
Abstract
Purpose
Despite significant improvements in the design and performance of continuous flow left ventricular assist devices (CFLVADs), one of the most important reasons hampering further penetration of this technology is the occurrence of adverse events, especially strokes. One of the well-known risk factors for strokes is hypertension which is particularly common in patients undergoing a CFLVAD implant. While the device is implanted in the heart, strokes happen due to pathology in the brain and we hypothesised that modelling the blood flow in the circle of Willis might shed light on the causation of strokes in this situation.
The aim of the study was two-fold:
-
1. What is the reason for hypertension in CFLVADs? Are there physical factors at play, besides neurohumoral mechanisms?
-
2. Do anatomical factors in the circle of Willis play a role in the causation of strokes in these patients?
Methods
The circle of Willis is often incomplete and has a number of anatomical variations, the commonest being the absence of the posterior communicating artery. Hypertension is common after CFLVAD implantation and is also a well-known risk factor for strokes. We examined the blood pressure in the cerebral circulation with pulsatile and non-pulsatile flow for identical conditions and the effect of the absence of the posterior communicating artery on regional cerebral blood flow and pressure. One-dimensional blood flow model was used, taking into account wave propagation and reflections and physiological data obtained from anatomically detailed arterial network (ADAN86) which has data from 86 arteries including detailed cerebral network.
Results
The mean arterial pressure was significantly higher in the non-pulsatile blood flow of CFLVADs compared to pulsatile flow, for identical conditions, across all arteries. With increasing imparted pulsatility to CFLVAD flow, the mean arterial pressure progressively decreased. Isolated absence of the posterior communicating artery had no effect on the flow as well as pressure in the middle cerebral artery. However, when combined with the absence of flow in the ipsilateral carotid artery, the flow as well as the pressure decreased very significantly in both continuous and pulsatile flow situations.
Conclusions
Physiologically significant pulsatility in CFLVADs can have important clinical advantages in lowering of blood pressure which can lead to lower incidence of strokes, pump thrombosis, gastrointestinal (GI) bleeds, and aortic incompetence. Patient-specific anatomical variations in the circle of Willis, especially the absence of the posterior communicating artery, can have important consequences in regional cerebral perfusion under some circumstances.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Continuous flow left ventricular assist devices (CFLVADs) have evolved over the last decade from being used as a bridge to transplant to destination therapy [1, 2]. They are now widely regarded as a viable therapeutic option in the management of end-stage heart failure with recent results indicating that the 2-year survival rates following implantation of HeartMate III compare very favourably with heart transplantation [3, 4]. Despite such impressive advances, major concerns regarding adverse events have impeded the growth and penetration of this technology to patients with class III heart failure [5]. Of all the major complications reported with left ventricular assist devices (LVADs), strokes are undoubtedly the most catastrophic and occur much more commonly, as much as twenty times more frequently according to some estimates, than in the general population [6]. While there is a relationship between strokes and LVAD therapy, the actual pathology is in the brain, and we hypothesised that modelling the blood flow in the brain in both pulsatile flow and continuous flow situations might throw more light on the causative mechanisms for strokes during LVAD therapy.
Materials and methods
The blood supply to the brain is from the internal carotid arteries which supply blood to the majority of cerebral hemispheres, the so-called anterior circulation and from the vertebral arteries which supply the brainstem, cerebellum, occipital lobes, and the basal ganglia, the so-called posterior circulation. The circle of Willis is an anatomical structure that provides an anastomotic connection between the anterior and posterior circulations and right and left side of the brain [7]. It is often incomplete and has a number of anatomical variations, the commonest being the absence of the posterior communicating artery [8, 9]. Hypertension is a well-known risk factor for stroke, especially with CFLVADs [10, 11]. We therefore decided to study the blood pressure in the arteries in the circle of Willis with pulsatile and non-pulsatile flow and the effect of the absence of posterior communicating artery on regional cerebral blood flow and pressure.
