
Abstract
Misfolding and accumulation of aberrant α-synuclein in the brain is associated with the distinct class of neurodegenerative diseases known as α-synucleinopathies, which include Parkinson’s disease, dementia with Lewy bodies and multiple system atrophy. Pathological changes in astrocytes contribute to all neurological disorders, and astrocytes are reported to possess α-synuclein inclusions in the context of α-synucleinopathies. Astrocytes are known to express and secrete numerous growth factors, which are fundamental for neuroprotection, synaptic connectivity and brain metabolism; changes in growth factor secretion may contribute to pathobiology of neurological disorders. Here we analysed the effect of α-synuclein overexpression in cultured human astrocytes on growth factor expression and release. For this purpose, the intracellular and secreted levels of 33 growth factors (GFs) and 8 growth factor receptors (GFRs) were analysed in cultured human astrocytes by chemiluminescence-based western/dot blot. Overexpression of human α-synuclein in cultured foetal human astrocytes significantly changes the profile of GF production and secretion. We found that human astrocytes express and secrete FGF2, FGF6, EGF, IGF1, AREG, IGFBP2, IGFBP4, VEGFD, PDGFs, KITLG, PGF, TGFB3 and NTF4. Overexpression of human α-synuclein significantly modified the profile of GF production and secretion, with particularly strong changes in EGF, PDGF, VEGF and their receptors as well as in IGF-related proteins. Bioinformatics analysis revealed possible interactions between α-synuclein and EGFR and GDNF, as well as with three GF receptors, EGFR, CSF1R and PDGFRB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Alpha-synuclein is a 140 amino-acid protein encoded by synuclein alpha (SNCA) gene widely expressed in the central nervous system (CNS). In neurones, α-synuclein contributes to neuroprotection, suppression of apoptosis of dopaminergic neurones, stabilisation of soluble NSF attachment protein receptor (SNARE)-complex structure, maintenance of vesicular trafficking in the perisynaptic terminals [1,2,3], and other, yet uncharacterised functions. Misfolding and accumulation of aberrant α-synuclein in the brain is associated with the distinct class of neurodegenerative diseases known as α-synucleinopathies. This class of disorders includes Parkinson’s disease (PD), dementia with Lewy bodies (DLB) and multiple system atrophy (MSA) [3]. The latter pathology is characterised by accumulation of glial cytoplasmic inclusions in oligodendrocytes, whereas the former two disorders are associated with appearance of intraneuronal filamentous Lewy bodies or Lewy dendrites [4, 5].
Although physiological expression of α-synuclein in astrocytes is rather low, there is ample evidence demonstrating astroglial accumulation of α-synuclein in pathology. Inclusions of α-synuclein have been detected in the post-mortem PD and DLB (but not in MSA) brain samples [6,7,8], which reflects substantial astroglial accumulation of this protein in the course of the disease [9, 10]. Astrocytes represent a class of neuroglial cells fundamentally responsible for homoeostasis of the CNS at all level of organisation from molecular to organ [11]. Astrocytes contribute to all neurological diseases; astrogliopathology is complex and includes (i) reactive astrogliosis, (ii) astroglial pathological remodelling and (iii) astrodegeneration with cellular atrophy and loss of function [12]. In α-synucleinopathies astrocytes present several pathological signatures. In MSA astrocytes become reactive, whereas DLB and PD are not associated with astrogliosis; in the midbrain of PD sufferers astrocytes undergo apoptotic cell death [13]. Overexpression of human mutant A53 α-synuclein under control of astroglial (glial fibrillary acidic protein-GFAP) promoter results in rapid neurodegeneration due to the compromised astrocytic glutamate uptake [14].
Astrocytes are bona fide secretory cells, which form gliocrine system and release over 200 neuroactive substances including neuromodulators, neurohormones, trophic factors, modulators of synaptogenesis, etc. [15]. In particular, astrocytes are synthesising and secreting an impressive array of growth factors (GFs) including brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), glia-derived neurotrophic factor (GDNF), basic fibroblast growth factor (bFGF), platelet-derived growth factor (PDGF), hepatocyte growth factor (HGF), insulin-like growth factors (IGFs) and vascular endothelial growth factor (VEGF-B) [16]. These growth factors regulate multiple signalling pathways and functional responses; they are related to cell growth and differentiation, synaptic transmission, angiogenesis and wound healing; GFs regulate expression of N-methyl-D-aspartate (NMDA) receptors and antioxidant enzymes such as superoxide dismutase (SOD) and glutathione (GSH) reductase [17, 18]. In the present paper we report in depth analysis of expression and secretion of growth factors and modification of the growth factor profile by specific overexpression of α-synuclein in human foetal astrocytes.
Materials and Methods
Human Astrocyte Cultures
Primary foetal human astrocytes were obtained from ScienCell Research Laboratories (Lonza, Walkersville, CC-2565 NHA Batch no: 0000514417; 17 WG, male). Astrocytes were cultured in Clonetics™ AGM™ BulletKit™ (CC-3186), containing one 500 ml bottle of Astrocyte Basal Medium (ABM™) and the following Growth Supplements: rhEGF, 0.5 ml; Insulin, 1.25 ml; Ascorbic Acid, 0.5 ml; GA-1000, 0.5 ml, L-Glutamine, 5.0 ml; FBS, 15 ml. Cells were subcultured when they reached 70-80% confluency. Cells were seeded to 6 well plates 4x104 cells/cm2 and incubated at 37°C and 5% CO2 in a humidified atmosphere. Since the primary astrocyte culture loose its ability to maintain its character after fourth subculture, all experiments carried out with passage number less than four.
Experimental Design and α-Synuclein Transfection
Following experimental groups were established: (i) Control group; (ii) SNCA group of astrocytes transfected with SNCA gene (Human synuclein, α (non A4 component of amyloid precursor), transcript variant 1; SNCA NM_000345 Human Tagged ORF Clone TrueORFGold oriGene cat no: RC210606); (iii) Negative control or MOCK group, which was treated with mock plasmid containing CMV promoter and Myc-DDK tag but no open reading frame (ORF) for any gene (pMVC6-Entry, mammalian vector with C-terminal Myc-DDK Tag, oriGene cat no: PS100001). This group was used to distinguish between mimicry and inhibitory/activatory effects and true effect caused by α-synuclein transfection.
For avoiding the adverse effect of transfection [19] we compared two different transfection techniques: (i) magnetic nanoparticles (Magnetofection NeuroMag-Oz Bioscience NM50500) and (ii) lipid based agents (Lipofectamine LTX with Plus Reagent Invitrogen™ 15338-100 or TurboFectin 8.0 Origene TF81001). Cytotoxicity was detected to select the most appropriate transfection technique or reagent and according the results (data not shown) Turbofection 8.0 was selected because of low cytotoxicity; antibiotics were not used after first passage.
