some studies have examined potential sociodemographic moderators of response to tailored interventions [30, 31], there is a need to explore potential psychologic moderators of program impact. Therefore, a secondary aim of the study was to explore possible user characteristics that may moderate response to the two interventions. Specifically, we hypothesized that individuals who prefer a more physician-centered style of communication would respond more strongly to the control intervention which was written in a more directive tone, and individuals who preferred a more patient-centered style of communication would be more responsive to the experimental intervention, which was written in a more autonomy-supportive tone.
Self-determination theory (SDT), originally proposed by Deci and Ryan and expounded on by others [32–34], differentiates between autonomous and controlled behavioral regulation [33, 35–37]. Behaviors are autonomous when they result from conscious choice and are personally relevant. Conversely, behaviors are considered controlled when performed due to pressure or coercion, either by external or internal forces. A key principal of SDT used to design the experimental intervention is that messages that enhance autonomy and perceived competence and are consistent with a person’s values and goals will be more effective in changing behavior than messages focusing on external rewards such as pleasing others, fear of disease, or avoiding guilt, anxiety, or shame.
Motivational interviewing (MI) is a counseling approach that employs many of the principles of SDT [34]. Key MI concepts adapted for the experimental intervention include allowing participants to develop their own arguments for change, not prematurely pushing an individual to change, selectively using directive behavioral advice and persuasive messages, and encouraging participants to find meaning in their decisions.
The study focuses on African Americans in part due to their higher rates of diet-related illness [38], higher prevalence of chronic disease risk factors, lower fruit and vegetable intake [39, 40], and historical lack of participation in tailored intervention studies.
Methods
Participants were recruited from the memberships of two integrated health care delivery systems, one based in the Detroit Metro area and the other in the Atlanta Metro area. Both health care systems were asked to provide randomly selected lists of African-American adults ages 21 to 70. The Detroit healthcare system had race indicated in their electronic records. The Georgia healthcare system did not contain race or ethnicity information in its medical records. Therefore, the Georgia study sample was randomly selected from healthcare system members who attended medical offices where members were primarily African American and who had home addresses in Census blocks in which 80% or more of the residents were African American.
Health plan members were mailed an invitation to participate in the study. The letter, which contained a $2 pre-incentive, contained a toll-free number that allowed members to opt out of the study. Health plan members who did not call to opt out were phoned beginning 7 days after the invitation letters were mailed to verify their eligibility and complete their baseline surveys. Unresolved cases were called a minimum of 14 times during the 8-week period after the invitation letters were sent. Eligibility criteria included self-identifying as Black or African American, living at least half of their life in the USA, being between 21 and 70 years of age, and consuming less than ten servings of fruit and vegetables (F & V) per day. Individuals who identified as bi-racial or bi-ethnic were excluded. Interviews were completed with 31% of eligible health plan members. Participants who enrolled and completed the baseline survey received a thank you letter containing a $5 bill.
A follow-up phone survey was administered approximately 3 months post-baseline to measure changes in F & V intake and other key variables. The follow-up survey also included questions about the perceived personal relevance of the newsletters, message recall, and the number of newsletters received and read. All participants who completed the follow-up survey received a choice of a $15 gift card to a local grocery or retail store. If no contact was made with participants (because of non-working numbers or no contact information), a letter was mailed to the participant asking him or her to make contact and provide a current phone number or preferred contact dates and times. Follow-up interviews were completed with 423 participants or 84% of the baseline participants.
The study was approved by Human Subjects Committees from the University of Michigan and the two participating integrated health care delivery sites.
Intervention
Participants in both the experimental and control groups received three newsletters by mail that were 12, 12, and 8 pages in length, respectively. The newsletters, delivered approximately once a month over 3 months, focused on increasing F & V intake. Each newsletter mailing included two recipe cards with small bags of spices that corresponded to the recipes in that edition and either a magnetized refrigerator notepad or a magnet with F & V serving size information.
Control Tailored Intervention
The control intervention was tailored on age, gender, medical history, and food preferences, as well as several SCT constructs such as outcome expectancies, social support, and barriers to eating F & V. Some sections of the newsletters were untailored and addressed such topics as nutrition information, “slow food”, and trivia about F & V. Testimonials were also included, some of which were tailored on barriers to eating F & V, geographic region of residence, and gender (Table 1).
