
Abstract
Although non-suicidal self-injury (NSSI) is a worldwide public health concern, the prevalence rate and risk factors for it among Chinese university students are not known. The present study aimed to address these knowledge gaps and examine the interrelationship between child abuse and NSSI frequency and functions as well as psychiatric co-morbidity with emotion dysregulation as a mediator and attachment style as a moderator. Five hundred and thirty-six (F = 359, M = 177) Chinese university students were recruited from two universities in Hong Kong and completed the Functional Assessment of Self-Mutilation, Childhood Trauma Questionnaire, Revised Adult Attachment Scale, Difficulties in Emotion Regulation Scale and General Health Questionnaire–28. The findings showed that the prevalent rate of NSSI was 22% in the past year. The results showed that child abuse was significantly correlated with psychiatric co-morbidity and emotion dysregulation, and the latter was also significantly correlated with positive and negative reinforcement, and psychiatric co-morbidity. Moderation effects were not established. Non-suicidal self-injurious behaviour was relatively common among Chinese university students in Hong Kong. Their difficulties in regulating their emotions may influence why they hurt themselves and the severity of psychological distress, especially for those who experienced a high level of child abuse in the past.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-suicidal self-injury (NSSI) is a worldwide public health issue with the prevalence rates ranging from 13% to 15% among Chinese adolescents in Hong Kong (Cheung et al., 2013; You et al., 2011). However, the rates for Chinese university students are not known. NSSI refers to direct, deliberate harm to the body without suicidal intent but outside of social acceptance (Baiden et al., 2017). NSSI behaviours include cutting, burning, scratching, skin-piercing, pulling-hair or plucking, self-hitting, biting, bruising, banging and punching, all of which serve different functions. Increasingly, research has been emphasizing the importance of examining NSSI functions since they inform us of what motivates or reinforces NSSI behaviour (Klonsky, 2007). Such information provides important implications for understanding NSSI, designing treatments, and predicting prognosis and suicidal risk.
The functions of NSSI have been classified into two domains: positive/negative automatic and positive/negative social reinforcement. Automatic positive reinforcement aims to increase individual’s emotional or physiological desired states such as relaxation or feeling something, even if the NSSI behaviour is painful. Automatic negative reinforcement serves to decrease aversive affective or physiological states in ways such as blocking negative feelings or relieving feelings of numbness or emptiness. Social positive reinforcement refers to increasing social support such as getting attention or gaining control in a social situation. Social negative reinforcement aims to remove social demands such as attending school or interacting with people (Nock & Prinstein, 2004).
There is a paucity of research examining the risk factors associated with NSSI among Chinese university students. For the current study, child abuse has been postulated as one possible factor since it has been shown to play an important role in predicting NSSI (D'Andrea et al., 2012), along with psychiatric outcomes such as depression and anxiety among non-university samples (Huh et al., 2017). Child abuse refers to early onset, chronic and sustained traumatic experiences involving emotional or physical neglect as well as physical, emotional or sexual abuse (Briere & Gil, 1998). Sexual and emotional abuse in childhood is associated with NSSI (Isohookana et al., 2016; Thomassin et al., 2016). Individuals engaging in NSSI are also reported to have a history of childhood neglect and separation (Johnstone et al., 2016). This link between child abuse and NSSI is not surprising given that prolonged and early trauma has profound adverse consequences on self-perception, which is possibly manifested in the form of self-injury (Colleen & Komal, 2011).
The link between child abuse and NSSI can be influenced by emotion dysregulation (Tresno et al., 2013). According to the self-trauma model (Briere, 2002), child abuse survivors often display high levels of negative affect, urgency (Powers et al., 2014), affective instability, and emotional sensitivity in reacting to challenges. They have altered their capacity to inhibit strong affects and dysphoric states and have adopted maladaptive emotion regulation strategies. Traumatized individuals who engage in NSSI tend to have difficulties in accepting and identifying emotions, controlling impulses, engaging in goal-directed behaviours, maintaining high levels of emotional clarity and awareness (Bresin, 2013), as well as using maladaptive emotion regulation strategies (Navarro-Haro et al., 2015). Endorsing these strategies is a risk factor for psychiatric co-morbid symptoms such as depression and anxiety (Lee et al., 2015).
What has been articulated amounts to a hypothesized mediational model depicting how child abuse might impact distress outcomes characterized by NSSI frequency or functions, and psychiatric co-morbidity through emotion dysregulation as a mediator. To the best of our knowledge, this model has not been examined among Chinese university students. In doing so, however, the role of attachment experience cannot be ignored. Attachment has been shown to influence the effects of child abuse and emotion dysregulation, which could in turn affect the severity of NSSI and psychiatric co-morbidity. Attachment experience can influence personality development, intrapsychic structure and inter-relationship with others. Our internal working model, or, more precisely: internal representations of self and others, act as a mirror reflecting the quality of early attachment experiences (Bowlby, 1982). Child abuse was positively associated with fearful, preoccupied and dismissing behaviours, but negatively associated with secure attachment styles (Erozkan, 2016). Specifically, physical child abuse was associated with fearful and preoccupied attachment styles (Unger & De Luca, 2014). Child physical neglect was strongly related to avoidant and anxious attachment styles (Mickelson et al., 1997).
