
Abstract
Little is known about how school and community conditions may impact the mental well-being of children with incarcerated parents. The present study investigates whether adverse childhood experiences (ACEs) measured at the family, school, and community levels explain the relationship between having incarcerated parents during childhood and mental health of young adults. Across four waves of data from the National Longitudinal Study of Adolescent to Adult Health (Add Health), 6,986 participants who were in grades 7–12 completed questionnaires on various sociodemographic, criminological, and health metrics. Results indicate that children with incarcerated parents are prone to depression, and the more often a parent has been incarcerated, the higher the level of depression for the child. Moreover, the more times a parent was incarcerated, the more likely other adversities are present. The school context provides a unique lens to explore the relationship between parental incarceration and depression. Inadequate school resources amplified the negative effects of parental incarceration on mental health. Taken together, the results of this study underscore how parental incarceration is a distinctly harmful childhood experience, and this work expands previous findings that experiencing parental incarceration during childhood has long-term, generational consequences to mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Millions of children are impacted by the ways the United States (US) defines, prosecutes, and punishes crime, especially when their parents are jailed and imprisoned. The emergence and consequences of mass incarceration over the last four decades are unseen by vast swaths of the public. Over half of the estimated 2.3 million incarcerated people, in jails, prisons, juvenile correctional facilities, immigration detention facilities, and settings such as military prisons and state psychiatric hospitals, have children (Sawyer & Wagner, 2020). Over the past two decades, studies have found that over half of the imprisoned population are parents of minor children (Glaze & Maruschak, 2008; Mumola, 2000; National Resource Center on Children & Families of the Incarcerated, 2014). More recently, one study estimates that over five million children under age 18 have lost a residential parent to criminal custody at some point in their childhoods (Murphey & Cooper, 2015). Incarcerated women are more likely to be parents than incarcerated men (Arditti & McGregor, 2019) and women, while a minority of the imprisoned population, are a fast growing demographic within the punishment system (The Sentencing Project, 2020).
The experiences of children whose parents have been under criminal justice system control, including via incarceration, is increasingly recognized as a wide-ranging and deeply impactful social fact (Condry & Scharff Smith, 2018; Eddy & Poehlmann-Tynan, 2019; Wakefield & Wildeman, 2013). Extensive research shows that children of incarcerated parents typically experience multiple harms when a parent or caregiver (including a custodial guardian and/or a financial provider) is incarcerated (Gabel & Johnston, 1995; Glaze & Maruschak, 2008; Martin, 2017). Children with imprisoned parents often face wide-ranging mental health problems, connected to disadvantages prior to, during, and following a parent’s incarceration (Craigie et al., 2018; Poehlmann-Tynan et al., 2018; Smyke et al., 2017; Western & Smith, 2018; Wildeman & Turney, 2014). Research also highlights other negative outcomes faced by children whose parents are jailed or imprisoned. These include physical, educational, and socioeconomic problems as well as a higher likelihood of exposure to violence and the criminal justice system (Eddy & Poehlmann-Tynan, 2019; Foster & Hagan, 2015; Smyke et al., 2017; TenEyck et al., 2021; Wakefield & Uggen, 2010; Western, 2018; Wildeman & Turney, 2014).
Previous research has identified negative mental health outcomes for young adults who had a parent incarcerated during their childhood (Miller & Barnes, 2015). In fact, prior work has recognized parental incarceration as an adverse child experience (ACE). ACEs are negative and usually traumatic occurrences during childhood grouped in three categories: abuse, neglect, and household dysfunction (Reavis et al., 2013). The relationship between imprisoned parents and harm to their children is complex. For instance, poor mental health may have been influenced by their parents prior to incarceration, including experiences that were precursors to or causes of parental incarceration. These may include ACEs such as a child going through parental divorce or separation; living with someone who has a substance abuse problem; is mentally ill or is suicidal; witnessing domestic violence; or, experiencing the death of a caretaker (Sacks & Murphey, 2018). Moreover, little is known about how school and community conditions may impact the mental well-being of children with incarcerated parents. To address limitations in the extant literature on this topic, the current study relies on cohort data from National Longitudinal Study of Adolescent to Adult Health (Add Health) to explore (1) how parental incarceration, a distinct criminological adverse childhood experience, is related to depression levels among their offspring as they transition into young adulthood, (2) how parental incarceration is related to other ACEs, and (3) whether school and community conditions alter how parental incarceration is related to depression. By separating out the distinct criminological ACE of parental incarceration from other ACEs, this study can provide practical policy implications in addition to providing further evidence of the damage to children when parents are incarcerated. Further, focusing on the school and neighborhood context allows for a greater understanding of the cascading and layered vulnerabilities faced by children and parents affected by incarceration, captured in part by Western’s notion of human frailty (Western, 2018) and Middlemass’s term social disability (Middlemass, 2017). Among the reasons to better understand the impact of losing a parent to penal custody is the sheer scale of carcerality in the United States, as well as its disproportionate effects upon distinct demographic groups in society.
Parental Incarceration
Counting the number of children under 18 who have an incarcerated parent, or counting imprisoned people with minor children, is a difficult exercise. Some studies focus on fathers (Andersen & Wildeman, 2014), some on mothers (Arditti, 2015; Myers et al., 1999; Roberts, 2012), and some on all parents (Foster & Hagan, 2015). Some measures focus only on prisons while others include jails. A 2015 study identified over five million children, or 7% of US children, as having had a parent with whom they lived be removed to jail or prison, but underestimates parental incarceration because it excludes non-residential parents (Murphey & Cooper, 2015). While certain correctional departments collect data about who in their custody are parents, tracking is not systematic or accurate. For example, parents may not disclose information for different reasons, including privacy or fearing the child welfare system (Davis & Shlafer, 2017; Nesmith & Ruhland, 2011).
Children with parents under different forms of criminal justice system control (e.g. arrest, pre-trial detention, prison, parole) typically experience stress related to parental carceral status. The jailing or imprisonment of a parent is likely the most consequential of these experiences for children, primarily because of the duration of the separation (Annie E. Casey Foundation, 2011; Martin, 2017; Phillips et al., 2010). Indeed, long sentences are a distinctive characteristic of US imprisonment (Mauer, 2018); over half of parents in state prisons are incarcerated for one to five years and 20% of parents are not expected to be released for more than five years, if at all (Nesmith & Ruhland, 2011). Importantly, many parents cycle in and out of jail, prison, and related institutions like residential drug treatment programs or psychiatric hospitals (Genty, 2012).
When children turn 18 they are still impacted by parental incarceration (Davis & Shlafer, 2017). About a third of the children whose parents are incarcerated and who are placed with alternative caregivers will turn 18 before their parents are released (Nesmith & Ruhland, 2011). In other words, “the substantially increased risk for poor mental health associated with parental incarceration is not limited to the time during which [a] parent is imprisoned” (Davis & Shlafer, 2017, p. 129; see also Craigie et al., 2018), nor to being a legal minor.
Research overwhelmingly suggests that most consequential outcomes of parental imprisonment are direct and harmful, from poverty to diminished school performance and beyond (Wakefield & Wildeman, 2013). Family incomes decline, family costs increase, homelessness and housing insecurity increase, and educational, behavioral, and health outcomes decline. Internalizing problems such as depression and anxiety as well as externalizing problems like aggression and delinquency are significant consequences of parental incarceration for both younger and older children (Murray et al., 2012; National Research Council, 2014; Wildeman & Wang, 2017). There are nuances and complexities in the individual studies such as racialized group variations (Craigie, 2011; Gaston, 2016), particular foci like aggression or gender differences (Emory, 2018; Geller et al., 2009; Wakefield & Wildeman, 2011), or risk of drug use or exposure to sexually transmitted diseases (Khan et al., 2018). Parental incarceration may have indirect effects, such as unhealthy weight increase (Roettger & Boardman, 2012), greater risks of homelessness, and sexual assault for daughters of incarcerated fathers (Foster & Hagan, 2007). Only a minority of children benefit from parental incarceration. Where a caregiver is a source of negative childhood experiences (such as abuse), incarceration may provide some relief as well as, or in contrast to, negative mental health repercussions (Arditti, 2015; Wildeman & Turney, 2014).