Experimental Tailored Intervention
Most of the tailoring in the control intervention was included in the experimental intervention. However, experimental group participants received additional tailored text and graphics aimed at increasing their autonomous motivation to eat more F & V. For example, participants were asked to explore how their personal values, religion, and spirituality might be related to their F & V intake. For individuals reporting no involvement in organized religion, messages referred to spirituality, whereas if they were active members of an organized religion, text referred to that specific religion. Rather than motivating by exhortation or direct persuasion, the SDT-based intervention encouraged participants to find their own motivation for change and solutions to barriers.
Here is an example of how messages were tailored to motivational predisposition using participant responses to the Treatment Self-Regulation Questionnaire (TSRQ; described below). Autonomous/intrinsic motivation: “Based on your survey responses it sounds like you have some meaningful reasons for wanting to eat better. You’ve told us that eating fruits and vegetables as part of a healthy diet is important for being as healthy as possible. In the following section we’re going to help you find additional reasons to motivate and inspire you to eat better and lead a healthier life.” Introjected motivation: “Based on your survey responses it seems you are often your own toughest critic when it comes to what you eat. You’ve told us that you feel guilty or ashamed if you do not eat fruits and vegetables. Reasons like these can get you started on the road to better eating, but many people find that lifestyle changes such as healthier eating are easier when they find more meaningful, personal reasons for doing them. In the following section we’re going to help you find additional reasons to motivate and inspire you to eat better and lead a healthier life.”
Borrowing a clinical strategy often used in MI [41, 42], participants were asked to rate their motivation and confidence to eat more F & V using a zero to ten scale. They were then asked to reflect on the numbers they chose, and, in subsequent sections or editions of the newsletter, they were asked to ponder whether their motivation and/or confidence ratings had changed, and, if so, why. Graphics were also tailored on personal values and motivational characteristics.
For most experimental group members, the tone of newsletters was written to encourage autonomy support [33, 43]. Accordingly, rather than motivating by exhortation or direct persuasion, participants were prompted to come up with their own motivations, solutions to barriers, and behavioral goals. Nonetheless, we assumed that some individuals would prefer a more directive style to their newsletters and would not respond to an autonomy-supportive tone. For this subgroup, identified by scores of 4 or lower (out of 7) on an abbreviated Need for Cognition Scale [44], more directive messages were provided.
Just as self-efficacy is a central element of SCT, the related concept of perceived competence is an important component of motivation within SDT. However, whereas self-efficacy is typically used to overcome barriers to change or lack of confidence in one’s ability to change in SCT, in SDT, perceived competence is used to build autonomous motivation in part through linkage to values and other sources of integrated regulation (Shaikh et al., under review) [36, 45]. In SDT, perceived competence is considered one of three universal human needs, along with autonomy and relatedness, and it appears empirically to covary with autonomous motivation but not extrinsic motivation (Shaikh et al., under review) [45, 36, 46]. Therefore, in this study, in part due to the unique relationship between perceived competence and autonomous motivation as well as to maximize conceptual separation between the two intervention groups, self-efficacy/perceived competence content was included only in the experimental newsletters.
Measures
The primary outcome for the study was servings of F & V consumed per day assessed with two brief frequency measures. The first measure (referred to as the long form) queried intake of fruit, 100% fruit or vegetable juice, beans, potatoes other than French fries, vegetables, and salads over the past week. The second measure (labeled short form) assessed usual daily intake of fruit, 100% fruit or vegetable juice, and vegetables. The two measures were also averaged to form a “triangulated” composite measure of fruit and vegetable intake, which was used as an outcome variable for selected analyses. Validity of prior similar versions of these measures can be found elsewhere [47, 48].
Four individuals (three females and one male) reporting implausible F & V intake values were excluded from all analyses. The plausible maximum value for intake was set at 14 servings per day on the composite F & V measure. The study was powered to detect a between group difference of 0.5 to 0.6 daily servings of F & V.