The model used in this work is a one-dimensional blood flow model [12,13,14,15,16,17]. The numerical procedure used to solve the equations are from literature [18]. One-dimensional models take into account wave propagation and reflections and need physiological data. These data are standard in the literature and are classified as 55 arteries data, called anatomically detailed arterial network (ADAN55) and 86 arteries data including a detailed cerebral network known as ADAN86 [19, 20]. In this work, ADAN86 has been used.
In the model, we have used area (A) and flow rate (Q) as the main variables. The arterial wall is assumed to be viscoelastic and the Kelvin-Voigt model [21] has been used. The equations used are summarized below.
Here α is the momentum correction coefficient, KR is the friction coefficient, P is the pressure, Pext is the reference pressure, β is the stiffness parameter, E is the Young’s modulus, h is the thickness of the vessel wall, and A0 is the reference area. Poisson’s ratio ʋ is taken to be 0.5 since biological materials are assumed to be incompressible, and ϕ is the coefficient of viscosity of the material.
The solution for the above equation is based on Roe type energy balanced Godunov scheme as elaborated by [22]. All simulations presented were run on a 12 core xenon central processing unit (CPU). The data required to model the cerebral network are from published studies [23].
Results
Normal pulsatile flow and LVAD flow with varying degrees of pulsatility
Normal pulsatile flow was modelled at 5 lpm for a heart rate of 75 beats per minute. The reflection coefficients are from literature [21]. The results presented are for the tenth cycle. The LVAD flow was also modelled at 5 L/min, with no pulsatility and later varying degrees of pulsatility were added. The pressure results for major arteries of the circle of Willis (Fig. 1) are presented in Table 1. Mean arterial pressure (MAP) was calculated as one-third systolic pressure added to two-thirds diastolic pressure compared against a constant pressure for LVAD. As can be seen from the table, LVAD pressures are significantly higher than the MAP for pulsatile flow, for identical conditions, even though the peak systolic pressure is higher in pulsatile flow. This is consistent over all arteries (Fig. 2).

Normal circle of Willis

LVAD pressures for identical conditions
In order to understand the effect of pulsatile flow, pulsatility was introduced in a constant LVAD flow. The total flow was maintained at 5 L/min, and this was split into a constant flow of 3 lpm and a pulsatile flow of 2 lpm. The pulse was run at three rates, namely, 60, 100, and 200 beats per minute.
The procedure to introduce pulse was as follows: A constant flow of 3 lpm was introduced until a steady state condition was reached, which took about 10 s. Then the flow was modified to include pulse and the simulation continued for another 10 s. The results are shown in Fig. 3 and are at the end of 10 s.

Results of the flow that was modified to include pulse and the simulation
The same cycle is repeated for constant flow of 4 lpm and pulsatile flow of 1 lpm. The above figures clearly bring out the effect of pulse. The MAP drops with increasing pulsatility. The drop is larger when the constant part of the flow decreases. Also, there is a marginal increase in MAP, when the rate increases, even though the peak pressure drops.
Flow simulation with anatomic variation in the circle of Willis
The circle of Willis is often incomplete, and the commonest variant is the absence of the posterior communicating artery [8, 9].
It has been shown that the position of the outflow graft in CFLVADs may influence the flow into the innominate artery and under certain conditions the flow may be very low [24]. In this study, we investigated the effect of lack of flow in the right common carotid artery when the posterior communicating artery is present or absent.
The flow in the right middle cerebral arteries was measured for the following conditions.
-
(i)
Absence of flow in the right posterior communicating artery (PCA)
-
(ii)
Absence of flow in the right common carotid artery (RCCA)
-
(iii)
Absence of flow in both PCA and RCCA.