Attachment styles can also relate to negative emotion regulation processes (Cabral et al., 2012) and the endorsement of emotion regulation strategies (Pascuzzo et al., 2013). For example, preoccupied and avoidant individuals tend to employ emotion-focused strategies such as distancing (Yates, 2004). On the other hand, secure individuals tend to process feelings, whilst insecure ones tend to deny negative emotional experiences (Mikulincer & Shaver, 2019). Attachment experience is also associated with the emergence of NSSI among college students (Kharsati & Bhola, 2016; Kokaliari, 2014). Given the potential influence of attachment on child abuse and emotion dysregulation, attachment needs to be taken into account as a possible moderator for the hypothesized model.
The current study aimed to examine 1) the prevalence rate for NSSI among Chinese university students, and 2) the hypothesized model depicting the interrelationship between child abuse, NSSI frequency or functions, and psychiatric co-morbidity with emotion dysregulation as a mediator and attachment experience as a moderator (see Fig. 1). Guided by literature, the hypotheses were as follows:
-
1.
The prevalence rate for NSSI would be compatible to that for Hong Kong Chinese adolescents between 13% and 15%.
-
2.
After controlling for the moderating effect of attachment, emotion dysregulation would mediate the impact of child abuse onto distress outcomes (NSSI frequency or functions and psychiatric co-morbidity).

The hypothesized model
Method
Participants and Procedures
This study was cross-sectional in design with participants recruited from one public university and one private university in Hong Kong. The researcher (first author) sent email invitations to lecturers from two faculties asking whether she could approach their students for the research. Upon approval, the researcher went to classrooms and lecture theatres to introduce the objectives of the study, explain the procedures, importance of confidentiality, and participants’ termination right. All students completed the consent form prior to the completion of questionnaires, the validated Chinese versions of which were adopted from literature (see the measures section below). Inclusion criteria were 1) aged 18+, 2) Chinese in ethnicity and 3) university students from Hong Kong or Mainland China. Exclusion criteria were 1) below 18, 2) non-students, 3) foreign or overseas students, 4) suicidal intent and 5) no consent given. In total, 540 students completed questionnaires with 4 of them excluded for not meeting the inclusion criteria, thus resulting in 536 retained for analysis.
Measures
Demographic Information
Participants were asked to provide demographic information of age, gender (1 = Female; 2 = Male), marital status (1 = Single; 2 = Married; 3 = Widower; 4 = Widow), academic year, study mode (1 = Full-time; 2 = Part-time) and student type (1 = Hong Kong; 2 = Mainland China).
Functional Assessment of Self-Mutilation (FASM) aims to examine NSSI methods, frequency and functions. It is widely used in both normative and psychiatric samples. It asks respondents to indicate the frequency of using eleven non-suicidal self-injurious behaviours: self-cutting, hitting, burning skin, biting, scratching, inserting objects on nails or skin, picking at a wound, pulling hair out and erasing skin over the past year. Since banging of the head is a common NSSI method (Jianing et al., 2015), it was added to the list of NSSI methods. The respondents’ suicidal intention, physical pain level and onset of NSSI were also measured. In addition to NSSI prevalence and methods, respondents were also asked to indicate NSSI purposes in twenty-two items on a four-point Likert scale ranging from 0 to 3 (0 = Never, 1 = Rarely, 2 = Some, 3 = Often). The purposes were grouped into four NSSI functions: automatic positive reinforcement, automatic negative reinforcement, social positive reinforcement and social negative reinforcement (Nock & Prinstein, 2004). The Chinese version of FASM has been validated (Cronbach’s alpha total = 0.94) (Leong et al., 2014). The Cronbach’s alpha total score of 0.87 was obtained from the current sample.
Childhood Trauma Questionnaire (CTQ-SF) is a standardized 28-item self-report inventory used as a screening tool for a history of child abuse and neglect. It consists of five subscales to measure the severity of five different types of childhood maltreatment, which are emotional abuse, sexual abuse, physical abuse, emotional neglect and physical neglect. It asks participants to indicate their childhood traumatic experiences on a 5-point Likert scale ranging from 1 = Never True to 5 = Very Often True. There are three additional items of Minimization-Denial to check whether respondents have extreme response bias. Respondents with high scores indicate they have experienced elevated child abuse. CTQ-SF is appropriate for use in a community sample. The Chinese version of CTQ-SF is a valid and reliable psychometric instrument for evaluation of Chinese childhood abuse (Cronbach’s alpha = 0.79) (He et al., 2019). Based on the current sample, the Cronbach’s alpha for the total score was 0.89.
Revised Adult Attachment Scale (RAAS) is an 18-item inventory measuring adults’ anxious and avoidant attachment styles. The measure asks participants to rate their feelings and behaviours towards close relationships on a 5- point Likert scale (1 = not at all a characteristic of myself to 5 = a definite characteristic of myself). There are 6 items for anxious attachment and 12 items for avoidant attachment. Anxious individuals tend to have a strong desire for intimacy and fear of abandonment. Avoidant individuals fear intimacy and are uncomfortable with closeness as well as less dependent on others. Cronbach’s alpha for the total score based on a non-clinical Chinese group is over 0.70 (Wu et al., 2004). From our sample, the Cronbach’s alpha for the total score was 0.91.
