
Abstract
Introduction
With the aim of providing cancer control indicators, this work presents cancer survival in adult (≥15 years) patients in Spain diagnosed during the period 2000–2007 from Spanish cancer registries participating in the EUROCARE project.
Methods
Cancer cases from nine Spanish population-based cancer registries were included and analysed as a whole. All primary malignant neoplasms diagnosed in adult patients were eligible for the analysis. Cancer patients were followed until 31 December 2008. For each type of cancer, 1-, 3- and 5-year observed and relative survival were estimated by sex, age and years from diagnosis. Furthermore, age-standardized 5-year relative survival for the period 2000–2007 has been compared with that of the period 1995–1999.
Results
Skin melanoma (84.6 95% CI 83.0–86.2), prostate (84.6% 95% CI 83.6–85.6) and thyroid (84.2% CI 95% 82.0–86.6) cancers showed the highest 5-year relative survival, whereas the worst prognosis was observed in pancreatic (6% 95% CI 5.1–7.0) and oesophageal (9.4% 95% CI 7.9–11.1) cancers. Overall, survival is higher in women (58.0%) than in men (48.9%). The absolute difference in relative survival between 2000–2007 and 1995–1999 was positive for all cancers as a whole (+4.8% in men, +1.6% in women) and for most types of tumours. Survival increased significantly for chronic myeloid leukaemia, non-Hodgkin’s lymphoma and rectum cancer in both sexes, and for acute lymphoid leukaemia, prostate, liver and colon cancers in men and Hodgkin’s lymphoma and breast cancer in women. Survival patterns by age were similar in Europe and Spain. A decline in survival by age was observed in all tumours, being more pronounced for ovarian, corpus uteri, prostate and urinary bladder and less for head and neck and rectum cancers.
Conclusion
High variability and differences have been observed in survival among adults in Spain according to the type of cancer diagnosed, from above 84% to below 10%, reflecting high heterogeneity. The differences in prognosis by age, sex and period of diagnosis reveal opportunities for improving cancer care in Spain.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Monitoring health outcomes by means of survival provides a valuable indicator for future actions in cancer control. Cancer prognosis is a major issue because, despite its aggressive spread, positive outcomes can progressively be achieved by means of cancer patient management in accordance with the recommended guidelines and more effective diagnoses and treatment [1]. Survival time after diagnosis is a quality indicator of cancer care and reflects the vital experience of patients with cancer. One-year survival is mainly related to tumour stage, 3-year survival partially indicates the aggressiveness and progression of the tumour and 5-year survival reflects the health care process as a whole. Cancer registries provide measures of survival at a population-based level, allowing comparisons among different regions and revealing the possibilities to improve prognosis.
The EUROCARE (EUROpean CAncer Registry-based project on Survival and CARE of cancer patients) collaborative research project has provided comparable estimates of cancer survival in Europe over 20 years. Recently, EUROCARE-5 has published 5-year survival estimates in Europe for patients diagnosed between 2000 and 2007 [2] and specific survival for several types of cancer [3,4,5]; however, few data have been published regarding specific indicators of cancer survival by country. Similarly, the CONCORD (global surveillance of cancer survival) programme measures worldwide survival, disseminating results on cancer prognosis around the world [6]. Both projects have included data from Spanish cancer registries, although adopting different scopes and methodology to fulfil their aims.
Specific studies on cancer survival at the population level are scarce in Spain. Marcos-Gragera et al. [7] published trends in prostate cancer survival, showing a significant increase from 1999 to 2003. Salmerón et al. [8] analysed lung cancer prognosis in Spain, evidencing low survival with slightly better prognosis in women. Survival rates for nine cancers [9] were presented in Spain for tumours diagnosed from 1995 to 1999. Detailed and updated information on cancer prognosis in Spain is, therefore, relevant, useful and needed. In accordance with one of the main goals of REDECAN [10] (Spanish Network of Cancer Registries) and in collaboration with EUROCARE [11], the present work provides data from Spanish cancer registries for cancer survival in adult patients in Spain diagnosed between 2000 and 2007 using information from EUROCARE-5. Survival has also been included for 1995–1999 (EUROCARE-4) to compare with the later period.