Secondary Outcomes
Outcome expectations were assessed with six items adapted from prior studies [49, 50] that queried physical and psychologic benefits of eating more fruit and vegetables such as “If I eat more fruit and vegetables I will feel proud of myself” and “Eating more fruit and vegetables will give me more energy.” Items were scaled from 1 (strongly disagree) to 4 (strongly agree) and summed. Internal consistency in this sample was 0.79.
Self-efficacy to eat fruit and vegetables was assessed with four items adapted from prior studies [49, 50] that included “How confident are you that you could eat a healthy snack, like fruit or vegetables, when you’re really hungry?” and “How confident are you that you could eat healthy foods, like fruit or vegetables, when you are depressed or in a bad mood?” Items were scaled from 1 (not at all confident) to 4 (very confident) and summed. Internal consistency in this sample was 0.73.
Autonomous/controlled motivation was assessed with an adapted version of the TSRQ developed by Williams et al. [37, 43, 51]. The 20-item measure yields two subscales: (1) autonomous motivation and (2) controlled motivation. The TSRQ was modified to address fruit and vegetable intake and increased by two items. All of the items begin with “A reason I eat fruits and vegetables is…” Sample items from the autonomous scale include “Because I personally believe it is a good thing for my health” and “Because I have carefully thought about it and believe it is very important for me”. Sample items from the controlled scale include “Because I would feel guilty or ashamed of myself if I didn’t” and “Because others would be upset with me if I didn’t.” Items were scaled from 1 (strongly disagree) to 7 (strongly agree) and summed. Internal consistency for the autonomous and controlled motivation scales was 0.89 and 0.86, respectively.
Intention to eat more fruit and vegetables in the next month was assessed with two items, one each for fruit and vegetables, and scaled 0 (strongly disagree) to 10 (strongly agree), worded as follows: “I intend to increase the amount of fruit/vegetables I eat over the next month.”
Moderator Variable
We used a single item to assess preference for autonomy supportive versus more directive communication: “In general, when it comes to my health I would rather an expert just tell me what I should do.” Reponses to this item ranged from 1 (strongly disagree) to 7 (strongly agree). We hypothesized that individuals who disagreed with this item (i.e., high autonomy support preference) would respond more positively to the experimental intervention than to the control intervention, as the experimental intervention was written, both in terms of tone and content, to support autonomous decision making.
Process Variables
Satisfaction with each member’s health plan and satisfaction with the overall intervention were assessed in both the experimental and control groups using single items scaled 1 (not at all satisfied) to 10 (extremely satisfied). Health plan satisfaction was queried both at baseline and follow-up, whereas program satisfaction was assessed only at follow-up.
Perceived relevance of the intervention was assessed by summing two items scaled 1 (not at all) to 4 (completely): (1) “How much do you feel that the Eat for Life newsletter(s) (was/were) written for you?” and (2) “How well do you feel that the Eat for Life newsletter(s) fit your personal values and beliefs?”
At follow-up, participants were also asked to respond “yes” or “no” to items querying whether they recalled seeing newsletter content related to personal values, religious themes, motivational quotes, the health effects of eating fruit and vegetables, serving size information, goal setting, and other topics. Some of these topics were addressed in the experimental intervention only, whereas other topics were found in both the experimental and control newsletters. A few topics not contained in either set of newsletters were included as distracters.
Statistical Analyses
The primary model for testing between-group effects was analysis of covariance (ANCOVA) using difference scores as the dependent variables while adjusting for potential confounds of age, income, site (Detroit/Atlanta), and gender. An identical model was utilized for follow-up only process measures. Within-group tests were based on paired t tests. Cases missing data at follow-up were dropped from analyses rather than imputed.
The initial ANCOVA models testing intervention effects included interaction terms for gender, age, income, site, and preference for autonomy support. Non-significant interactions (p > 0.10) were dropped from subsequent models. Servings of F & V on the long, short, and composite measures were transformed using their square root to normalize their distribution. All reported significance levels are based on the transformed values.
