
Abstract
We sought to determine the relationship between dispositional mindfulness, Big Five personality traits, and psychopathology in a sample of adolescents at high risk for mood and anxiety disorders. The incremental utility of dispositional mindfulness in predicting psychopathology over and above the Big Five was investigated using a facet-level approach. One hundred and thirty-one adolescents (M = 13.76, SD = 1.65) who had a parent with a history of mood or anxiety disorders completed measures of dispositional mindfulness and facets of mindfulness (i.e., attention and awareness, nonreactivity, nonjudgement, and self-acceptance), the Big Five model of personality, psychopathology (i.e., internalizing, externalizing, and total problems scales), and mindfulness experience. Hierarchical multiple regressions were performed. Controlling for sex, mindfulness experience, and theory driven Big Five factors, higher dispositional mindfulness related to fewer internalizing, externalizing, and total problems. Mindfulness facet self-acceptance was key to this association. Nonreactivity moderated effects of attention and awareness, such that higher attention and awareness correlated to fewer internalizing and total problems only when nonreactivity was also high. Therefore, self-acceptance and nonreactive observing may be unique components of mindfulness that have implications for adolescent psychopathological symptoms, even controlling for well-established personality vulnerability factors. Future adolescent mindfulness intervention research and practice should emphasize techniques that involve observation while concurrently enhancing nonreactivity and self-acceptance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Adolescence is a sensitive period of development marked by significant psychosocial and biological changes increasing vulnerability to psychopathology (Kanwal, Jin Jung, & Zhang, 2016). Internalizing (e.g., depression and anxiety) and externalizing (e.g., attention deficit hyperactivity disorder, ADHD, and oppositional defiant disorder, ODD) problems (Achenbach, 1991; Krueger, 1999) are highly comorbid among adolescents (Lahey et al., 2008), are associated with peer rejection and deficits in social skills (Kingery, Erdley, Marshall, Whitker, & Reuter, 2010; Milledge et al., 2019), and are robust predictors of diagnosable episodes of mental illness in adulthood (Pine, Cohen, Cohen, & Brook, 1999). As such, substantial research has examined dispositional or trait-like factors that are intertwined with and confer risk for or resilience against psychopathology (e.g., Kotov et al., 2017; Krueger & Markon, 2014). The Big Five traits are perhaps the most widely studied personality vulnerability to mental illness. Meta-analyses specify maladaptive traits as high neuroticism, low extraversion, conscientiousness, and agreeableness, and, depending on psychopathology, high or low openness to experience (Chmielewski et al., 2014; Kotov et al., 2010; Malouff, Thorsteinsson, & Schutte, 2005). Neuroticism and extraversion predict the development of internalizing disorders (Kopala-Sibley, Klein, Perlman, & Kotov, 2017; Kotov et al., 2010). Neuroticism, conscientiousness, and agreeableness predict externalizing disorders (Watts, Poore, Lilienfeld, & Waldman, 2019).
More recently, dispositional mindfulness has been examined as a potential resiliency factor against psychopathology (Tan & Martin, 2012). Broadly, mindfulness is defined as the mode of perception in which attention is directed to experiences in the present moment with an orientation of open curiosity (Brown & Ryan, 2003). Originally considered to be a unidimensional trait, dispositional mindfulness is now commonly conceptualized as multidimensional (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006; Grossman & Van Dam, 2011), in which two constructs of mindfulness are important to cultivate together: (1) the ‘what’ of mindfulness; awareness of present moment experiences (e.g., thoughts, feelings, and sensations), and (2) the ‘how’ of mindfulness; a nonjudgmental, nonreactive, and accepting secondary reaction to such experiences (Baer et al., 2006; Bishop, Lau, Shapiro, Carlson, Anderson, Carmody et al., 2004). Thus, the synergetic nature of mindfulness has recently galvanized theoretical and empirical investigation into mindfulness facet interactions.
Despite positive associations between mindfulness and mental well-being, there is overlap in the association between mindfulness and Big Five traits (e.g., Giluk, 2009). It is not clear whether mindfulness is uniquely associated with psychopathology relative to the Big Five personality dimensions. Filling this gap in the literature is important in order to understand the ways in which personality and psychopathology are intertwined and inform unique versus overlapping preventive and psychotherapy approaches for adolescent mental health. Accordingly, the aims of the current study were to (i) investigate the relationships between adolescent psychopathology, five-factor personality traits, and dispositional mindfulness, and (ii) examine the incremental utility of dispositional mindfulness, mindfulness facets, and their interactions in predicting psychopathological symptoms over and above Big Five traits.
Dispositional Mindfulness & Psychopathology
Although most research has explored dispositional mindfulness and psychopathology among adults (see Carpenter, Conroy, Gomez, Curren, & Hofmann, 2019; Tomlinson, Yousaf, Vittersø, & Jones, 2018), several studies have echoed findings in non-clinical adolescent samples (e.g., Calvete, Orue, & Sampedro, 2017; Ciarrochi, Kashdan, Leeson, Heaven, & Jordan, 2011; Ciesla, Reilly, Dickson, Emanuel, & Updegraff, 2012; Marks, Sobanski, & Hine, 2010; Tan & Martin, 2012). The Childhood and Adolescent Mindfulness Measure (CAMM), a unifactorial adolescent measure, inversely correlates with internalizing symptoms, thought suppression, and psychological inflexibility (Greco, Baer, & Smith, 2011). Furthermore, youth mindfulness interventions improve adolescent mental health (Zoogman, Goldberg, Hoyt, & Miller, 2014), including anxiety (Borquist-Conlon, Maynard, Brendel, & Farina, 2019) and ADHD symptoms (Chimiklis et al., 2018). The mechanism through which these improvements occur, however, is not well known and may best be understood through the examination of mindfulness facets and their interactions.
The Adolescent and Adult Mindfulness Scale (AAMS; Droutman, Golub, Oganesyan, & Read, 2018) is a recently validated multifaceted questionnaire for youth derived from items on the CAMM and adult multifaceted mindfulness measures. Using factor analysis, the authors found four facets of dispositional mindfulness: (1) attention and awareness, the ability to observe the present moment including all thoughts, feelings and sensations, (2) nonreactivity, the ability to acknowledge and accept thoughts, feelings, and sensations while inhibiting secondary elaborative processing like rumination, (3) nonjudgement, the ability to observe one’s thoughts, opinions and feelings without evaluating them, and (4) self-acceptance, the ability to accept the self without criticism. AAMS facets nonreactivity and self-acceptance predict emotional regulation and self-compassion in middle-school aged children (Droutman et al., 2018). Further, higher endorsement of acting with awareness, nonjudgement and nonreactivity on the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2008) predict lower levels of psychological problems, including depression, in adults (Cash & Whittingham, 2010; Dixon & Overall, 2016) and adolescents over time (Cortazar & Calvete, 2019; Gómez-Odriozola & Calvete, 2020).
