
Abstract
Objective
To validate effectiveness of low intensity, home based early intervention (EI) models in autism for countries with low disability resources.
Methods
Fifty-two toddlers and young children were assessed before and after intervention with Childhood Autism Rating Scale, Vineland Social Maturity Scale, and Receptive-Expressive Emergent Language Scale. Developmental and speech therapists helped mothers assemble low-cost training kits based on the developmental age of the child, gave initial training in the basic behavioral technique to address the three autism symptom clusters at home. Follow-up support was given either on a weekly, fortnightly or monthly basis. Most of the children were also placed in play-schools. Data was analyzed using appropriate bivariate and multivariate techniques.
Results
There was statistical and clinical amelioration in the severity of autism, with acquisition of social skills and language skills (all P = 0.001) after intervention in children with mild to severe autism. Gender showed a trend in becoming a significant predictor for intervention response.
Conclusions
Low-intensity, home-based EI can be effectively used in situations where there is paucity of disability resources in countries like India, especially in primary-care and community settings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Early interventions (EI) for Autism Spectrum Disorders (ASD) focus on all the three symptom clusters of ASD [1]. Dissimilar models, different sized programs in diverse settings, different countries, with slightly older children have been found to be effective for improving autism symptoms [2, 3]. A review shows that four out of five meta-analyses have concluded that EI also is effective in ASD. The mean effect sizes across meta-analyses was substantial for IQ and adaptive behavior gain with EI, which ranged from g = 0.38 to 1.19 and g = 0.30 to 1.09 respectively [4].
Nevertheless scientific community is uncertain about the universality of effectiveness of EI, as most EI are developed in the Western context [5]; while efficacy is proven, effectiveness of EI has not been substantiated in clinical settings [6]; and finally, it is clear that high intensity EI are more effective than low intensity EI [7]. However, it is clear that teaching ASD children in their natural environment, utilizing daily routines as teachable moments is the best practice [8]. It is necessary to validate such low intensity interventions that can be provided by the family members in countries with low health resources. Therefore, this study was conducted to document the effectiveness of a low intensity home based EI in India.
Material and Methods
This study was conducted at the Autism Evaluation Clinic, Child Development Centre, a regional referral centre in South India. Children ≤ 6 y with ASD diagnosed by a pediatrician and a developmental therapist and had enrolled for the home-training program was recruited in to this study.
The Childhood Autism Rating Scale (CARS) [9] scores were collected as an outcome measure to assess the amelioration of severity of autism following intervention and quantify the severity of autism. Vineland Social Maturity Scale (VSMS) [10] and Receptive-Expressive Emergent Language Scale (REELS) [11] were used to assess the effect of intervention on the adaptive skill and language skill acquisition. The pre intervention assessment with the CARS, VSMS and REEL was done by one of the developmental therapists (Post Graduate Diploma in Clinical Child Development holders). The same therapist assessed the participant with the same instruments after the intervention also independently. One of the four therapists administered the intervention and the other therapists were unaware of the intervention details. The study was reviewed and approved by the local Institutional Review Board of Child Development Centre.
The home EI had two components: firstly, the parental training that was given in the clinic after the pre-intervention assessments. Each parent was given skills to identify the developmental age of the child, and based on the identified developmental age, intervention kit was assembled with inexpensive materials that were available in the local market or at home. The parent was educated to train the child using simple behavioral strategies (e.g., prompt and rewards) in the areas of language, socialization and repetitive behaviors. Also, cognitive, academic, and prevocational skills essential to later school success were addressed. Strategy learned and used for each domain was noted down by the developmental therapist in the clinical record and by the parents in their handbook. Each clinical session took about 15–20 min and was given by Developmental Therapy trainees supervised by experienced Developmental Therapists. Parents were demonstrated about the intervention strategies and were advised to practice the same at home till the next visit. In addition, a speech therapist gave the parent 15 to 20-min session on an individual basis and targeted one or two language skills per visit for teaching at home. Following the clinical session of demonstration, depending upon the convenience of the parents, children were enrolled into different follow-up schedules, which were weekly, fortnightly or monthly drop-in follow-ups. The parent was encouraged to give the intervention every day at home. During each follow-up visit improvements in each domain was noted and recorded as ‘emerging’ or ‘attained’. Secondly, whenever possible the parent was advised to place the child with autism in a playschool or anganwadi to improve the group based stimulation of various target symptom clusters.