Lipid based transfection reagent (TurboFectin 8.0)/plasmid complex was prepared by diluting plasmids in ABM a 1:250 (μg:μl) and adding 3 μl of TurboFectin 8.0 (ORIGENE TF81001) according to manufacturer’s protocol. All transfections were performed on cultures that reached 70% confluency (7 – 8 days in culture). Culture medium was replaced with serum-free medium 24 h prior to the transfection. Cells were transfected with the SNCA plasmid or mock plasmid for 24 h. After 24 h, medium was replaced with fresh, serum-free medium and protein isolation was performed at 48 or 72 h of treatments and the supernatants were collected at the same time points. Transient transfection of astrocytes was performed and transfection success was monitored at 48 and 72 h of treatments with quantitative real-time polymerase chain reaction (qRT-PCR) or immunofluoresence labelling [20].
Quantitative Real-Time Polymerase Chain Reaction
RNA isolation was performed with a PureLink RNA Mini Kit (Thermo Fischer 12183018A) at 48 and 72 h after transfection. RNA was set to 20 ng/μL for each sample during the cDNA synthesis reaction with a iScript™ cDNA Synthesis Kit (Biorad #1708891). SNCA mRNA level was analyzed by qRT-PCR with Universal Probe Library (UPL) probe and a Lightcycler 480 Probe Master Mix kit (Roche 04707494001) with LIGHTCYCLER 480. Primers and probe were as follows: NM_000345.3 Homo sapiens synuclein α (SNCA), transcript variant 1, UPL Probe #0.25 (Roche 04686993001). NM_012423.2 Homo sapiens ribosomal protein L13a (RPL13A) UPL Probe #28, Roche 04687604001) were used as endogenous reference gene for normalisation. Each qRT-PCR was performed in triplicates for a single experiment, and each experiment was repeated three times independently.
Immunofluorescence
Cellular localisation and expression of α-synuclein, DDK-tag, GFAP and ALDH1L1 were identified by immunofluorescent labelling (IF). Astrocytes were labelled with GFAP and ALDH1L1 antibodies Astrocytes were fixed with 3.7% paraformaldehyde (pH 7.4), and blocked with 30% goat serum in 0.02% T-PBS for 1 h at room temperature. Subsequently, cells were incubated with primary antibodies to GFAP (1:200, Millipore AB5804 Millipore Corp. California, USA), ALDH1L1 (1:25, Millipore MABN495 Millipore Corp. California, USA), anti-DDK (Clone OTI4C5 mouse monoclonal Antibody ORIGINE Lot:A043) and anti-α-syn-211 (1:250, Thermo Scientific, Thermo Fisher Scientific Inc. Illinois, USA Lot:SC244203) overnight at 4 °C. On the second day, they were further processed with corresponding secondary antibodies (Alexa Fluor® 568, Abcam, ab175471 or Fluorescein isothiocyanate Millipore AP181F California, USA).
Cells were examined under inverted fluorescence microscope Leica DMIL, (Leica Microsystems Ltd., Heerbrugg, Germany) and imaged with fluorescence camera system (Leica DFC 300 FX, Leica Microsystems Ltd., Heerbrugg, GE) using TR, I3 and A3 filters. Images of the same area taken with different filters were overlaid using dedicated software (The Leica Application Suite Image Overlay Software, Leica Microsystems Ltd., Heerbrugg, GE). Some imaging experiments were made using Leica TCS SP8 confocal microscope with LasX software (Leica Microsystems Ltd., Heerbrugg, Germany) or Lionheart FX Automatic Fluorescent Microscope with Gen5 (BioTek, Winooski, USA) software. ImageJ 1.44a software was used to analyse immunofluorescent intensities. Briefly, at least ten images of random areas from each group were analyzed for anti-DDK or α-synuclein expression; the corrected total cell fluorescence (CTCF) was determined and calculated as CTCF = integrated density − (area of selected cell × mean fluorescence of background readings) as previously described [20, 21].
Human Growth Factor Antibody Array
Total protein extracts from 2x106 cells were obtained with M-PER Mammalian Protein extraction reagent (78501, Thermo Scientific USA) including 0.75% Halt Protease Inhibitor (78429, Thermo Scientific, USA) and 1× Phos-Stop (04906845001, Roche USA) phosphatase inhibitor according to the manufacturer’s protocol. The protein concentrations were assessed using a Qubit 2.0 Fluorometer (Invıtrogen, USA). The GF antibody array was repeated three times using samples from three independent cell cultures.
The following growth factors were detected in cell lysates and supernatants by chemiluminescence based western dot blot method using Ray Biotech C-Series Human Growth Factor Antibody Array C1 (cat. no: AAH-GF-1-8): Basic fibroblast growth factor (bFGF), β-nerve growth factor (βNGF), epidermal growth factor (EGF), epidermal growth factor receptor (EGFR), FGF-4, FGF-6, FGF-7, granulocyte colony stimulating factor (G-) CSF), glia-derived neurotrophic factor (GDNF), granulocyte macrophage colony stimulating factor (GM-CSF), heparin binding EGF-like growth factor (HB-EGF), hepatocyte growth factor (HGF), insulin-like growth factor binding protein-1 (IGFBP-1), IGFBP-2, IGFBP-3, IGFBP-4, IGFBP-6, insulin-like growth factor-1 (IGF-1), anti-insulin-like growth factor-I receptor (IGF-I sR), IGF-2, macrophage colony stimulating factor (M-CSF), macrophage colony stimulating factor receptor (M-CSFR), neurotrophin-3 (NT-3), neurotrophin-4 (NT-4), platelet-derived growth factor (PDGF AA, PDGF AB, PDGF BB), platelet-derived growth factor receptor alpha (PDGFRa, PDGF Rb, placental growth factor (PIGF), stem cell growth factor (SCF), stem cell growth factor receptor (SCFR), transforming growth factor-α alpha (TGF-α), TGF-β, TGF-β2, TGF-β3, vascular endothelial growth factor (VEGF), vascular endothelial growth factor receptor 2 (VEGF R2), VEGF R3, VEGF D.
Cytotoxicity Assay
Cytotoxicity was determined by measuring the levels of lactate dehydrogenase (LDH) secreted to the culture medium after 72 h of treatment using ELISA in a cytotoxicity detection kit (Roche 11 644 793 001, Roche Diagnostics GmbH Roche Applied Science Mannheim, GE) according to manufacturer’s protocol as previously described [22,23,24]. Each sample was measured in triplicate.
