
Abstract
Objective
To examine the effect of parental training on disturbed behavior of early childhood cases presented to the pediatricians.
Methods
The patients who reported in pediatric OPD of the Himalayan Institute of Medical Sciences, Dehradun, with complaints of low learning, poor memory, vertigo, speech problem, stress, headache, depression, adjustment problems, aggression, and hostile behavior were included in the study. Children aged 3 through 6 (N = 60), were screened through PBQ (Preschool Behavior Questionnaire), DST (developmental screening Test), and Vineland Social Maturity Scale (VSMS). Children included in the study had an average range of developmental quotient 85–90 (mean DQ = 87.5). Range of social quotient was 40–45 (mean SQ = 42.5). Twenty four fortnightly sessions of ‘parental training’ using the model of ‘Mindful Parenting’ were conducted. Single group t test method was applied in order to see the difference in mean of pre and post assessment of PBQ.
Results
After concluding parental training (after 24 sessions), mean difference of total disturbed behavior was found to be significant (t value: 5.31 > .05) Similarly, the mean difference of hostile/aggressive behavior (t value: 10.2 > .05), anxious behavior (t value: 18.5 > .05), and hyperactive/distractible behavior (t value: 1.97 > .05) were found to be significant.
Conclusions
These results provide some evidence in favor of parental training in managing behavioral problems occurring in early childhood. Instead of putting the child immediately on medication, parents can get training and prepare a plan to understand and make a change in child’s behavior leading to better health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Early childhood, is a time of tremendous growth across all areas of development. Physical changes in early childhood are accompanied by rapid changes in the child’s socioemotional, cognitive and language development. It has been found that young children face mental health problems due to an environment of relationships that can include parents, relatives, caregivers, teachers, and peers [1, 2]. Lack of appropriate help and support for emotional difficulties that emerges in early years of life can become more serious disorders over time [3–5]. National Survey of Children’s Health (2007) reported that children aged 4–8 years were more likely to be taking medicine for attention deficit/hyperactivity disorder than older children or adolescents [6]. The increasing use of psychoactive drugs for small children with behavioral or mental health problems, without having standard criteria, of efficacy and safety of these drugs at early age, is attracting the health professionals to find out better treatment options [7]. Early prevention strategies and efforts to identify and treat emergent mental health problems are likely to be more psychologically beneficial and cost effective than trying to treat emotional difficulties after they become more serious at a later age [8].
Because a healthy growth of young children depends so closely on the emotional status of their parents and family caregivers, the emotional and behavioral needs of young children are best met through a holistic approach that focuses on their full environment of relationship. Thus family centered approach, mainly the parental training suggests the most promising models for preventing and treating mental health problems in young children. Parental training provides information and support to address problematic child behavior.
Thus, in the present study researcher proposes to analyze the effect of parental training in managing behavioral problems (hostile/aggressiveness, anxious, hyperactive, distractible) occurring in early childhood.
The main relevance of present study is to know how to engender positive and healthy relationship between young children leading to positive actions and a constructive lifestyle. This study is also helpful in understanding how parenting should be made a dynamic and interactive process during early childhood.
Material and Methods
Participants
A total of 165 children, between the year 2004–2009, reported to pediatric OPD and psychiatric OPD for behavioral problems like low learning, poor memory, vertigo, speech problem, stress and headache, depression, and adjustment problems. Out of out of them 60 children were included in this study. Selected children had no other psychiatric diagnosis or any other co-morbidity. One of the important inclusion criteria was parents’ willful commitment to participate in the training program. The study was single group pre and post research design, (36 girls, 24 boys, mean age = 4 years, age range: 3–6 years). The research was carried out in the Department of Holistic Medicine, Himalayan Institute of Medical Sciences at Dehradun, India.
Materials
Preschool Behavior Questionnaire (PBQ), Developmental Screening Test (DST) and Vineland Social Maturity Scale (VSMS) were used as research tools for the study.