Difficulties in Emotion Regulation Scale (DERS) consists of 36 items measuring emotion dysregulation in six dimensions: the lack of emotional awareness, the lack of emotional clarity, difficulties controlling impulsive behaviours when in distress, difficulties engaging in goal-directed behaviours, non-acceptance of negative emotional responses and limited access to emotion regulation strategies. It asks participants to rate individual items using a 5-point Likert scale ranging from 1 = almost never to 5 = almost always. High scores indicate increased emotion regulation difficulties. The Chinese version of this scale (Cronbach’s alpha total score = 0.9) has been validated (Li et al., 2018). For the current sample, the Cronbach’s alpha was 0.93.
General Health Questionnaire–28 (GHQ 28) is a screening tool to detect whether participants are likely to have general psychiatric disorders. It consists of four subscales: somatic symptoms, anxiety with insomnia, social dysfunction and severe depression. It asks participants to select the appropriate response out of four options: 0 = Not at all, 1 = no more than usual, 2 = more than usual, 3 = much more than usual. The reliability of the questionnaire has been examined with Cronbach’s alpha ranging from 0.78 to 0.95 (Goldberg & Bridges, 1987). From our current sample, the Cronbach’s alpha for the total score was 0.92.
Statistical Analysis
Descriptive statistics were used to describe means and standard deviations for demographic variables. T and chi-square tests were used to compare the differences between NSSI and non-NSSI groups in terms of demographic variables, child abuse traumas, psychiatric co-morbidity, emotional dysregulation, as well as attachment. Correlation coefficients were performed to establish whether demographic variables were associated with distress outcomes. The hypothesized model was examined using path analysis. Full information maximum likelihood was used to examine the estimation of model parameters and fit statistics. The following criteria would be indicative of a good fit for the data: (1) a ratio of chi-square/d.f. under 3, (2) 0.95 or greater for the Tucker–Lewis Index (TLI), and (3) Incremental Fit Index (IFI), (4) 0.06 or smaller for the root mean square error of approximation (RMSEA), (5) a value closer to 1 for the Comparative Fit Index (CFI), and (6) Normal Fit Index (NFI) and (7) the Goodness of Fit Index (GFI) ≥ 0.95 was not recommended.
The assumptions and diagnostics related to the path analysis were checked. The maximum likelihood fitting criterion used and the resultant statistics assume that the distribution of the indicative variables are multi-variate normal. We checked normality and found no variables needed for transformation. No outliers were detected during the exploration of diagnostics (Mahalanobis distance = 3 SD). Assumptions relating to linearity and homoscedasticity were met. Regression imputation was used to address missing data.
PROCESS, is an alternative to the causal steps approach (Baron & Kenny, 1986), and is used to examine mediational effects. Bias-corrected bootstrapping is used in PROCESS to generate confidence intervals, which addresses the problem of power resulting from the asymmetric and non-normal sampling distributions of an indirect effect (MacKinnon et al., 2004). In this study, the bootstrapping sampling (N = 1000) distributions of the indirect effects were produced by selecting a sample of cases from the complete data set and calculating the indirect effects in the resamples. The indirect effects were estimated based on point estimates and confidence intervals (95%). When the confidence interval did not contain zero, point estimates of indirect effects were considered significant. An Expectation Maximization (EM) algorithm (Enders, 2011) was used to replace missing data. Regression imputation is considered a valid method in dealing with missing data (Schafer & Graham, 2002) when omitted questionnaire items total less than 5%. For the current study, 1% of responses were missing.
Results
Sample Demographic Information
Of 536 participants, 359 (67%) were female and 177 (33%) were male with a mean age of 20.42 (SD = 2.29, range: 18–51). Almost all (99%) were full-time students from Hong Kong and single; 62% were in academic years 1 and 2 followed by years 3 (18%) and 4 (20%).
NSSI vs Non-NSSI Groups
Using the FASM, students were allocated into NSSI and non-NSSI groups based on whether they had engaged in at least one NSSI in the past year; 118 students (22%) were identified as NSSI injurers; the rest were not (n = 418, 78%). There were no significant differences between groups in demographic variables (See Table 1). However, NSSI injurers reported significantly higher levels of child abuse, emotion dysregulation, anxious attachment and psychiatric co-morbidity compared to non-NSSI injurers (See Table 1).
NSSI Characteristics
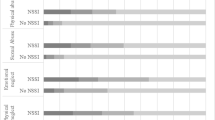
A large proportion (69%) engaged in NSSI impulsively; 62% reported a mild level of physical pain (62%) from doing NSSI, whilst 3%, 16% and 19% reported a severe, moderate and zero pain respectively. A large proportion (71%) started engaging in NSSI just prior to or during adolescence (10–17 years old); 5% had their first NSSI episode during childhood (≤ 9 years old) and 10% during young adulthood (≥ 18 years old); 14% did not report the onset of NSSI. The mean age of onset was 14.72 years old (SD = 3.71). In terms of NSSI frequency and methods, during the year before the study began, a large group of non-suicidal self-injurers (68%) engaged in 5 or above NSSI incidents, whilst the rest 4 or less. 40% of non-suicidal self-injurers engaged in one NSSI method, 53% in two, and the rest 3 or more. Biting was the most prevalent NSSI method (54%), followed by hitting (36%) and scratching (30%). Burning was the least-endorsed NSSI method (1%). In terms of NSSI purposes, the three most-commonly reported came under automatic positive reinforcement (See Table 2). For example, just over half of non-suicidal self-injurers reported the reason as relaxation. Less than half reported a desire to feel pain and participating in self-punishment as reasons. Approximately 40% engaged in NSSI either to decrease bad feelings or relieve numbness or emptiness. There were also reasons such as seeking social positive and negative reinforcements. For example, some NSSI injurers were motivated by avoidance such as avoiding school, work, doing something unwanted, or avoiding people. A quarter engaged in NSSI because of trying to over-control a situation.