Methods
Study population
Spanish data on primary malignant tumours were gathered and analysed within the context of the EUROCARE-5 [2] study, covering cases diagnosed from 2000 to 2007. Moreover, to allow comparisons with previous years, data from the EUROCARE-4 [12] study (1995–1999) were also analysed. The number of malignant cancers in ≥15 year-olds diagnosed in Spain from 2000 to 2007 and 1995–1999 were, respectively, 157,149 and 103,231. The nine participating population-based cancer registries in EUROCARE-5 are in the north (Euskadi and Navarra), central (Cuenca), east (Girona, Tarragona, Castellón) and south (Albacete, Murcia and Granada) of Spain. With the exception of Cuenca, all participated in EUROCARE-4. These cancer registries are included in the REDECAN network, which covers more than 7 million inhabitants and represents almost 20% of the total Spanish population.
The participant cancer registries regularly publish their data on incidence in CI5 (cancer incidence on five continents) [13] and their results on survival in EUROCARE and CONCORD, with good global quality indicators and high population coverage. Most of the registries have been operating for over 20 years [1].
Cancer patients
Spanish cancer registries collected and registered all new malignant tumours diagnosed in their covered areas. The study design and database have been described in Rossi et al. [14]. Briefly, cases included in the analysis were defined by topography and morphology following the International Classification of Disease for Oncology, 3rd edition (ICDO-3) [15]. Haematological tumours were grouped using the WHO classification [16]. All primary tumours and invasive malignant neoplasms were eligible for analysis. Non-melanoma skin cancers were excluded and urothelial cancer of the bladder, benign, in situ or uncertain, were included to ensure comparability among regions. Only adult patients (15 years old or over at cancer diagnosis) were selected for analysis. All primary cancers according to IARC–ENCR (International Agency for Research in Cancer/European Network of Cancer Registries) rules for multiple primary cancers have been included in EUROCARE-5, regardless of whether first, second and following multiple primary cancers have occurred [17]. In EUROCARE-4, applying the same criteria for primary cancer, only first primary cancers were included in the analysis. Cases whose only source of information were the death certificate (DCO) or cases diagnosed at autopsy were excluded from the survival analysis.
Cancer registries contributed to the EUROCARE database and jointly carried out the quality control procedures to correct missing or invalid data and inconsistencies. Finally, the information was analysed by EUROCARE for all participating European countries. Here, we present a sub-analysis of the EUROCARE-4 and -5 projects using data from Spain.
Follow-up
Follow-up of cancer patients diagnosed between 2000 and 2007 was done using common criteria for the collection of variables in all cancer registries. Cases were followed from the date of diagnosis to the end of follow-up (31 December 2008) ascertaining vital status. Multiple sources of information like the National Death Index, the social security database, municipal census and hospital and primary care records were used when necessary and available. Patients’ life status was categorized as follows: alive at the end of follow-up, dead at the end of follow-up—including date of exitus—or censored by loss or incomplete follow-up. For the incident cases in the period 1995–1999, the follow-up was carried out until 31 December 2003.
The datasets of the nine cancer registries are registered as stipulated by law with the Spanish data protection authority [18]. All data collected in the database for survival analysis were anonymous, and therefore, no ethical approval was required [19].
Statistical methods
Statistical analysis has been described elsewhere [14]. Briefly, for the period 2000–2007, 5-year observed survival, 5-year relative survival (5y-RS), and age-standardized relative survival at 1, 3 and 5 years since diagnosis, with 95% confidence interval (95% CI) were computed using the Ederer II method [20]. We present results by all malignant neoplasms by specific cancer types. Relative survival estimate is the ratio of observed patient survival to the survival that would have been expected if cancer patients had the same all-cause mortality as the general population of the same age, sex, region and period. Thus, it reflects the excess mortality in cancer patients and is an indicator for the comparison of population-based cancer survival when the cause of death is unknown.
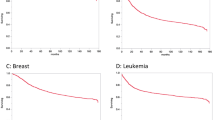
Age specific survival was estimated by age group (15–44, 45–54, 55–64, 65–74 and 75+ years) for all tumours, except prostate cancer (15–54, 55–64, 65–74, 75–84 and 85+ years) because of its higher median age at diagnosis. Figures comparing mean European survival with the Spanish survival by age group were performed for all specific tumours. To take into account differences in the age distribution of the population and to warrant comparability between sexes, regions and periods, we estimated age-standardized 5y-RS using international standards [21].
For the period 1995–1999 (EUROCARE-4), the Hakulinen method [22] was used to estimate the age-standardized 5y-RS, which was extracted from published results and compared with the most recent 2000–2007 results. The methods used in EUROCARE-4, slightly different from those used in EUROCARE-5, have also been previously described [12]. The cohort approach was used in both EUROCARE 4 and 5 to estimate the relative survival as a prognosis indicator of cancer. The Z test [23] was used to compare survival between periods, and the differences were considered to be significant when p value <0.05.