Statistical Analysis
Preliminary analysis of growth factor expression and release was performed with RayBio Analysis Tool-SO2-AAH-GF-1. Trophic factor levels, cytotoxicity assays and corrected total cell fluorescence (CTCF) values were compared using GraphPad InStat DTCG 3.06 (GraphPad Software, Inc. San Diego USA) or SPSS 24.0 software. Comparisons were performed according to whether the data are normally distributed and whether the difference between the SDs obtained is significant, first by one-way ANOVA, followed by Tukey Kramer Multiple Comparison tests for multiple comparisons, or first with Kruskal Wallis and then with Dunn’s Multiple Comparison tests for multiple comparisons. Bonferroni adjustment was performed when required. p < 0.05 was accepted as statistically significant difference.
Cycle threshold (Ct) values that were obtained from qRT-PCR were calculated by the ΔCt = 2 (Geometric mean of reference genes - Ct target gene) formula for determining relative target gene expression levels of groups as previously described [20]. The 95% Confidence Interval (CI) values of intracellular or secreted GF/GF receptors levels of each group of human astrocytes were calculated. The 95% CI values were set as upper or lower threshold values for detected GF levels.
Corrected total cell fluorescence values of the cells labelled with anti-DDK antibody were used to determine the efficacy of transfection. The upper value of the 95% CI of the CTCF values of the anti-DDK labelling of the control group was considered the threshold value. The percentage of cells in the SNCA group with a higher CTCF value than the upper threshold of the control group is 57%, indicating transfection percentage of 57%.
The CTCF values of cells labelled with anti-α-synuclein antibody were also used to determine an increase in α-synuclein expression increased. The upper value of the 95% CI of the CTCF values of the anti-α-synuclein labelling of the MOCK group was considered the threshold. The percentage of cells in the SNCA group with CTCF above the threshold of the MOCK group is 80, indicating that α-synuclein expression increased by 80% after transfection.
Protein-Protein Interaction and Pathway Analysis
The potential interaction of α-synuclein and target proteins was evaluated with a web-based prediction tool, the FpClass tool (https://omictools.com/fpclass-tool) which is a data mining-based method for proteome-wide protein-protein interaction (PPI) prediction. Protein IDs of target proteins were used for the analysis of PPI prediction as previously described [25]. The levels of proteins of groups were analyzed to determine the most significant pathways by Reactome Pathway Browser 3.6 [26, 27]. The altered proteins in treatments were used for the pathway analysis in STRING (https://string-db.org/) [28] and Cytoscape 3.8.0 [29].
Results
Expression of α-Synuclein in Human Cultured Astrocytes
Astrocytes in control cultures were characterised by polymorphic morphology and expression of classical astroglial markers GFAP and ALDH1L1 (Fig. 1). GFAP was expressed by 85 ± 8.7%, n = 682 of cells, while 93 ± 3.6% of cells expressed ALDH1L1, n = 745 cells. Transfection of astrocytes with α-synuclein affected neither cell morphology nor their immunocytochemical profile; 88 ± 5.3%, n = 414 of transfected astrocytes were immunopositive for GFAP and 92 ± 7.1%, n = 438 of cells were immunopositive for ALDH1L1 (Fig. 2A–C).

Morphological features of cultured human astrocytes. A–F Human astrocytes labelled with the ALDH1L1 and GFAP antibodies (ALDH1L1-green, GFAP-red). G Morphological diversity of GFAP-positive astrocytes

Expression of α-synuclein at 72 h in mock and SNCA experimental groups. A–C Efficiency of plasmid transfection was demonstrated by anti-DDK antibody (green); nuclei were labelled with DAPI (blue). (A) Untreated control group, (B) MOCK group, (C) SNCA group. (Both MOCK and SNCA groups include DDK tag in order to demonstrate transfection.) D–F Astrocytes labelled with α-synuclein antibody (green) and DAPI (blue). (D) Control group, (E) MOCK group, (F) SNCA group. G Evaluation of the CTCF of DDK labelling between the groups. DDK CTCF of MOCK and SNCA groups was significantly increased compared with the control group (p < 0.01, p < 0.05 respectively). H Evaluation of CTCF of α-synuclein between groups. The CTCF of α-synuclein increased significantly in the SNCA plasmid treated group compared with the untreated control or MOCK plasmid treated groups (p < 0.001). I Cytotoxicity was determined by LDH levels of the groups at 72 h. LDH release of untreated control group was accepted as 0%. No statistically significant difference was observed between groups after 72 h of transfections (p > 0.05). J–S ALDH1L1 (green) and GFAP (red) labelling of control, negative control (mock) and α-synuclein overexpressing astrocytes. The CTCF of AdhL1 and GFAP did not change between groups (p > 0.05; n = 470)
The efficiency of α-synuclein transfection was determined by mRNA analysis, as well as by anti-DDK and anti-α-synuclein staining of cultured astrocytes. The qRT-PCR demonstrated that expression οf α-synuclein mRNA significantly increased in SNCA transfected astrocytes at 48 or 72 h after transfection. The results for relative mRNA expression of groups were as follows (mean ± SD): (i) at 48 h after transfection mRNA expression was for control group 0.09 ± 0.01; for MOCK group 0.05 ± 0.02, for SNCA group 328.9 ± 69.5, p values were < 0.0001 (p values after MTC are: control vs. MOCK p > 0.05, control vs. SNCA p < 0.001, MOCK vs. SNCA p < 0.001); (ii) at 72 h after transfection expression was: control 0.001 ± 0.0009, MOCK group 0.04 ± 0.03), SNCA group 187.9 ± 79.9; p values were < 0.003 (after MTC control vs. MOCK p > 0.05, control vs. SNCA p < 0.01, MOCK vs. SNCA p < 0.01) for 72 h of treatment.
The total corrected cell fluorescence, CTCF, of anti-DDK labelling of MOCK and SNCA groups were significantly increased compared with the control group (Fig. 3A–D). Overexpression of α-synuclein was demonstrated by specific immunofluorescent labelling. The CTCF of anti-α-synuclein labelling increased significantly in the SNCA group compared with both the untreated control and MOCK groups (Fig. 3E–H). Transfection with SNCA did not affect cell viability: no statistically significant difference was observed between LDH levels of the groups up to 72 h after transfection (Fig. 3I).

GF profile of cultured human astrocytes in control conditions. A The dot blot of human astrocytes and the table indicating target names and their positions. B Growth factor expression profile of untreated human astrocytes. Yellow colour labels proteins detected above the high threshold value, white colour shows the proteins at the average values and grey colour shows the proteins below the low threshold value (95% CI for intracellular protein levels of untreated astrocytes: GFs—95% CI 0.21–0.28, GF receptors—95% CI 0.16–0.27; 95% CI for secreted protein levels of untreated astrocytes: GFs—95% CI 0.23–0.31, GF receptors—95% CI 0.17–0.31)
GF Profiles of Cultured Human Astrocytes Are Affected by α-Synuclein Overexpression
Using dot blot array we determined intracellular and secreted levels of GF in astroglial cultures; we also measured intracellular and secreted levels of 8 receptors for GFs. Results of our experiments are summarised in Tables 1 (intracellular proteins) and 2 (secreted proteins).