Path Analysis
Before the path analysis, correlation coefficients (point bi-serial correlation included) with Bonferroni correction (p < 0.01) were carried out to examine whether demographic variables (gender, age and academic years) were related to outcome variables (NSSI frequency or purposes and psychiatric co-morbidity). Full or part time student status, student type and marital status were not taken into account because almost all were full time Hong Kong students and single. The results showed that gender and age were not significantly correlated with both outcomes (r values ranged from 0.08 to 0.19). No background variables were therefore controlled for in the analysis.
The model was fit with an allowance for child abuse to correlate with emotion dysregulation, NSSI frequency or functions and psychiatric co-morbidity. Emotion dysregulation difficulty was also allowed to correlate with the three outcomes. Two product variables were created, (z scores of attachment total x child abuse total; z scores of attachment total x emotion dysregulation total) which were allowed to be correlated with outcomes. The results revealed a good fit [CMIN/DF = 1.21; TLI = 0.97; IFI = 0.99; RMSEA = 0.04, 90% CI = 0.00–0.25; CFI = 0.99; NFI = 0.99; GFI = 0.95] with child abuse being significantly correlated with psychiatric co-morbidity and emotion dysregulation, and this was significantly correlated with positive reinforcement, negative reinforcement and psychiatric co-morbidity. No moderation effects were established in that the two product variables were not correlated with outcomes. These results implied that emotion dysregulation could have mediated the impact that child abuse had on NSSI purposes and psychiatric co-morbidity. Mediational analysis confirmed these results (see Table 3 & Fig. 2).

The final model showing significant paths (in bold) at 5% or better
Discussion
The present study examined the prevalence rate for NSSI among Chinese university students in Hong Kong, and the interrelationship between child abuse, emotion dysregulation, NSSI frequency or function and psychiatric co-morbidity with attachment as a moderator. The results showed that approximately 22% of university students reported having engaged in NSSI in the past year. Child abuse was significantly correlated with psychiatric co-morbidity and emotion dysregulation, which was also significantly correlated with positive and negative reinforcement, as well as psychiatric co-morbidity. No moderation effects were found.
The prevalence rate for NSSI in the present study was lower than those reported based on other Eastern samples from India (38%) and Indonesia (31%) (Kharsati & Bhola, 2016; Tresno et al., 2012). However, it was higher than those in Japan, and Western countries ranging between 9% and 15% (Paul et al., 2014; Tresno et al., 2013). Contrary to our hypothesis, it was higher than what was reported among adolescents in Hong Kong ranging between 13% and 15% (Cheung et al., 2013; You et al., 2011). Different assessments (e.g. Deliberate Self-Harm Inventory, the Counselling Center Assessment for Psychological Symptoms or some self-constructed questionnaires measuring self-harm) used to measure NSSI in different studies could have attributed to this variation in NSSI prevalence.
Surprisingly, contrary to our hypothesis and the wealth of literature mentioned in the introduction (e.g. Colleen & Komal, 2011; Thomassin et al., 2016), child abuse was not significantly correlated with NSSI frequency. Even before the path analysis, on a bivariate level, the correlations between the total child abuse, child abuse types and NSSI frequency were weak (r values ranged from 0.01 to 0.08). This suggested that the frequency of hurting themselves was not related to the effects of child abuse but some other factors. Cultural characteristics could play a role in influencing NSSI behaviour (Chesin et al., 2013). Among university students in Hong Kong, academic success plays an important part of the cultural fabric in Hong Kong. It is important for not only their future career, but also their self-worth that they meet familial expectations of academic excellence (Costigan et al., 2010). Failure to do so could result in feelings of inadequacy, self-doubt, and a sense of internalized inferiority (Breen et al., 2013). Previous studies have supported the significant association between inferiority and NSSI (Tan et al., 2015). Furthermore, they might have felt ashamed due to the loss of ‘face’ from unsatisfactory academic performance (Mortenson, 2006). This ‘face’-based emotion is significantly associated with NSSI (Fox et al., 2018).
Turning to the results on the correlations between child abuse, NSSI functions and psychiatric co-morbidity, in line with our hypothesis (on bivariate levels) child abuse was significantly correlated with both positive (r = 0.19, p < 0.05) and negative (r = 0.32, p < 0.001) reinforcement. However, mediational analysis suggested that emotional dysregulation completely mitigated the impact that child abuse had on NSSI functions. It also partially mitigated the impact child abuse had on psychiatric co-morbidity, which substantiated previous findings (Crow et al., 2014; Jennissen et al., 2016). Child abuse still had a direct impact on psychiatric co-morbidity. These results could reflect the fact that students with experience of child abuse might be prone to emotion liability-negativity, effectively rendering them sensitive to affective environmental cues (Jungmeen et al., 2013). Consequently, they might experience heightened levels of emotional and physical responses (Van der Kolk et al., 1991) triggered by these difficult environmental situations. At the same time, they have disrupted capacity to identify, recognize and regulate these emotions but experience an urgency to reduce their aversive impact (Arens et al., 2012) by engaging in maladaptive emotion regulation strategies. These strategies were in turn associated with high levels of subjective distress. Such distress seemed to be expressed through not only psychiatric co-morbid symptoms, but also NSSI behaviour with the intention to alleviate distress, feel relaxed by regaining a sense of inner homeostasis and aliveness (Connors, 1996), increasing a somatic or affective state, achieving a sense of relief or control (automatic positive reinforcement) and blocking bad feelings (automatic negative reinforcement).