Results
Sample Description
A total of 1,650 (854 from the Atlanta site and 796 from the Detroit site) randomly selected participants were sent recruitment letters. Of the 1,650 recruits, 512 (31%), comprising 255 (30%) from the Atlanta site and 257 (32%) from the Detroit site, eligible African Americans were enrolled. Eight subjects were removed due to incomplete or invalid data. Of the remaining 504 subjects, 423 (82%; 206 from Atlanta and 217 from Detroit) provided usable 3-month follow-up data. As shown in Table 2, the final cohort sample was predominantly female (72%), with a mean age of 48 years (ranging from 22 to 69). Most (78%) worked full time, and about half (45%) were married. Most participants earned at least $40,000 annually, and the majority had at least some college education. Mean F &V intake at baseline was somewhat higher on the short than long fruit and vegetable measure, 4.1 and 3.3 servings per day, respectively (Fig. 1).

Subject flow
As shown in Table 2, the 81 participants lost to follow-up did not differ from the 423 cohort members with regard to gender, employment status, or income. However, dropouts were significantly younger, had lower educational attainment, and were less likely to be married than cohort members. Dropouts also reported significantly lower baseline F & V intake on the short and composite measures, but not the long form. With regard to differential attrition, dropouts between study groups did not differ significantly for any of the variables contained in Table 2.
At baseline, participants in the two study groups did not differ significantly on any of the variables listed in Table 3. At follow-up, the two groups recalled receiving similar numbers of newsletters. In the experimental group, 34% reported receiving two newsletters and 53% reported receiving all three newsletters. The corresponding rates in the control group were 30% and 56%. An almost equivalent percentage of experimental (70%) and control group (68%) participants reported reading most or all of their newsletters.
Primary Outcome
The experimental and control groups showed similar increases in self-reported F & V intake at the 3-month follow-up of 0.9 and 0.8 servings per day, respectively, on the short F&V measure (Table 4). These within-group changes were significant (p < 0.01). Similarly, significant within-group changes of 0.5 and 0.4 servings per day were observed for the experimental and control groups, respectively, on the long form. There were no significant between-group differences for the short, long, or composite measures in the full sample.
There was a significant interaction of the intervention by participants’ response to the item “In general, when it comes to my health I would rather an expert just tell me what I should do” (F = 4.3; p < 0.05). This item was used to assess preference for autonomy-supportive versus more directive communication. To elucidate this interaction effect, after examining the pattern of responses, we divided the sample into “low” (score >5; n = 242) and ‘high” (score < = 5; n = 181) on the seven-point disagree–agree scale. Higher scores indicated higher agreement, while lower scores (stronger disagreement) indicated greater preference for autonomy support. As shown in Fig. 2a, high autonomy support individuals in the experimental intervention increased their F & V intake by 1.07 servings compared to 0.43 servings among high autonomy support controls (p = 0.14). Conversely, low autonomy support experimental and control participants showed almost identical changes in F & V at 0.60 and 0.64 servings, respectively (p = 0.86). For every subgroup other than low autonomy controls, within-group change in F & V intake based on the composite measure was significant (p < 0.05).

a Interaction of F & V change* with autonomy preference. b Interaction of F & V change* with age. *Difference of 3 month minus baseline values
There was also a significant interaction of intervention with age (F = 4.8; p < 0.05; see Fig. 2b). To elucidate this pattern, we divided age into terciles. Among participants in the lower tercile (ages 22–43), there was a larger change in F & V intake (0.59 servings) in controls compared to their experimental group counterparts (0.29 servings), although this difference was not significant (p = 0.29). Conversely, among those in the upper tercile (ages 54–69), experimental group participants showed a larger change in F & V intake (1.09 servings) than controls (0.48 servings). This difference approached statistical significance (p = 0.07). There was no difference in F & V change by study group amongst those in the middle tercile of age. For all groups except younger experimentals, the within-group changes in F & V intake based on the composite measure were significant (p < 0.05).
There was a borderline significant interaction of intervention with study site (F = 3.4; p = 0.06). Participants from the Detroit health care system showed slightly larger F & V change (p = 0.43) in the control than the experimental group, whereas in the Atlanta health care system, a larger (p = 0.11) change was observed in the experimental group. For both sites, the within-group change in F & V intake based on the composite measure was significant (p < 0.05; data not shown).
With regard to psychosocial outcomes, as shown in Table 5, significant within-group changes for both the control and experimental conditions were observed for intention to eat fruit, intention to eat vegetables, outcome expectancies, and intrinsic motivation. No between-group differences were observed for any of these measures, and none of the treatment by age or treatment by autonomy support preference interaction terms were significant.