In contrast to these findings, the observing facet of the FFMQ, which corresponds to AAMS attention and awareness, is often positively associated with psychopathological symptoms, particularly in non-meditating adult (Baer et al., 2006, 2008) and adolescent samples (Cortazar & Calvete, 2019; Hambour, Zimmer-Gembeck, Clear, Rowe, & Avdagic, 2018). Calvete, Fernández-González, Echezarraga, and Orue (2019) found that adolescents with the FFMQ profile high observing and low acting with awareness and nonjudgment had higher levels of depressive symptoms, maladaptive schemas, stress perception, and stress-associated hormones. Without the ability to attend to inner and outer experiences in a nonreactive and nonjudgmental way, observation of the present moment may lead to maladaptive cognitions and behaviours (Baer, 2019; Eisenlohr-Moul, Walsh, Charnigo, Lynam, & Baer, 2012).
Interactions between observing and nonreactivity on the FFMQ have been found to predict distress and maladaptive coping. For example, observing was positively associated with periods of substance abuse in an undergraduate sample when levels of nonreactivity were low, but was negatively associated with substance abuse when levels of nonreactivity were high (N = 296, Eisenlohr-Moul et al., 2012). Two other studies have reported a similar interaction, such that nonreactivity moderated the direct effect of observing on adult depression symptoms (N = 189, Desrosiers, Vine, Curtiss, & Klemanski, 2014) and biomarkers of physical health among an undergraduate sample (N = 130, Tomfohr, Pung, Mills, & Edwards, 2014). The only study with adolescents, to our knowledge, to report on this interaction did not observe significant results while predicting internalizing and externalizing problems, potentially due to the fact that nonreactivity had low internal consistency in the sample (N = 737, Cortazar & Calvete, 2019). Further research is needed to confirm this interaction in adolescents, as it is unclear whether recent youth mindfulness interventions and school-based programs (e.g., Semple, Droutman, & Reid, 2017; Zenner, Herrnleben-Kurz, & Walach, 2014) have taken the interaction into account by placing emphasis on increasing nonreactivity in the context of cultivating present-moment observation.
Dispositional Mindfulness & The Big Five
Several reviews and meta-analyses in adults have revealed that dispositional mindfulness overlaps with Big Five personality factors (Giluk, 2009; Hanley & Garland, 2017; Rau & Williams, 2016). In particular, high levels of neuroticism predict low dispositional mindfulness (Giluk, 2009; Hanley & Garland, 2017), where acting with awareness, nonreactivity, and nonjudgement demonstrate the most reliable associations among FFMQ facets (Hanley & Garland, 2017; Rau & Williams, 2016). Additionally, conscientiousness, extroversion, agreeableness, and openness are positively associated with mindfulness, albeit more weakly than with neuroticism (Giluk, 2009; Hanley & Garland, 2017). As Big Five traits are robust predictors of psychopathology, associations with mindfulness must be teased apart from underlying personality configurations to confirm its potential resiliency profile and therapeutic benefit.
High levels of dispositional mindfulness have moderated and mediated the relationship between neuroticism and the development of depressive symptoms (Barnhofer, Duggan, & Griffith, 2011) and psychological wellbeing (Iani, Lauriola, Cafaro, & Didonna, 2017; Wenzel, von Versen, Hirschmüller, & Kubiak, 2015), suggesting they are at least somewhat distinct. Further, dispositional mindfulness showed incremental validity over and above Big Five traits when predicting psychological wellbeing (Mehta & Hicks, 2018), psychological distress, life satisfaction, and burnout (Grevenstein, Aguilar-Raab, & Bluemke, 2018). However, other results have been contradictory. Tran, Wasserbauer, and Voracek (2020) found that dispositional mindfulness and the Big Five share a common latent structure and the incremental validity of mindfulness relative to the Big Five in predicting psychopathology is negligible, with acting with awareness as a weak predictor. To our knowledge, however, no research has examined the incremental utility of dispositional mindfulness relative to the Big Five while predicting psychopathology in adolescents.
Present Study
The present study examined the relationship between mindfulness, Big Five factors, and psychopathology. Given that prior research has found mindfulness to be linked to a range of psychopathologies and an underlying transdiagnostic structure exists among psychopathology in general (e.g., Kotov et al., 2017), we did not expect differential associations of mindfulness with internalizing versus externalizing versus total problems, although we examined each separately to test this possibility. Over and above Big Five traits, it was hypothesized that elevated adolescent dispositional mindfulness would be negatively correlated with internalizing, externalizing, and total problems. Specifically, we hypothesized that nonreactivity, nonjudgement, and self-acceptance would drive these associations. We had no a priori hypotheses regarding the association for attention and awareness with the other variables, as previous associations with similar factor FFMQ observing have been inconsistent (Baer et al., 2006, 2008; Cortazar & Calvete, 2019; Hambour et al., 2018). Rather, it was hypothesized that higher levels of attention and awareness would correlate with lower psychopathology symptoms when nonreactivity was also high. We further expected these associations to be independent of Big Five personality traits.
Methods & Materials
Participants & Procedure
One hundred and thirty-one adolescents aged 11–18 (M = 13.76, SD = 1.65) were recruited via internet advertisements targeted at parents. Power analyses with an alpha of .05 suggested that a sample size of 113 would provide 80% power to detect a medium effect size between psychopathology, BFI factors, and dispositional mindfulness with up to 9 predictors (Cohen’s f2 = .15). The sample was somewhat weighted to females (61.8%, n = 81). The majority of the sample was of White/Caucasian descent (72.5%, n = 95) with an average household income of approximately $100,000. The highest level of parental education was, most frequently, partial college/university (25.2%, n = 33), a trade/technical/vocational degree (16.8, n = 22), an undergraduate degree (28.2%, n = 37), or postgraduate education (14.5%, n = 19).