Results
The Spanish cancer cases included in the survival analysis, after applying the exclusion criteria detailed below, comprised 227,006 incident cases diagnosed in the participating cancer registries for the period 1995–2007. Cases excluded from the analyses were DCO (3.5%) and diagnosed incidentally at autopsy (0.1%). A total of 9% of cases were censored after fewer than 5 years of follow-up in EUROCARE-4 and 2.5% of cases were lost to follow-up in EUROCARE-5. Over 90% were diagnosed by microscopic verification.
In both sexes, for the nine Spanish regions combined in the period 2000–2007 (Table 1), the 5y-RS was lower than 10% for pancreatic (5.0% 95% CI 4.2–5.9) and oesophagus cancer (9.6% 95% CI 8.2–11.3). Thyroid cancer showed a 5y-RS of 90.4% (95% CI 88.8–92.1) followed by Hodgkin’s lymphoma (85.0% 95% CI 82.4–87.6) and skin melanoma (84.3% 95% CI 82.6–86.0). In men, testicular cancer presented a survival of 95.0% (95% CI 93.2–96.8), followed by prostate cancer with 84.5% (95% CI 83.6–85.4). 5y-RS for breast cancer in women was 85.2% (95% CI 84.5–85.8). The largest differences between relative and observed survival were found in cancers of the prostate, urinary bladder, colorectal and chronic lymphoid leukaemia.
The age-standardized 5y-RS increased from 1995–1999 to 2000–2007 for most of the analysed tumours, and for both sexes overall. In particular, there was a 4.8 percentage point (+4.8%) increase in age-standardized 5y-RS in men and a +1.6% rise in women (Table 2), both statistically significant. In men, the age-standardized 5y-RS increased for chronic myeloid leukaemia, acute lymphoid leukaemia, prostate, non-Hodgkin’s lymphoma, rectum, liver and colon cancers, whilst urinary bladder and larynx cancer showed a decrease in survival. In women, the improvement was observed for chronic myeloid leukaemia, non-Hodgkin’s lymphoma, acute myeloid leukaemia, Hodgkin’s lymphoma, rectum and breast cancer. A decrease in survival was observed for urinary bladder cancer. All these differences were statistically significant.
The differences in age-standardized relative survival at 1, 3 and 5 years from diagnosis (Table 3) for all malignant neoplasms were larger between 1- and 3-year survival (decrease of 13.5%) than between 3- and 5-year survival (5.2%). There was a higher reduction among men than women in the first period (14.8% vs. 11.8%), but percentages were the same in the second period (Suppl Table 1). Pancreatic cancer presented the worst prognosis at 1-year with 23.3% (95% CI 21.8–24.8), and skin melanoma the highest (96.1% 95% CI 95.3–96.9). The fastest decline from 1- to 3-year survival was observed in oesophagus cancer (age-standardized 5y-RS: from 38.2 to 12.8%), and the slowest in thyroid cancer (age-standardized 5y-RS: from 90.8 to 87.5%). In the second period, the fastest decrease was found in myeloma and the slowest in acute myeloid leukaemia.
Figure 1 shows that, in general, patterns of 5y-RS by age group and sex in Europe and Spain were similar, with the exception of stomach cancer, liver cancer and chronic myeloid leukaemia, which had a slightly better prognosis in Spain, and pancreatic cancer and lung cancer, which had a worse prognosis than in Europe. Prognosis falls with advancing age, and was as good in women as in men or better than in men for most cancers. For all cancers combined, 5y-RS figures across age groups ranged from 80 to 40% in women and 70–40% in men, overlapping with the European mean.


Relative survival at 5 years for adult patients (≥15) diagnosed in 2000–2007 with cancer. Spain and Europe by age class and sex
Discussion
The present study provides useful information for monitoring cancer prognosis in the Spanish population as a whole, showing differences in survival within cancer types by sex, age group and time from diagnosis. We analysed more than 260,000 patients diagnosed in nine population cancer registries (representing 20% of the total Spanish population) between 1995 and 2007, with a follow-up at least 5 years from diagnosis. Melanoma displayed the highest survival in both study periods and sexes, with higher values among women than men at 5 years from diagnosis. These differences by gender were the largest observed by cancer type and have also been found in several other studies [24,25,26]. Although explanations for these findings are scarce, those that have been postulated include more self-detection among women, more melanoma on non-easily visible locations in men than women, and differences in hormonal regulation [27, 28].
Thyroid cancer was the tumour with the second most favourable prognosis, also much better among females than males. An increase in thyroid examination by benign lesion leads to early detection of thyroid cancer, greatly increasing the incidence of papillary thyroid microcarcinoma [29] (less than 1 cm) in high-income countries [30].