Parental absence due to incarceration increases children’s exposure to risks of mental health harms. Particular facts, such as the frequency or timing of the parent’s imprisonment, or the child’s relationship to the incarcerated person, may also be impactful. In some research, the timing of incarceration or having a father incarcerated is associated with problem behaviors for their children (Gabel, 1992; Kjellstrand & Eddy, 2011), while in other studies, having a mother incarcerated is associated with drug use and depression (Murray & Farrington, 2008; Murray et al., 2012). Being an adolescent with a parent in prison might increase risks of depression (Foster & Hagan, 2013). One study found that among those children who seek out professional mental health treatment, parental incarceration may limit the success of such treatment (Phillips et al., 2002). Diminished mental health is also often increased by other factors related to parental incarceration such as poverty, parental substance abuse, and neglect (Nikulina et al., 2011; Widom & White, 1997). The number of times a parent has been incarcerated is likely to be a chronic stressor that affects child health (Massoglia & Pridemore, 2015).
Intersecting Disadvantage and Parental Incarceration
Multiple identities and demographic characteristics, including age, financial status, racialized group membership, gender, and health, intersect in how parental incarceration affects children. First, parenting and incarceration overlap because of age. Violent, property, and drug crime, is disproportionately committed by young people. Age is well-established as one of the most important factors influencing engagement in, or desistance from, crime (Ulmer & Steffensmeier, 2014). Additionally, becoming a parent is significantly influenced by age. Slightly fewer than 50% of fathers, and a little more than 50% of mothers in prison were under 24 (Annie E. Casey Foundation, 2016). The median age of parents in state prisons in 2000 was 32 in the late 1990s (Mumola, 2000), but average parental age has increased in the intervening decades due to much longer sentences (Bureau of Prisons, 2020; Courtney et al., 2017; Kaeble, 2018).
Second, crime and punishment are profoundly linked with material disadvantage, arguably a stronger measure than socioeconomic status (SES) (Bellair et al., 2019; Western, 2018). Low SES, associated with low income as well as educational and occupational status, has long been linked to higher levels of crime and punishment. Material hardship is more than a potentially short-term state of low or no income; instead, it is more all-encompassing, involving the continuing inability to afford life necessities. In turn, this deprivation creates persistent economic stress that undermines family and parental social control (Bellair et al., 2019). Bellair and colleagues (2019) found that greater material hardship relates to higher levels of parental incarceration. Imprisoned people are dramatically concentrated at the lowest ends of the national income distribution (Rabuy & Kopf, 2015). Poverty and material disadvantage can be criminogenic, contributing “not just to street crime but also to family violence, child neglect, and fighting among youth” (Western, 2018, p. 67).
Third, racialized group membership is a critical indicator of who is most likely to face imprisonment and, more broadly, be subject to criminal justice control (Alexander, 2012; Wacquant, 2009; Western, 2006). As the Sentencing Project notes, “African Americans are more likely than white Americans to be arrested; once arrested, they are more likely to be convicted; and once convicted, and they are more likely to experience lengthy prison sentences” (2018, p. 1). Incarceration rates for less serious offenses “are not well explained by high crime rates” (Western, 2006, p. 50). Violent crime tends to reflect and reinforce inequalities and often an overlap between victims and offenders shaped by contexts such as trauma, poverty, racism, and familial disruption (Berg & Schreck, 2022; Delong & Reichert, 2019; Western, 2018). The impact of poverty and structural racism on crime, criminal justice systems, victimization, and collateral consequences are both distinct and intertwined. Being Black, Latinx, and Native American, as well as being young, minimally educated, and poor, dramatically increases the likelihood of incarceration (Daniel, 2020; National Research Council, 2014; Western, 2006). One reason for this pattern is that the schools which serve mostly youth of color are more likely to be under-resourced overall and the resources they do have are often invested more in policing than supporting students (American Civil Liberties Union, 2019). These processes are captured in the metaphor of the school to prison pipeline which highlights how educational system choices influence exposure to or capture by criminal justice system apparatuses (McGrew, 2016): The “school-to-prison pipeline reinforces elements of racial segregation, penalizes students of color with disproportionate ACEs, and functions to exclude them from the educational process by redirecting them into the criminal justice system” (Carr, 2020, p. 116). Absent incarcerated parents, disproportionately Black, are even less able to support their already vulnerable children.
Fourth, gender shapes incarceration and its consequences. Being male exacerbates risks of entry into juvenile and adult criminal justice systems; the vast majority of incarcerated people are men. The rate of growth of women’s incarceration (as well as other juvenile and criminal justice system’s entanglements) is very much higher than men’s (The Sentencing Project, 2020). Further, women are disproportionately more likely than men to go to jail rather than prison, whether for pre-trial detention or misdemeanor convictions (Arditti, 2015). Imprisoned parents are more often women than men, particularly custodial parents (Arditti & McGregor, 2019). In 2004, more than half of incarcerated mothers stated they were providing the primary financial care for their children the month before their arrest (Roberts, 2012). Maternal incarceration both reflects and reinforces greater negative outcomes for children with parents in custody so that gender distinction is important (Foster & Hagan, 2015). Although fathers are incarcerated at much higher rates, it is maternal incarceration that has the greatest impact on children of incarcerated parents (Wildeman et al., 2018).
Fifth, incarcerated people are more likely to have physical and/or mental illnesses than the comparable public at large, often related to problems of substance abuse. Cumulative disadvantage (Kurlychek & Johnson, 2019), and the above noted ideas of human frailty (Western, 2018) and social disability (Middlemass, 2017), capture these compounding and overlapping harms. Dominant socio-legal and cultural portrayals of imprisoned people emphasize imprisoned people as dangerous. Indeed, most people subject to penal punishment have harmed others, directly and indirectly. Simultaneously, however, the majority of people in jail and prisons have also experienced trauma, usually through factors such as material hardship, violence, mental illness, and substance abuse. In addition, imprisoned people are far more likely to have ACEs than the general population (Briere et al., 2016; Henry, 2020; Roos et al., 2016; Tripodi & Pettus-Davis, 2013; Wolff & Shi, 2012). In particular, past studies of incarcerated women show a high prevalence of ACEs, such as physical victimization and sexual victimization prior to age 18 (Logan-Greene et al., 2014; Tripodi & Pettus-Davis, 2013; Wolff et al., 2020). Imprisonment, parenting, and mental health problems are bound up with “intergenerational, intersectional, and interinstitutional” histories and realities of “social inequality and systemic exclusion” (Foster & Hagan, 2015, p. 136).
These compounding disadvantages provide a reminder that concerns for children of incarcerated parents should not assume that those mothers and fathers are all simply bad parents who malignly harm their children. Children are usually hurt by their parent’s incarceration. Parents in prison are themselves likely to have experienced material deprivation, childhoods exposed to mental illness and substance abuse, racial and/or other discrimination, as well as victimization, including through violent crime (Roos et al., 2016).
Adverse Childhood Experiences (ACEs) and Incarceration
Extensive evidence shows that exposures to ACEs are associated with unhealthy behaviors such as increased use of alcohol and drugs (Anda et al., 2006), higher likelihood of unemployment (Liu et al., 2013), and poor physical and mental health (Wakefield & Wildeman, 2013). Moreover, past studies have shown that experiences of adversity in childhood can negatively impact physical and mental health throughout the life course, including through exposure to the criminal justice system (Craig et al., 2020; Danese et al., 2009; Felitti et al., 1998; Nurius et al., 2015; Turner et al., 2006), and can enhance the risk of recidivism. In the United States, approximately half of children have at least one adverse experience; one in ten children experience three or more adversities (Sacks & Murphey, 2018). Reflecting the high rate of children who experience multiple adversities, many studies have focused on cumulative experiences, and assessed not only individual-level factors but also neighborhood or community-level childhood stressors (Schwartz et al., 2019; Wade et al., 2016).