Parent and child dyads were involved in a broader study assessing adolescent premorbid risk and resiliency factors for the development of clinical depressive and anxiety episodes. Thus, all adolescent participants in this study had a parental history of mood or anxiety disorders but did not meet current or lifetime clinical criteria for these disorders themselves. The Mini-International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) was used to confirm parental lifetime history of either major depression, persistent depression, bipolar disorder, or generalized or social anxiety disorder. The MINI for Children and Adolescents (MINI-Kid; Sheehan et al., 2010) was used to confirm no lifetime history of depression or anxiety in the sample of adolescents. Based on DSM-V (Diagnostic and Statistical Manual of Mental Disorders Fifth Addition; American Psychiatric Association, 2013) diagnostic criteria, 73 parents (55.7%) met criteria for a mood disorder (i.e., major depression, persistent depression, or bipolar disorder), 11 parents (8.4%) met criteria for an anxiety disorder (i.e., generalized or social anxiety disorder), and 47 parents (35.9%) met criteria for both. This is therefore a sample of youth at high risk for the development of mental illness (Weissman, Warner, Wickramaratne, Moreau, & Olfson, 1997) who have yet to develop clinically significant symptoms, although they had varying levels of subclinical symptoms. This is a unique sample in which to understand predictors of subclinical levels of psychopathology symptoms given that elevated subclinical symptoms are robust predictors of later diagnosable mental illness (Pine et al., 1999).
Participants reported on dispositional mindfulness, Big Five personality factors, and psychopathology. The majority of the survey was completed during a visit to the lab. The Big Five Inventory (BFI) and mindfulness experience questions were completed at home.
Measures
Psychopathology
To test DSM-V mental illnesses, the widely used, well-validated diagnostics interviews MINI and MINI-Kid were used. The MINI and MINI-Kid respectively converge well (Sheehan et al., 1998; Sheehan et al., 2010) with the Structured Clinical Interview for the DSM (SCID; First, 2014) and the Kiddie Schedule for Affective Disorders (KSADS; Kaufman et al., 1997).
Youth Self Report (YSR, Achenbach, 1991) was employed to assess adolescent psychopathological symptoms. The YSR consists of 103 items related to emotional and behavioural problems that are combined to form narrowband and broadband scales. Internalizing problems is a broadband scale that incorporates items from the anxious/depressed, withdrawn/depressed, and somatic complaints subscales. The externalizing problems broadband scale includes items from the rule breaking behaviour and aggressive behaviour subscales. In this study, the attention problems subscale was also aggregated into externalizing problems. The total problems scale combines subscales from internalizing and externalizing problems scales in addition to thought problems and social problems. For each item in the YSR, the respondent rates how well the item describes him or herself on a 3-point Likert scale from ‘0 – Not True’ to ‘2 – Very True or Often True.’ This questionnaire is validated for adolescents between 11 to 18 years old, is cross-culturally generalizable, and shows good concurrent validity including discriminability of anxious and depressed youth from non-anxious and non-depressed youth (Ebesutani, Bernstein, Martinez, Chorpita, & Weisz, 2011). Among our sample, we found excellent internal consistency for internalizing, externalizing, and total problems psychometric properties with Cronbach alphas of .91, .89, and .95, respectively.
The Big Five
The Big Five Inventory (BFI; John & Srivastava, 1999) was used to investigate five broad dimensions of personality: neuroticism, extraversion, conscientiousness, agreeableness, and openness to experience. The BFI converges well with other Big Five instruments (John & Srivastava, 1999), and has been validated for use with adolescents (Fossati, Borroni, Marchione, & Maffei, 2011). The questionnaire consists of 8–10 propositions for each domain (44 total) in which participants indicate the degree to which the items describe themselves on a 5-point Likert scale from strongly disagree (1) to strongly agree (5). The measure had good internal consistency in our sample for neuroticism (α = .84), extraversion (α = .84) and agreeableness (α = .83). Internal consistency for conscientiousness was satisfactory (α = .78). Openness to experience showed somewhat low internal consistency (α = .64).
Dispositional Mindfulness
To examine mindfulness facets and their interaction, we used the Adult and Adolescent Mindfulness Scale (AAMS) questionnaire, one of first factor-analytically derived multi-faceted mindfulness questionnaires validated for adolescents. The AAMS consists of 19 questions on a 5-point Likert scale. It provides a total score as well as scores for four separate domains of mindfulness: attention and awareness (e.g., “when I take a shower or a bath, I notice how water feels on my body”), nonreactivity (e.g., “when you realize that you missed something important in a class or during a lecture or a work meeting, how often do you get angry with self?”), nonjudgment (e.g., “I make judgments about whether my thoughts are good or bad”), and self-acceptance (e.g., “I tell myself that I shouldn’t be feeling the way I am feeling”). Nonreactivity, nonjudgment, and self-acceptance subscales are reverse scored. The AAMS has good convergent validity with emotional regulation and self-compassion (Droutman et al., 2018). The internal consistency of the mindfulness facets in our sample was good to satisfactory (attention and awareness, α = .85; nonreactivity α = .82; nonjudgment α = .77; self-acceptance α = .88). The AAMS total had a low alpha (α = .61), which is unsurprising given its multi-faceted structure. In this study, only facets were examined.
The AAMS is still a relatively new questionnaire, having only received validation from the original publication (Droutman et al., 2018). Thus, we incorporated a widely used unifactorial self-report measure, the Child and Adolescent Mindfulness Measure (CAMM), which is a 10-item scale that defines dispositional mindfulness as present-centered nonjudgmental accepting awareness. The questionnaire is reverse scored and consists of items such as, “I get upset with myself for having feelings that don’t make sense” and “at school, I walk from class to class without noticing what I’m doing.” Respondents are required to indicate how often they experience each item on a 5-point Likert scale from never (0) to always (4). The CAMM shows good internal consistency and convergent validity with lower levels of thought suppression and psychological inflexibility (Greco et al., 2011). In our sample, internal consistency was good (α = .85).
Mindfulness Experience
Given the effect mindfulness training can have on dispositional mindfulness (for meta-analysis see, Baer, Gu, Cavanagh, & Strauss, 2019), mindfulness experience was included as a control variable in our analyses. Participants were asked, in separate questions, to identify the frequency in which they practice mindfulness meditation and/or yoga on a 6-point Likert scale from ‘0-Never’ to ‘6 – Every day to nearly every day for more than 2 years (meditation)/At least once per week for over 4 years (yoga).’ For those that practiced mindfulness meditation, they were asked to indicate how long the average session was, from ‘1 – 1-3 minutes’ to ‘6 – Over 25 minutes.’ For those that practiced yoga, they indicated how much time they typically spent actively attending to the sensations of their body and breath during the practice, from ‘0 - Not at all’ to ‘6 – Throughout the entire practice.’ Scores on meditation and yoga questions were summed to compute a mindfulness experience total score. The internal consistency for mindfulness experience was satisfactory (α = .79).