The most aggressive tumour was pancreatic cancer, a rapidly progressive illness that presented 23% standardized RS at 1 year from diagnosis, decreasing to 6% at 5 years. Compared with the European mean, 1st year survival was lower in Spain, while 5th year was similar; both were very low [2, 5]. It is also worth pointing out that no improvement in survival has been detected in Spain and Europe for pancreatic cancer, coinciding with the findings of a study in Canada, where there had been little or no improvement in long-term survival in patients diagnosed with this cancer [31]. Despite advances in new selective molecules against specific cellular targets becoming available for pancreatic cancer therapy in recent years, prognosis of this cancer remains poor. Early detection is not effective, although molecular biomarkers and imaging techniques are now being developed [32, 33].
Head and neck cancers displayed better prognosis among women than men, and the decline with age was not as pronounced as with other tumours. Survival during the two analysed periods did not show improvements in Spain, whereas in Europe a slight overall increase was observed between the periods 1999–2001 and 2005–2007 [34]. With a Spanish mean near to 40%, similar to Europe, prognosis remained poor. Survival of larynx cancer slightly decreased in Spain, although the average is also close to the European mean. Anatomical subsites are important for interpreting these results because case-mix could partly explain the differences. Thus, cancers arising in the hypopharynx displayed lower survival than those located in the larynx. Other factors like tobacco exposure, papillomavirus infection or differences in stage at diagnosis could influence disparities in survival [35].
The gastrointestinal tumour that presented the worst prognosis was oesophagus cancer (9.4% 5y-RS), which was lower than the European mean (12.4%) [36]. The most favourable prognosis was found in colon and rectal cancer (60%), which was equal to the European figures [37] and within the range 50–59% described for many countries worldwide [6]. Stomach cancer, with a survival rate of <30%, and liver and gallbladder cancer, with <20%, showed a bad prognosis, although 1–2% above the European mean. Data published in CONCORD showed that in most countries survival from stomach cancer remained within the narrow range of 25–30% [6]. However, international comparisons are more limited for liver cancer than for other malignant tumours due to a high proportion of cancer registered with death certificate only. The increase in 5y-RS from 1995–1999 to 2000–2007 in Spain was from 1 to 5 percentage points for all gastrointestinal tumours, except oesophagus and stomach cancer, where no improvement was seen.
Lung cancer, which is very common in men and emerging in women, is a very aggressive disease. Some histology groups, such as squamous cell carcinoma and adenocarcinoma, presented better prognosis than others, like small-cell carcinoma [8]. This heterogeneity should be considered when interpreting results. No changes in prognosis were detected for the two study periods and survival was two points lower than the European mean [33]. For most geographical areas, worldwide survival was typically low (10–20%) [6].
Kidney cancer continued to have a moderate prognosis. Bladder cancer survival worsened during the two periods. Urinary bladder tumours are a heterogeneous malignancy difficult to compare due to problems following international recommendations, with several different grading classifications and non-standardized pathological reports. Differences in coding and registration practices need to be considered when comparing results over time [38]. For this reason, there was a large variation among regions within the same country or between different countries, as observed in EUROCARE-5, where 5y-RS age-standardized ranged from 50 to 80% [39].
Poor prognosis was detected for malignancies of the central nervous system. In this group of tumours, a specific analysis by sub-type would be necessary due to its heterogeneous composition causing marked differences in survival, ranging from 58% in ependymoma to only 6% in glioblastoma [40].
Females presented very different cancer survival patterns when measured by site of malignancy diagnosed, the highest values being for breast cancer, with 95% survival at 1 year from diagnosis, and the lowest for ovarian cancer with 70% at 1 year, but decreasing to 37% at 5 years. The prognosis was similar for both periods analysed and close to the European average [2, 4]. Ovarian cancer is a tumour with an unfavourable prognosis and no clear increase in survival rate has been detected in recent decades. Survival rates for cervix and corpus uteri cancer were stable when comparing the two periods studied. The global range for cervical cancer survival was very wide in different parts of the world, the majority of countries falling within the range 60–69% [6].
Tumours diagnosed only in males showed high survival figures, testicular cancer being the tumour with the best prognosis (95% of patients alive 5 years from diagnosis), which remained stable during the periods studied. Improvements in prostate cancer prognosis have been observed in the present study, in accordance with the findings of other studies [7], but survival dropped rapidly among older age groups for advanced stage at diagnosis and high-risk category on the Gleason scale [41, 42]. The elevated survival observed can be partially attributable to over diagnosis through PSA testing [6]. Low survival (<40% at 5th year) was observed in other regions around the world.