These results could also be interpreted in terms of the basic tenet of the self-trauma model (Briere, 1992). It argues that child abuse can result in a traumatized schema incompatible with existing schema causing psychological distress (Janoff-Bulman, 2010). A defense mechanism is then triggered to protect the self (Hentschel et al., 2004). Such defense tends to be maladaptive in nature, which aims to regulate distressing emotions by detaching or disconnecting themselves from these emotions (Thomson & Jaque, 2018). In the context of the current studies, these kinds of detachment, disconnection or emotion dysregulatory strategies might be expressed through NSSI, along with psychiatric co-morbid symptoms. In this study, further analysis revealed that emotion dysfunction was correlated with all psychiatric co-morbid symptoms ranging from r = 0.37 to 0.62, p < 0.001 echoing existing literature (Huh et al., 2017).
Somewhat surprisingly, attachment did not interact with child abuse and emotion dysregulation to influence distress outcomes. These results need to be interpreted with caution. They were referring to the impact of interaction terms on outcomes. However, when looking at attachment style in itself, based on bivariate analysis, both anxious and avoidant attachment styles were in fact significantly correlated with positive and negative reinforcement as well as psychiatric co-morbidity ranging from r = 0.26 to 0.48, p < 0.001. In that sense, these results provided further support to research suggesting that attachment, for example: the anxious type, is associated with the emergence of NSSI among university students (Kharsati & Bhola, 2016; Kokaliari, 2014). They echoed the idea that due to the psychopathology of affection bonds originated from childhood trauma (Bowlby, 1977), individuals with child abuse likely adopt negative self-worth and/or negative internal working models which are vulnerable to later NSSI (Yates, 2004).
However, whilst attachment experience could impact NSSI characteristics or psychiatric co-morbidity, such an impact was versatile in that its impact on distress outcomes would depend on the kinds of factors with which it was associated. In other words, even if people share the diathesis for developing some psychological disorders, the manifestation of them would still vary depending on environmental or individual differences such as trauma exposure or trauma type throughout developmental stages (Barlow et al., 2017). Similarly, even if the students in the current study share the diathesis for developing NSSI tendencies along with other psychological symptoms, their manifestation of them would vary depending on other “specific” experiences along with attachment experience developed during their developmental stages. This echoes the connectionist system hypothesis (Mischel & Shoda, 1995) in that individuals (students in this case) differ in how they selectively focus on different features of particular situations or experiences (specific attachment experience, child abuse types, or emotional regulation strategies) throughout their developmental stages. They also categorize and encode them cognitively and emotionally, and how these encodings activate and interact with specific cognitions and affects to specific distress outcomes. In this case, the outcomes were other than NSSI functions and psychiatric co-morbid symptoms.
Limitations of the study need to be acknowledged. Firstly, there might be a sample bias in that students might have taken part in the research thinking that this would be a good opportunity to debrief their trauma-related distress. On the other hand, some might have avoided participation as a part of their avoidance emotional regulation strategy. Secondly, self-reported measures could have increased the likelihood for social desirability affecting the reporting of distress measures (Caputo, 2017). Thirdly, although this study explored mediational effects between psychological constructs, it was based on a cross-sectional design. Comments on causality could not be made due to the lack of temporal precedence (Cole & Maxwell, 2003). A longitudinal study would have been necessary for interpreting causality. Thus, the mediational results of the study should only be interpreted in terms of understanding the structural relationship between the constructs as opposed to causality inference (Holland, 1986). Finally, whilst emotion dysregulation played a major part in the current findings, to what extent Chinese cultural characteristics might influence it was unknown. Research suggests that trauma reactions, psychological symptom presentation, and coping behaviour can vary depending on cultural differences (Jayawickreme et al., 2013). Furthermore, it has been suggested that emotional expression or regulation is restricted to at a degree to which group harmony and status hierarchies are being affected as a result. This might be why in Chinese culture, emotion tended to be experienced in a low frequency, intensity and duration (Bond, 1993).
To conclude, non-suicidal self-injury is a psychological phenomenon, which cannot be ignored among Chinese university students in Hong Kong. Problems with regulating distressing emotions can influence why they hurt themselves and the severity of their psychological distress. This is the case especially for those who were abused as a child.
Data Availability
The authors declare that all data supporting the findings of this study are available within the article.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Arens, A. M., Gaher, R. M., & Simons, J. S. (2012). Child maltreatment and deliberate self-harm among college students: Testing mediation and moderation models for impulsivity. American Journal of Orthopsychiatry, 82(3), 328–337. https://doi.org/10.1111/j.1939-0025.2012.01165.x.
Baiden, P., Stewart, S. L., & Fallon, B. (2017). The role of adverse childhood experiences as determinants of non-suicidal self-injury among children and adolescents referred to community and inpatient mental health settings. Child Abuse & Neglect, 69, 163–176. https://doi.org/10.1016/j.chiabu.2017.04.011.