Expression profile of growth factors in the control astrocytes was refined by using 95% CI values of intracellular or secreted GF/GF receptors levels of untreated human astrocytes as cut-off values for upper or lower threshold levels. The 95% CI was calculated from the average GFs/GFRs at 48 h and 72 h as presented in Tables 1 and 2. EGF, FGF2, IGF1, AREG, IGFBP2-4, FGF6, VEGFD, PDGFB, KITLG, PGF, PDGFA, IGF1R and CSF1R were expressed at higher levels (the 95% CI for intracellular protein levels of untreated astrocytes: GFs—95% CI 0.21–0.28, GF receptors—95% CI 0.16–0.27), whereas IGFBP2, EGF, IGF1, VEGFD, IGFBP4, PDGFA, AREG, FGF6, TGFB3, PGF, NTF4, FLT4 and IGFR1 were secreted at higher levels by untreated human astrocytes (95% CI for secreted protein levels of untreated astrocytes: GFs—95% CI 0.23–0.31, GF receptors—95% CI 0.17–0.3) (Fig. 3, GF profile for each time point is shown in Supplementary Figure 1).
Modifications of GF profile by α-synuclein overexpression are presented in Tables 1 and 2. Intracellular levels of EGF, FGF4, NGF, IGFBP1-4 and 6, PDGFAA, VEGFD and FLT4 increased, whereas HBEGF, KITLG, NTF3, NTF4, GDNF, CSF2, and CSF1R decreased at 48 h in SNCA group compared with MOCK group after Bonferroni adjustment (BA). At 72 h in the SNCA group, KITLG, FGF6 intracellular levels increased; HBEGF, NTF4, GDNF, CSF1, IGF2, PDGFAA, TGFB1 and CSF1R intracellular levels decreased compared with MOCK group after BA.
At 48 h after transfection in SNCA plasmid treated group secreted levels of FGF4, IGFBP3, PDGFAA, and FLT4 increased, while EGF, HBEGF, HGF, PGF, NGF, NTF3, NTF4, GDNF, CSF2, IGFBP2, IGFBP4 and 6, and CSFR1, PDGFRA decreased when compared with MOCK group after Bonferroni adjustment. At 72 h in SNCA group secreted levels of PDGFBB increased, whereas secretion of VEGFD decreased when compared with MOCK group after Bonferroni-adjustment. All results presented in Tables 1 and 2 are summarised in Fig. 4, which includes only the proteins altered by α-synuclein overexpression significantly after Bonferroni-adjustment (αc value for GFs = 0.002; αc value for GF receptors = 0.006).

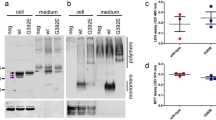
Effect of α-synuclein overexpression on GF profile of human astrocytes. A The dot blot membranes of MOCK plasmid or SNCA plasmid treated human astrocytes and the table with the target names and their positions were shown. B Alterations in GF and GF receptors in α-synuclein overexpressing human astrocytes, created according to the data presented in Tables 1 and 2. The figure includes only the proteins which were altered by 〈α-synuclein overexpression significantly after Bonferroni-adjustment (αc value for GFs = 0.002; 〈c value for GF receptors = 0.006).
Bioinformatic Analysis of GF Expression And Secretion
Reactome pathway results are presented in Supplementary Table 1. The 95% CI values of secreted GF levels were used to determine which GF is detected above the high threshold value. Accordingly, in the SNCA group only KITLG, CSF1, IGF2, PDGFAB, PDGFBB were secreted at level higher than the upper threshold. On the other hand, EGF, IGF1, IGFBP4, AREG, TGFB3 and GDNF were secreted at higher level than the upper threshold in control and MOCK groups but not in SNCA group. Additionally, intracellular levels of FGF2, AREG, IGFBP2, 4, PDGFAA, BB and AB, PGF in SNCA group was higher than the upper threshold when compared with MOCK group.
Levels of GFs and GF receptors in the cell and in the extracellular medium in α-synuclein overexpressing human astrocytes are shown in Fig. 4B. The figure presents only GFs and their receptors levels of which were altered significantly as confirmed by Bonferroni test. These data points were used for the pathway analysis in STRING (Fig. 5A). The analysis showed that there is almost no known information about interactions between synuclein and the GFs/GFRs, levels of which change with the overexpression of α-synuclein, except predicted interaction with EGFR and GDNF. Reactome analysis of these proteins showed significant pathways, the pathways and false discovery rate (FDR) scores are presented in Fig. 5B and Supplementary Table 1. Among the GFs that we investigated, the PPI tool showed a possibility for α-synuclein and bFGF interaction (total score: 0.70). Additionally, three GF receptors, EGFR, CSF1R and PDGFRB were also predicted to be interacting with α-synuclein (Total Score: 0.84, 0.43, and 0.34, respectively). According to our analysis possible relations between α-synuclein and significantly changed GFs or GFRs were created by Cytoscape 3.8.0 (Fig. 5C).

PPI and Pathway analysis. A Protein levels of which were changed α-synuclein overexpressing astrocytes. STRING analysis shows that α-synuclein is related only to EGFR and GDNF. B Top 10 related reactome pathways (see also Supplementary Table 1). C Possible relations between 〈α-synuclein and significantly changed GFs or GFRs were created by Cytoscape 3.8.0 [29]. The information from text mining in in green, from databases in turquoise and data from this study are in black
Discussion
This study reports the profiles of intracellular expression and secretion of growth factors and major growth factor receptors in human foetal cultured astrocytes. To the best of our knowledge this is the first in depth analysis of expression and secretion of growth factors by human astrocytes. We analysed protein expression of 33 growth factors (GFs) and 8 growth factor receptors (GFRs).
We found high levels of expression and secretion of GFs associated with RAF/MAPK and PI3K/Akt signalling pathways [30, 31]. These are FGF2 and FGF6, EGF, IGF-1, AREG, IGFBP2 and IGFBP4, VEGFD, PDGFs, KITLG, PGF, TGFB3 and NTF4; expression level of these GFs was relatively higher compared with neurotrophic factors such as NGF, GDNF, NTF3 (Fig. 4A). Intracellular expression and secretion of NGF was below the threshold whereas NTF4 was the highest expressed and secreted neurotrophic factor. Additionally, Insulin growth factor 1 (IGF-1) receptor, Fms Related Receptor Tyrosine Kinase 4 (FLT4) and Colony Stimulating Factor 1 Receptor (CSF1R) were expressed and released by human astrocytes. The IGF-1 is one of the major regulators of RAF/MAPK and PI3K/Akt cascades [32]; human astrocytes expressed IGF-1, its receptor IGF-1R and IGF binding proteins (IGFBPs; particularly IGFBP2 and 4).