This study argues that parental incarceration is a unique dimension of ACEs that needs further exploration, not only considering composite ACE measures. Parental incarceration is the sole criminological ACE measure often used in the literature, and the mental health consequences for having incarcerated parents may be different than other ACEs measures. Indeed, children with incarcerated parents are found to develop shame and stigma that differ from other forms of parental absence (Davies et al., 2008). Moreover, the effects of parental incarceration may vary by contextual dimensions of ACEs. Past work has shown the effects of ACEs are mitigated by higher levels of social cohesion or collective efficacy of school, neighborhood, or community environments (Longhi et al., 2021). Nevertheless, little is known about how the impact of having incarcerated parents on children may vary by school and neighborhood/community contexts. This is partly due to the reliance on a composite measure of ACEs in prior works. In the following analysis, this study fills this void by assessing the effect of distinct criminological ACE of parental incarceration on mental health and how the context may influence the association.
Data and Methods
The current study relies on restricted-use data from the National Longitudinal Study of Adolescent to Adult Health (Add Health). This longitudinal study of a nationally representative sample follows, to date, five waves of over 20,745 adolescents who were in grades 7 to 12 during the 1994–95 school year (Harris, 2013). Add Health has a complex sampling design that incorporates stratified, clustered, and school-based methods. The primary sampling frame was derived from the Quality Education Database. From this frame we selected a stratified sample of 80 high schools using probability proportionate to size (PPS) sampling. Each high school selected also had a feeder junior high school identified, leading to one school pair in each of the 80 communities. In the initial wave, more than 70 percent of the originally selected schools agreed to participate in the study. Replacement schools were selected within each stratum until an eligible school or school-pair was found. Overall, 79 percent of the schools contacted agreed to participate in the study (Harris, 2013). This research uses the first four waves of the Add Health dataset, which spans from 1994 to 2009 (when respondents were between age 24 and 32). By the fourth wave, 75.7% of the respondents participated. The first two waves of data were collected both in homes and schools; subsequent waves used home interviews with the now-adult respondents. Our research relies solely on the in-home interview data, which has a total sample size of 15,701. This study restricts the sample to respondents with complete data, leading to an analytic sample of 6,986 individuals across all four waves.
Depression
The outcome measure of interest in the current study is mental health, and, in particular, depression. In all four waves, respondents were asked to indicate the extent to which eight statements reflected their moods over the past seven to 30 days. Specifically, respondents were asked to rate on a scale of 0–3 the extent to which (1) You were bothered by things that usually don't bother you, (2) You could not shake off the blues, even with help from your family and your friends, (3) You were depressed, (4) You were sad, and (5) You were too tired to do things. Additionally, three positively-worded prompts were also included in the depression measure: (6) You enjoyed life, (7) You felt you were just as good as other people, and (8) How satisfied are you with your life as a whole? For the final question, the attributes ranged from 0–4 (i.e., a Likert scale). We created a depression scale from these eight statements. The last three measures were reverse-coded so that for all measures, higher values indicated more depressive symptoms. While we calculated both unstandardized and standardized depression scales, we relied on the standardized scale given that one of the items is scaled differently than the others (0–3 versus 0–4). The internal consistency (Cronbach’s alpha) of the standardized depression scale varies by wave, but it is quite high: (Wave 1 α = 0.74, Wave 2 α = 0.81, Wave 3 α = 0.81, and Wave 4 α = 0.84).
Parental Incarceration
This study is focused on the relationship between parental incarceration and mental health. We use the respondent’s self-report of their biological and/or custodial parents' direct interactions with the criminal justice system to create a measure of parental incarceration. At Wave 4, respondents were asked if their biological mother, biological father, mother-figure, or father-figure had ever spent time in jail or prison, as well as the number of times each of these parental figures spent time in jail or prison. From these measures, we created two parental incarceration variables. We first created a variable to indicate whether any parental figure was incarcerated. Second, we created a frequency variable to indicate the total maximum number of times any one of the parental figures was incarcerated. For example, if the biological mother was incarcerated once, the biological father was incarcerated twice, the mother-figure (such as a grandmother) was incarcerated three times and the father-figure (such as an uncle) was incarcerated once, the total maximum number of times that one parental figure was incarcerated would be three. We opted to include the total maximum number rather than the summed total of parental incarceration events because we are unable to account for residential histories for both parents and parental figures.
Adverse Childhood Experiences (ACEs)
One of the guiding hypotheses of the current study is that the effect of incarceration on depression is likely due to the concurrent ACEs that adolescents may experience. We include nine ACE measures in this study. All measures are coded as dichotomous variables. While past work created a composite variable using ACE measures (Brumley et al., 2017; Schwartz et al., 2019), this study includes all measures separately due to low Cronbach's alpha value obtained when we created a scale. Six ACE measures were collected at the individual level, asking respondents about histories of alcoholism, parental warmth (or lack thereof), communication, overall relationships with parents, experiences of physical and/or sexual abuse at particular points, family income levels, and any experience of foster care. The various waves posed different questions. The remaining three ACE measures are related to childhood neighborhood/community disadvantage and included whether a respondent attended an under-resourced school, was exposed to violence, or lived in a disadvantaged neighborhood. These community-level questions were asked in Wave 1. It is important to note that all ACE measures were collected prior to Wave IV, and the ACE measures used in this study are validated by prior work (Brumley et al., 2017; Schwartz et al., 2019).
Control Variables
We include several demographic and other literature-informed control variables to address confounding in the current study. We selected males to be the contrast category due to the slightly higher number of adolescent boys in the sample. The respondent’s race and ethnicity were measured using a series of dichotomous variables. These include non-Hispanic white, non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other, and Hispanic. Non-Hispanic white is the reference category in the analyses. Nativity, or whether the respondent was born in the United States, was included as a control variable. Respondent income was assessed in Wave 4. Education levels of the respondent at Wave 4, between ages 24 and 32, were collapsed into five categories: less than high school education, high school graduate (including GED), some college (including trade/professional schools), college graduate, and graduate/professional degree (whether or not their advanced degree was completed). To account for the number of caregivers in the home during the first two waves of data collection, we created a measure called single family home. One caregiver was given the value of 1 and two (or more) caregivers were given the value 0.
In addition, we controlled for familial and social experiences that may play a role in depression over time. A key question concerned parental death. Respondents were asked in Wave 4 to indicate the year that their parent (or parent figure) died. Respondents were also asked in Waves 1 and 2 about family or friend’s attempted or actual death by suicide during the preceding past 12 months. To measure relationship violence, in Wave 4 respondents were asked how often their named partner threatened them with violence, pushed or shoved them, or threw something that could hurt the respondent. The attributes are ordered from 0 to 6 where larger numbers correspond to greater frequency. We recoded this variable into a dichotomous variable indicating whether the respondent indicated any frequency of violence. That is, values greater than one were coded as 1 for the recoded variable. Those who were not currently partnered were given a value of 0, which also corresponds to no current relationship violence.
We created two measures of time: age, measured in years, and wave of data, which corresponds to the time of data collection. Both are highly collinear, so we were unable to use both variables. We rely on the wave of data collection (1–4) as the singular measure of time.
Analytic Strategy
The current study uses several analytic tools to explore the nature of the relationship among parental incarceration, ACEs, and depression. To get an overall sense of the sample distribution, we generate univariate statistics (means and percentages) for the analytic sample. These statistics are weighted by the survey weights included in Add Health. Next, we examine bivariate relationships for the ACE and depression measures by parental incarceration frequency. We sought to test whether, on average, depression increases with multiple parental incarcerations as well as whether the percentage of respondents who experience ACEs increases as the number of parental incarcerations rises. We divide parental incarceration frequency into three categories: none, one incarceration, and two or more incarcerations, and we test those bivariate relationships using ANOVA (for depression) and Chi-square tests of independence (for ACEs). These analyses are also weighted because of the complex sampling design of the study.
We utilize linear fixed-effects regression models in a multivariate framework to examine whether parental incarceration and ACEs are associated with depression over time for this cohort. We use the Add Health sampling weights and estimate these models using the svy commands in Stata MP, version 16.1 (Stata Statistical Software: Release 16, 2019) to adjust for the complex sampling design. The models are cumulative: Model 1 includes the wave of data collection to see the effect of time on depression and Model 2 adds parental incarceration to the previous model. While we ran analyses with both focal independent measures, we only present the results for whether a parental figure was ever incarcerated. The effect sizes were similar, so we chose the more statistically efficient model to present. Model 3 adds the ACE measures to see whether any effect of parental incarceration is attenuated by the inclusion of ACEs. The final model is the full model that includes the control measures. Lastly, we performed post-hoc interaction tests with race, gender, parental incarceration, and ACE measures.