Analytic Strategy
Data analysis for this study was conducted in three steps using IBM SPSS Statistics and AMOS 24.0. First, bivariate correlations were computed to examine the association between internalizing, externalizing and total problems, BFI personality domains, dispositional mindfulness, mindfulness experience, and demographic information. Second, hierarchical multiple regressions were performed to assess the predictive power of dispositional mindfulness on psychopathology beyond BFI traits. Internalizing, externalizing, and total problems were individually regressed onto BFI factors and mindfulness variables, controlling for sex and mindfulness experience. Based on prior theory and research (Kopala-Sibley et al., 2017; Kotov et al., 2010; Watts et al., 2019), neuroticism and extraversion were included in analyses examining internalizing problems, while neuroticism, agreeableness, and conscientiousness were included in analyses examining externalizing problems. All five BFI factors were included as covariates in analyses examining total problems. Two separate models were computed to examine the difference in contribution between CAMM mindfulness scores and AAMS mindfulness facets. The first block included sex and mindfulness experience; the second block included theory-driven BFI factors; the final block incorporated the mindfulness measure of interest. Third, to test the moderation of observing on psychopathology by nonreactivity, the interaction between mean-centered scores on attention and awareness and nonreactivity was examined using the PROCESS macro for SPSS (Hayes, 2013). The Johnson-Neyman technique was then conducted to determine conditional effects of attention and awareness on psychopathology at different levels of nonreactivity. Analyses were also repeated after excluding and including all BFI variables in order to examine how they may have influenced patterns of associations between mindfulness and psychopathology. We report standardized betas, R-squared values, and confidence intervals.
As some questionnaires were completed in the lab and others at home, missing data was present. Specifically, 25 youth had missing data on the AAMS, 16 on the CAMM, 21 on the BFI, and 6 on the YSR. Little’s MCAR test (Little, 1988) indicated that data were missing at random (MAR; c = 60.61 (61), p = .490). Accordingly, missing data were singly imputed via regression imputation with Full Information Maximum Likelihood (FIML) estimation. The FIML approach is generally acknowledged to be preferable to other methods for dealing with missing data, such as listwise deletion or mean imputation, as these latter approaches are more likely to yield biased estimates (Estabrook & Neale, 2013; Schafer & Graham, 2002).
Results
Bivariate Correlations
Table 1 displays descriptive statistics and zero-order correlations among study variables. Age, household income, and ethnicity had no associations with the variables of interest. Females scored significantly higher than males on internalizing problems (t(129) = 2.62, p = .010), neuroticism (t(129) = 3.25, p = .001), CAMM (t(129) = −2.23, p = .028), and nonreactivity (t(129) = −2.22, p = .028). The majority of the sample either had no meditation experience (40.5%, n = 53) or indicated meditating once or twice in their lifetime (18.3%, n = 24). The sample either had no yoga experience (30.5%, n = 40) or had practiced yoga once or twice in their lifetime (28.2%, n = 37). Mindfulness experience (aggregate meditation and yoga score) was positively correlated to attention and awareness and negatively correlated to nonjudgement and self-acceptance. Based on these results, participant sex and mindfulness experience were included in analyses.
Nonreactivity, nonjudgement and self-acceptance were negatively correlated to internalizing problems. Self-acceptance was linked to fewer externalizing problems. Attention and awareness had no association with either mental health outcome. Notably, personality traits also correlated with dispositional mindfulness. Neuroticism was negatively associated with the CAMM, nonreactivity, nonjudgement, and self-acceptance. Extraversion positively correlated to the CAMM and nonreactivity. Conscientiousness positively correlated to the CAMM and self-acceptance. Agreeableness was positively associated with the CAMM and self-acceptance.
Hierarchical Regression Analyses
Internalizing Problems
Controlling for sex and mindfulness experience, high neuroticism and low extraversion significantly predicted greater internalizing problems and explained a significant portion of the variance (Table 2). Next, CAMM explained an additional 16.6% of the variance in internalizing problems (Table 2). In a separate model, AAMS facets explained an additional 7.1% of the variance (Table 3), with higher self-acceptance being the sole significant predictor of fewer internalizing problems. Without covarying for BFI factors, nonreactivity also significantly predicted fewer internalizing problems (ß = −.243, t(124) = −2.78, p = .006, CI = [−13.7, −0.23]).
Externalizing Problems
Low conscientiousness and low agreeableness significantly predicted and explained a significant portion of the variance in high externalizing problems when controlling for sex and mindfulness experience (Table 2). Next, CAMM explained 5.9% of additional variance, such that elevated dispositional mindfulness related to fewer externalizing problems (Table 2). In a separate model, higher self-acceptance significantly predicted fewer externalizing problems, although the overall block did not explain a significant portion of the variance (Table 3).
Total Problems
Controlling for sex and mindfulness experience, high neuroticism, low conscientiousness, and low agreeableness significantly predicted higher total problems scores and explained a significant portion of the variance (Table 2). Next, CAMM explained 15.1% of additional variance, such that higher levels of dispositional mindfulness related to fewer total problems (Table 2). In a separate model, AAMS facets explained 6.2% of additional variance, with higher self-acceptance solely and significantly predicting fewer total problems (Table 3).
Facet Interaction
Internalizing Problems
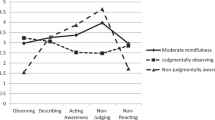
Controlling for sex, mindfulness experience, neuroticism, extraversion, and main effects of predictors, the interaction between attention and awareness and nonreactivity significantly predicted internalizing problems (ß = −.069, t(123) = −2.46, p = .015, 95% CI = [−0.12, −0.01], R2 = .496, F(7, 123) = 20.31, p < .001). Analysis of the shape of the interaction showed that elevated attention and awareness predicted lower internalizing problems only when nonreactivity was high (Fig. 1). The Johnson-Neyman test indicated that the effect of attention and awareness on internalizing problems was significant when participants had a mean-centered score above of 2.76 on nonreactivity (20.45% of sample; Fig. 2).

Moderation of the Effect of Attention and Awareness on Internalizing and Total Problems at Values of the Moderator Nonreactivity when Controlling for Sex, Mindfulness Experience, and Theory-Driven BFI factors. Note. The above interaction significantly predicted internalizing problems even after mindfulness experience was removed as a covariate and significantly predicted total problems after BFI factors and mindfulness experience were removed as covariates

Johnson-Neyman Plot for the Conditional Effect of Attention and Awareness on Internalizing Problems and Total Problems at Values of the Moderator Nonreactivity. Note. Controlling for sex, mindfulness experience, and theory-driven BFI traits, the effect of attention and awareness on internalizing problems was significant above mean-centered scores of 2.76 on nonreactivity, and the effect of attention and awareness on total problems was significant above mean-centered scores of 4.33 on nonreactivity
Externalizing Problems
No significant interaction was found between attention and awareness and nonreactivity in predicting externalizing problems when controlling for sex, mindfulness experience, neuroticism, conscientiousness, agreeableness, and main effects of predictors (ß = −.058, t(122) = −1.42, p = .157, 95% CI = [−0.14, 0.02]).