Comparisons of haematological malignancies over time are difficult due to changes in disease classification between the EUROCARE-4 [43] and EUROCARE-5 [14] study periods. Hodgkin’s lymphoma showed the best prognosis, with values of 82% for 5 years overall survival and maintained until 54 years of age, similar to the European mean (81%) [44]; this value also increased significantly between 1995–1999 and 2000–2007 in women but not men. Contrarily, acute myeloid leukaemia showed the worst prognosis with 19%, higher than the European mean of 17%. Chronic myeloid leukaemia experienced the highest increase in survival when comparing the two periods of study, followed by non-Hodgkin’s lymphoma; this reflects the benefits of therapeutic advances in specific haematological malignancies [45]. In all haematological malignancies, we observed a better prognosis among women than men, with the exception of acute lymphoid leukaemia. The largest difference between relative and observed survival was in prostate cancer, a tumour that mainly affects old people.
The gap in survival by gender for all malignant tumours was close to the absolute value of 10%, and higher among women. This difference has been widely described in many regions of the world [46]. Between-sex differences could be influenced by cancer case-mix because cancers with low survival rates (e.g. lung cancer) are more frequent in men and cancers with high survival rates are more common in women (e.g. breast cancer). That said, differences in prognosis between men and women still remain after adjusting for case-mix [47, 48]. Of the diverse causes hypothesized, the most commonly described is the role of sex hormone patterns giving women an advantage over men with regard to survival [46, 49].
Among the strengths of the study, we should mention that all available survival data from cancer registries have been included and that this is the most accurate information available on survival for the Spanish population. Although variations across Spain cannot be ruled out, a previous study did not show a clear pattern by regions in Spain [9]. One limitation of the study is the lack of results for some regions where cancer registries do not operate and it was not possible to collect information for survival or incidence. A common methodology used for population-based cancer registries (mainly European rules) was applied to collect and follow cancer cases, and a common procedure was carried out to ensure good quality indicators by means of checking data in the European context. Nevertheless, some slight differences in case registration and follow-up procedures cannot be ruled out across registries. It is worth noting the high number of cancer patients included in the study when all cases are considered, whether hospitalized or not, in private or public facilities, and involved in clinical trials or not. Thus, the results will be applicable to the general population.
Some limitations have to be taken into account in the comparison between EUROCARE-4 and 5. In EUROCARE-5, all primary tumours diagnosed in patients were included in the analysis so as to reduce possible differences in survival when comparing long- and recently established cancer registries. However, in EUROCARE-4 only first primary cancers were considered in the analysis. Rosso et al. [50] have shown that the overall effect of selecting all primary tumours is to reduce survival. Thus, although a direct comparison could be misleading, the increasing survival for some cancer types indicates not only a slight improvement in prognosis over time, but also an additional step forward in survival. This excess increase cannot be evaluated due to the different methodologies applied in the two periods of comparison. A further aspect to consider is the slight differences in follow-up. EUROCARE-5 followed all cancer patients until the end of 2008 and EUROCARE-4 did so until the end of 2003. This difference could underestimate survival in EUROCARE-5 because it has more accurate information on vital status for patients with short survival. Different methods were used to estimate relative survival (Ederer II in EUROCARE-5 and Hakulinen in EUROCARE-4). However, 5y-RS was adjusted for age using the same international standard and significant differences between these two approached are therefore, not expected [51]. Additionally, as shown in Rosso et al. [50], the Ederer II estimator provided lower RS than the Hakulinen estimator and the differences in survival estimates are larger for non age-standardized values.
In summary, high variability and large differences have been observed in Spain depending on the cancer type diagnosed in adults. Skin melanoma was the tumour that presented the best prognosis, followed by thyroid cancer. The most aggressive tumour was pancreatic cancer, a rapidly progressive disease, followed by oesophagus and lung cancer. Women presented both the highest survival, for breast cancer, and the lowest, for ovarian cancer. Men diagnosed with testis and prostate cancer presented good prognosis. Among the haematological malignancies, Hodgkin’s lymphoma showed the best prognosis and acute myeloid leukaemia the worst. Although a decline in survival by age was observed for all tumours, this was more pronounced for ovarian and prostate cancer and less for head and neck cancer. Most cancers showed improvement in survival between the two periods studied (colorectal, thyroid, prostate, breast, chronic myeloid leukaemia, non Hodgkin’s lymphoma), while some displayed a stable (lung, ovary, testis) or slightly lower (larynx, urinary bladder) rate. However, these changes must be interpreted with care. A gap in survival was found by gender for all malignant tumours combined, it being ten points higher among women than men. Many years of registering incident cancer cases and determining vital status have made it possible to monitor the prognosis of all types of tumours at the population level in Spain, highlighting the important role played by population-based cancer registries. This information is of great use for professionals involved in the management of cancer patients, for cancer prevention and for the patients themselves, improving information on cancer prognosis in Spain.