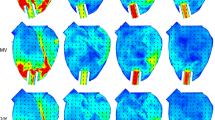
These results are presented in Fig. 4 for the right middle cerebral artery in a pulsatile flow. The above results clearly show that when PCA is absent, there is no change in flow as well as pressure in the middle cerebral artery. On the other hand, when the right carotid is not perfused, the flow as well as the pressure drops. This is further accentuated by the absence of PCA. The flow and pressure in the left side of the brain are not affected. The trends for CFLVAD flow are similar to those of the pulsatile flow (Fig. 5). Impedance in the ascending aorta with respect to frequency was calculated along with the phase (Fig. 6).

Results for the right middle cerebral artery in a pulsatile flow

Trends for CFLVAD flow

Impedance in the ascending aorta with respect to frequency
Discussion
The growth of ventricular assist devices over the last two decades has been achieved to a large extent because of a shift to continuous flow pumps. This has allowed the pumps to be smaller, making less invasive implantation possible and with better long-term survival [5]. However, there have been consequences of non-pulsatile flow, namely, a higher incidence of gastrointestinal bleeds, more systemic hypertension, and higher incidence of aortic incompetence as compared to pulsatile pumps [25]. Hypertension has been associated with a higher incidence of strokes both haemorrhagic and ischaemic, and aortic incompetence has been shown to affect long-term survival and cerebral perfusion [11]. The reason for hypertension in CFLVADs has been a subject of intense debate and several factors including marked sympathetic activation due to baroreceptor unloading [26] and increased arterial stiffness [27] have been implicated.
We hypothesised that modelling blood flow in the circle of Willis in both normal pulsatile flow and CFLVAD might shed some light on the causation of strokes.
The first interesting finding of the study was the fact that the physics of non-pulsatile blood flow was responsible for up to 10 mmHg increase in mean blood pressure across the arterial tree including all the cerebral vessels quite independent of any vasomotor and endocrine causes. Progressive increase of pulsatility to CFLVAD flow led to progressive lowering of blood pressure. The reason for lowering of the mean pressure due to pulsatility is complex. The magnitude and phase of the impedance, shown in Fig. 6, seem to play a role. A complex interaction of the forward and backward moving waves may be the reason for this phenomenon.
The second interesting finding was that the absence of PCA, while in itself, of no consequence, can have a profound impact on cerebral blood flow and pressure in the presence of ipsilateral hypoperfusion of the internal carotid artery. This finding assumes great significance in light of the fact that hypoperfusion of the innominate has been postulated to happen during LVAD implant depending on the arch anatomy, outflow graft angle, and size [24] and during aortic cannulation for cardiopulmonary bypass [28]. This fact has been highlighted in neurological literature as well [29]. Strokes are multifactorial and elimination of this dreaded complication needs attention to multiple factors including inflow cannula design, pump design, and anticoagulation management. What this study has shown is the benefits of imparting pulsatility in lowering blood pressure and the role of patient-specific anatomical factors which might contribute to the risk of stroke. Pump designs with flatter HQ (pump head flow) curves and greater physiologic pulsatility have demonstrated lower incidence of aortic incompetence and gastrointestinal (GI) bleeds [30,31,32].
Limitations of the study
By the very nature of a mathematical simulation study, clinical confirmation of our conclusion regarding pulsatility and blood pressure is not feasible. It is well known, of course, that pulsatile pumps do not have hypertension as a significant side effect. We have no clinical data correlating anatomical variation in the cerebral circulation with strokes in our LVAD patients though the association between absence of PCA and strokes in the presence of ipsilateral carotid blocks is well documented in neurological literature.
Conclusion
Physiologically significant pulsatility can have important clinical advantages in lowering of blood pressure which can lead to lower incidence of strokes, pump thrombosis, GI bleeds, and aortic incompetence. If this can be achieved by pump design with more favourable HQ curves or software algorithm, then it is possible to have the best of both worlds, all the advantages of a continuous flow pump while retaining the benefits of a pulsatile flow.
Data availability
Not applicable.
References
Holley CT, Harvey L, John R. Left ventricular assist devices as a bridge to cardiac transplantation. J Thorac Dis. 2014;6:1110–9. https://doi.org/10.3978/j.issn.2072-1439.2014.06.46.