Total Problems
Controlling for sex, all BFI factors, and main effects of predictors, the interaction between attention and awareness and nonreactivity significantly predicted total problems (ß = −.186, t(120) = −2.13, p = .035, 95% CI = [−0.36, −0.01], R2 = .450, F(10, 120) = 10.79, p < .001). That is, elevated attention and awareness predicted fewer total problems but only when nonreactivity was also high (Fig. 1). Based on the Johnson-Neyman test, the effect of attention and awareness on internalizing problems was significant when participants had a mean-centered score above 4.32 on nonreactivity (5.3% of sample; Fig. 2).
Discussion
Dispositional mindfulness and Big Five personality traits are often viewed as conceptually distinct personality domains linked to psychopathology in youth. Nonetheless, Big Five traits and mindfulness facets overlap, particularly neuroticism and acting with awareness, nonreactivity, and nonjudgment (Rau & Williams, 2016). Given the overlapping nature of the constructs, the incremental validity of dispositional mindfulness in explaining psychopathology over and above the Big Five traits has been questioned (e.g., Tran et al., 2020). As mindfulness strategies are increasing in frequency in youth demographics in an effort to combat the onset of psychopathological disorders (e.g., Zoogman et al., 2014), this study tested the incremental utility of dispositional mindfulness while predicting psychopathology symptoms over and above psychological constructs known to share a relationship with mental health and well-being. Elevated dispositional mindfulness predicted youth psychopathological symptoms even after covarying for the influence of Big Five personality traits, such that high levels of self-acceptance as well as high nonreactive observing (attention and awareness x nonreactivity) related to fewer internalizing and total problems. Higher self-acceptance also related to fewer externalizing problems over and above the Big Five, but nonreactive observing was not significant.
Results broadly replicate correlations found previously between facets of mindfulness and adolescent psychopathology (Droutman et al., 2018; Cortazar & Calvete, 2019). As predicted, high levels of nonjudgement, nonreactivity, and self-acceptance were related to fewer internalizing problems. In contrast, only self-acceptance was associated (negatively) with externalizing problems. The inability to accept one’s cognitions and emotions (self-acceptance) may, in part, relate to poor emotional regulation strategies, such as emotional suppression or avoidance, that could result in externalizing behaviours like inattention and physical aggression. However, the ability to be nonevaluative (nonjudgmental) and to “let go” and accept experiences (nonreactive) may be a better predictor of internalizing rather than externalizing problems, as attentional bias toward negative emotionally valenced personal experiences have been associated with internalizing problems (Peckham, McHugh, & Otto, 2010). We note, however, that there is considerable overlap between internalizing and externalizing symptomology and thus interpret these findings with caution.
Meta-analyses show that dispositional mindfulness is highly associated with Big Five personality factors (Giluk, 2009; Hanley & Garland, 2017; Rau & Williams, 2016). In our sample, a strong negative correlation between dispositional mindfulness and neuroticism (in particular, with nonreactivity, nonjudgement, and self-acceptance), conscientiousness, and agreeableness (in particular, with self-acceptance) was confirmed. Our study also found that higher levels of extraversion moderately related to higher CAMM and nonreactivity scores. Findings regarding the association between extraversion and mindfulness, however, are mixed and meta-analyses indicate extraversion as the Big Five factor that is least associated with dispositional mindfulness (Giluk, 2009; Hanley & Garland, 2017).
In determining the incremental utility of dispositional mindfulness, the CAMM explained additional variance beyond BFI traits when predicting internalizing, externalizing, and total problems, suggesting, at the very least, its usefulness as a preventative strategy and therapy for youth psychopathology. In particular, AAMS self-acceptance predicted psychopathology symptoms over and above the BFI factors. Alternatively, it is also possible that self-acceptance offers additional coverage of broad personality domains (namely, neuroticism) that were not exhaustively assessed in the BFI. This may explain why the facet predicts incremental variance in psychopathology controlling for BFI factors, suggesting it may not in fact be a unique predictor in and of itself. Further, self-acceptance may be an explicit coping strategy, particularly in adolescence, yet overlap with neuroticism. It is therefore unclear how various mindfulness items map onto the Big Five, and further research is required.
Based on Bishop et al. (2004) two-component model and other accounts (Baer et al., 2006), mindfulness involves the combination of what one does when being mindful (i.e., paying attention and observing the present moment) as well as the elements of how one does it (i.e., in an accepting, nonjudgmental, and nonreactive way), yet the investigation of mindfulness facets and their interactions are rarely explored in the literature. As mindfulness practices become more mainstream in adolescent interventions and school curricula (Semple et al., 2017; Zenner et al., 2014), clinicians and teachers run the risk of reducing the construct to a series of actions with little consideration for the way in which mindfulness should be cultivated (Grossman & Van Dam, 2011). The interaction term ‘nonreactive observing’ has previously been linked to reductions in depression symptoms (Desrosiers et al., 2014), substance use (Eisenlohr-Moul et al., 2012), and proinflammatory cytokines (Tomfohr et al., 2014). To our knowledge, this is the first study to find a similar interaction in adolescents. In our sample, attention and awareness was negatively correlated to internalizing and total problems, over and above the Big Five, but only when nonreactivity was also high. Further evidence has shown that a similar relationship may be shared with acting with awareness and nonjudgment, such that acting with awareness is only beneficial when the capacity to refrain from judging emotions, thoughts, and sensations is also cultivated (Cortazar & Calvete, 2019; Peters, Eisenlohr-Moul, Upton, & Baer, 2013; Tomfohr et al., 2014). These findings shed light on the necessity to sequence present-centered observation with a nonreactive and nonjudgmental attitude during mindfulness training.
Designing interventions focused on enhancing self-acceptance and nonreactive observing may benefit mental health outcomes among youth beyond reducing well-established maladaptive traits. Furthermore, given that dispositional mindfulness showed additive effects in predicting psychopathology beyond the Big Five, mindfulness training may be beneficial for decreasing psychopathology symptoms in adolescent higher in maladaptive Big Five personality traits. It is important to acknowledge that other factors, including societal, political, and structural issues, contribute to the risk and resilience for psychopathology. It should also be noted that there are a range of effective interventions for adolescent mental health, and matching treatment preferences is an important predictor of outcomes (see, Swift & Callahan, 2009). Thus, the implementation of mindfulness interventions must be individually considered for their relative benefit.