Preschool Behavior Questionnaire (PBQ) by Lenore Behar and Samual Stringfield (1974) was used to assess the aggressive behavior, anxious behavior, hyperactive behavior, and total disturbed behavior of early childhood [9]. PBQ contains 30 items indicating either of the above said behavior. Scoring are done based on selected choice of three options (“Does not Apply”−0, “Applies Sometimes”−1, and “Certainly applies”−2). PBQ is a screening tool to be used by mental health professionals. This instrument shows validity in discriminating between normal and deviant population and both inter-rater and test-retest reliability.
Developmental screening Test (DST-2006) by Dr. J. Bharath Raj, was used for assessing identified issues with socio-emotional, cognitive, language, and motor development in the selected children. DST has 88 items that stand for discrete and discernible behavioral characteristics representative of the respective age levels.
Vineland Social Maturity Scale (Indian Adoption) by Dr. A.J. Malin and Dr. J. Bharath Raj was used to find out the social maturity level of these children. VSMS has 89 items that stand for social characteristics representative of the respective age levels.
Model of ‘Mindful Parenting’ was used for the parental training program in present study. Mindful parenting is an approach to parenting that is reflected in qualitatively different interpersonal processes within the dynamics of parent–child relationship. The model of ‘Mindful Parenting’ has been introduced by the Larissa G. Duncan, J. Douglas Coatsworth, and Mark T. Greenberg (2009) [10]. The ‘Mindful Parenting’ model has five dimensions, 1) listening with full attention, 2) non judgmental acceptance of self and child, 3) emotional awareness of self and child, 4) self-regulation in the parenting relationship, 5) compassion for self and child.
These five dimensions are culture free and a natural phenomenon of parent child relationship living in any culture. This was the training of the parents to make a modification in their interaction style as per their cultural setup.
Procedure
After initial history taking, those children who showed positive findings of disturbed behavior but had no other psychiatric diagnosis or MR were administered PBQ, DST, and VSMS. Twenty four fortnightly sessions of parental training were conducted with each case. These sessions were held individually for each case. Participants were not subjected to group training. Each session was of 90 min. Parents were assigned to maintain daily dairy at home. DST, VSMS and PBQ were administered before the first session. Reassessment of PBQ was done after the 12th and 24 sessions of parental training. A separate play time and informal interview session of each child was held at the end of every visit of parental training. Separate telephonic interview of the concerned teachers of subjected children was conducted before starting the first session of parental training and after completion of the last session of training. Purpose of teachers’ interview was to understand children’s overall performance during school hours.
Scoring was undertaken at the end of 24th session of parental training. Single group t test method has been applied in order to see the difference in mean of pre and post assessment of PBQ.
Results
Each case adopted for the study was similar in its basic profile (Table 1). On assessment of DST and VSMS, it was found that children included in the study had a normal grade of developmental growth and social maturity level (Table 1). The range of developmental quotient was 85–90 (mean DQ = 87.5). The range of social quotient was 40–45 (mean SQ = 42.5).
Pre and post assessment difference between means of scores of PBQ was tested with single group t test method. After concluding parental training (after 24 sessions), mean difference of total disturbed behavior was found to be significant (t value: 38.7 > .05) (Table 2). Similarly the mean difference of hostile/aggressive behavior (t value: 17.1 > .05), anxious behavior (t value: 28 > .05), and hyperactive/distractible behavior (t value: 25.4 > .05) were found significant (Table 2).
As shown in Table 2, there is an incremental change in the total disturbed behavior, hostile/aggressive, anxious behavior and hyperactive/distractible behavior. But the change was more significant between end assessment and mid assessment than between mid assessment and baseline.
Thus, these results provide sufficient evidence to prove the effectiveness of parental training in managing the behavioral problems occurring in early childhood.
Discussion
The problems, as reported by the participatory parents of this study, in early childhood are manifold like low learning, poor memory, vertigo, speech problem, stress, headache, depression, adjustment problems, aggression, hostile behavior and so on. These problems were quite similar to the most commonly identified behavioral problems encountered by the pediatricians, found in an overview for pediatrician who conducted behavioral assessment of children and adolescents [11]. A similar study revealed that there are externalizing, internalizing and learning problems in children with scholastic difficulties [12].