References
Navarro C, Martos C, Ardanaz E, Galceran J, Izarzugaza I, Peris-Bonet R, Spanish Cancer Registries Working Group, et al. Population-based cancer registries in Spain and their role in cancer control. Ann Oncol. 2010;21(Suppl 3):iii3–13.
De Angelis R, Sant M, Coleman MP, Francisci S, Baili P, Pierannunzio D, et al. Cancer survival in Europe 1999–2007 by country and age: results of EUROCARE–5-a population-based study. Lancet Oncol. 2014;15(1):23–34.
Francisci S, Minicozzi P, Pierannunzio D, Ardanaz E, Eberle A, Grimsrud TK, et al. Survival patterns in lung and pleural cancer in Europe 1999–2007: results from the EUROCARE-5 study. Eur J Cancer. 2015;51:2242–53.
Sant M, Chirlaque Lopez MD, Agresti R, Sánchez Pérez MJ, Holleczek B, Bielska-Lasota M, et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: results of the EUROCARE-5 study. Eur J Cancer. 2015;51:2191–205.
Lepage C, Capocaccia R, Hackl M, Lemmens V, Molina E, Pierannunzio D, et al. Survival in patients with primary liver cancer, gallbladder and extrahepatic biliary tract cancer and pancreatic cancer in Europe 1999–2007: results of EUROCARE-5. Eur J Cancer. 2015;51:2169–78.
Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS, et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet. 2015;385(9972):977–1010.
Marcos-Gragera R, Salmerón D, Izarzugaza I, Ardanaz E, Serdà BC, Larrañaga N, et al. Trends in prostate cancer survival in Spain: results from population-based cancer registries. Clin Transl Oncol. 2012;14(6):458–64.
Salmerón D, Chirlaque MD, Isabel Izarzugaza M, Sánchez MJ, Marcos-Gragera R, Ardanaz E, et al. Lung cancer prognosis in Spain: the role of histology, age and sex. Respir Med. 2012;106(9):1301–8.
Chirlaque MD, Salmerón D, Ardanaz E, Galceran J, Martínez R, Marcos-Gragera R, et al. Cancer survival in Spain: estimate for nine major cancers. Ann Oncol. 2010;21(Suppl 3):iii21–9.
http://redecan.org/en/index.cfm. Accessed 2 Jun 2017.
http://www.EUROCARE.it. Accessed 2 Jun 2017.
Sant M, Allemani C, Santaquilani M, Knijn A, Marchesi F, Capocaccia R, EUROCARE Working Group. EUROCARE-4. Survival of cancer patients diagnosed in 1995–1999. Results and commentary. Eur J Cancer. 2009;45(6):931–91.
Forman D, Bray F, Brewster DH, Gombe Mbalawa C, Kohler B, Piñeros M, et al. editors. Cancer incidence in five continents, vol. X. IARC scientific publication no. 164. Lyon: International Agency for Research on Cancer; 2014.
Rossi S, Baili P, Capocaccia R, Caldora M, Carrani E, Minicozzi P, EUROCARE-5 Working Group, et al. The EUROCARE-5 study on cancer survival in Europe 1999–2007: database, quality checks and statistical analysis methods. Eur J Cancer. 2015;51:2104–19.
Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin M, et al. International classification of diseases for oncology. 3rd ed. Geneva: World Health Organization. 2000.
Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon: IARC; 2008.
IACR-ENCR. International rules for multiple primary cancers (ICD-O 3rd ed). Lyon: IACR; 2004. http://www.encr.eu/images/docs/recommendations/MPrules_july2004.pdf. Accessed 2 Jun 2017.
Spanish Data Protection Agency. https://www.agpd.es (2004). Accessed 2 Jun 2017.
European Network of Cancer Registries. Guidelines on confidentiality in population-based Cancer Registration in the European Union. Lyon: ENCR; 2002.
Ederer F, Heise H. Instructions to IBM 650 programmers in processing survival computations. Methodological note no. 10. End results evaluation section. National Cancer Institute: Bethseda; 1959.