All data for the effects of SNCA overexpression were gathered from the comparison between MOCK and SNCA (α-synuclein overexpressing) groups in order to avoid false positive or negative results that may occur with the transfection of the plasmid backbone [19]. First, we analysed levels of GFs within the groups themselves to identify the levels of GF expression and release in a single group. Overexpression of α-synuclein in human astrocytes affected the profile of GF expression. We detected an increase in the intracellular levels of FGF2, AREG, IGFBP2 and 4, PDGFAA, BB and AB, PGF and an increase in secretion of KITLG, CSF1, IGF2, PDGFAB, PDGFBB. At the same time release of EGF, IGF1, IGFBP4, AREG, TGFB3 and GDNF decreased.
Release of NGF was decreased, despite an increase in the intracellular level in SNCA group. Our results mostly support the studies which suggested modification of neurotrophic factors in neurodegenerative diseases [33]. However, neither expression nor release of these neurotrophic factors was higher than other GFs. NTF4 was predominant neurotrophin in human astrocytes. On the other hand, NTF3 and especially NGF release and expression were lower compared with the majority of other GFs.
According to our results, IGF-I is one of the highest synthesised growth factor in human astrocytes. IGF-1 is a potent trophic factor that decreases significantly with age [34]. IGF-1 signals through the conjugated receptor, IGFR. IGF-1 ligand binding activates downstream signalling cascades, including the prototypic PI3K/Akt pathway, which regulates cell survival and growth [35]. The IGF-1 signal regulates essential aspects of astrocyte function, including glucose uptake, regulation of glutamate transport, and protection against oxidative stress in the brain [36, 37]. Astrocyte-specific overexpression of IGF-1 protects hippocampal neurones and improves cognitive impairment caused by oxidative stress following traumatic brain injury [38]. Knockout of IGFR makes astrocytes more susceptible to peroxide-induced cytotoxicity [35]. Majority of circulating IGF-I is linked to six different IGFBPs. On the cell surface or in the extracellular matrix, IGFBPs may inhibit or increase the delivery of IGF-I to the receptor [39]. Our results revealed relatively high levels of IGF and IGFBPs2,4 in all experimental groups. These results are in agreement with previous studies that predominantly find IGFBP2,4,5 expression in the brain [39]. Overexpression of α-synuclein significantly increased intracellular levels of IGF1 and IGFBPs at 48 h after transfection. Release of IGF1 and IGFBPs, however, was significantly decreased. Arguably α-synuclein limits the release of these factors, thus the intracellular levels of these proteins are increased. In this scenario α-synuclein aggregation might initially affect IGF metabolism which impairs upon RAF/MAPK and PI3K/Akt pathways thus contributing to neurodegeneration [32]. Decreased IGF1 signalling in astrocytes affects their supportive capabilities under conditions of stress and this is associated with defects in the mitochondrial respiratory chain in astrocytes and is related to neurodegeneration [40].
We found that PDGF-AA and PDGF-BB are highly expressed and secreted by astrocytes (Fig. 4A). Overexpression of α-synuclein increased secreted levels of PDGF-AA and PDGF-BB. Secreted PDGFRB level did not change, while intracellular level of this protein increased. Increased expression of PDGF and PDGF-R was found in lesioned areas of CNS in studies on experimental animal models of stroke, Huntington’s and Parkinson’s diseases [41, 42]. PDGFR-B activates the Akt pathway, promoting neuronal survival and produces a more potent anti-apoptotic effect than PDGFR-A [43,44,45].
Recent studies demonstrated that glia maturation factor (GMF) is highly expressed in astrocytes, and its expression is altered in several neurological conditions [46,47,48]. Although we did not include GMF in our analysis we may speculate that, similarly to other growth factors, α-synuclein may also affect production and release of GMF.
We used Fp-Class PPI prediction tool in order to determine possible interactions between α-synuclein and GFs or their receptor. Among the GFs that we investigated, the PPI tool showed only a possibility for interaction between α-synuclein and bFGF (FGF2). Three receptors, EGFR, CSF1R and PDGFRB were also predicted to be interacting with α-synuclein. Although the PPI score of CSF1R and PDGFRB are low, the intracellular levels of this three receptors and extracellular level of CSFR1 were affected by overexpression of α-synuclein. In addition, the intracellular and extracellular levels of VEGFD and FLT4 (VEGFR3), which is receptor for VEGFD, were increased in α-synuclein overexpressing cells. VEGF induces angiogenesis, exhibits neuroprotective and neurotrophic properties and is secreted by astrocytes under hypoxia conditions. VEGF can also increase astrocyte proliferation and neurogenesis, and contribute to the survival of neurones and astrocytes. Inhibition of VEGF reduces angiogenesis and astrocyte proliferation in the brain injury [49]. The fact that VEGFD and its receptor is one of the highest in untreated human astrocytes confirms the importance of this pathway, which might be one of the major targets for α-synuclein.
In astrocytes, as in many other cells, protein misfolding generates the unfolded protein response which is a part of endoplasmic reticulum (ER) stress, a complex cascade of molecular events aimed at the restoration of ER homeostasis [50]. It is widely acknowledged that α-synuclein interacts with ER chaperones, while overexpression of α-synuclein makes neuronal cells susceptible to ER stress-induced toxicity [51]. It has been also reported that α-synuclein mutation or overexpression may interfere with SNARE proteins [52, 53]. Besides, α-synuclein has been implicated in ER-Golgi secretion pathways [54]. The ER stress not only affects secretory pathways and protein synthesis but may compromise astroglial Ca2+ signalling [55]. We can therefore surmise that over-expression of α-synuclein in astrocytes leads to deterioration of early and late secretory pathways, including the endomembrane system. All these pathways are essential for regulation of synthesis and release of growth factors, and indeed, as we demonstrated, excessive expression of α-synuclein affects astroglial growth factor profile.
The GFs that we investigated are linked to RAF/MAPK or PI3K/Akt pathways according to Reactome pathway analysis but they are possibly separated from each other in downstream cascades. Neurotrophic factors, IGF-1, VEGF, PDGF, EGF, FGF, HGF, PDGF can stimulate signalling through intracellular PI3K/Akt or MAPK pathways which might trigger the ubiquitin proteasome system (UPS) and autophagy [56,57,58,59,60,61,62]. In physiological conditions the UPS is the main degradation pathway for α-synuclein while an increased α-synuclein burden recruits the autophagy-lysosomal pathway. Alterations of the UPS in α-synuclein overexpressing transgenic mice suggested that UPS role in α-synuclein degradation is age dependent [63]. There was a significant change in neurotrophic factors with α-synuclein, but the change in EGF, PDGF, VEGF and their receptors and IGF-related proteins appears to be more prominent. Furthermore, FpClass PPI data highlight pathways related to EGFR, PDGFRB and CSFR1, providing information about receptors with which α-synuclein can interact directly. We may suggest therefore, that α-synuclein has a potential to impact upon RAF/MAPK or PI3K/Akt pathways, which can regulate the response for protein misfolding and cell death in neurodegeneration.