Mindfulness Experience
Mindfulness experience in adolescents is often limited and difficult to interpret (Greco et al., 2011). Two studies report contrary outcomes in adolescents with meditation or yoga experience where more experience related to significantly lower scores on the Mindful Attention and Awareness Scale-Adolescents (MAAS-A; Brown, West, Loverich, & Biegelet, 2011) and the CAMM (de Bruin, Zijlstra, & Bögels, 2014; de Bruin, Zijlstra, van de Weijer-Bergsma, & Bögels, 2011). In our sample, level of mindfulness experience was negatively correlated to self-acceptance and nonjudgment. One interpretation of these results is that a lack of self-acceptance and feelings of judgment may motivate youth to practice mindfulness meditation or yoga as a means of self-improvement or as a coping mechanism. Another interpretation comes from evidence that meditation experience affects the interpretation of mindfulness questionnaires (Van Dam, Earleywine, & Danoff-Burg, 2009). Meditators are suggested to have increased meta-awareness (including greater awareness of mindlessness), which may cause them to rate themselves as less mindful than someone without meditation experience (Grossman & Van Dam, 2011). They may also compare themselves to meditation experts and therefore rate themselves lower than the general population. In this sample, only three participants indicated having practiced mindfulness meditation for 2 or more years. As such, it is unlikely that mindfulness experience reflected heightened meta-awareness or a reference effect and thus the first interpretation is likely more plausible.
Limitations & Future Directions
There are several important limitations to note. First, the cross-sectional nature of the study did not allow for causal inferences to be drawn nor the examination of changes in psychopathology as a result of dispositional mindfulness over time. It also cannot establish the direction of effects, as mindfulness and psychopathology may have bidirectional effects. As this is the first study to our knowledge to explore the predictive utility of adolescent dispositional mindfulness in terms of psychopathology over and above the Big Five, establishing cross-sectional incremental effects is important prior to conducting longitudinal research. Second, reliance upon self-report measures may inflate associations due to shared method variance, although this would not explain the significant interaction found in our data. Third, adolescent multifaceted dispositional mindfulness questionnaires are still in their infancy. Previous research in adults using the FFMQ have found that acting with awareness (defined as the opposite of automatic pilot, Baer et al., 2008) is weakly associated to psychopathology over and above the Big Five (Tran et al., 2020) and interacts with nonjudgement to predict measures of positive wellbeing (Cortazar & Calvete, 2019; Peters et al., 2013; Tomfohr et al., 2014). The AAMS does not include acting with awareness, a core component of mindfulness. The CAMM does include items directly related to the facet (e.g., “At school, I walk from class to class without noticing what I am doing” reverse scored), but this questionnaire does not have a multi-factorial structure (Greco et al., 2011). Thus, we were unable to examine specific effects related to acting with awareness and its interactions on adolescent psychopathology in our sample. Lastly, the internal consistency for openness was somewhat low in our study, which may have impacted results with total problems. Future research should take note of these limitations and aim to replicate findings using longitudinal designs.
Conclusion
As more attention has been focused on preventive strategies and treatments targeting the onset of psychopathology in youth, determining the usefulness of constructs such as mindfulness is important to structuring such interventions. The research presented here supports the incremental utility of mindfulness as at least somewhat distinct from highly correlated personality domains in its link to psychopathology in youth. Self-acceptance may be a unique component of mindfulness that offers resilience against adolescent psychopathological symptoms. Moreover, while attention and awareness and nonreactivity on their own were not related to psychopathology over and above personality traits, their interaction (i.e., attention and awareness x nonreactivity) may predict psychopathology. Further research may benefit from a facet-level approach, including investigating interaction terms, when designing clinical interventions and tracking mechanistic changes related to mindfulness.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Achenbach, T. M. (1991). Manual for the youth self-report and 1991 profile. Burlington, VT: University of Vermont, Department of Psychiatry.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). VA: Arlington.
Baer, R. A. (2019). Assessment of mindfulness by self-report. Current Opinion in Psychology, 28, 42–48.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self- report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., Walsh, E., Duggan, D., & Williams, M. G. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15, 329–342.
Baer, R., Gu, J., Cavanagh, K., & Strauss, C. (2019). Differential sensitivity of mindfulness questionnaires to change with treatment: A systematic review and meta-analysis. Psychological Assessment, 31(10), 1247–1263.
Barnhofer, T., Duggan, D., & Griffith, J. (2011). Dispositional mindfulness moderates the relation between neuroticism and depressive symptoms. Personality and Individual Differences, 51(8), 958–962.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., Segal, Z. V., Abbey, S., Speca, M., Velting, D., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11, 230–241.
Borquist-Conlon, D. S., Maynard, B. R., Brendel, K. E., & Farina, A. S. J. (2019). Mindfulness-based interventions for youth with anxiety: A systematic review and meta-analysis. Research on Social Work Practice, 29(2), 195–205.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.
Brown, K., West, A., Loverich, T., & Biegel, G. (2011). Assessing adolescent mindfulness: Validation of an adapted mindful attention awareness scale in adolescent normative and psychiatric populations. Psychological Assessment, 23(4), 1023–1033.
Calvete, E., Orue, I., & Sampedro, A. (2017). Does the acting with awareness trait of mindfulness buffer the predictive association between stressors and psychological symptoms in adolescents? Personality and Individual Differences, 105, 158–163.
Calvete, E., Fernández-González, L., Echezarraga, A. & Orue, I. (2019). Dispositional mindfulness profiles in adolescents and their associations with psychological functioning and hypothalamic–pituitary–adrenal Axis hormones. Journal of Youth And Adolescence, 49(7), 4068–1419.
Carpenter, J., Conroy, K., Gomez, A., Curren, L., & Hofmann, S. (2019). The relationship between trait mindfulness and affective symptoms: A meta-analysis of the five facet mindfulness questionnaire (FFMQ). Clinical Psychology Review, 74, 101785.
Cash, M., & Whittingham, K. (2010). What facets of mindfulness contribute to psychological well-being and depressive, anxious, and stress-related symptomatology? Mindfulness, 1(3), 177–182.
Chimiklis, A., Dahl, V., Spears, A., Goss, K., Fogarty, K., & Chacko, A. (2018). Yoga, mindfulness, and meditation interventions for youth with ADHD: Systematic review and meta-analysis. Journal of Child and Family Studies, 27(10), 3155–3168.
Chmielewski, M., Bagby, R., Markon, K., Ring, A., & Ryder, A. (2014). Openness to experience, intellect, schizotypal personality disorder, and psychoticism: Resolving the controversy. Journal of Personality Disorders, 28(4), 483–499.
Ciarrochi, J., Kashdan, T., Leeson, P., Heaven, P., & Jordan, C. (2011). On being aware and accepting: A one-year longitudinal study into adolescent well-being. Journal of Adolescence, 34(4), 695–703.