Corazziari I, Quinn M, Capocaccia R. Standard cancer patient population for age standardising survival ratios. Eur J Cancer. 2004;40(15):2307–16.
Hakulinen T. Cancer survival corrected for heterogeneity in patient withdrawal. Biometrics. 1982;38:933–42.
Parkin DM, Hakulinen T. Cancer registration: principles and methods. Analysis of survival. IARC Sci Publ. 1991;95:159–76.
Crocetti E, Mallone S, Robsahm TE, Gavin A, Agius D, Ardanaz E, EUROCARE Working Group, et al. Survival of patients with skin melanoma in Europe increases further: results of the EUROCARE-5 study. Eur J Cancer. 2015;51:2179–90.
Lyth J, Mikiver R, Nielsen K, Isaksson K, Ingcar C. Prognostic instrument for survival outcome in melanoma patients: base on data from the population-based Swedish Melanoma Register. Eur J Cancer. 2016;59:171–8.
Crocetti E, Fancelli L, Manneschi G, Caldarella A, Pimpinelli N, Chiarugi A, et al. Melanoma survival: sex does matter, but we do not known how. Eur J cáncer Prev. 2016;25(5):404–9.
Avilés-Izquierdo JA, Molina-López I, Rodríguez-Lomba E, Marquez-Rodas I, Suarez-Fernandez R, Lazaro-Ochaita P. Who detects melanoma? Impact of detection patterns on characteristics and prognosis of patients with melanoma. J Am Acad Dermatol. 2016;75(5):967–74.
Nosrati A, Wei ML. Sex disparities in melanoma outcomes: the role of biology. Arch Biochem Biophys. 2014;563:42–50.
Chirlaque MD, Moldenhauer F, Salmerón D, Navarro C. Trends pattern of the incidence of thyroid cancer in Murcia Region (Spain) from 1984 to 2008. Gac Sanit. 2014;28(5):397–400.
Leboulleux S, Tuttle RM, Pacini F, Schlumberger M. Papillary thyroid microcarcinoma: time to shift from surgery to active surveillance? Lancet Diabetes Endocrinol. 2016;4:933–42.
Akhtar-Danesh GG, Finley C, Akhtar-Danesh N. Long-term trends in the incidence and relative survival of pancreatic cancer in Canada: a population-based study. Pancreatology. 2016;16(2):259–65.
Romiti A, Falcone R, Roberto M, Marchetti P. Tackling pancreatic cancer with metronomic chemotherapy. Cancer Lett. 2017;394:88–95.
Zhou B, Xu JW, Cheng YG, Gao JY, Hu SY, Wang L, et al. Early detection of pancreatic cancer: where are we now and where are we going? Int J Cancer. 2017;141:231–41.
Gatta G, Botta L, Sánchez MJ, Anderson LA, Pierannunzio D, Licitra L, the EUROCARE Working Group. Prognoses and improvement for head and neck cancers diagnosed in Europe in early: the EUROCARE-5 population-based study. Eur J Cancer. 2015;51:2130–43.
Guizard AV, Uhry Z, de Raucourt D, Mazzoleni G, Sánchez MJ, Ligier K, GRELL EUROCARE-5 Working Group. Trends in net survival from head and neck cancer in six European Latin countries: results from the SUDCAN population-based study. Eur J Cancer Prev. 2017;26:S16–23.
Anderson LA, Tavilla A, Brenner H, Luttmann S, Navarro C, Gavin AT, EUROCARE-5 Working Group, et al. Survival for oesophageal, stomach and small intestine cancers in Europe 1999–2007: results from EUROCARE-5. Eur J Cancer. 2015;51:2144–57.
Holleczek B, Rossi S, Domenic A, Innos K, Minicozzi P, Francisci S, EUROCARE-5 Working Group, et al. On-going improvement and persistent differences in the survival for patients with colon and rectum cancer across Europe 1999–2007—results from the EUROCARE-5 study. Eur J Cancer. 2015;51:2158–68.
Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol. 2017;71(1):96–108.
Marcos-Gragera R, Mallone S, Kiemeney LA, Vilardell L, Malats N, Allory Y, EUROCARE-5 Working Group, et al. Urinary tract cancer survival in Europe 1999–2007: results of the population-based study EUROCARE-5. Eur J Cancer. 2015;51:2217–30.
Visser O, Ardanaz E, Botta L, Sant M, Tavilla A, Minicozzi P, EUROCARE-5 Working Group. Survival of adults with primary malignant brain tumours in Europe; results of the EUROCARE-5 study. Eur J Cancer. 2015;51:2231–41.