Results
Table 1 presents descriptive statistics of the dependent and independent variables. Almost one fifth (17 percent) of adults in our sample had at least one incarcerated parent and the average number of parents incarcerated was 0.43. Poverty was the most reported adverse childhood experience (54 percent) among all ACEs. About 20 to 25 percent of respondents reported other ACEs such as low parental warmth, physical abuse, attending an under-resourced school, and residing in a community where respondents were exposed to violence.
All adversities were more likely to be experienced by respondents with parents who were incarcerated more than once (Table 2). While the difference in percentages of ACEs between respondents without incarcerated parents and those with parents who were incarcerated once is small, the difference for respondents with parents who were incarcerated more than once was stark. For instance, about one in five respondents reported low parental warmth, physical abuse, and attended under-resourced school compared to about two to four percent experienced such adversities by the remaining respondents. Accordingly, the mean of depression is the highest among those with parents who were incarcerated more than once.
The results of the weight linear fixed-effects regression analyses presented in Table 3 reveal that time is associated with low levels of depression but the effect becomes more positive over time (b = -0.10; p < 0.00 to b = -0.08; p < 0.00). That is, depression decreases on average across the waves, but this decrease weakens in models that include the predictors of interest and covariates. Moreover, having a parent who was ever incarcerated is associated with higher levels depression over time (b = 0.16; p < 0.00) but that effect decreases when adjusting for the presence of ACE (b = 0.09; p < 0.01) and confounders (b = 0.07; p < 0.01).
Of the nine ACE variables, there are only two that are not statistically related to depression levels, namely being placed in a foster home and living in a disadvantaged neighborhood. However, when adjusting for confounders, two additional ACE measures’ statistical significance is attenuated: having a parent with a history of alcoholism and being a victim of sexual abuse. The other five ACE measures are positively and statistically associated with depression: having parents who offer low parental warmth (b = 0.21; p < 0.00), being a victim of physical abuse (b = 0.10; p < 0.00), growing up in a poor household (b = 0.05; p < 0.01), attending an under-resourced school (b = 0.05; p < 0.05), and living in a neighborhood plagued with community violence (b = 0.09; p < 0.00) are all associated with higher levels of depression, net of other characteristics.
Model 4 from Table 3 also presents the effects of the confounders on depression levels after adjusting for time, parental incarceration, and ACEs. Males in the sample have lower levels of depression than females (b = -0.15; p < 0.00). Compared to non-Hispanic whites, non-Hispanic Blacks (b = 0.05; p < 0.05) and non-Hispanic Asians (b = 0.11; p < 0.05) are associated with higher levels of depression. Larger incomes are associated with lower levels of depression (b = -0.01; p < 0.01). The education categories used in this study show a monotonic decrease in depression. That is, compared to being a high school graduate, those who did not complete high school are associated with higher levels of depression (b = 0.07; p < 0.05), and respondents who completed some college (b = -0.04; p < 0.05), finished college (b = -0.11; p < 0.00), or attended post-baccalaureate training (b = -0.12; p < 0.00) were all associated with increasingly lower levels of depression. Having one parent in the home during adolescence is associated with a 0.06 increase in depression levels (p < 0.01). Finally, if the respondent had a family member or friend attempt suicide, their depression levels were 0.12 points higher than those respondents who did have, or did not know of any, family or friends who attempted suicide (p < 0.00).
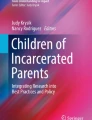
Furthermore, we assess multiple post hoc interaction effects: gender, race, parental incarceration, and ACEs. In unshown analyses, none of the gender-race interactions were statistically significant. Further, only one interaction between parental incarceration and the remaining ACEs proved to be statistically significant: parental incarceration and attending an under-resourced school was associated with depression levels (b = 0.60; p < 0.01). As shown in Fig. 1, the statistically positive effect of attending an under-resourced school on depression levels is larger for respondents whose parents have been incarcerated. In particular, the effect of 0 for individuals with parents who have never been incarcerated and attended a school with adequate resources is similar to the effect of 0.03 for those respondents whose parents have never been incarcerated but attended an under-resourced school. When the respondent’s parents have a history of incarceration, we see the effects on the respondent’s depression levels diverge. Respondents whose parents have been incarcerated but attended a school with adequate resources are associated with lower levels of depression compared to respondents whose parents have been incarcerated and attended an under-resourced school (0.06 and 0.70 respectively).

Parental Incarceration by Under-Resourced School Interaction
Discussion
This study used a nationally representative sample of adolescents as they transition into adulthood to test whether parental incarceration was associated with depression and whether adversities at school and neighborhood levels could potentially explain the relationship between parental incarceration and mental health. There are four important findings that emerged from this research. First, children with incarcerated parents are prone to depression, and the more often a parent has been incarcerated, the higher the level of depression for the child. This study confirms other research, mostly using different data sources, that also finds a relationship between parental incarceration and later experiences of depression (Jackson et al., 2021; Miller & Barnes, 2015). This result is consistent with prior work that found that children of incarcerated parents face wide-ranging mental health problems (Poehlmann-Tynan et al., 2019). These mental health problems can follow children into adulthood, especially if left unaddressed. This research found that at least into young adulthood, the age at Wave 4, parental incarceration during childhood has long-term effects. Unfortunately, we were unable to test how the timing and length of parental incarceration may impact depression levels. Parental incarceration at some developmental moments during childhood and adolescence may be more detrimental than at other times. Some research suggests that the timing of external factors, such as a rise or decline in SES, can influence later life health outcomes (Jones, 2018). Future research should attempt to locate how potential timing issues of parental incarceration may affect mental health outcomes of their children.
Second, the more times a parent was incarcerated, the more likely other ACEs are present. The frequency of incarcerations was associated with both increased levels of depression and increased presence of other ACE measures, and this relationship was monotonic (i.e., each additional incarceration of a parent was associated with a higher number of ACEs experienced by respondents). The relationship between the ACE of parental incarceration and other ACEs therefore needs to be studied further. Still, the relationship between parental incarceration frequency and related adverse childhood experiences underscores the extensive literature which shows that multiple interactions with the criminal justice system are connected to cumulative disadvantage. While it is true that parental incarceration during childhood is linked to ACEs, the causal pathway that links these experiences is unknown. Nevertheless, these results suggest that intervening in one of these experiences, like parental incarceration, could potentially improve life quality because of its potential to precipitate the chances of experiencing other ACEs. Intervening or preventing one ACE is unlikely to cancel out all the effects of having other adverse experiences. While the frequency of parental incarcerations is a novel finding of this research, we do not yet know whether or how the duration of each incarceration of a parent is linked to ACEs. New research should be conducted to explore how the frequency, timing, and duration of incarceration are related to both depression and ACEs.
Third, parental incarceration is a distinctly harmful ACE that has an effect even when controlling for other ACEs and confounders. This finding could suggest that parental incarceration directly contributes to depression levels among children. (Conversely, this finding may also point to other measures through which parental incarceration operates that were not included in this study.) There are a couple of plausible explanations for this finding. Substantively, parental incarceration can take a caregiver out of the home, and complicate the definition of a family. Other types of parental absences (such as death, military deployment, or relationship dissolution), and experiences of ambiguous loss (Bocknek et al., 2009; Boss, 2016; Brown & Coker, 2019), may too produce similar effects on depression. Ambiguous loss involves relational stress in response to an ongoing trauma (Brown & Coker, 2019). However, these types of absences are unlikely to be tied to ACEs in the same way as parental incarceration, which typically involves numerous and ongoing ACEs. As Bocknek et al. note, children of prisoners experience parental loss and trauma uniquely “because of the complex family issues and instability experienced before, during and after their parent’s incarceration” (2009, p. 324). Methodologically, the ACE variables were dichotomous rather than continuous, so the measures do not fully showcase the variation in these experiences, which is another explanation for this finding. If this study could have used continuous measures of ACEs, the parental incarceration effect may have been attenuated. Similar to the argument that the timing of parental incarceration may affect depression levels, the timing of the ACE measures (which were not directly assessed), particularly when the incarceration took place, may have provided stronger evidence of the ACEs being indirect mediators in the relationship between incarceration and mental health. These are only conjectures for future research to test whether or how parental incarceration has direct or indirect relationships with later life depression.