Suarez-Pierre A, Zhou X, Fraser CD III, Grimm JC, Crawford TC, Lui C, et al. Survival and functional status after bridge-to-transplant with a left ventricular assist device. ASAIO J. 2019;65:661–7.
Fukunaga N, Rao V. Left ventricular assist device as destination therapy for end stage heart failure: the right time for the right patients. Curr Opin Cardiol. 2018;33:196–201. https://doi.org/10.1097/HCO.0000000000000486.
Lim S, Shaw S, Venkateswaran R, Abu-Omar Y, Pettit SJ, Chue CD. HeartMate 3 compared to heart transplant outcomes in England. J Heart Lung Transplant. 2020;39:S15–6.
Pagani FD. Adverse event burden and mechanical circulatory support: looking toward the future. J Thorac Cardiovasc Surg. 2016;151:10–2.
Loyaga-Rendon RY, Jani M, Fermin D, McDermott JK, Vancamp D, Lee S. Prevention and treatment of thrombotic and hemorrhagic complications in patients supported by continuous-flow left ventricular assist devices. Curr Heart Fail Rep. 2017;14:465–77.
Uston C. NEUROwords Dr. Thomas Willis’ famous eponym: the circle of Willis. J Hist Neurosci. 2005;14:16–21.
Gunnal SA, Farooqui MS, Wabale RN. Anatomical variations of the circulus arteriosus in cadaveric human brains. Neurol Res Int. 2014;2014:1–16.
Jones JD, Castanho P, Bazira P, Sanders K. Anatomical variations of the circle of Willis and their prevalence, with a focus on the posterior communicating artery: a literature review and meta-analysis. Clin Anat. 2020;34:978–90. https://doi.org/10.1002/ca.23662.
Acharya D, Loyaga-Rendon R, Morgan CJ, Sands KA, Pamboukian SV, Rajapreyar I, et al. INTERMACS analysis of stroke during support with continuous-flow left ventricular assist devices. JACC Heart Fail. 2017;5:703–11.
Lampert BC, Eckert C, Weaver S, Scanlon A, Lockard K, Allen C, et al. Blood pressure control in continuous flow left ventricular assist devices: efficacy and impact on adverse events. Ann Thorac Surg. 2014;97:139–46.
Westerhof N, Bosman F, De Vries CJ, Noordergraaf A. Analog studies of the human systemic arterial tree. J Biomech. 1969;2:121–43.
Stergiopulos N, Young DF, Rogge TR. Computer simulation of arterial flow with applications to arterial and aortic stenoses. J Biomech. 1992;25:1477–88.
Formaggia L, Lamponi D, Quarteroni A. One-dimensional models for blood flow in arteries. J Eng Math. 2003;47:251–76.
Mynard JP, Nithiarasu P. A 1D arterial blood flow model incorporating ventricular pressure, aortic valve and regional coronary flow using the locally conservative Galerkin (LCG) method. Commun Numer Methods Eng. 2008;24:367–417.
Müller LO, Toro EF. A global multiscale mathematical model for the human circulation with emphasis on the venous system. Int J Numer Meth Biomed Eng. 2014;30:681–725.
Safaei S, Bradley CP, Suresh V, Mithraratne K, Muller A, Ho H, et al. Roadmap for cardiovascular circulation model. J Physiol. 2016;594:6909–28.
Krishna S, Balakrishnan KR, Kumar RK. A comparison of blood pressure in a pulsatile flow and LVAD flow with imposed pulsatility using wave propagation model. BIODEVICES. In: Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies BIOSTEC - (Volume 1); 2019. pp. 167–74.
Fossan FE. Comparison of numerical schemes for nonlinear 1-D arterial blood flow modeling. NTNU; 2015. Available at - https://folk.ntnu.no/leifh/alumni/2015_Fredrik_Eikeland_Fossan.pdf. Accessed 7 Sept 2024.