Descriptive analysis was used to express the participant characteristics. For establishing the improvement of autistic symptoms with intervention, pre and post intervention scores were compared with Wilcoxon matched pair rank test. The post-intervention differences between the mild and severe autism groups were analyzed using Mann–Whitney U test. For identifying the factors associated with intervention gain, linear multiple regression analyses were used with post-intervention total CARS score, VSMS-SQ, REEL-RQ and REEL-EQ as the dependent variable and chronological age, gender of child, pre-intervention total CARS score, VSMS-SQ, REEL-RQ as well as REEL-EQ as the independent variables using multiple linear regression analyses. P < 0.05 (two tailed test) was considered significant. Statistical analysis was performed using the SPSS (version 19).
Results
There were 42 (80.8 %) boys and 10 (19.2 %) girls in the sample. There mean (SD) age was 36.27 (14.14) mo (range of 22–108 mo). All parents involved in training were mothers. The mean (SD) period the child had undergone intervention was 6 (3.42) mo. The mean (SD) of time spent in home training by various family members was 4.2 (1.9) h per day and except 2 children all were in balwadi, anganwadi, or other types of play schools for 1–4 h per day . The means (SD) of pre-intervention CARS, VSMS, REEL-RQ and REEL-EQ scores are given in Table 1.
The intervention showed a clinically and statistically significant amelioration of severity of autism symptoms, and acquisition of social skills, receptive language and expressive language as reflected by the CARS, VSMS-SQ, REEL-RQ and REEL-EQ respectively (Table 1).
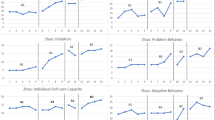
Analysis of specific CARS items demonstrated that there was statistically a significant change in the areas of relationship with people, imitation, affect, relation to nonhuman objects, adaptation to environmental changes, visual responsiveness, auditory responsiveness, verbal communication and non-verbal communication. There was a trend towards a statistically significant change post intervention in the areas of near receptor responsiveness and activity level. There was no change following intervention in the areas of use of body, anxiety reaction, intellectual functioning and general impression (Table 1).
When the intervention was compared for its effectiveness, there was no statistically significant difference in the absolute score difference in the CARS, VSMS-SQ, REEL-RQ and REEL-EQ total score between the participants with mild and severe autism, suggesting that the intervention was equally effective in helping those with as mild and severe autism (Table 2).
Gender of the child showed a trend towards contributing to the acquisition of Receptive language [β (SE) = −11.35 (6.32); P = 0.08] after controlling for the pre-intervention receptive language ability, which also significantly contributed to the expressive language acquisition [β (SE) = 0.64 (0.11); P = 0.001]. Similarly, gender showed a trend towards contributing to the acquisition of expressive language [β (SE) =−12.50 (6.85); P = 0.07] after controlling for the pre-intervention expressive language skills. Also, gender also significantly contributed to the expressive language acquisition [β (SE) = 0.74 (0.16); P = 0.001]. The age and pre-intervention developmental profile of the child did not contribute to the acquisition of language social skills or amelioration of the severity of autism.
Discussion
In this naturalistic observational study, low-intensity, home-based intervention was effective for reducing the severity of autism, gaining social skill and language ability. The intervention was equally effective for children with mild and severe autism. Only the gender of the child had some value in predicting the intervention response.