Fourth, inadequate school resources, an ACE context measure, amplified the negative effects of parental incarceration on mental health. The effect of parental incarceration on depression remained low if the child went to a school that was not under-resourced. Importantly, the effect of parental incarceration on depression was greater for children who went to under-resourced schools. This conditional effect may be explained through the lens of cumulative disadvantage. For example, families of children of incarcerated parents commonly face economic disadvantage (Geller et al., 2009; Western, 2018). Thus, it may not just be that parental incarceration relates to adverse outcomes; instead, additional challenges may intensify the experience of parental incarceration (Jackson et al., 2021; Travis & Waul, 2003). While this research did not find other conditional effects of having incarcerated parents partly due to small sample size, future research should further examine the way in which characteristics of parents as well as children, including age, race, gender, socio-economic status, affect the impact of parental incarceration on children.
This research is not without its limitations. Because the Wave 4 question about parental incarceration relies on the adult memory of a child, respondents’ memories, especially their understanding of what penal control their parent may have been subject to, could slightly under- or overstate the carceral experiences of their parent(s). The reduction in the number of respondents over the four waves, and the lack of complete data for all respondents, may point to another limitation, namely an undercount of respondents most affected by incarceration. Add Health researchers followed up with respondents who were in confinement under criminal justice system control, which increases the value of this data set. Nevertheless, the people most likely to be affected by incarceration, mental illness, and associated social ills of cumulative disadvantage are also more likely to be difficult for researchers to contact in follow up interviews for a longitudinal study. Commenting on those who are formerly incarcerated and other “hard-to-reach” populations, Western notes: “Survey nonresponse and study attrition can bias studies of former prisoners and other highly marginal groups” (2018, p. 11). The lack of qualitative data in this study is a related limitation. The inclusion of qualitative data and analysis may have supplied a more nuanced and complex discussion surrounding the impact of parental incarceration in tandem with the quantitative work supplied through the longitudinal study. This research identified clear relationships between parental incarceration, adverse childhood experiences, and depression in young adulthood, so a qualitative focus is the ideal next step to see the processes by which these three variables relate to one another.
Finally, the focus on only one aspect of mental health, depression, may be another limitation. Not only can comorbidity be a factor in an individual’s mental health but depression is only one mental illness and does not account for other diagnoses, such as bipolar disorder or anxiety. The relationships of parental incarceration to different diagnoses of physical and/or mental illness is worthy of study. Despite this potential limitation, a narrow focus on one mental health outcome provides clarity on the relations between incarceration, ACEs, and depression overall while also providing a foundation for further studies to focus on other mental health disorders, comorbidity, and their connection to parental incarceration.
Findings from this research can inform policy on at least three levels. First, at the individual level, this study shows the importance of identifying children of incarcerated parents. They are burdened by the stress and stigma of having an absent parent while simultaneously dealing with an enhanced risk of being depressed. Having incarcerated parents can additionally be a source a chronic stress for children, as the stigma of criminality and/or incarceration can move beyond the individual who committed the law-breaking acts to their family members (Davies et al., 2008; Murray & Farrington, 2008; Nesmith & Ruhland, 2011). In school settings, these individuals could be identified by mental health counselors or other professionals to receive the health care and social support that they need to deal with this change in their life. This work is being done in schools and private health care settings through trauma-focused cognitive behavioral therapy with children of incarcerated parents (Morgan-Mullane, 2018) and is discussed in counseling training manuals as part of continuing education learning experiences (Bennett et al., 2012). Given the pervasiveness of parental incarceration and this research finding regarding its tie to depression, a more widespread and national focus on this training and intervention strategy is essential.
Second, at the community level, this study highlights the importance of well-resourced schools in limiting depression. Of course, well-resourced schools may raise different concerns for children’s mental health access (Luthar et al., 2021), but children in under-resourced learning environments are likely to be subject to other cumulative disadvantages (including other ACEs) that take a mental toll on them. While we need increased funding for school systems to provide mental health services, the distribution of school funding to enable more equitable resources allocation is critical. In both of these recommendations, the key is to identify where the most vulnerable are – individuals and school systems – and finding ways to make sure they have the resources available to them to thrive.
Third, and perhaps most importantly, the US has overused imprisonment (and the criminal justice system more generally) to respond to social ills, including activities that are valuably or legitimately criminalized. As evidenced in this study, there are real, generational consequences for this tactic. Mental health is tangibly compromised or worsened when parents are incarcerated. When the prison system is the cure for crime, the cure can become worse than the disease, reinforcing or exacerbating disadvantage and inequality. How we define and respond to social harms needs to be rethought. Criminalization of certain social harms may exacerbate rather than stop or reverse the negative outcomes. Punishment approaches that perpetuate collateral consequences for vulnerable families need to be replaced by investments that redress economic, racial, health, and other inequalities. Imprisoning and jailing people, including parents, reflects and reinforces ACEs and other cumulative disadvantages, including by worsening the mental health of children who have parents in state custody, especially in the contexts of multiple incarcerations and under-resourced schools.
References
Alexander, M. (2012). The New Jim Crow: Mass incarceration in the age of colorblindness. The New Press.
American Civil Liberties Union. (2019). Cops But No Counselors: How the Lack of School Mental Health Staff Is Harming Students. American Civil Liberties Union. https://www.aclu.org/report/cops-and-no-counselors. Accessed 28 July 2022.
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C. L., Perry, B. D., Dube, S. R., & Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Child: Care, Health and Development, 32(2), 253–256. https://doi.org/10.1111/j.1365-2214.2006.00614_2.x
Andersen, S. H., & Wildeman, C. (2014). The Effect of Paternal Incarceration on Children’s Risk of Foster Care Placement. Social Forces, 93(1), 269–298. https://doi.org/10.1093/sf/sou027
Annie E. Casey Foundation. (2011). When a Parent is Incarcerated: A Primer for Social Workers. (pp. 1–34). Annie E. Casey Foundation. https://www.aecf.org/resources/when-a-parent-is-incarcerated/. Accessed 28 July 2022.
Annie E. Casey Foundation. (2016). A Shared Sentence: The devastating toll of parental incarceration on kids, families and communities. Annie E. Casey Foundation. https://www.aecf.org/resources/a-shared-sentence/. Accessed 28 July 2022.
Arditti, J. A. (2015). Family Process Perspective on the Heterogeneous Effects of Maternal Incarceration on Child Wellbeing Maternal Incarceration and Child Wellbeing: Policy Essay. Criminology & Public Policy, 14(1), [i]-184. https://heinonline.org/HOL/P?h=hein.journals/crpp14&i=173. Accessed 28 July 2022.
Arditti, J. A., & McGregor, C. M. (2019). A Family Perspective: Caregiving and Family Contexts of Children with an Incarcerated Parent. In J. M. Eddy & J. Poehlmann-Tynan (Eds.), Handbook on Children with Incarcerated Parents: Research, Policy, and Practice (pp. 117–130). Springer International Publishing. https://doi.org/10.1007/978-3-030-16707-3_9
Bellair, P. E., McNulty, T. L., Roscigno, V. J., & Lei, M. K. (Karlo). (2019). Childhood Material Hardship and Externalizing Behavior. Justice Quarterly, 0(0), 1–25. https://doi.org/10.1080/07418825.2019.1584326
Bennett, E., Lewis, M., & Hunsaker, E. (2012). Counseling Kids with Incarcerated Caregivers. In Ideas and Research You Can Use: VISTAS 2012. Retrieved June 8, 2022 from https://www.counseling.org/resources/library/vistas/vistas12/Article_56.pdf
Berg, M. T., & Schreck, C. J. (2022). The Meaning of the Victim–Offender Overlap for Criminological Theory and Crime Prevention Policy. Annual Review of Criminology, 5(1), annurev-criminol-030920–120724. https://doi.org/10.1146/annurev-criminol-030920-120724
Bocknek, E. L., Sanderson, J., & Britner, P. A. (2009). Ambiguous Loss and Posttraumatic Stress in School-Age Children of Prisoners. Journal of Child and Family Studies, 18(3), 323–333. https://doi.org/10.1007/s10826-008-9233-y
Boss, P. (2016). The Context and Process of Theory Development: The Story of Ambiguous Loss. Journal of Family Theory & Review, 8(3), 269–286. https://doi.org/10.1111/jftr.12152
Briere, J., Agee, E., & Dietrich, A. (2016). Cumulative Trauma and Current Posttraumatic Stress Disorder Status in General Population and Inmate Samples. Psychological Trauma: Theory, Research, Practice, and Policy, 8(4), 439–446. https://doi.org/10.1037/tra0000107
Brown, E. C., & Coker, A. D. (2019). Promoting the Resiliency of African American Teens Experiencing Ambiguous Loss. Journal for Specialists in Group Work, 44(4), 286–299. https://doi.org/10.1080/01933922.2019.1669751
Brumley, L. D., Jaffee, S. R., & Brumley, B. P. (2017). Pathways from Childhood Adversity to Problem Behaviors in Young Adulthood: The Mediating Role of Adolescents’ Future Expectations. Journal of Youth and Adolescence, 46(1), 1–14. https://doi.org/10.1007/s10964-016-0597-9
Bureau of Prisons. (2020). Inmate Age. https://www.bop.gov/about/statistics/statistics_inmate_age.jsp. Accessed 28 July 2022.