Boileau E, Nithiarasu P, Blanco PJ, Müller LO, Fossan FE, Hellevik LR, et al. A benchmark study of numerical schemes for one-dimensional arterial blood flow modelling. Int J Numer Meth Biomed Eng. 2015;31. https://doi.org/10.1002/cnm.2732.
Wang X. 1D modeling of blood flow in networks : numerical computing and applications. Mechanics [physics]. Université Pierre et Marie Curie - Paris VI, 2014. English.<NNT : 2014PA066626>.
Murillo J, García-Navarro P. A roe type energy balanced solver for 1D arterial blood flow and transport. Comput Fluids. 2015;117:149–67.
Reymond P, Merenda F, Perren F, Rüfenacht D, Stergiopulos N. Validation of a one-dimensional model of the systemic arterial tree. Am J Physiol-Heart Circ Physiol. 2009;297:H208–22.
Bhat S, Mathew J, Balakrishnan KR, Krishna KR. Effect of outflow graft size on flow in the aortic arch and cerebral blood flow in continuous flow pumps: possible relevance to strokes. ASAIO J. 2017;63:144–9.
Castagna F, Stöhr EJ, Pinsino A, Cockcroft JR, Willey J, ReshadGaran A, et al. The unique blood pressures and pulsatility of LVAD patients: current challenges and future opportunities. Curr Hypertens Rep. 2017;19:85. https://doi.org/10.1007/s11906-017-0782-6.
Markham DW, Fu Q, Palmer MD, Drazner MH, Meyer DM, Bethea BT, et al. Sympathetic neural and hemodynamic responses to upright tilt in patients with pulsatile and nonpulsatile left ventricular assist devices. Circ Heart Fail. 2013;6:293–9.
McDonnell BJ, Rosenblum H, Cornwell WK, Kanwar M, Cockcroft JR, Stöhr EJ. Bionic women and men - Part 2: Arterial stiffness in heart failure patients implanted with left ventricular assist devices. Exp Physiol. 2020;105:755–8.
Kaufmann TAS, Hormes M, Laumen M, Timms DL, Schmitz-Rode T, Moritz A, et al. Flow distribution during cardiopulmonary bypass in dependency on the outflow cannula positioning. Artif Organs. 2009;33:988–92.
Oumer M, Alemayehu M, Muche A. Association between circle of Willis and ischemic stroke: a systematic review and meta-analysis. BMC Neurosci. 2021;22:3.
Imamura T, Kinugawa K. Centrifugal pump EVAHEART prevents development of aortic insufficiency preserving pulse pressure. Int Heart J. 2016;57:127–8.
Fine NM, Park SJ, Stulak JM, Topilsky Y, Daly RC, Joyce LD, et al. Proximal thoracic aorta dimensions after continuous-flow left ventricular assist device implantation: longitudinal changes and relation to aortic valve insufficiency. J Heart Lung Transplant. 2016;35:423–32.
Bartoli CR, Kang J, Zhang D, Howard J, Acker M, Atluri P, et al. Left ventricular assist device design reduces von Willebrand factor degradation: a comparative study between the HeartMate II and the EVAHEART left ventricular assist system. Ann Thorac Surg. 2017;103:1239–44.
Funding
None.
Author information
Authors and Affiliations
Contributions
SK and RKK were responsible for the modelling and simulation studies and interpreting the data. KB was responsible for defining the problem, interpreting the clinical relevance of the results, and preparation of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
No human or animal data; therefore, no consent/welfare of animals involved.
Consent
Not applicable.
Conflict of interest
No conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Krishna, S., Balakrishnan, K. & Kumar, R.K. Modelling blood flow in the circle of Willis in continuous flow left ventricular assist devices: possible relevance to strokes. Indian J Thorac Cardiovasc Surg (2024). https://doi.org/10.1007/s12055-024-01806-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12055-024-01806-6