Barlow, M. R., Goldsmith Turow, R. E., & Gerhart, J. (2017). Trauma appraisals, emotion regulation difficulties, and self-compassion predict posttraumatic stress symptoms following childhood abuse. Child Abuse and Neglect, 65, 37–47. https://doi.org/10.1016/j.chiabu.2017.01.006.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173.
Bond, M. H. (1993). Emotions and their expression in Chinese culture. Journal of Non-verbal Behaviour, 17(4), 245–262.
Bowlby, J. (1977). The making and breaking of affectional bonds. II. Some principles of psychotherapy. The fiftieth Maudsley Lecture. British Journal of Psychiatry, 130(5), 421–431. https://doi.org/10.1192/bjp.130.5.421.
Bowlby, J. (1982). Attachment and loss: Retrospect and Prospect. American Journal of Orthopsychiatry, 52(4), 664–678. https://doi.org/10.1111/j.1939-0025.1982.tb01456.x.
Breen, A. V., Lewis, S. P., & Sutherland, O. (2013). Brief report: Non-suicidal self-injury in the context of self and identity development. Journal of Adult Development, 20(1), 57–62. https://doi.org/10.1007/s10804-013-9156-8.
Bresin, K. (2013). Five indices of emotion regulation in participants with a history of nonsuicidal self-injury: A daily diary study. Behavior Therapy, 45(1), 56–66. https://doi.org/10.1016/j.beth.2013.09.005.
Briere, J. (1992). Methodological issues in the study of sexual abuse effects. Journal of Consulting and Clinical Psychology, 60(2), 196–203. https://doi.org/10.1037//0022-006X.60.2.196.
Briere, J., & Gil, E. (1998). Self-mutilation in clinical and general population samples: Prevalence, correlates, and functions. American Journal of Orthopsychiatry, 68(4), 609–620. https://doi.org/10.1037/h0080369.
Briere, J. (2002). Treating adult survivors of severe childhood abuse and neglect: further development of an integrative model (From The APSAC [American Professional Society on the Abuse of Children] Handbook on Child Maltreatment, P 175–203, 2002, John EB Myers, Lucy Berliner, et al., eds. 19.
Cabral, J., Matos, P. M., Beyers, W., & Soenens, B. (2012). Attachment, emotion regulation and coping in Portuguese emerging adults: A test of a mediation hypothesis. The Spanish Journal of Psychology, 15(3), 1000–1012. https://doi.org/10.5209/rev_SJOP.2012.v15.n3.39391.
Caputo, A. (2017). Social desirability bias in self-reported well-being measures: Evidence from an online survey. Universitas Psychologica, 16(2), 245-255. https://doi.org/10.11144/Javeriana.upsy16-2.sdsw.
Chesin, M. S., Moster, A. N., & Jeglic, E. L. (2013). Non-suicidal self-injury among ethnically and racially diverse emerging adults: Do factors unique to the minority experience matter? Current psychology (New Brunswick, N.J.), 32(4), 318-328. https://doi.org/10.1007/s12144-013-9185-2, 32, 318, 328.
Cheung, Y. T. D., Wong, P. W. C., Lee, A. M., Lam, T. H., Fan, Y. S. S., & Yip, P. S. F. (2013). Non-suicidal self-injury and suicidal behavior: Prevalence, co-occurrence, and correlates of suicide among adolescents in Hong Kong. Social Psychiatry Psychiatric Epidemiology, 48(7), 1133–1144. https://doi.org/10.1007/s00127-012-0640-4.
Cole, D. A., & Maxwell, S. E. (2003). Testing Mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology, 112(4), 558–577. https://doi.org/10.1037/0021-843X.112.4.558.
Colleen, M. L., & Komal, S. P. (2011). The relation between childhood maltreatment and self-injury: A review of the literature on conceptualization and intervention. Trauma Violence & Abuse, 12(1), 23–37. https://doi.org/10.1177/1524838010386975.
Connors, R. (1996). Self-injury in trauma survivors: 1. Functions and meanings. American Journal of Orthopsychiatry, 66(2), 197–206. https://doi.org/10.1037/h0080171.
Costigan, C. L., Hua, J. M., & Su, T. F. (2010). Living up to expectations: The strengths and challenges experienced by Chinese Canadian students. Canadian Journal of School Psychology, 25(3), 223–245. https://doi.org/10.1177/0829573510368941.
Crow, T., Cross, D., Powers, A., & Bradley, B. (2014). Emotion dysregulation as a mediator between childhood emotional abuse and current depression in a low-income African-American sample. Child Abuse & Neglect, 38(10), 1590–1598. https://doi.org/10.1016/j.chiabu.2014.05.015.
D'Andrea, W., Ford, J., Stolbach, B., Spinazzola, J., & van der Kolk, B. A. (2012). Understanding interpersonal trauma in children: Why we need a developmentally appropriate trauma diagnosis. American Journal of Orthopsychiatry, 82(2), 187–200. https://doi.org/10.1111/j.1939-0025.2012.01154.x.
Enders, C. K. (2011). Missing not at random models for latent growth curve analyses. Psychological Methods, 16(1), 1–16. https://doi.org/10.1037/a0022640.
Erozkan, A. (2016). The link between types of attachment and childhood trauma. Universal Journal of Educational Research, 4(5), 1071-1079. https://doi.org/10.13189/ujer.2016.040517.
