
Abstract
Extracorporeal membrane oxygenation (ECMO) has become the standard of care for potentially reversible cardiopulmonary conditions intractable to conventional medical management. Single site, dual-lumen veno-venous ECMO has proven to be safe and advantageous with respect to mobilization of the patient. Nevertheless, adequate respiratory support demands optimal cannula positioning and catastrophic cannulation complications have been reported. We describe herein the utilization of an angulated guiding catheter to obtain trans-caval access for the successful placement of a single site dual-lumen cannula for veno-venous ECMO in a patient with unfavorable trans-caval anatomy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Extracorporeal membrane oxygenation (ECMO) has become the standard of care for potentially reversible cardiopulmonary conditions intractable to conventional medical management [1]. Strategies for implementation have evolved from multiple site cannulation of both veno-arterial (traditionally femoral vein to femoral artery) and veno-venous (VV) ECMO (mainly the femoral vein to the internal jugular vein), to single site, dual-lumen cannulation for VV ECMO. Several studies have shown that single site, dual-lumen cannulation for VV ECMO is safe and advantageous with respect to mobilization of the patient [2, 3]. Malplacement of ECMO cannulas can lead to physiologic insult with inadequate distribution of oxygenated blood, as well as anatomic/structural insult with atrial and/or ventricular rupture [4], both of which can contribute to worsening clinical decline and even death. We describe the utilization of an angulated guiding catheter to successfully obtain trans-caval access for the successful placement of a single site dual-lumen cannula for VV ECMO in a patient with unfavorable trans-caval anatomy.
Case report
Institutional review board permission was not required to report this case. The patient is a 63-year-old gentleman with past medical history of end-stage interstitial lung disease and secondary pulmonary hypertension on 4-l home oxygen, awaiting lung transplant. He presented to the emergency department with worsening shortness of breath. On examination, he was tachypneic with use of accessory muscles. Blood pressure 120/72 mmHg, pulse 92/min, respiratory rate of 39 breaths/min, and oxygen saturation was 95% on FiO2 of 10 L/min. Chest X-ray showed bilateral infiltrate. The patient was empirically started on broad spectrum antibiotics and admitted to the medical intensive care unit. Over the next 72 h despite maximal medical optimization, his respiratory status continued to decline, and he required emergent endotracheal intubation. Given his rapid course of disease and acceptable rehabilitation potential, the decision was made to take the patient to the operating theater and proceed with VV ECMO as a bridge to transplantation.
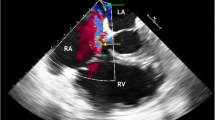
While many institutions perform ECMO cannulations at the bedside, at our institution, we preferentially perform our cannulations in the operating theater to allow for both fluoroscopy as well as transesophageal echocardiogram which enables us to direct wire placement, as well as cannula orientation. We obtained central venous access with ultrasound guidance and Seldinger technique through the right internal jugular vein. However, given the acute trans-caval angulation, we had difficulty obtaining trans-caval access required for the single site, dual-lumen Avalon cannula (Avalon Laboratories, California). We experienced the wire entering the right ventricle and buckling in the right atrium, both of which have the inherent potential to create perforations in the right atrium/ventricle/coronary sinus/tricuspid valve leaflet. Instances like these can be remedied with changing wire stiffness, employing torque devices, and the utilization of guiding catheters, as we did. In centers where ECMO is less readily utilized, it is safe to proceed with dual site cannulation; however, it comes with the tremendous sacrifice of patient mobilization. In this setting of unfavorable caval anatomy, we advocate utilizing a directing catheter to obtain trans-caval access. Here, we employed a multipurpose Slip-Cath® Tip catheter (Cook Medical, Bloomington, IN) (Fig. 1) and were able to direct the wire into the inferior vena cava and successfully position it in the trans-caval position (Fig. 2b). At this point, if trans-caval access is not readily obtained, a venogram should be performed to better orient the operator to the inferior vena cava orifice. We subsequently complete single site, dual-lumen cannulation for VV ECMO (Fig. 3b, and the ensuing intraoperative transesophageal echocardiogram confirmed the arterial lumen to be positioned toward the tricuspid valve.

Fluoroscopy image displaying multipurpose Slip-Cath® Tip catheter

a Fluoroscopy image of wire in the trans-caval position in the setting of favorable anatomy and b fluoroscopy image of wire in the trans-caval position in the setting of unfavorable anatomy

a Fluoroscopy image showing successful single site, dual-lumen VV ECMO cannulation in the setting of favorable anatomy and b Fluoroscopy image showing successful single site, dual-lumen VV ECMO cannulation in the setting of unfavorable anatomy
Comment
Many times, when there is minimal angulation and favorable trans-caval anatomy, we can obtain trans-caval access (Fig. 2a) and subsequently cannulate (Fig. 3a) without the aid of wire exchanges, torque devices, or even guiding catheters. However, in the instances of extreme angulation and unfavorable anatomy, persistent wire manipulation can lead to iatrogenic injury to the right atrium/ventricle/coronary sinus/tricuspid valve leaflets [5]. ECMO cannulation can be daunting even in expert hands, and so having an array of tools and techniques to employ can better enable successful ECMO cannulation. We believe that utilizing guiding catheters in challenging instances of unfavorable trans-caval anatomy can increase the number of cases of successful single site, dual-lumen ECMO cannulation.
References
Lewandowski K, Rossaint R, Pappert D, Gerlach H, Slama KJ, Weidemann H, et al. High survival rate in 122 ARDS patients managed according to a clinical algorithm including extracorporeal membrane oxygenation. Intensive Care Med. 1997;23:819–35.
Javidfar J, Brodie D, Wang D, Ibrahimiye AN, Yang J, Zwischenberger JB, et al. Use of bicavaldual-lumencatheter for adult venovenous extracorporeal membrane oxygenation. Ann Thorac Surg. 2011;91:1763–8.
Bermudez CA, Rocha RV, Sappington PL, Toyoda Y, Murray HN, Boujoukos AJ. Initial experience with single cannulation for venovenous extracorporeal oxygenation in adults. Ann Thorac Surg. 2010;90:991–5.
Hirose H, Yamae K, Marhefka G, Cavarocchi N. Right ventricular rupture and tamponade caused by malposition of the Avalon cannula for venovenous extracorporeal membrane oxygenation. J Cardiothorac Surg. 2012;7:36.
Paden ML, Conrad SA, Rycus PT, Thiagarajan PR. Extacorporeal life support organization registry report 2012. ASAIO J. 2013;59:202–10.
Acknowledgements
We would like to acknowledge Hannah Jeng for her efforts in formatting our figures.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All of the authors are in agreement with the content in the manuscript. There are no sources of financial support in the form of grants, equipment, and/or pharmaceutical items for this research. There are no potential conflicts of interest for all authors. This has been presented as a poster at the American Lung Association Tri-State Conference in 2016. It has not been published previously and is not currently under consideration elsewhere. Thank you for considering our manuscript for publication.
Ethical approval
All procedures performed were in accordance with the ethical standards of the institution and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statement of informed consent
Informed consent was obtained from participants.
Human and animal rights and informed consent
All procedures followed were in accordance with the institutional and national ethical standards. No local institutional review body approval was required for this case.
Additional information
No research scholarship awarded
Rights and permissions
About this article

Cite this article
I-Hun Jeng, E., Klodell, C.T., Beaver, T.M. et al. Catheter-directed guidance for ECMO cannulation with unfavorable caval anatomy. Indian J Thorac Cardiovasc Surg 34, 391–393 (2018). https://doi.org/10.1007/s12055-017-0585-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-017-0585-z