Process Measures
As shown in Table 6, perceived relevance of the intervention was borderline (p = 0.058) greater in the experimental than the control group, 5.75 and 5.50 (out of 8 maximum), respectively. Similar to F & V outcomes, there was also a significant interaction (F = 6.8; p = 0.01) of intervention group and age on perceived relevance. Individuals in the upper tercile for age showed a significantly (p < 0.05) higher level of perceived relevance, 6.88, than their control counterparts, 5.36 (data not shown).
There was also a marginally significant interaction of intervention group and autonomy support preference (F = 2.8; p = .09) on perceived relevance. Similar to what was observed for the F & V analyses, high autonomous individuals in the experimental group reported significantly (p = 0.02) higher levels of perceived relevance, 6.0, than their control counterparts, 5.4 (data not shown).
There were no between-group differences in either health plan satisfaction or overall program satisfaction (Table 6). However, health plan satisfaction, which was measured at baseline and follow-up, increased significantly (p < 0.01) in both groups (not indicated in Table).
As a manipulation check, participants were queried as to whether they recalled seeing various topics or sections in their newsletters (Table 6). Some items were contained in only the experimental newsletters, whereas others were contained in both the experimental and control interventions or neither (distracters). Individuals in the experimental group were more likely to recall seeing content related to religious themes (p < 0.001), motivational quotes (p < 0.001), personal values and goals (p = 0.19), and measuring heart rate (p = 0.06). With the exception of the latter, this content was only addressed in the experimental intervention. Conversely, there were no group differences in the percent reporting seeing content related to health effects of F & V, serving size information, importance of eating F & V, exercise, and setting goals, which were all addressed in both the control and experimental newsletters. The between-group difference for recalling content related to measuring heart rate, which was listed as a distracter item, was unanticipated, as this topic was not addressed in any newsletters.
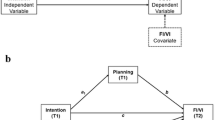
Mediation Analyses
A mediation model based on the Barron and Kenny method [52] was fit to examine the marginally higher level of perceived relevance in the experimental group. Mediators included in the model were those items recalled more frequently in the experimental versus the control group. When recall of content related to religious themes, personal values, motivational quotes, and measuring heart rate were entered into the regression equation, the significance level of the between-group differences in perceived relevance increased from 0.06 to 0.71, indicating that perceived relevance was mediated by recall of this content (data not shown).
Exploratory Analyses
To elucidate why there were differential responses to the two interventions based on autonomy support preference, we examined correlations between change in autonomous and controlled motivation with change in fruit and vegetable intake by response to the preference for autonomy support item. There was a positive correlation between change in autonomous motivation and change in fruit and vegetable intake for participants who scored below 5 on the seven-point scale (r = 0.18; P = 0.10) and only a negligible correlation (r = 0.01; P = 0.85) between change in controlled motivation and change in F & V intake. Conversely, for participants who scored 5 or higher (i.e., they agreed with the item), there was a small positive (non-significant) correlation between change in extrinsic motivation (r = 0.09; P = 0.10) and only a negligible correlation (r = −0.03; P = 0.66) between change in autonomous motivation and change in F & V intake. Thus, for individuals who preferred a more autonomy-supportive style, change in autonomous motivation was related to their change in F & V intake, which was not the case for those preferring a more directive style. We also examined demographic characteristics of those in the group preferring high autonomy support. They had higher income and educational attainment than those preferring more directive advice.
Discussion
This study was designed to test whether tailoring a fruit and vegetable print intervention on some novel psychological constructs would enhance program impact beyond that of more traditional social cognitive tailoring. Considering all participants, there was no evidence that tailoring on these newer constructs impacted F & V intake or the associated psychosocial mediators above that of standard tailoring.
However, there were two significant treatment moderators on F & V outcomes: age and preference for autonomy support. Preference for autonomy support was assessed at baseline with a single, experimental item: “In general, when it comes to my health I would rather an expert just tell me what I should do”. We hypothesized that (1) individuals who were more likely to agree with this statement would respond more strongly to the control intervention which was written in a more directive tone, and (2) individuals who disagreed with the item would be more responsive to the experimental intervention, which was written in a more autonomy-supportive tone. The results supported the second of these hypotheses.