Fox, K. R., Ribeiro, J. D., Kleiman, E. M., Hooley, J. M., Nock, M. K., & Franklin, J. C. (2018). Affect toward the self and self-injury stimuli as potential risk factors for nonsuicidal self-injury. Psychiatry Research, 260, 279–285. https://doi.org/10.1016/j.psychres.2017.11.083.
Goldberg, D., & Bridges, K. (1987). Screening for psychiatric illness in general practice: The general practitioner versus the screening questionnaire. The Journal of the Royal College of General Practitioners, 37(294), 15–18.
He, J., Zhong, X., Gao, Y., Xiong, G., & Yao, S. (2019). Psychometric properties of the Chinese version of the childhood trauma questionnaire-short form (CTQ-SF) among undergraduates and depressive patients. Child Abuse & Neglect, 91, 102–108. https://doi.org/10.1016/j.chiabu.2019.03.009.
Hentschel, U., Draguns, J. G., Ehlers, W., & Smith, G. (2004). Defense mechanisms: Current approaches to research and measurement. In U. Hentschel, G. Smith, J. G. Draguns, & W. Ehlers (Eds.), Defense mechanisms: Theoretical, research and clinical perspectives (pp. 3–41, chapter xviii, 646 pages). Elsevier Science Ltd, Oxford.
Holland, P. W. (1986). Statistics and causal inference. Journal of the American Statistical Association, 81(396), 945–960. https://doi.org/10.1080/01621459.1986.10478354.
Huh, H. J., Kim, K. H., Lee, H.-K., & Chae, J.-H. (2017). The relationship between childhood trauma and the severity of adulthood depression and anxiety symptoms in a clinical sample: The mediating role of cognitive emotion regulation strategies. Journal of Affective Disorders, 213, 44–50. https://doi.org/10.1016/j.jad.2017.02.009.
Isohookana, R., Marttunen, M., Hakko, H., Riipinen, P., & Riala, K. (2016). The impact of adverse childhood experiences on obesity and unhealthy weight control behaviors among adolescents. Comprehensive Psychiatry, 71, 17–24. https://doi.org/10.1016/j.comppsych.2016.08.002.
Janoff-Bulman, R. (2010). Shattered assumptions. Simon and Schuster.
Jayawickreme, N., Jayawickreme, E., & Foa, E. B. (2013). Using the individualism-collectivism construct to understand cultural differences in PTSD. In (pp. 55–76). In K. Gow & M. Celinski (Eds.), Natural disaster research, prediction and mitigation. Mass trauma: Impact and recovery issues (p. 55–76). Nova Science Publishers.
Jennissen, S., Holl, J., Mai, H., Wolff, S., & Barnow, S. (2016). Emotion dysregulation mediates the relationship between child maltreatment and psychopathology: A structural equation model. Child Abuse & Neglect, 62, 51–62. https://doi.org/10.1016/j.chiabu.2016.10.015.
Jianing, Y., Congfen, M., Min-Pei, L., & Freedom, L. (2015). Comparing among the experiences of self-cutting, hitting, and scratching in Chinese adolescents attending secondary schools: An interview study. Behavioral disorders, 40(2), 122-137. https://doi.org/10.17988/BD-14-9.1.
Johnstone, J. M., Carter, J. D., Luty, S. E., Mulder, R. T., Frampton, C. M., & Joyce, P. R. (2016). Childhood predictors of lifetime suicide attempts and non-suicidal self-injury in depressed adults. Australian and New Zealand Journal of Psychiatry, 50(2), 135–144. https://doi.org/10.1177/0004867415585581.
Jungmeen, K.-S., Dante, C., & Fred, A. R. (2013). A longitudinal study of emotion regulation, emotion Lability-negativity, and internalizing symptomatology in maltreated and nonmaltreated children. Child Development, 84(2), 512–527. https://doi.org/10.1111/j.1467-8624.2012.01857.x.
Kharsati, N., & Bhola, P. (2016). Self-injurious behavior, emotion regulation, and attachment styles among college students in India. Industrial Psychiatry Journal, 25(1), 23–28. https://doi.org/10.4103/0972-6748.196049.
Klonsky, E. D. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review, 27(2), 226–239. https://doi.org/10.1016/j.cpr.2006.08.002.
Kokaliari, E. D. (2014). An exploratory study of the nature and extent of nonsuicidal self-injury among college women. International journal of population research, 2014, 1–7. https://doi.org/10.1155/2014/879269.
Lee, D. J., Witte, T. K., Weathers, F. W., & Davis, M. T. (2015). Emotion regulation strategy use and posttraumatic stress disorder: Associations between multiple strategies and specific symptom clusters. Journal of Psychopathology and Behavioral Assessment, 37(3), 533–544. https://doi.org/10.1007/s10862-014-9477-3.
Leong, C. H., Wu, A. M. S., & Poon, M. M.-y. (2014). Measurement of perceived functions of non-suicidal self-injury for Chinese adolescents. Archives of Suicide Research, 18(2), 193–212. https://doi.org/10.1080/13811118.2013.824828.
Li, J., Han, Z. R., Gao, M. M., Sun, X., & Ahemaitijiang, N. (2018). Psychometric properties of the Chinese version of the difficulties in emotion regulation scale (DERS): Factor structure, reliability, and validity. Psychological Assessment, 30(5), e1–e9. https://doi.org/10.1037/pas0000582.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128. https://doi.org/10.1207/s15327906mbr3901_4.