Carr, E. M. (2020). Educational Equality and the Dream That Never Was: The Confluence of Race-Based Institutional Harm and Adverse Childhood Experiences (ACEs) in Post-Brown America. Georgetown Journal of Law & Modern Critical Race Perspectives, 12(2), 115–142. https://heinonline.org/HOL/P?h=hein.journals/gjmodco12&i=123. Accessed 28 July 2022.
Condry, R., & Scharff Smith, P. (2018). Prisons, Punishment, and the Family Towards a New Sociology of Punishment? (Vol. 1). Oxford University Press. https://doi.org/10.1093/oso/9780198810087.001.0001
Courtney, L., Eppler-Epstein, S., Pelletier, E., King, R., & Lei, S. (2017). A Matter of Time: The Causes and Consequences of Rising Time Served in America’s Prisons. https://apps.urban.org/features/long-prisonterms/a_matter_of_time.pdf
Craig, J. M., Trulson, C. R., DeLisi, M., & Caudill, J. W. (2020). Toward an Understanding of the Impact of Adverse Childhood Experiences on the Recidivism of Serious Juvenile Offenders. American Journal of Criminal Justice, 45(6), 1024–1039. https://doi.org/10.1007/s12103-020-09524-6
Craigie, T.-A., Pratt, E., & McDaniel, M. (2018). Father Reentry and Child Outcomes. Urban Institute. https://www.urban.org/research/publication/father-reentry-and-child-outcomes. Accessed 28 July 2022.
Craigie, T.-A.L. (2011). The Effect of Paternal Incarceration on Early Child Behavioral Problems: A Racial Comparison. Journal of Ethnicity in Criminal Justice, 9(3), 179–199. https://doi.org/10.1080/15377938.2011.594349
Danese, A., Moffitt, T. E., Harrington, H., Milne, B. J., Polanczyk, G., Pariante, C. M., Poulton, R., & Caspi, A. (2009). Adverse childhood experiences and adult risk factors for age-related disease: Depression, inflammation, and clustering of metabolic risk markers. Archives of Pediatrics & Adolescent Medicine, 163(12), 1135–1143. https://doi.org/10.1001/archpediatrics.2009.214
Daniel, R. (2020). Since you asked: What data exists about Native American people in the criminal justice system? https://www.prisonpolicy.org/blog/2020/04/22/native/. Accessed 28 July 2022.
Davies, E., Brazzell, D., Vigne, N. G. L., & Shollenberger, T. (2008). Understanding the Experiences and Needs of Children of Incarcerated Parents (p. 14). Urban Institute, Justice Policy Center. https://www.urban.org/sites/default/files/publication/31486/411616-Broken-Bonds-Understanding-and-Addressing-the-Needs-of-Children-with-Incarcerated-Parents.PDF
Davis, L., & Shlafer, R. J. (2017). Mental health of adolescents with currently and formerly incarcerated parents. Journal of Adolescence, 54, 120–134. https://doi.org/10.1016/j.adolescence.2016.10.006
Delong, C., & Reichert, J. (2019). The Victim-Offender Overlap: Examining the Relationship Between Victimization and Offending. ICJIA | Illinois Criminal Justice Information Authority. https://icjia.illinois.gov/researchhub/articles/the-victim-offender-overlap-examining-the-relationship-between-victimization-and-offending. Accessed 28 July 2022.
Eddy, J. M., & Poehlmann-Tynan, J. (Eds.). (2019). Handbook on children with incarcerated parents: Research, policy and practice (2nd ed. 2019.). Springer. https://link-springer-com.proxygw.wrlc.org/book/10.1007%2F978-3-030-16707-3. Accessed 28 July 2022.
Emory, A. D. (2018). Explaining the Consequences of Paternal Incarceration for Children’s Behavioral Problems. Family Relations; Minneapolis, 67(2), 302–319. https://doi.org/10.1111/fare.12301
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Foster, H., & Hagan, J. (2007). Incarceration and Intergenerational Social Exclusion. Social Problems, 54(4), 399–433. https://doi.org/10.1525/sp.2007.54.4.399
Foster, H., & Hagan, J. (2013). Maternal and paternal imprisonment in the stress process. Social Science Research, 42(3), 650–669. https://doi.org/10.1016/j.ssresearch.2013.01.008
Foster, H., & Hagan, J. (2015). Punishment Regimes and the Multilevel Effects of Parental Incarceration: Intergenerational, Intersectional, and Interinstitutional Models of Social Inequality and Systemic Exclusion. Annual Review of Sociology, 41(1), 135–158. https://doi.org/10.1146/annurev-soc-073014-112437
Gabel, K., & Johnston, D. (1995). Children of Incarcerated Parents. Lexington Books.
Gabel, S. (1992). Behavioral Problems in Sons of Incarcerated or Otherwise Absent Fathers: The Issue of Separation. Family Process, 31(3), 303–314. https://doi.org/10.1111/j.1545-5300.1992.00303.x
Gaston, S. (2016). The Long-term Effects of Parental Incarceration: Does Parental Incarceration in Childhood or Adolescence Predict Depressive Symptoms in Adulthood? Criminal Justice and Behavior, 43(8), 1056–1075. https://doi.org/10.1177/0093854816628905
Geller, A., Garfinkel, I., Cooper, C. E., & Mincy, R. B. (2009). Parental Incarceration and Child Well-Being: Implications for Urban Families. Social Science Quarterly, 90(5), 1186–1202. https://doi.org/10.1111/j.1540-6237.2009.00653.x
Genty, P. M. (2012). Moving beyond generalizations and stereotypes to develop individualized approaches for working with families affected by parental incarceration. Family Court Review, 50(1), 36–47. https://doi.org/10.1111/j.1744-1617.2011.01426.x
Glaze, L. E., & Maruschak, L. M. (2008). Parents in Prison and Their Minor Children (NCJ 222984). Bureau of Justice Statistics. https://www.bjs.gov/index.cfm?ty=pbdetail&iid=823. Accessed 28 July 2022.
Harris, K. M. (2013). The Add Health Study: Design and Accomplishments. https://doi.org/10.17615/C6TW87
Henry, B. F. (2020). Typologies of Adversity in Childhood & Adulthood as Determinants of Mental Health and Substance Use Disorders of Adults Incarcerated in US Prisons. Child Abuse & Neglect, 99, 104251. https://doi.org/10.1016/j.chiabu.2019.104251
Jackson, D. B., Testa, A., Semenza, D. C., & Vaughn, M. G. (2021). Parental Incarceration, Child Adversity, and Child Health: A Strategic Comparison Approach. International Journal of Environmental Research and Public Health, 18(7), 3384. https://doi.org/10.3390/ijerph18073384
Jones, A. (2018). Race, Socioeconomic Status, and Health during Childhood: A Longitudinal Examination of Racial/Ethnic Differences in Parental Socioeconomic Timing and Child Obesity Risk. International Journal of Environmental Research and Public Health, 15(4), 728. https://doi.org/10.3390/ijerph15040728
Kaeble, D. (2018). Time Served in State Prison, 2016 (NCJ 252205; pp. 1–6). Bureau of Justice Statistics. https://www.bjs.gov/index.cfm?ty=pbdetail&iid=6446. Accessed 28 July 2022.