Further work developing measures that discriminate what type of motivational tone/style an individual may prefer and/or respond to appears warranted. In particular, measures are needed that directly tap preference for specific types of interventions (e.g., interpersonal, print, web, etc.) and different types of directive and autonomy-supportive content. Our measure, based on a single item, only queried general preference for style of health communication. How our measure correlates to other constructs such as health locus of control, decision-making style, and perceived competence also merits examination. Despite the need for more sophisticated measures of this predisposition, these findings nonetheless suggest that a simple measure of “motivational preference” may be helpful in tailoring health communications to individual needs and preferences.
Interestingly, we found that most of our sample preferred a more directive style of communication, with 57% responding 6 or higher on the seven-point disagree–agree continuum. It is possible that this rate may be related to the ethnicity of our sample, as African Americans may respond more to an extrinsic motivation approach than other groups [46, 51, 53]. Further research is needed to evaluate the style preferences in other populations, as other groups may prefer the autonomy-supportive content/tone.
With regard to the moderating effect of age, older participants responded more favorably to the experimental intervention. This finding was not anticipated, and we could find no prior studies where age similarly moderated the relationship with self-determination variables. Age and the preference for directive advice were actually positively correlated, r = 0.12, with older participants more likely to prefer directive communication. This suggests that the reason the intervention may have worked more favorably with older participants may not have been due to the autonomy supportive nature of the experimental intervention.
Despite a general lack of overall group difference in primary or secondary outcomes, participants in the experimental group did report marginally higher levels of perceived relevance and were generally more likely to recall content that was exclusively contained in the experimental newsletters. These manipulation checks suggest that the intended content and tone differences were attended to by the users. Moreover, recall of experimental content appeared to mediate the intervention effect on perceived relevance, suggesting that inclusion of such content may have enhanced message processing.
Although no between-group differences were observed, both study groups reported significant improvements in satisfaction with their health care provider. This may be an important finding for health care delivery systems considering implementing tailored intervention systems. How much tailoring and what type of tailoring is needed to impact client satisfaction merits additional research. Even modest amounts of tailoring may be sufficient to create positive consumer response.
The study has limitations. First, the primary outcome of fruit and vegetable intake was based on self-report. Prior versions of the instruments used here have been validated against 24-h recalls and serum carotenoids amongst African Americans [48, 53]. Nonetheless, differential social desirability bias on the part of individuals in the experimental group cannot be entirely ruled out and remains a potential alternative interpretation for our findings. The sample was entirely African American and medically insured, so there may be limited generalizability to other ethnic groups and those with lower socioeconomic status. Finally, although significant interaction effects of a priori moderators were observed, the study was only powered to detect between-group differences in the primary outcome. Thus, some of the interaction effects that were only marginally significant would have been more so if with a larger sample.
Despite these limitations, our findings suggest that tailoring on values and other constructs drawn from SDT and MI can, at least for those who prefer an autonomy-supportive style of communication, enhance message impact and perceived relevance. Our study also confirms the importance of tailoring on a range of potential motivators and the need to consider individual differences in designing health communications.
References
Campbell MK, Bernhardt JM, Waldmiller M, et al. Varying the message source in computer-tailored nutrition education. Patient Educ Couns. 1999; 36: 157–169.
Campbell MK, DeVellis BM, Strecher VJ, et al. Improving dietary behavior: The effectiveness of tailored messages in primary care settings. Am J Public Health. 1994; 845: 783–787.
Rimer BK, Orleans CT, Cristinzio S, et al. Does tailoring matter? The impact of a tailored guide on ratings and short-term smoking related outcomes for older smokers. Health Educ Res. 1994; 9: 69–84.
Strecher VJ, Kreuter M, Den Boer DJ, et al. The effects of computer-tailored smoking cessation messages in family practice settings. J Fam Pract. 1994; 393: 262–270.
Kreuter MW, Strecher VJ. Do tailored behavior change messages enhance the effectiveness of health risk appraisal? Results from a randomized trial. Health Educ Res. 1996; 111: 97–105.