The aim of the present research work was to see the effect of parental training on the specific behavioral problems like hostile/aggressiveness, anxious, hyperactive, distractible behavior of early childhood.
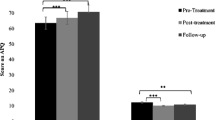
A significant difference was observed in pre and post parental training assessment at all the selected dimensions of disturbed behavior of early childhood (Table 2). Other researches and set doctrine on parenting shows that children’s personality, values and habit patterns changes at different stages of life but are greatly affected by the interactive style of the parents in early childhood. The concentrated goal of parents and teachers does not allow young children to explore the environment on their own. Consequently, young children then act out a sequence of four mistaken goals: first they seek attention. If they do not get it, they aim for power, then revenge and finally feel inadequate. It was described that children’s misbehavior was caused by their unfulfilled wish to be a member of a social group; they then act out a sequence of these four mistaken goals [13]. The results of the present study support to these findings where hyperactive/destructible behavior and anxious behavior are comparatively low than the hostile/aggressive behavior (Fig. 1). Some of the common causes for these problems were attributed to the following behavioral problems in the parental practice:
-
1)
Inappropriate expectations for the young child’s age.
-
2)
Parents were having preconceived ideas about educational performance of their children.
-
3)
Almost all the parents want their children to blindly follow their family norms.
-
4)
Almost all the parents were having differences between themselves in deciding who is responsible for the child’s growth and educational performances.
-
5)
Almost all the parents were harsh in training their child for the cultural discipline and educational aspects. This came up as the major cause of the emotional disturbance among young children.

Comparison between parameters before and after assessment of parental training (mean value)
Keeping these origination factors in mind, the ‘Mindful Parenting’ training module was found useful. This training taught the parent to develop sensitivity towards their children but prior to that towards themselves.
Most of the dimensions that differentiate parenting styles can be divided into three main factors; 1) warmth and caring, 2) level of structure, 3) level of intrusion. Through ‘warmth and caring’ factor, parents respond appropriately to the needs of their children. In ‘level of structure’ factor, parents introduce clear expectation. In ‘level of intrusion’, parents restrict their child instead of granting autonomy and choice [14]. Model of ‘Mindful Parenting’ used in the present study has emerged from the concepts and practices of psychological mindfulness, mindfulness-based interventions, and contemporary theoretical and empirical writings about parenting.
Mindfulness has been defined as “a receptive attention to and awareness of present events and experience” or “paying attention in a particular way: on purpose, in the present moment” [15–17]. Mindfulness training is increasingly employed in innovative therapies and interventions such as Mindfulness-Based Stress Reduction, Mindfulness-Based Cognitive Therapy, Dialectical Behavior Therapy, and Acceptance and Commitment Therapy [18–22]. These and other secular mindfulness-based interventions have been shown in some studies to effectively reduce psychological and physiological reactivity to a variety of stressful life situations and chronic illnesses, treat anxiety, and decrease recurrence of depressive episodes and substance abuse relapse in adults [23–27].
Results of present study also show a significant improvement in children’s behavior after implying the ‘Mindful Parenting’ training. Parents, after learning to listen with full attention became more sensitive both to the content of conversations as well as their child’s tone of voice, facial expressions, and body language, effectively using these indications to successfully detect their child’s needs or intended meaning. The improvements (after 24 sessions of “Mindful Parental Training”) were registered in following aspects:
-
1.
The level of total disturbed behavior decreased form 48.66 (mean of pre-assessment) to 15.01 (Fig. 1). Using the percentile rank table from manual of PBQ, it was found that total disturbed behavior came down form 99 to 74 percentile rank after 24 sessions of parental training (Fig. 2).
-
2.
Aggressive behavior reduced down from 99 percentile rank to 77(Fig. 2).