Ciesla, J., Reilly, L., Dickson, K., Emanuel, A., & Updegraff, J. (2012). Dispositional mindfulness moderates the effects of stress among adolescents: Rumination as a mediator. Journal of Clinical Child & Adolescent Psychology, 41(6), 760–770.
Cortazar, N., & Calvete, E. (2019). Dispositional mindfulness and its moderating role in the predictive association between stressors and psychological symptoms in adolescents. Mindfulness, 10(10), 2046–2059.
de Bruin, E., Zijlstra, B., van de Weijer-Bergsma, E., & Bögels, S. (2011). The mindful attention awareness scale for adolescents (MAAS-A): Psychometric properties in a Dutch sample. Mindfulness, 2(3), 201–211.
de Bruin, E., Zijlstra, B., & Bögels, S. (2014). The meaning of mindfulness in children and adolescents: Further validation of the child and adolescent mindfulness measure (CAMM) in two independent samples from the Netherlands. Mindfulness, 5, 422–430.
Desrosiers, A., Vine, V., Curtiss, J., & Klemanski, D. H. (2014). Observing nonreactively: A conditional process model linking mindfulness facets, cognitive emotion regulation strategies, and depression and anxiety symptoms. Journal of Affective Disorders, 165, 31–37.
Dixon, H. C., & Overall, N. C. (2016). Dispositional mindfulness attenuates the link between daily stress and depressed mood. Journal of Social and Clinical Psychology, 35, 255–268.
Droutman, V., Golub, I., Oganesyan, A., & Read, S. (2018). Development and initial validation of the Adolescent and Adult Mindfulness Scale (AAMS). Personality and Individual Differences, 123, 34–43.
Ebesutani, C., Bernstein, A., Martinez, J. I., Chorpita, B. F., & Weisz, J. R. (2011). The youth self report: Applicability and validity across younger and older youths. Journal of Clinical Child and Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 40(2), 338–346.
Eisenlohr-Moul, T. A., Walsh, E. C., Charnigo, R. J., Lynam, D. R., & Baer, R. A. (2012). The “what” and the “how” of dispositional mindfulness. Assessment, 19, 276–286.
Estabrook, R., & Neale, M. (2013). A comparison of factor score estimation methods in the presence of missing data: Reliability and an application to nicotine dependence. Multivariate Behavioral Research, 48(1), 1–27.
First, M, B. (2014). Structured clinical interview for the DSM (SCID). The Encyclopedia of Clinical Psychology, 1–6.
Fossati, A., Borroni, S., Marchione, D., & Maffei, C. (2011). The big five inventory (BFI): Reliability and validity of its Italian translation in three independent nonclinical samples. European Journal of Psychological Assessment, 27(1), 50–58.
Giluk, T. L. (2009). Mindfulness, big five personality, and affect: A meta-analysis. Personality and Individual Differences, 47, 805–811.
Gómez-Odriozola, J., Calvete, E. (2020) Longitudinal bidirectional associations between dispositional mindfulness, maladaptive schemas, and depressive symptoms in adolescents. Mindfulness, 11, 1943–1955.
Greco, L. A., Baer, R. A., & Smith, G. T. (2011). Assessing mindfulness in children and adolescents: Development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychological Assessment, 23(3), 606–614.
Grevenstein, D., Aguilar-Raab, C., & Bluemke, M. (2017). Mindful and resilient? Incremental validity of sense of coherence over mindfulness and big five personality factors for quality of life outcomes. Journal of Happiness Studies, 19(7), 1883–1902.
Grossman, P., & Van Dam, N. T. (2011). Mindfulness, by any other name…: Trials and tribulations of sati in western psychology and science. Contemporary Buddhism, 12(1), 219–239.
Hambour, V., Zimmer-Gembeck, M., Clear, S., Rowe, S., & Avdagic, E. (2018). Emotion regulation and mindfulness in adolescents: Conceptual and empirical connection and associations with social anxiety symptoms. Personality and Individual Differences, 134, 7–12.
Hanley, A., & Garland, E. (2017). The mindful personality: A meta-analysis from a cybernetic perspective. Mindfulness, 8(6), 1456–1470.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. The Guilford Press.
Iani, L., Lauriola, M., Cafaro, V., & Didonna, F. (2017). Dimensions of mindfulness and their relations with psychological well-being and neuroticism. Mindfulness, 8(3), 664–676.
John, O. P., & Srivastava, S. (1999). The big-five trait taxonomy: History, measurement, and theoretical perspectives. In L. A. Pervin & O. P. John (Eds.), Handbook of personality: Theory and research (Vol. 2, pp. 102–138). New York: Guilford Press.
Kanwal, J, S., Jin Jung, Y., Zhang, M. (2016). Brain plasticity during adolescence: Effects of stress, sleep, sex and sounds on decision making. Anatomy & Physiology, 6(1), 1000e135.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., Williamson, D., & Ryan, N. (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child and Adolescent Psychiatry, 36(7), 980–988.
Kingery, J. N., Erdley, C. A., Marshall, K. C., Whitker, K. G., & Reuter, T. R. (2010). Peer experiences of anxious and socially withdrawn youth: An integrative review of the developmental and clinical literature. Clinical Child and Family Psychology Review, 13, 91–128.
Kopala-Sibley, D. C., Klein, D. N., Perlman, G., & Kotov, R. (2017). Self-criticism and dependency in female adolescents: Prediction of first onsets and disentangling the relationships between personality, stressful life events, and internalizing psychopathology. Journal of Abnormal Psychology, 126(8), 1029–1043.
Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010). Linking “big” personality trait to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136, 768–821.
Kotov, R., Krueger, R. F., Watson, D., Achenbach, T. M., Althoff, R. R., Bagby, R. M., Brown, T. A., Carpenter, W. T., Caspi, A., Clark, L. A., Eaton, N. R., Forbes, M. K., Forbush, K. T., Goldberg, D., Hasin, D., Hyman, S. E., Ivanova, M. Y., Lynam, D. R., Markon, K., Miller, J. D., Moffitt, T. E., Morey, L. C., Mullins-Sweatt, S. N., Ormel, J., Patrick, C. J., Regier, D. A., Rescorla, L., Ruggero, C. J., Samuel, D. B., Sellbom, M., Simms, L. J., Skodol, A. E., Slade, T., South, S. C., Tackett, J. L., Waldman, I. D., Waszczuk, M. A., Widiger, T. A., Wright, A. G. C., & Zimmerman, M. (2017). The hierarchical taxonomy of psychopathology (HiTOP): A dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 126(4), 454–477.