Brug J, Glanz K, Van Assema P, et al. The impact of computer-tailored feedback and iterative feedback on fat, fruit, and vegetable intake. Health Educ Behav. 1998; 254: 517–531.
Dijkstra A, De Vries H, Roijackers J. Long-term effectiveness of computer-generated tailored feedback in smoking cessation. Health Educ Res. 1998; 132: 207–214.
Brug J, Steenhuis I, van Assema P, et al. Computer-tailored nutrition education: Differences between two interventions. Health Educ Res. 1999; 142: 249–256.
de Vries H, Brug J. Computer-tailored interventions motivating people to adopt health promoting behaviours: Introduction to a new approach. Patient Educ Couns. 1999; 362: 99–105.
Lipkus IM, Lyna PR, Rimer BK. Using tailored interventions to enhance smoking cessation among African-Americans at a community health center. Nicotine Tob Res. 1999; 11: 77–85.
Strecher VJ. Computer-tailored smoking cessation materials: A review and discussion. Patient Educ Couns. 1999; 36: 107–117.
Campbell MK, Motsinger BM, Ingram A, et al. The North Carolina Black Churches United for Better Health Project: Intervention and process evaluation. Health Educ Behav. 2000; 272: 241–253.
Bernhardt J. Tailoring messages and design in a Web-based skin cancer prevention intervention. Int Electron J Health Educ. 2001; 4: 290–297.
Kreuter MW, Sugg-Skinner C, Holt CL, et al. Cultural tailoring for mammography and fruit and vegetable intake among low-income African-American women in urban public health centers. Prev Med. 2005; 411: 53–62.
Brug J, Oenema A, Campbell MK. Past, present, and future of computer-tailored nutrition education. Am J Clin Nutr. 2003; 774 Suppl: 1028S–1034S.
Kroeze W, Werkman A, Brug J. A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Ann Behav Med. 2006; 313: 205–223.
Marcus BH, Napolitano MA, King AC, et al. Telephone versus print delivery of an individualized motivationally tailored physical activity intervention: Project STRIDE. Health Psychol. 2007; 264: 401–409.
Kreuter MW, Strecher VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Ann Behav Med. 1999; 214: 276–283.
Kreuter MW, Wray RJ. Tailored and targeted health communication: Strategies for enhancing information relevance. Am J Health Behav. 2003; 27 Suppl 3: S227–S232.
Brug J, Campbell M, van Assema P. The application and impact of computer-generated personalized nutrition education: A review of the literature. Patient Educ Couns. 1999; 36: 145–156.
Smeets T, Kremers SPJ, de Vries H, Brug J. Effects of tailored feedback on multiple health behaviors. Ann Behav Med. 2007; 332: 117–123.
Oenema A, Tan F, Brug J. Short-term efficacy of a web-based computer tailored nutrition intervention: Main effects and mediators. Ann Behav Med. 2005; 291: 54–63.
Haerens L, Deforche B, Maes L, et al. Evaluation of a 2-year physical activity and healthy eating intervention in middle school children. Health Educ Res. 2006; 216: 911–921.
Strolla LO, Gans KM, Risica PM. Using qualitative and quantitative formative research to develop tailored nutrition intervention materials for a diverse low-income audience. Health Educ Res. 2005; 214: 465–476.
Dijkstra A, De Vries H, Roijackers J. Targeting smokers with low readiness to change with tailored and nontailored self-help materials. Prev Med. 1999; 282: 203–211.
Rakowski W, Ehrich B, Goldstein MG, et al. Increasing mammography among women aged 40–74 by use of a stage-matched, tailored intervention. Prev Med. 1998; 275 Pt 1: 748–756.
Ershoff DH, Quinn VP, Boyd NR, et al. The Kaiser Permanente Prenatal Smoking Cessation Trial: When more isn’t better, what is enough? Am J Prev Med. 1999; 173: 161–168.
Brug J, van Assema P. Differences in use and impact of computer-tailored dietary fat-feedback according to stage of change and education. Appetite. 2000; 343: 285–293.
van Sluijs EM, van Poppel MN, Twisk JW, et al. Effect of a tailored physical activity intervention delivered in general practice settings: Results of a randomized controlled trial. Am J Public Health. 2005; 9510: 1825–1831.
Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol Bull. 2007; 1334: 673–693.