Data Availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Bellani S, Sousa VL, Ronzitti G, Valtorta F, Meldolesi J, Chieregatti E (2010) The regulation of synaptic function by α-synuclein. Commun Integr Biol 3(2):106–109. https://doi.org/10.4161/cib.3.2.10964
Emamzadeh FN (2016) α-synuclein structure, functions, and interactions. J Res Med Sci 21:29. https://doi.org/10.4103/1735-1995.181989
Goedert M, Jakes R, Spillantini MG (2017) The synucleinopathies: twenty years on. J Parkinsons Dis 7(s1):S51–S69. https://doi.org/10.3233/JPD-179005
Spillantini MG, Crowther RA, Jakes R, Hasegawa M, Goedert M (1998) alpha-Synuclein in filamentous inclusions of Lewy bodies from Parkinson’s disease and dementia with lewy bodies. Proc Natl Acad Sci U S A 95(11):6469–6473. https://doi.org/10.1073/pnas.95.11.6469
Jellinger KA, Lantos PL (2010) Papp-Lantos inclusions and the pathogenesis of multiple system atrophy: an update. Acta Neuropathol 119(6):657–667. https://doi.org/10.1007/s00401-010-0672-3
Braak H, Sastre M, Del Tredici K (2007) Development of α-synuclein immunoreactive astrocytes in the forebrain parallels stages of intraneuronal pathology in sporadic Parkinson’s disease. Acta Neuropathol 114(3):231–241. https://doi.org/10.1007/s00401-007-0244-3
Wakabayashi K, Hayashi S, Yoshimoto M, Kudo H, Takahashi H (2000) NACP/α-synuclein-positive filamentous inclusions in astrocytes and oligodendrocytes of Parkinson’s disease brains. Acta Neuropathol 99(1):14–20. https://doi.org/10.1007/pl00007400
Song YJ, Halliday GM, Holton JL, Lashley T, O’Sullivan SS, McCann H, Lees AJ, Ozawa T et al (2009) Degeneration in different parkinsonian syndromes relates to astrocyte type and astrocyte protein expression. J Neuropathol Exp Neurol 68(10):1073–1083. https://doi.org/10.1097/NEN.0b013e3181b66f1b
Sorrentino ZA, Giasson BI, Chakrabarty P (2019) α-Synuclein and astrocytes: tracing the pathways from homeostasis to neurodegeneration in Lewy body disease. Acta Neuropathol 138(1):1–21. https://doi.org/10.1007/s00401-019-01977-2
Booth HDE, Hirst WD, Wade-Martins R (2017) The role of astrocyte dysfunction in Parkinson’s disease pathogenesis. Trends Neurosci 40(6):358–370. https://doi.org/10.1016/j.tins.2017.04.001
Verkhratsky A, Nedergaard M (2018) Physiology of astroglia. Physiol Rev 98(1):239–389. https://doi.org/10.1152/physrev.00042.2016
Verkhratsky A, Zorec R, Parpura V (2017) Stratification of astrocytes in healthy and diseased brain. Brain Pathol 27(5):629–644. https://doi.org/10.1111/bpa.12537
Kosel S, Egensperger R, von Eitzen U, Mehraein P, Graeber MB (1997) On the question of apoptosis in the parkinsonian substantia nigra. Acta Neuropathol 93(2):105–108. https://doi.org/10.1007/s004010050590
Gu XL, Long CX, Sun L, Xie C, Lin X, Cai H (2010) Astrocytic expression of Parkinson’s disease-related A53T α-synuclein causes neurodegeneration in mice. Mol Brain 3:12. https://doi.org/10.1186/1756-6606-3-12
Verkhratsky A, Matteoli M, Parpura V, Mothet JP, Zorec R (2016) Astrocytes as secretory cells of the central nervous system: idiosyncrasies of vesicular secretion. EMBO J 35(3):239–257. https://doi.org/10.15252/embj.201592705
Cabezas R, Avila-Rodriguez M, Vega-Vela NE, Echeverria V, Gonzalez J, Hidalgo OA, Santos AB, Aliev G et al (2016) Growth Factors and astrocytes metabolism: possible roles for platelet derived growth factor. Med Chem 12(3):204–210. https://doi.org/10.2174/1573406411666151019120444
Mattson MP (2008) Glutamate and neurotrophic factors in neuronal plasticity and disease. Ann N Y Acad Sci 1144:97–112. https://doi.org/10.1196/annals.1418.005
Peterson AL, Nutt JG (2008) Treatment of Parkinson’s disease with trophic factors. Neurotherapeutics 5(2):270–280. https://doi.org/10.1016/j.nurt.2008.02.003
Stepanenko AA, Heng HH (2017) Transient and stable vector transfection: pitfalls, off-target effects, artifacts. Mutat Res 773:91–103. https://doi.org/10.1016/j.mrrev.2017.05.002
Gezen-Ak D, Atasoy IL, Candas E, Alaylioglu M, Yilmazer S, Dursun E (2017) Vitamin D receptor regulates amyloid β1-42 production with protein disulfide isomerase A3. ACS Chem Neurosci 8(10):2335–2346. https://doi.org/10.1021/acschemneuro.7b00245
Atasoy IL, Dursun E, Gezen-Ak D, Metin-Armagan D, Ozturk M, Yilmazer S (2017) Both secreted and the cellular levels of BDNF attenuated due to tau hyperphosphorylation in primary cultures of cortical neurons. J Chem Neuroanat 80:19–26. https://doi.org/10.1016/j.jchemneu.2016.11.007
Dursun E, Gezen-Ak D, Yilmazer S (2014) The influence of vitamin D treatment on the inducible nitric oxide synthase (INOS) expression in primary hippocampal neurons. Noro Psikiyatr Ars 51(2):163–168. https://doi.org/10.4274/npa.y7089
Gezen-Ak D, Dursun E, Yilmazer S (2014) The effect of vitamin D treatment on nerve growth factor (NGF) release from hippocampal neurons. Noro Psikiyatr Ars 51(2):157–162. https://doi.org/10.4274/npa.y7076
Dursun E, Candas E, Yilmazer S, Gezen-Ak D (2019) Amyloid β1-42 Alters the expression of miRNAs in cortical neurons. J Mol Neurosci 67(2):181–192. https://doi.org/10.1007/s12031-018-1223-y
Dursun E, Gezen-Ak D (2017) Vitamin D receptor is present on the neuronal plasma membrane and is co-localized with amyloid precursor protein, ADAM10 or Nicastrin. PLoS One 12(11):e0188605. https://doi.org/10.1371/journal.pone.0188605
Fabregat A, Jupe S, Matthews L, Sidiropoulos K, Gillespie M, Garapati P, Haw R, Jassal B et al (2018) The reactome pathway knowledgebase. Nucleic Acids Res 46(D1):D649–D655. https://doi.org/10.1093/nar/gkx1132
Jassal B, Matthews L, Viteri G, Gong C, Lorente P, Fabregat A, Sidiropoulos K, Cook J et al (2020) The reactome pathway knowledgebase. Nucleic Acids Res 48(D1):D498–D503. https://doi.org/10.1093/nar/gkz1031