Krueger, R. F. (1999). The structure of common mental disorders. Archives of General Psychiatry, 56(10), 921–926.
Krueger, R., & Markon, K. (2014). The role of the DSM-5 personality trait model in moving toward a quantitative and empirically based approach to classifying personality and psychopathology. Annual Review of Clinical Psychology, 10(1), 477–501.
Lahey, B., Rathouz, P., Van Hulle, C., Urbano, R., Krueger, R., Applegate, B., et al. (2008). Testing structural models of DSM-IV symptoms of common forms of child and adolescent psychopathology. Journal of Abnormal Child Psychology, 36(2), 187–206.
Little, R. J. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202.
Malouff, J. M., Thorsteinsson, E. B., Schutte, N. S. (2005) The relationship between the Five-Factor model of personality and symptoms of clinical disorders: A meta-analysis. Journal of Psychopathology and Behavioral Assessment, 27 (2), 101–114.
Marks, A., Sobanski, D., & Hine, D. (2010). Do dispositional rumination and/or mindfulness moderate the relationship between life hassles and psychological dysfunction in adolescents? Australian & New Zealand Journal of Psychiatry, 44(9), 831–838.
Mehta, Y., & Hicks, R. (2018). The big five, mindfulness, and psychological well-being. Global Science and Technology Forum (GSTF) Journal of Psychology, 4(1), 1–6.
Milledge, S. V., Cortese, S., Thompson, M., McEwan, R., Rolt, M., Meyer, B., Sonuga-Barke, E., & Eisenbarth, H. (2019). Peer relationships and prosocial behaviour differences across disruptive behaviours. European Child & Adolescent Psychiatry, 28(6), 781–793.
Peckham, A., D., McHugh, R. K., & Otto, M. W. (2010) A meta-analysis of the magnitude of biased attention in depression. Depression and Anxiety, 27(12), 1135–1142.
Peters, J. R., Eisenlohr-Moul, T. A., Upton, B. T., & Baer, R. A. (2013). Nonjudgment as a moderator of the relationship between present-centered awareness and borderline features: Synergistic interactions in mindfulness assessment. Personality and Individual Differences, 55, 24–28.
Pine, D. S., Cohen, E., Cohen, P., & Brook, J. (1999). Adolescent depressive symptoms as predictors of adult depression: Moodiness or mood disorder? American Journal of Psychiatry, 156(1), 133–135.
Rau, H., & Williams, P. (2016). Dispositional mindfulness: A critical review of construct validation research. Personality and Individual Differences, 93, 32–43.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177.
Semple, R. J., Droutman, V., & Reid, B. A. (2017). Mindfulness goes to school: Things learned (so far) from research and real-world experiences. Psychology in the Schools, 54(1), 29–52.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Weiller, E., Hergueta, T., Baker, R., Dunbar, D. C. & (1998). The mini-international neuropsychiatric interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59(20), 22–57.
Sheehan, D. V., Sheehan, K. H., Shytle, R., Janavs, J., Bannon, Y., Rogers, J., et al. (2010). Reliability and validity of the Mini international neuropsychiatric interview for children and adolescents (MINI-KID). The Journal of Clinical Psychiatry, 71(03), 313–326.
Swift, J. K., & Callahan, J. L. (2009). The impact of client treatment preferences on outcome: A meta-analysis. Journal of Clinical Psychology, 65(4), 368–381. https://doi.org/10.1002/jclp.20553.
Tan, L. B., & Martin, G. (2012). Mind full or mindful: A report on mindfulness and psychological health in healthy adolescents. International Journal of Adolescence and Youth, 21, 64–74.
Tomfohr, L. M., Pung, M. A., Mills, P. J., & Edwards, K. (2014). Trait mindfulness is associated with blood pressure and interleukin-6: Exploring interactions among subscales of the five facet mindfulness questionnaire to better understand relationships between mindfulness and health. Journal of Behavioral Medicine, 38, 28–38.
Tomlinson, E., Yousaf, O., Vittersø, A., & Jones, L. (2018). Dispositional mindfulness and psychological health: A systematic review. Mindfulness, 9(1), 23–43.
Tran, U., Wasserbauer, J., & Voracek, M. (2020). Testing the incremental validity of dispositional mindfulness over and above the big five in accounting for mental health: A facet-level structural-equation modeling and predictor communality and dominance approach. Personality and Individual Differences, 156, 109769.
Van Dam, N., Earleywine, M., & Danoff-Burg, S. (2009). Differential item function across meditators and non-meditators on the five facet mindfulness questionnaire. Personality and Individual Differences, 47(5), 516–521.
Watts, A., Poore, H., Lilienfeld, S., & Waldman, I. (2019). Clarifying the associations between big five personality domains and higher-order psychopathology dimensions in youth. Journal of Research in Personality, 82, 103844.
Weissman, M. M., Warner, V., Wickramaratne, P., Moreau, D., & Olfson, M. (1997). Offspring of depressed parents: 10 years later. Archives of General Psychiatry, 54(10), 932–940.
Wenzel, M., von Versen, C., Hirschmüller, S., & Kubiak, T. (2015). Curb your neuroticism – Mindfulness mediates the link between neuroticism and subjective well-being. Personality and Individual Differences, 80, 68–75.
Zenner, C., Herrnleben-Kurz, S., & Walach, H. (2014). Mindfulness-based interventions in schools: A systematic review and meta-analysis. Frontiers in Psychology, 5(603).
Zoogman, S., Goldberg, S., Hoyt, W., & Miller, L. (2014). Mindfulness interventions with youth: A meta-analysis. Mindfulness, 6(2), 290–302.
Funding
This research was supported by funding from Social Sciences and Humanities Research Council of Canada, the Natural Sciences and Engineering Research Council of Canada, the Canadian Institutes of Health Research, and the Brain and Behaviour Research Foundation, awarded to Dr. Daniel Kopala-Sibley. Jade Stein was supported by a Branch Out Neurological Foundation Master’s Grant and Natural Sciences and Engineering Research Council of Canada Master’s Scholarship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
On behalf of all authors, the corresponding author states there are no conflicts of interest to declare.
Ethical Approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional Conjoint Health Research Ethics Board (CHREB) certificate number REB17–2377.
Informed Consent
Informed consent was obtained from all participants included in the study as well as from the parents of minor participants.
Code Availability
Not Applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Stein, J.A., Tomfohr-Madsen, L.M., Bray, S. et al. Self-acceptance and nonreactive observing predict adolescent psychopathology over and above the big five. Curr Psychol 41, 7185–7199 (2022). https://doi.org/10.1007/s12144-020-01291-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-020-01291-1