Trama A, Foschi R, Larrañaga N, Sant M, Fuentes-Raspall R, Serraino D, EUROCARE-5 Working Group, et al. Survival of male genital cancers (prostate, testis and penis) in Europe 1999–2007: results from the EUROCARE-5 study. Eur J Cancer. 2015;51:2206–16.
Campá J, Mar-Barrutia G, Extramiana J, Arróspide A, Mar J. Advanced prostate cancer survival in Spain according to the Gleason score, age and stage. Actas Urol Esp. 2016;40(8):499–506.
De Angelis R, Francisci S, Baili P, Marchesi F, Roazzi P, Belot A, et al. The EUROCARE-4 database on cancer survival in Europe: data standardisation, quality control and methods of statistical analysis. Eur J Cancer. 2009;45(6):909–30.
De Angelis R, Minicozzi P, Sant M, Dal Maso L, Brewster DH, Osca-Gelis G, EUROCARE-5 Working Group, et al. Survival variations by country and age for lymphoid and myeloid malignancies in Europe 2000–2007: results of EUROCARE-5 population-based study. Eur J Cancer. 2015;51:2254–68.
Osca-Gelis G, Puig-Vives M, Saez M, Gallardo D, Lloveras N, Guàrdia R, et al. Is survival in myeloid malignancies really improving? A retrospective 15-year population-based study. Leuk Lymphoma. 2015;56(4):896–902.
Ellison LF. Differences in cancer survival in Canada by sex. Health Rep. 2016;27(4):19–27.
Oberaigner W, Siebert U. Do women with cancer have better survival as compared to men after adjusting for staging distribution? Eur J Public Health. 2011;21(3):387–91.
Baili P, Di Salvo F, Marcos-Gragera R, Siesling S, Mallone S, Santaquilani M, et al. Age and case mix-standardised survival for all cancer patients in Europe 1999–2007: results of EUROCARE-5, a population-based study. Eur J Cancer. 2015;51:2120–9.
Micheli A, Ciampichini R, Oberaigner W, Ciccolallo L, de Vries E, Izarzugaza I, et al. The advantage of women in cancer survival: an analysis of EUROCARE-4 data. Eur J Cancer. 2009;45(6):1017–27.
Rosso S, De Angelis R, Ciccolallo L, Carrani E, Soerjomataram I, Grande E, EUROCARE Working Group, et al. Multiple tumours in survival estimates. Eur J Cancer. 2009;45(6):1080–94.
Rutherford MJ, Dickman PW, Lambert PC. Comparison of methods for calculating relative survival in population-based studies. Cancer Epidemiol. 2012;36(1):16–21.
Acknowledgements
Compagnia Intesa San Paolo (Grant No. 2010.1354) and the Fondazione Cariplo (Grant No. 2010.1984).
REDECAN Working Group: Albacete (Antonio Mateos, Enrique Almar), Asturias (José Ramón Quirós, Marcial V. Argüelles, Virginia Menéndez), Canarias (Dolores Rojas, Araceli Alemán), Castellón (Ana Torrella, Consol Sabater, Paloma Botella), Ciudad Real (Matilde Chico, María Ripoll, Cristina Díaz), Infantil de la Comunitat Valenciana (Marisa Vicente, Nieves Fuster, Paloma Botella), Cuenca (José María Díaz, Rosario Jiménez, Ana Isabel Marcos Navarro), Euskadi-Basque Country (Nerea Larrañaga, Joseba Bidaurrazaga, Arantza Lopez-de-Munain), Girona (Rafael Marcos-Gragera, Àngel Izquierdo, Loreto Vilardell), Granada (María José Sánchez, Elena Molina-Portillo, Miguel Rodríguez-Barranco), La Rioja (Josefina Perucha), Mallorca (Paula Franch, Maria Ramos), Murcia (Carmen Navarro, María Dolores Chirlaque, Diego Salmerón), Navarra (Eva Ardanaz, Marcela Guevara, Rosana Burgui), Tarragona (Jaume Galceran, Alberto Ameijide, Marià Carulla, Jàmnica Bigorra), Registro Español de Tumores Infantiles (Rafael Peris Bonet, Elena Pardo).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This work does not contain clinical studies or patient data.
Informed consent
For this type of study formal consent is not required.
Additional information
the REDECAN Working Group are listed in Acknowledgements.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chirlaque, M.D., Salmerón, D., Galceran, J. et al. Cancer survival in adult patients in Spain. Results from nine population-based cancer registries. Clin Transl Oncol 20, 201–211 (2018). https://doi.org/10.1007/s12094-017-1710-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-017-1710-6