Szklarczyk D, Gable AL, Lyon D, Junge A, Wyder S, Huerta-Cepas J, Simonovic M, Doncheva NT et al (2019) STRING v11: protein-protein association networks with increased coverage, supporting functional discovery in genome-wide experimental datasets. Nucleic Acids Res 47(D1):D607–D613. https://doi.org/10.1093/nar/gky1131
Shannon P, Markiel A, Ozier O, Baliga NS, Wang JT, Ramage D, Amin N, Schwikowski B et al (2003) Cytoscape: a software environment for integrated models of biomolecular interaction networks. Genome Res 13(11):2498–2504. https://doi.org/10.1101/gr.1239303
Ramaswamy S, Kordower JH (2009) Are growth factors the answer? Parkinsonism Relat Disord 15(Suppl 3):S176–S180. https://doi.org/10.1016/S1353-8020(09)70809-0
Yasuda T, Mochizuki H (2010) Use of growth factors for the treatment of Parkinson’s disease. Expert Rev Neurother 10(6):915–924. https://doi.org/10.1586/ern.10.55
Pennuto M, Pandey UB, Polanco MJ (2020) Insulin-like growth factor 1 signaling in motor neuron and polyglutamine diseases: from molecular pathogenesis to therapeutic perspectives. Front Neuroendocrinol:100821. https://doi.org/10.1016/j.yfrne.2020.100821
Weis J, Saxena S, Evangelopoulos ME, Kruttgen A (2003) Trophic factors in neurodegenerative disorders. IUBMB Life 55(6):353–357. https://doi.org/10.1080/1521654031000153021
Sonntag WE, Ramsey M, Carter CS (2005) Growth hormone and insulin-like growth factor-1 (IGF-1) and their influence on cognitive aging. Ageing Res Rev 4(2):195–212. https://doi.org/10.1016/j.arr.2005.02.001
Logan S, Pharaoh GA, Marlin MC, Masser DR, Matsuzaki S, Wronowski B, Yeganeh A, Parks EE et al (2018) Insulin-like growth factor receptor signaling regulates working memory, mitochondrial metabolism, and amyloid-beta uptake in astrocytes. Mol Metab 9:141–155. https://doi.org/10.1016/j.molmet.2018.01.013
Suzuki K, Ikegaya Y, Matsuura S, Kanai Y, Endou H, Matsuki N (2001) Transient upregulation of the glial glutamate transporter GLAST in response to fibroblast growth factor, insulin-like growth factor and epidermal growth factor in cultured astrocytes. J Cell Sci 114(Pt 20):3717–3725
Genis L, Davila D, Fernandez S, Pozo-Rodrigalvarez A, Martinez-Murillo R, Torres-Aleman I (2014) Astrocytes require insulin-like growth factor I to protect neurons against oxidative injury. F1000Res 3:28. https://doi.org/10.12688/f1000research.3-28.v2
Ni W, Rajkumar K, Nagy JI, Murphy LJ (1997) Impaired brain development and reduced astrocyte response to injury in transgenic mice expressing IGF binding protein-1. Brain Res 769(1):97–107. https://doi.org/10.1016/s0006-8993(97)00676-8
Aberg ND, Brywe KG, Isgaard J (2006) Aspects of growth hormone and insulin-like growth factor-I related to neuroprotection, regeneration, and functional plasticity in the adult brain. ScientificWorldJournal 6:53–80. https://doi.org/10.1100/tsw.2006.22
Ratcliffe LE, Vazquez Villasenor I, Jennings L, Heath PR, Mortiboys H, Schwartzentruber A, Karyka E, Simpson JE et al (2018) Loss of IGF1R in human astrocytes alters complex I activity and support for neurons. Neuroscience 390:46–59. https://doi.org/10.1016/j.neuroscience.2018.07.029
Funa K, Sasahara M (2014) The roles of PDGF in development and during neurogenesis in the normal and diseased nervous system. J NeuroImmune Pharmacol 9(2):168–181. https://doi.org/10.1007/s11481-013-9479-z
Ballagi AE, Odin P, Othberg-Cederstrom A, Smits A, Duan WM, Lindvall O, Funa K (1994) Platelet-derived growth factor receptor expression after neural grafting in a rat model of Parkinson’s disease. Cell Transplant 3(6):453–460. https://doi.org/10.1177/096368979400300602
Iihara K, Hashimoto N, Tsukahara T, Sakata M, Yanamoto H, Taniguchi T (1997) Platelet-derived growth factor-BB, but not -AA, prevents delayed neuronal death after forebrain ischemia in rats. J Cereb Blood Flow Metab 17(10):1097–1106. https://doi.org/10.1097/00004647-199710000-00012
Funa K, Ahgren A (1997) Characterization of platelet-derived growth factor (PDGF) action on a mouse neuroblastoma cell line, NB41, by introduction of an antisense PDGF beta-receptor RNA. Cell Growth Differ 8(8):861–869
Zhang SX, Gozal D, Sachleben LR Jr, Rane M, Klein JB, Gozal E (2003) Hypoxia induces an autocrine-paracrine survival pathway via platelet-derived growth factor (PDGF)-B/PDGF-beta receptor/phosphatidylinositol 3-kinase/Akt signaling in RN46A neuronal cells. FASEB J 17(12):1709–1711. https://doi.org/10.1096/fj.02-1111fje
Lim R, Liu YX, Zaheer A (1990) Cell-surface expression of glia maturation factor beta in astrocytes. FASEB J 4(15):3360–3363. https://doi.org/10.1096/fasebj.4.15.2253851
Zaheer A, Mathur SN, Lim R (2002) Overexpression of glia maturation factor in astrocytes leads to immune activation of microglia through secretion of granulocyte-macrophage-colony stimulating factor. Biochem Biophys Res Commun 294(2):238–244. https://doi.org/10.1016/S0006-291X(02)00467-9
Kempuraj D, Khan MM, Thangavel R, Xiong Z, Yang E, Zaheer A (2013) Glia maturation factor induces interleukin-33 release from astrocytes: implications for neurodegenerative diseases. J NeuroImmune Pharmacol 8(3):643–650. https://doi.org/10.1007/s11481-013-9439-7
Krum JM, Khaibullina A (2003) Inhibition of endogenous VEGF impedes revascularization and astroglial proliferation: roles for VEGF in brain repair. Exp Neurol 181(2):241–257. https://doi.org/10.1016/s0014-4886(03)00039-6
Hetz C (2012) The unfolded protein response: controlling cell fate decisions under ER stress and beyond. Nat Rev Mol Cell Biol 13(2):89–102. https://doi.org/10.1038/nrm3270