-
3.
Anxious behavior came down from 99 to 74 percentile rank (Fig. 2).
-
4.
Hyperactive behavior reduced from 96 to 53 percentile rank in comparison to the first assessment and last session of parental training session (Fig. 2).

Comparison between parameters before and after parental training (percentile rank)
Interview with teachers revealed an improved study performance of children whose parents participated in the training. Parents and teachers also reported that after four or five sessions of training, children started taking interest in going to school. By bringing their full attention to the interactions with children, parents may perceive their adolescents’ thoughts and feelings more accurately, which in turn, may reduce conflict and disagreement and promote more self-disclosure by the children [28, 29]. Parents vary in their overprotective or responsive practice to the needs and concerned of their children. These parental practices significantly affect the temperament, relationships, personality, motivation, and progress of their children, and these effects can persist throughout life.
Conclusions
The findings of the research show us how to create environment for children that support healthy development. The outcomes of study also suggest the procedure to develop a team approach to formulate Positive Behavior Support Plans for disturbed children with persistent challenging behavior. Instead of putting the child immediately on medication, parents can get training and prepare a plan to understand and make a change in child’s behavior leading to a better health.
Hence it can be concluded from the study that ‘mindful parental training’ can be effective in helping young children to grow in a healthier way. However, its validation needs more number of studies with larger sample size, various educational and socioeconomic backgrounds of the family and also in other aspects of emotional and disturbed behavior of younger children. It is suggested that practice of ‘Mindful Parenting’ can be applied to other stages of life.
References
Lewit E, Baker L. School readiness. Future Child. 1995;5:128–39.
Erimm-Kaufman S, Pianta R, Cox M. Teachers’ judgments of problems in the transition to kindergarten. Early Child Res Q. 2000;15:147–66.
Keenan K, Shaw D, Delliquadri E. Evidence for the continuity of early problem behaviors: application of a developmental model. J Abnorm Child Psychol. 1998;26:441–52.
Shaw DS, Gilliom M, Ingoldsby EM. Trajectories leading to school-age conduct problems. Dev Psychol, Special issue: Violent Children. 2003;39:189–200.
Suveg C, Southam-Gerow MA, Goodman KL. The role of emotion theory and research in child therapy development. Clin Psychol Sci Pract. 2007;14:358–71.
Visser SN, Lesesne CA, Perou R. National estimates and factors associated with medication treatment for childhood attention-deficit/hyperactivity disorder. Pediatrics. 2007;119:99–106.
Gleason MM, Egger HL, Emslie GJ, et al. Psychopharmacological treatment for very young children: contexts and guidelines. J Am Acad Child Adolesc Psych. 2007;46:1532–72.
National Scientific Council on the Developing Child. Mental health problems in early childhood can impair learning and behavior for life: working paper #6. 2008; http://www.developingchild.net.
Behar L, Stringfield S. Manual for pre school behavior questionnaire. 1st ed. Durham: Lenore Behar; 1974.
Duncan LG, Coatsworth JD, Greenberg MT. A model of mindful parenting: implications for parent–child relationships and prevention research. Clin Child Fam Psychol Rev. 2009;12:255–70.
Phillips EL, Kollins S, Edgerly D. Behavioural assessment of children and adolescents. Indian J Pediatr. 1999;66:389–99, PubMed PMID:10798087.
Hirisave U, Shanti K. Scholastic difficulties with behavioural problems. Indian J Pediatr. 2002;69:963–4, PubMed PMID: 12503661.
Dreikurs R. Coping with children’s misbehavior, a parent’s guide. New York: Hawthorn Books; 1972.
Prinzie P, Stams GJJM, Dekovic M, Reijintjes AHA, Belsky J. The relations between parents’ Big Five personality factors and parenting: a meta-analytic review. J Pers Soc Psychol. 2009;97:351–62.