Shegog R, McAlister AL, Hu S, Ford KC, Meshack AF, Peters RJ. Use of interactive health communication to affect smoking intentions in middle school students: a pilot test of the “Headbutt” risk assessment program. Am J Health Promot. 2005; 195: 334–338.
Williams GC, Rodin GC, Ryan RM, et al. Autonomous regulation and long-term medication adherence in adult outpatients. Health Psychol. 1998; 173: 269–276.
Williams GC, Gagne M, Ryan RM, Deci EL. Facilitating autonomous motivation for smoking cessation. Health Psychol. 2002; 211: 40–50.
Markland D, Ryan RM, Tobin VJ, Rollnick S. Motivational interviewing and self-determination theory. J Soc Clin Psychol. 2005; 246: 811–831.
Deci E, Ryan R. Intrinsic Motivation and Self-Determination in Human Behavior. New York: Plenum; 1985.
Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000; 551: 68–78.
Williams GC, Freedman ZR, Deci EL. Supporting autonomy to motivate patients with diabetes for glucose control. Diabetes Care. 1998; 2110: 1644–1651.
National Center for Health Statistics, Health, United States, 2006 With Chartbook on Trends in the Health of Americans. Hyattsville, Maryland: National Center for Health Statistics; 2006.
Serdula MK, Gillespie C, Kettel-Khan L, et al. Trends in fruit and vegetable consumption among adults in the United States: Behavioral risk factor surveillance system, 1994–2000. Am J Public Health. 2004; 946: 1014–1018.
Kant A, Graubard B, Kumanyika S. Trends in black–white differentials in dietary intakes of U.S. adults, 1971–2002. Am J Prev Med. 2007; 324: 264–272.
Resnicow K, DiIorio C, Soet JE, et al. Motivational interviewing in health promotion: It sounds like something is changing. Health Psychol. 2002; 215: 444–451.
Resnicow K, Davis R, Rollnick S. Motivational interviewing for pediatric obesity: Conceptual issues and evidence review. J Am Diet Assoc. 2006; 10612: 2024–2033.
Williams GC, Deci EL. Activating patients for smoking cessation through physician autonomy support. Med Care. 2001; 398: 813–823.
Cacioppo JT, Petty RE, Feinstein JA, Jarvis WBG. Dispositional differences in cognitive motivation: The life and times of individuals varying in need for cognition. Psychol Bull. 1996; 1192: 197–253.
Deci E, Ryan R. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol Inq. 2000; 11: 227–268.
Fuemmeler BF, Masse LC, Yaroch AL, et al. Psychosocial mediation of fruit and vegetable consumption in the Body and Soul Effectiveness Trial. Health Psychol. 2006; 254: 474–483.
Thompson FE, Subar AF, Smith AF, et al. Fruit and vegetable assessment: performance of 2 new short instruments and a food frequency questionnaire. J Am Diet Assoc. 2002; 10212: 1764–1772.
Resnicow K, Odom E, Wang T, et al. Validation of three food frequency questionnaires and twenty four hour recalls with serum carotenoids in a sample of African American adults. Am J Epidemiol. 2000; 152: 1072–1080.
Resnicow K, Coleman-Wallace D, Jackson A, et al. Dietary Change through Black Churches: Baseline results and program description of the eat for life trial. J Cancer Educ. 2000; 15: 156–163.
Resnicow K, Jackson A, Braithwaite R, et al. Healthy body/healthy spirit: Design and evaluation of a church-based nutrition and physical activity intervention using motivational interviewing. Health Educ Res. 2002; 172: 562–573.
Resnicow K, Campbell MK, Carr C, et al. Body and soul. A dietary intervention conducted through African-American churches. Am J Prev Med. 2004; 272: 97–105.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986; 516: 1173–1182.
Resnicow K, Jackson A, Blissett D, et al. Results of the healthy body healthy spirit trial. Health Psychol. 2005; 244: 339–348.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Resnicow, K., Davis, R.E., Zhang, G. et al. Tailoring a Fruit and Vegetable Intervention on Novel Motivational Constructs: Results of a Randomized Study. ann. behav. med. 35, 159–169 (2008). https://doi.org/10.1007/s12160-008-9028-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-008-9028-9