Khan, M. R., Scheidell, J. D., Rosen, D. L., Geller, A., & Brotman, L. M. (2018). Early age at childhood parental incarceration and STI/HIV-related drug use and sex risk across the young adult lifecourse in the US: Heightened vulnerability of black and Hispanic youth. Drug and Alcohol Dependence, 183, 231–239. https://doi.org/10.1016/j.drugalcdep.2017.11.006
Kjellstrand, J. M., & Eddy, J. M. (2011). Parental Incarceration During Childhood, Family Context, and Youth Problem Behavior Across Adolescence. Journal of Offender Rehabilitation, 50(1), 18–36. https://doi.org/10.1080/10509674.2011.536720
Kurlychek, M. C., & Johnson, B. D. (2019). Cumulative Disadvantage in the American Criminal Justice System. Annual Review of Criminology, 2(1), 291–319. https://doi.org/10.1146/annurev-criminol-011518-024815
Liu, Y., Croft, J. B., Chapman, D. P., Perry, G. S., Greenlund, K. J., Zhao, G., & Edwards, V. J. (2013). Relationship between adverse childhood experiences and unemployment among adults from five US states. Social Psychiatry and Psychiatric Epidemiology, 48(3), 357–369. https://doi.org/10.1007/s00127-012-0554-1
Logan-Greene, P., Green, S., Nurius, P. S., & Longhi, D. (2014). Distinct contributions of adverse childhood experiences and resilience resources: a cohort analysis of adult physical and mental health. Social Work in Health Care, 53(8), 776–97. https://doi.org/10.1080/00981389.2014.944251
Longhi, D., Brown, M., & Fromm Reed, S. (2021). Community-wide resilience mitigates adverse childhood experiences on adult and youth health, school/work, and problem behaviors. American Psychologist, 76(2), 216–229. https://doi.org/10.1037/amp0000773
Luthar, S. S., Ciciolla, L., & Suh, B. C. (2021). Adverse childhood experiences among youth from high-achieving schools: Appraising vulnerability processes toward fostering resilience. American Psychologist, 76(2), 300–313. https://doi.org/10.1037/amp0000754
Martin, E. (2017). Hidden Consequences: The Impact of Incarceration on Dependent Children. National Institute of Justice Journal, 278, 7. https://nij.gov/journals/278/Pages/impact-ofincarceration-on-dependent-children.aspx. Accessed 28 July 2022.
Massoglia, M., & Pridemore, W. A. (2015). Incarceration and Health. Annual Review of Sociology, 41(1), 291–310. https://doi.org/10.1146/annurev-soc-073014-112326
Mauer, M. (2018). Long-Term Sentences: Time to Reconsider the Scale of Punishment. The Sentencing Project, 87(1), 1–19. https://www.sentencingproject.org/wp-content/uploads/2018/11/UMKC-Law-Review-Scale-of-Punishment.pdf. Accessed 28 July 2022.
McGrew, K. (2016). The Dangers of Pipeline Thinking: How the School-To-Prison Pipeline Metaphor Squeezes Out Complexity. Educational Theory, 66(3), 341–367. https://doi.org/10.1111/edth.12173
Middlemass, K. (2017). Convicted and condemned: The politics and policies of prisoner reentry. New York University Press.
Miller, H. V., & Barnes, J. C. (2015). The Association Between Parental Incarceration and Health, Education, and Economic Outcomes in Young Adulthood. American Journal of Criminal Justice, 40(4), 765–784. https://doi.org/10.1007/s12103-015-9288-4
Morgan-Mullane, A. (2018). Trauma Focused Cognitive Behavioral Therapy with Children of Incarcerated Parents. Clinical Social Work Journal, 46(3), 200–209. https://doi.org/10.1007/s10615-017-0642-5
Mumola, C. J. (2000). Incarcerated Parents and Their Children (p. 12). https://www.sentencingproject.org/wp-content/uploads/2016/01/Incarcerated-Parents-and-Their-Children-Trends-1991-2007.pdf
Murphey, D., & Cooper, P. M. (2015). Parents Behind Bars: What Happens to Their Children? Child Trends, Inc. https://nicic.gov/parents-behind-bars-what-happens-their-children. Accessed 28 July 2022.
Murray, J., & Farrington, D. P. (2008). The Effects of Parental Imprisonment on Children. Crime and Justice, 37(1), 133–206. JSTOR. https://doi.org/10.1086/520070
Murray, J., Farrington, D. P., Sekol, I., & Olsen, R. F. (2012). Systematic Review of the Effects of Parental Imprisonment on Child Antisocial Behavior and Mental Health, 1960–2008: Version 1. ICPSR - Interuniversity Consortium for Political and Social Research. https://doi.org/10.3886/ICPSR31704.V1
Myers, B. J., Amlund-Hagen, K., Smarsh, T., & Kennon, S. (1999). Children of Incarcerated Mothers (No. 1). 8(1), 15. https://springerlink.bibliotecabuap.elogim.com/content/pdf/10.1023/A:1022990410036.pdf. Accessed 28 July 2022.
National Research Council. (2014). The Growth of Incarceration in the United States: Exploring Causes and Consequences. https://doi.org/10.17226/18613
National Resource Center on Children & Families of the Incarcerated. (2014). Children and Families of the Incarcerated Fact Sheet [Fact sheet]. Rutgers. https://nrccfi.camden.rutgers.edu/resources/fact-sheets/. Accessed 28 July 2022.
Nesmith, A., & Ruhland, E. (2011). Caregivers of Children with Incarcerated Parents. The Open Family Studies Journal, 4(1), Article 1. https://benthamopen.com/contents/pdf/TOFAMSJ/TOFAMSJ-4-105.pdf. Accessed 28 July 2022.
Nikulina, V., Widom, C. S., & Czaja, S. (2011). The role of childhood neglect and childhood poverty in predicting mental health, academic achievement and crime in adulthood. American Journal of Community Psychology, 48(3–4), 309–321. https://doi.org/10.1007/s10464-010-9385-y
Nurius, P. S., Green, S., Logan-Greene, P., & Borja, S. (2015). Life course pathways of adverse childhood experiences toward adult psychological well-being: A stress process analysis. Child Abuse & Neglect, 45, 143–153. https://doi.org/10.1016/j.chiabu.2015.03.008
Phillips, S. D., Burns, B. J., Wagner, H. R., Kramer, T. L., & Robbins, J. M. (2002). Parental Incarceration Among Adolescents Receiving Mental Health Services. Journal of Child and Family Studies, 11(4), 385–399. https://doi.org/10.1023/A:1020975106679
Phillips, S. D., Venema, R., & Roque, L. (2010). The Unmet Need for Mental Health Services Among Probationers’ Children. Journal of Offender Rehabilitation, 49(2), 110–125. https://doi.org/10.1080/10509670903534845
Poehlmann-Tynan, J., Runion, H., Weymouth, L. A., & Burnson, C. (2018). Children With Incarcerated Parents (T. H. Ollendick, S. W. White, & B. A. White, Eds.; Vol. 1). Oxford University Press. https://doi.org/10.1093/oxfordhb/9780190634841.013.33
Poehlmann-Tynan, J., Sugrue, E., Duron, J., Ciro, D., & Messex, A. (2019). Separation and Detention of Parents and Children at the Border: Lessons from Impacts of Parental Incarceration on Children and Families. In J. M. Eddy & J. Poehlmann-Tynan (Eds.), Handbook on Children with Incarcerated Parents: Research, Policy, and Practice (pp. 345–352). Springer International Publishing. https://doi.org/10.1007/978-3-030-16707-3_23
Rabuy, B., & Kopf, D. (2015, July 9). Prisons of Poverty: Uncovering the pre-incarceration incomes of the imprisoned. Prison Policy Initiative. https://www.prisonpolicy.org/reports/income.html. Accessed 28 July 2022.