Martin-Jimenez CA, Garcia-Vega A, Cabezas R, Aliev G, Echeverria V, Gonzalez J, Barreto GE (2017) Astrocytes and endoplasmic reticulum stress: a bridge between obesity and neurodegenerative diseases. Prog Neurobiol 158:45–68. https://doi.org/10.1016/j.pneurobio.2017.08.001
Thayanidhi N, Helm JR, Nycz DC, Bentley M, Liang Y, Hay JC (2010) Alpha-synuclein delays endoplasmic reticulum (ER)-to-Golgi transport in mammalian cells by antagonizing ER/Golgi SNAREs. Mol Biol Cell 21(11):1850–1863. https://doi.org/10.1091/mbc.E09-09-0801
Lai Y, Kim S, Varkey J, Lou X, Song JK, Diao J, Langen R, Shin YK (2014) Nonaggregated α-synuclein influences SNARE-dependent vesicle docking via membrane binding. Biochemistry 53(24):3889–3896. https://doi.org/10.1021/bi5002536
Colla E, Coune P, Liu Y, Pletnikova O, Troncoso JC, Iwatsubo T, Schneider BL, Lee MK (2012) Endoplasmic reticulum stress is important for the manifestations of α-synucleinopathy in vivo. J Neurosci 32(10):3306–3320. https://doi.org/10.1523/JNEUROSCI.5367-11.2012
Alberdi E, Wyssenbach A, Alberdi M, Sanchez-Gomez MV, Cavaliere F, Rodriguez JJ, Verkhratsky A, Matute C (2013) Ca2+-dependent endoplasmic reticulum stress correlates with astrogliosis in oligomeric amyloid β-treated astrocytes and in a model of Alzheimer’s disease. Aging Cell 12(2):292–302. https://doi.org/10.1111/acel.12054
Matsuzaki H, Daitoku H, Hatta M, Tanaka K, Fukamizu A (2003) Insulin-induced phosphorylation of FKHR (Foxo1) targets to proteasomal degradation. Proc Natl Acad Sci U S A 100(20):11285–11290. https://doi.org/10.1073/pnas.1934283100
Vlachostergios PJ, Papandreou CN (2013) The Bmi-1/NF-kappaB/VEGF story: another hint for proteasome involvement in glioma angiogenesis? J Cell Commun Signal 7(4):235–237. https://doi.org/10.1007/s12079-013-0198-2
Chang J, Yang B, Zhou Y, Yin C, Liu T, Qian H, Xing G, Wang S et al (2019) Acute methylmercury exposure and the hypoxia-inducible factor-1α signaling pathway under normoxic conditions in the rat brain and astrocytes in vitro. Environ Health Perspect 127(12):127006. https://doi.org/10.1289/EHP5139
Latina V, Caioli S, Zona C, Ciotti MT, Borreca A, Calissano P, Amadoro G (2018) NGF-dependent changes in ubiquitin homeostasis trigger early cholinergic degeneration in cellular and animal AD-model. Front Cell Neurosci 12:487. https://doi.org/10.3389/fncel.2018.00487
Du Y, Zhang X, Tao Q, Chen S, Le W (2013) Adeno-associated virus type 2 vector-mediated glial cell line-derived neurotrophic factor gene transfer induces neuroprotection and neuroregeneration in a ubiquitin-proteasome system impairment animal model of Parkinson’s disease. Neurodegener Dis 11(3):113–128. https://doi.org/10.1159/000334527
Nagano K, Bornhauser BC, Warnasuriya G, Entwistle A, Cramer R, Lindholm D, Naaby-Hansen S (2006) PDGF regulates the actin cytoskeleton through hnRNP-K-mediated activation of the ubiquitin E3-ligase MIR. EMBO J 25(9):1871–1882. https://doi.org/10.1038/sj.emboj.7601059
Papaevgeniou N, Chondrogianni N (2014) The ubiquitin proteasome system in Caenorhabditis elegans and its regulation. Redox Biol 2:333–347. https://doi.org/10.1016/j.redox.2014.01.007
Ebrahimi-Fakhari D, Cantuti-Castelvetri I, Fan Z, Rockenstein E, Masliah E, Hyman BT, McLean PJ, Unni VK (2011) Distinct roles in vivo for the ubiquitin-proteasome system and the autophagy-lysosomal pathway in the degradation of alpha-synuclein. J Neurosci 31(41):14508–14520. https://doi.org/10.1523/JNEUROSCI.1560-11.2011
Funding
The study is supported by the Scientific and Technological Research Council of Turkey-TUBITAK (Project No. 216S887) and by Research Fund of Istanbul University-Cerrahpasa (Project No: YKL-23616). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualisation: BS, DGA; data curation: BS; formal analysis: BS, ED, DGA; funding acquisition: DGA; investigation: BS, DGA; methodology: BS, ED, DGA; project administration: ED, DGA; resources: ED, DGA; supervision: AV, DGA; writing–original draft preparation: BS, ED, AV, DGA; writing–review and editing: AV, ED, DGA. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interests
Ethics Approval
Not applicable
Consent to Participate
Not applicable
Consent for Publication
Not applicable
Code Availability
Not applicable
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Supplementary figure 1:
Growth factor expression profile of human astrocytes. The 95% CI values of intracellular or secreted GF/GF receptors levels in untreated human astrocytes were set as upper or lower threshold values for GF production. For the calculation of 95% CI, mean levels of GFs at 48 hours and 72 hours were used (DOCX 14 kb)
Supplementary figure 2:
Growth factor expression profile of mock or α-synuclein overexpressing human astrocytes. The 95% CI values of intracellular or secreted GF/GF receptors levels in each group were set as upper or lower threshold values for GF detection. For the calculation of 95% CI, mean levels of GFs at 48 hours (the most significant time point). (DOCX 18 kb)
Supplementary table 1:
Reactome analysis results. Secreted or intracellular levels of 33 GFs and 8 GF receptors in control or α-synuclein overexpressing human astrocytes were used for analysis. Only the pathway results of secreted proteins in untreated human astrocytes were given. (https://reactome.org/PathwayBrowser/#/ANALYSIS=MjAyMDAyMjcwOTQyMzNfMzQyMzU%3D) (DOCX 142 kb)
Rights and permissions
About this article

Cite this article
Şengül, B., Dursun, E., Verkhratsky, A. et al. Overexpression of α-Synuclein Reorganises Growth Factor Profile of Human Astrocytes. Mol Neurobiol 58, 184–203 (2021). https://doi.org/10.1007/s12035-020-02114-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-020-02114-x