Mickelson, K. D., Kessler, R. C., & Shaver, P. R. (1997). Adult attachment in a nationally representative sample. Journal of Personality and Social Psychology, 73(5), 1092–1106. https://doi.org/10.1037/0022-3514.73.5.1092.
Mikulincer, M., & Shaver, P. R. (2019). Attachment orientations and emotion regulation. Current Opinion in Psychology, 25, 6–10. https://doi.org/10.1016/j.copsyc.2018.02.006.
Mischel, W., & Shoda, Y. (1995). A cognitive-affective system theory of personality: Reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychological Review, 102(2), 246–268. https://doi.org/10.1037/0033-295X.102.2.246.
Mortenson, S. T. (2006). Cultural differences and similarities in seeking social support as a response to academic failure: A comparison of American and Chinese college students. Communication Education, 55(2), 127–146. https://doi.org/10.1080/03634520600565811.
Navarro-Haro, M. V., Wessman, I., Botella, C., & García-Palacios, A. (2015). The role of emotion regulation strategies and dissociation in non-suicidal self-injury for women with borderline personality disorder and comorbid eating disorder. Comprehensive Psychiatry, 63, 123–130. https://doi.org/10.1016/j.comppsych.2015.09.001.
Nock, M. K., & Prinstein, M. J. (2004). A functional approach to the assessment of self-Mutilative behavior. Journal of Consulting Clinical Psychology, 72(5), 885–890. https://doi.org/10.1037/0022-006X.72.5.885.
Pascuzzo, K., Cyr, C., & Moss, E. (2013). Longitudinal association between adolescent attachment, adult romantic attachment, and emotion regulation strategies. Attachment and Human Development, 15(1), 83–103. https://doi.org/10.1080/14616734.2013.745713.
Paul, E., Tsypes, A., Eidlitz, L., Ernhout, C., & Whitlock, J. (2014). Frequency and functions of non-suicidal self-injury: Associations with suicidal thoughts and behaviors. Psychiatry Research, 225(3), 276–282. https://doi.org/10.1016/j.psychres.2014.12.026.
Powers, A., Cross, D., Fani, N., & Bradley, B. (2014). PTSD, emotion dysregulation, and dissociative symptoms in a highly traumatized sample. Journal of Psychiatric Research, 61, 174–179. https://doi.org/10.1016/j.jpsychires.2014.12.011.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177. https://doi.org/10.1037/1082-989X.7.2.147.
Tan, A. C. Y., Rehfuss, M. C., Suarez, E. C., & Parks-Savage, A. (2015). Nonsuicidal self-injury in an adolescent population in Singapore (vol 19, pg 58, 2014). Clinical Child Psychology and Psychiatry, 20(3), 525–525. https://doi.org/10.1177/1359104515594961.
Thomassin, K., Shaffer, A., Madden, A., & Londino, D. L. (2016). Specificity of childhood maltreatment and emotion deficit in nonsuicidal self-injury in an inpatient sample of youth. Psychiatry Research, 244, 103–108. https://doi.org/10.1016/j.psychres.2016.07.050.
Thomson, P., & Jaque, S. V. (2018). Childhood adversity and the creative experience in adult professional performing artists. Frontiers in Psychology, 9, 111–111. https://doi.org/10.3389/fpsyg.2018.00111.
Tresno, F., Ito, Y., & Mearns, J. (2012). Self-injurious behavior and suicide attempts among Indonesian college students. Death Studies, 36(7), 627–639. https://doi.org/10.1080/07481187.2011.604464.
Tresno, F., Ito, Y., & Mearns, J. (2013). Risk factors for nonsuicidal self-injury in Japanese college students: The moderating role of mood regulation expectancies. International Journal of Psychology, 48(6), 1009–1017. https://doi.org/10.1080/00207594.2012.733399.
Unger, J. A. M., & De Luca, R. V. (2014). The relationship between childhood physical abuse and adult attachment styles. Journal of Family Violence, 29(3), 223–234. https://doi.org/10.1007/s10896-014-9588-3.
Van der Kolk, B. A., Perry, J. C., & Herman, J. L. (1991). Childhood origins of self-destructive behavior. American Journal of Psychiatry, 148(12), 1665–1671.
Wu, W. L., Zhang, W., & Liu, X. H. (2004). The reliability and validity of adult attachment scale (AAS-1996 revised edition): A report on its application in China. Sichuan Da Xue Xue Bao. Yi Xue Ban, 35(4), 536–538.
Yates, T. M. (2004). The developmental psychopathology of self-injurious behavior: Compensatory regulation in posttraumatic adaptation. Clinical Psychology Review, 24(1), 35–74. https://doi.org/10.1016/j.cpr.2003.10.001.
You, J., Leung, F., Fu, K., & Lai, C. M. (2011). The prevalence of nonsuicidal self-injury and different subgroups of self-injurers in Chinese adolescents. Archives of Suicide Research, 15(1), 75–86. https://doi.org/10.1080/13811118.2011.540211.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Approval was obtained from the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong. The procedures used in this study adhere to the tenets of the declaration of the university.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wong, S.L., Chung, M.C. Child abuse and non-suicidal self-injury among Chinese university students: the role of emotion dysregulation and attachment style. Curr Psychol 42, 4862–4872 (2023). https://doi.org/10.1007/s12144-021-01832-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-01832-2