Reavis, J. A., Looman, J., Franco, K. A., & Rojas, B. (2013). Adverse Childhood Experiences and Adult Criminality: How Long Must We Live before We Possess Our Own Lives? The Permanente Journal, 17(2), 44–48. https://doi.org/10.7812/TPP/12-072
Roberts, D. E. (2012). Prison, Foster Care, and the Systemic Punishment of Black Mothers. UCLA Law Review, 59(6), 1474–1501. https://www.uclalawreview.org/prison-foster-care-and-the-systemic-punishment-of-black-mothers-2/. Accessed 28 July 2022.
Roettger, M. E., & Boardman, J. D. (2012). Parental Incarceration and Gender-based Risks for Increased Body Mass Index: Evidence From the National Longitudinal Study of Adolescent Health in the United States. American Journal of Epidemiology, 175(7), 636–644. https://doi.org/10.1093/aje/kwr409
Roos, L. E., Afifi, T. O., Martin, C. G., Pietrzak, R. H., Tsai, J., & Sareen, J. (2016). Linking Typologies of Childhood Adversity to Adult Incarceration: Findings from a Nationally Representative Sample. The American Journal of Orthopsychiatry, 86(5), 584–593. https://doi.org/10.1037/ort0000144
Sacks, V., & Murphey, D. (2018). The prevalence of adverse childhood experiences, nationally, by state, and by race or ethnicity (Research Brief No. 2018–03). https://www.childtrends.org/publications/prevalence-adverse-childhood-experiences-nationally-state-race-ethnicity. Accessed 28 July 2022.
Sawyer, W., & Wagner, P. (2020). Mass Incarceration: The Whole Pie 2020 [Online.]. Prison Policy Initiative. https://www.prisonpolicy.org/reports/pie2020.html. Accessed 28 July 2022.
Schwartz, J. A., Wright, E. M., & Valgardson, B. A. (2019). Adverse childhood experiences and deleterious outcomes in adulthood: A consideration of the simultaneous role of genetic and environmental influences in two independent samples from the United States. Child Abuse & Neglect, 88, 420–431. https://doi.org/10.1016/j.chiabu.2018.12.022
Smyke, A. T., Bailey, L. O., & Zeanah, C. H. (2017). Mental Health Implications for Children of Incarcerated Parents Symposium. Loyola Law Review, 63(3), 405–434. https://heinonline.org/HOL/P?h=hein.journals/loyolr63&i=429. Accessed 28 July 2022.
Stata Statistical Software: Release 16. (2019). College Station, TX: StataCorp LLC.
TenEyck, M. F., Knox, K. N., & El Sayed, S. A. (2021). Absent Father Timing and its Impact on Adolescent and Adult Criminal Behavior. American Journal of Criminal Justice. https://doi.org/10.1007/s12103-021-09640-x
The Sentencing Project. (2018). Report to the United Nations on Racial Disparities in the U.S. Criminal Justice System. The Sentencing Project. https://www.sentencingproject.org/publications/un-report-on-racial-disparities/. Accessed 28 July 2022.
The Sentencing Project. (2020). Incarcerated Women and Girls [Fact sheet]. https://www.sentencingproject.org/publications/incarcerated-women-and-girls/. Accessed 28 July 2022.
Travis, J., & Waul, M. (2003). Prisoners Once Removed: The Impact of Incarceration and Reentry on Children, Families, and Communities. The Urban Institute.
Tripodi, S. J., & Pettus-Davis, C. (2013). Histories of childhood victimization and subsequent mental health problems, substance use, and sexual victimization for a sample of incarcerated women in the US. International Journal of Law and Psychiatry, 36, 30–40.
Turner, H. A., Finkelhor, D., & Ormrod, R. (2006). The effect of lifetime victimization on the mental health of children and adolescents. Social Science & Medicine, 62(1), 13–27. https://doi.org/10.1016/j.socscimed.2005.05.030
Ulmer, J. T., & Steffensmeier, D. (2014). The Age and Crime Relationship: Social Variation, Social Explanations. In K. Beaver, J. C. Barnes, & B. Boutwell (Eds.), The Nurture Versus Biosocial Debate in Criminology: On the Origins of Criminal Behavior and Criminality (pp. 377–396). SAGE Publications Ltd. https://doi.org/10.4135/9781483349114.n24
Wacquant, L. J. D. (2009). Punishing the poor: The neoliberal government of social insecurity. Duke University Press.
Wade, R., Cronholm, P. F., Fein, J. A., Forke, C. M., Davis, M. B., Harkins-Schwarz, M., Pachter, L. M., & Bair-Merritt, M. H. (2016). Household and community-level Adverse Childhood Experiences and adult health outcomes in a diverse urban population. Child Abuse & Neglect, 52, 135–145. https://doi.org/10.1016/j.chiabu.2015.11.021
Wakefield, S., & Uggen, C. (2010). Incarceration and Stratification. Annual Review of Sociology, 36(1), 387–406. https://doi.org/10.1146/annurev.soc.012809.102551
Wakefield, S., & Wildeman, C. (2011). Mass imprisonment and racial disparities in childhood behavioral problems. Criminology & Public Policy, 10(3), 793–817. https://doi.org/10.1111/j.1745-9133.2011.00740.x
Wakefield, S., & Wildeman, C. (2013). Children of the Prison Boom: Mass Incarceration and the Future of American Inequality | Sociology (1st ed.). Oxford University Press. https://sociology.yale.edu/publications/children-prison-boom-mass-incarceration-and-future-american-inequality. Accessed 28 July 2022.
Western, B. (2006). Punishment and Inequality in America. Russell Sage Foundation; JSTOR. https://www.jstor.org/stable/10.7758/9781610445559. Accessed 28 July 2022.
Western, B. (2018). Homeward: Life in the year after prison. Russell Sage Foundation.
Western, B., & Smith, N. (2018). Formerly Incarcerated Parents and Their Children. Demography, 55(3), 823–847. https://doi.org/10.1007/s13524-018-0677-4
Widom, C. S., & White, H. R. (1997). Problem behaviours in abused and neglected children grown up: Prevalence and co-occurrence of substance abuse, crime and violence. Criminal Behaviour and Mental Health, 7(4), 287–310. https://doi.org/10.1002/cbm.191
Wildeman, C., Haskins, A. R., & Poehlmann-Tynan, J. (2018). When parents are incarcerated: Interdisciplinary research and interventions to support children (First edition.). American Psychological Association.
Wildeman, C., & Turney, K. (2014). Positive, Negative, or Null? The Effects of Maternal Incarceration on Children’s Behavioral Problems. Demography, 51(3), 1041–1068. https://doi.org/10.1007/s13524-014-0291-z
Wildeman, C., & Wang, E. A. (2017). Mass incarceration, public health, and widening inequality in the USA. The Lancet, 389(10077), 1464–1474. http://dx.doi.org.proxygw.wrlc.org/https://doi.org/10.1016/S0140-6736(17)30259-3
Wolff, N., & Shi, J. (2012). Childhood and adult trauma experiences of incarcerated persons and their relationship to adult behavioral health problems and treatment. International Journal of Environmental Health Research, 9(5), 1908–26. https://doi.org/10.3390/ijerph9051908
Wolff, K. T., Baglivio, M. T., Klein, H. J., Piquero, A. R., DeLisi, M., & Howell, JC (Buddy). (2020). Adverse Childhood Experiences (ACEs) and gang involvement among juvenile offenders: Assessing the mediation effects of substance use and temperament deficits. Youth Violence and Juvenile Justice, 18(1), 24–53.
Acknowledgements
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgement is given to Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. No direct support was received from grant P01-HD31921 for this analysis. The authors would also like to acknowledge Samantha Brooks, Mansi Patel, and Rajesh Satpathy for their work on the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
No funding was received to assist with the preparation of this manuscript. Authors declare they have no financial interests. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Research involving Human Participants and/or Animals
The study was approved by the institutional review board at The George Washington University, and IRB certifies that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure of Potential Conflicts of Interest
The authors do not have any conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jones, A., Buntman, F., Ishizawa, H. et al. The Mental Health Consequences of Parental Incarceration: Evidence from a Nationally Representative Longitudinal Study of Adolescents through Adulthood in the United States. Am J Crim Just 49, 1–24 (2024). https://doi.org/10.1007/s12103-022-09689-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12103-022-09689-2