Baer RA, Krietemeyer J. Overview of mindfulness- and acceptance-based treatment approaches. In: Baer RA, editor. Mindfulness-based treatment approaches. Burlington: Elsevier Academic Press; 2006. pp. 3–27.
Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84:822–48. doi:10.1037/0022-3514.84.4.822, [PubMed].
Kabat-Zinn J. Wherever you go there you are: mindfulness meditation in everyday life. 1st ed. New York: Hyperion; 1994. ISBN 1562827693.
Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4:33–47. doi:10.1016/0163-8343(82)90026-3, [PubMed].
Segal ZV, Williams JMG, Teasdale JD. Mindfulness-based cognitive therapy for depression. 1st ed. New York: The Guilford Press; 2002. ISBN 1572307064.
Linehan MM. Cognitive behavioral treatment of borderline personality disorder. NewYork: Guilford Press; 1993. ISBN 0898621836.
Hayes AM, Feldman G. Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clin Psychol Sci Pract. 2004;11:255–62. doi:10.1093/clipsy/bph080.
Hayes SC, Strosahl K, Wilson KG. Acceptance and commitment therapy. New York: Guilford Press; 1999.
Brantley J. Mindfulness-based stress reduction. In: Orsillo SM, Roemer L, editors. Acceptance and mindfulness-based approaches to anxiety: conceptualization and treatment. Series in anxiety and related disorders. New York: Springer; 2005. pp. 131–45.
Carlson LE, Speca M, Patel KD, Goodey E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom Med. 2003;65:571–81. doi:10.1097/01.PSY.0000074003.35911.41, [PubMed].
Roemer L, Orsillo SM. An open trial of an acceptance-based behavior therapy for generalized anxiety disorder. Behav Ther. 2007;38:72–85. doi:10.1016/j.beth.2006.04.004, [PubMed].
Ma SH, Teasdale JD. Mindfulness-based cognitive therapy for depression: replication and exploration of different relapse prevention effects. J Consult Clin Psychol. 2004;72:31–40. doi:10.1037/0022-006X.72.1.31, [PubMed].
Bowen S, Witkiewitz K, Dillworth TM, et al. Mindfulness meditation and substance use in an incarcerated population. Psychol Addict Behav. 2006;20:343–7. doi:10.1037/0893-164X.20.3.343, [PubMed].
Hastings PD, Grusec JE. Parenting goals as organizers of responses to parent–child disagreement. Dev Psychol. 1998;34:465–79. doi:10.1037/0012-1649.34.3.465, [PubMed].
Smetana JG, Metzger A, Gettman DC, Campione-Barr N. Disclosure and secrecy in adolescent-parent relationships. Child Dev. 2006;77:201–17. doi:10.1111/j.1467-8624.2006.00865.x, [PubMed].
Acknowledgments
This research study would not have been possible unless our clients had supported us, specially the children, who with their loving and emerging smiles reinforced us to continue this research. We are greatly obliged to Larissa G. Duncan, J. Douglas Coatsworth, and Mark T. Greenberg for granting open access to use “Mindful Parenting” model for this study. We also pay our regards to Lenore Behar and Samual Stringfield for PBQ, Dr. J. Bharath Raj for DST, and Dr. A.J. Malin for VSMS. We are indebted to many of our colleagues to support us thought-out this work. At the last but not the lest, we would like to show our gratitude to the librarians, all other staff members of the department and authors of citied references who directly are indirectly helped us in this work.
Contributions
M S; Planning and designing of the study paper, assessment and conduction of parental training program. Assistance in statistical analysis report preparation and writing the paper, AG and BPK; Helped in planning the study paper, initial assessment and referral of the cases to the Psychiatry OPD for study, UT and VL; Helped in planning the study paper and initial assessment.
Conflict of Interest
None.
Role of Funding Source
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Srivastava, M., Gupta, A., Talukdar, U. et al. Effect of Parental Training in Managing the Behavioral Problems of Early Childhood. Indian J Pediatr 78, 973–978 (2011). https://doi.org/10.1007/s12098-011-0401-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-011-0401-5