A low-intensity intervention (20 h per wk) based on Lovaas has also been found to be effective [12] and is comparable with the index study in its approach. More recently another study has documented similar improvement in children with autism and their parents with home training using TEACCH model [13]. In the index study with intervention there was mean (SD) reduction of CARS total score by 3.66 (0.98) suggesting that the overall severity of autism related symptoms have ameliorated. Similar findings have been documented by another Indian study where the nature of the intervention was also of moderate intensity (60–90 min per day with professional input and multiple family members when available was used) resulting in more significant reduction in CARS total score [14]. The gain in social skills is comparable with the previous Indian study despite the difference in the intensity of the input. Other forms of parent-mediated therapies have noted to improve the conversational ability, peer entry and exiting skill, developing friendship networks, good sportsmanship, good host behavior during get-togethers, changing bad reputations, and handling teasing, bullying, arguments, assertion, cooperation, and responsibility among children with autism [15]. Such specific skills were not addressed in the intervention or assessment in the index study. In the present study the language gains were seen in both the receptive and expressive areas of the child unlike the previous Indian study where the gains were noted in only the expressive domain [14]. The present intervention was equally effective in reducing autism symptoms in mild and severe form of illness. Despite being a prospective effectiveness study, it should be kept in mind that this was a naturalistic study and thus blinding of the raters and therapists to the intervention was not done, which is required for making a stronger association between the intervention and improvement. Conversely, the strength of the present study is that the naturalistic nature of the study lends support to the effectiveness than efficacy of the intervention. In conclusion, it is demonstrated that this low intensity, home based intervention can effectively address all the symptom clusters in autism and is useful in countries with low health resources.
References
Dingfelder HE, Mandell DS. Bridging the research-to-practice gap in autism intervention: an application of diffusion of innovation theory. J Autism Dev Disord. 2011;41:597–609.
Sallows GO, Graupner TD. Intensive behavioral treatment for children with autism: four-year outcome and predictors. Am J Ment Retard. 2005;110:417–38.
Handleman JS, Harris SL. Preschool education programs for children with autism. 3rd ed. Austin, TX: PRO-ED; 2008.
Reichow B. Overview of meta-analyses on early intensive behavioral intervention for young children with autism spectrum disorders. J Autism Dev Disord. 2012;42:512–20.
Freitag CM, Feineis-Matthews S, Valerian J, Teufel K, Wilker C. The Frankfurt early intervention program FFIP for preschool aged children with autism spectrum disorder: a pilot study. J Neural Transm. 2012;119:1011–21.
Bibby P, Eikeseth S, Martin NT, Mudford OC, Reeves D. Progress and outcomes for children with autism receiving parent-managed intensive interventions. Res Dev Disabil. 2002;23:81–104.
Dawson G, Rogers S, Munson J, Smith M, Winter J, Greenson J, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics. 2010;125:e17–23.
Meadan H, Ostrosky MM, Zaghlawan HY, Yu SY. Promoting the social and communicative behavior of young children with autism spectrum disorders: a review of parent-implemented intervention studies. Top Early Child Spec Educ. 2009;29:90–104.
Schopler E, Reichler RJ, Renner BR. Childhood Autism Rating Scale. Los Angeles: Western Psychological Services; 1988.
Doll EA. A Genetic Scale of Social Maturity. Am J Orthopsychiatry. 1935;5:180–8.
Bzoch KR, League R. Assessing language skills in infancy. Baltimore: University Park Press; 1971.
Birnbrauer JS, Leach DJ. The Murdoch Early Intervention Program after two years. Behav Chang. 1993;10:63–74.
Welterlin A, Turner-Brown LM, Harris S, Mesibov G, Delmolino L. The home TEACCHing program for toddlers with autism. J Autism Dev Disord. 2012;42:1827–35.
Juneja M, Mukherjee SB, Sharma S, Jain R, Das B, Sabu P. Evaluation of a parent-based behavioral intervention program for children with autism in a low-resource setting. J Pediatr Neurosci. 2012;7:16–8.
Laugeson EA, Frankel F, Gantman A, Dillon AR, Mogil C. Evidence-based social skills training for adolescents with autism spectrum disorders: the UCLA PEERS program. J Autism Dev Disord. 2012;42:1025–36.
Acknowledgments
The authors gratefully acknowledge the cooperation and support received from staff of Child Development Centre, Kerala, specially Dr. G. Suresh Kumar, Registrar; Ms. Deepa N.R., PS to Director; Mr. Asokan N, PA to Director; Ms. Suja S, Junior Programmer; CDC, Medical College, Thiruvananthapuram, in conduction of this study.
Conflict of Interest
None.
Source of Funding
This study is supported by Child Development Centre, Thiruvananthapuram.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Nair, M.K.C., Russell, P.S.S., George, B. et al. CDC Kerala 9: Effectiveness of Low Intensity Home Based Early Intervention for Autism Spectrum Disorder in India. Indian J Pediatr 81 (Suppl 2), 115–119 (2014). https://doi.org/10.1007/s12098-014-1474-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-014-1474-8