
Abstract
Background
Acute metabolic crises in inborn errors of metabolism (such as urea cycle disorders, organic acidemia, maple syrup urine disease, and mitochondrial disorders) are neurological emergencies requiring management in the pediatric intensive care unit (PICU). There is a paucity of data pertaining to electroencephalograms (EEG) characteristics in this cohort. We hypothesized that the incidence of background abnormalities and seizures in this cohort would be high. Neuromonitoring data from our center’s PICU over 10 years are presented in this article.
Methods
Data were collected by retrospective chart review for patients with the aforementioned disorders who were admitted to the PICU at our institution because of metabolic/neurologic symptoms from 2008 to 2018. Descriptive statistics (χ2 test or Fisher’s exact test) were used to study the association between EEG parameters and outcomes.
Results
Our cohort included 40 unique patients (8 with urea cycle disorder, 7 with organic acidemia, 3 with maple syrup urine disease, and 22 with mitochondrial disease) with 153 admissions. Presenting symptoms included altered mentation (36%), seizures (41%), focal weakness (5%), and emesis (28%). Continuous EEG was ordered in 34% (n = 52) of admissions. Twenty-three admissions were complicated by seizures, including eight manifesting as status epilepticus (seven nonconvulsive and one convulsive). Asymmetry and focal slowing on EEG were associated with seizures. Moderate background slowing or worse was noted in 75% of EEGs. Among those patients monitored on EEG, 4 (8%) died, 3 (6%) experienced a worsening of their Pediatric Cerebral Performance Category (PCPC) score as compared to admission, and 44 (86%) had no change (or improvement) in their PCPC score during admission.
Conclusions
This study shows a high incidence of clinical and subclinical seizures during metabolic crisis in patients with inborn errors of metabolism. EEG background features were associated with risk of seizures as well as discharge outcomes. This is the largest study to date to investigate EEG features and risk of seizures in patients with neurometabolic disorders admitted to the PICU. These data may be used to inform neuromonitoring protocols to improve mortality and morbidity in inborn errors of metabolism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
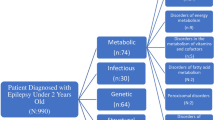
Metabolic decompensation in inborn errors of metabolism (IEMs) is a life-threatening emergency that frequently results in admission to the pediatric intensive care unit (PICU). Most patients recurrently admitted to the PICU with an IEM have a proximal urea cycle disorder (UCD), an organic acidemia (OA), maple syrup urine disease (MSUD), or a mitochondrial disease (MD), including mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) [1, 2]. The mechanism of brain injury in each disorder is distinct, reflecting differences in biochemical pathways [3]. UCD is a rare group of disorders caused by a genetic defect in one of the six enzymes or two carrier molecules involved in removal of nitrogen in the liver. As a result, there is accumulation of ammonia, which leads to astrocyte swelling, dysregulation of glutaminergic neurotransmission, and secondary mitochondrial dysfunction [4, 5]. OAs are a heterogenous group of disorders characterized by accumulation of toxic organic acid moieties in the plasma. For example, methylmalonic acidemia and propionic acidemia are inborn errors of the propionate pathway characterized by accumulation of methylmalonic acid and propionic acid, respectively, which can lead to metabolic brain injury in the deep nuclei and cortex. There can be hyperammonemia (HA) and lactic acidosis due to secondary inhibition of urea cycle enzymes and the pyruvate dehydrogenase complex, respectively, which become additional contributors to brain injury [6,7,8,9]. MSUD is caused by a genetic defect of the enzyme complex branched chain amino acid (BCAA) dehydrogenase, leading to elevated levels of leucine (and other BCAAs), which results in malignant cerebral edema. Pathogenesis is complicated by depletion of neurotransmitters, such as dopamine, γ-aminobutyric acid, and glutamate, and dysregulation of vasopressin. The cerebral edema can be difficult to treat because renal excretion of BCAA leads to obligate sodium loss [10,11,12,13]. MDs are a heterogenous group of conditions that can present with neurologic or nonneurologic symptoms at any age. In MELAS and related conditions, genetic defect in mitochondrial (or nuclear) DNA leads to impaired production of the subunits of the electron transport chain. This in turn leads to defective oxidative phosphorylation in cerebral vessels, culminating in lactic acidosis and stroke-like episodes. The area of cortical injury often involves the parieto-occipital lobes or subcortical nuclei and does not conform to a vascular territory. The role of nitric oxide deficiency is well established and becomes the rationale for treatment with arginine [14,15,16] (Fig. 1).

Simplified diagram showing mechanisms of brain injury in urea cycle disorder (UCD), organic acidemia (OA), maple syrup urine disease (MSUD), and mitochondrial disease (MD). ICP intracranial pressure, MMA methylmalonic acidemia, NMDAR N-methyl-D-aspartate receptor, NO nitric oxide, PA propionic acidemia
Because of the high incidence of acute seizures in these disorders, we hypothesized that continuous electroencephalogram (cEEG) monitoring could lead to changes in acute care. cEEG monitoring has been used as a neuromonitoring tool in the PICU to guide management and provide prognostic information for a diverse group of neurologic disorders, including traumatic brain injury, stroke, cardiac arrest, and congenital cardiac defects [17,18,19,20]. EEG has not been studied systematically in IEMs, and therefore there is a lack of data regarding its usefulness in these disorders [21]. We present our data over 10 years from a single center studying EEG characteristics in our cohort.
Methods
Data Collection
Data was collected by retrospective chart review for patients with proximal UCD, OA, MSUD, and MD who were admitted to the PICU at our institution because of metabolic or neurologic symptoms from 2008 to 2018. The study was approved by the Institutional Review Board of Children’s National Hospital (Pro0001495). Consent was not required. Study data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Children’s National. REDCap is a secure Web-based application designed to support data capture for research studies [22]. Inclusion criteria included a confirmed diagnoses of UCD, MD, OA, or MSUD and admission to the PICU because of metabolic failure or neurologic symptoms. Patients with a suspected but not confirmed metabolic disorder were excluded.
At our institution, cEEG is used in accordance with the American Clinical Neurophysiology Society consensus statement on cEEG in pediatric and adult patients [23]. Patients on cEEG are monitored for a minimum of 24 h, with prolonged recordings for patients with seizures or other high-risk EEG background features [23]. EEGs are recorded using the modified 10–20 system of electrode placement and interpreted by board-certified pediatric epileptologists and neurophysiologists in accordance with American Clinical Neurophysiology Society standardized critical care EEG terminology [24]. EEG features were extracted from reports in the electronic medical record. EEG features analyzed were as follows: best and worst background during the first 24 h of cEEG, state change, reactivity, symmetry, voltage, focal slowing, sleep spindles, sporadic epileptiform discharges, rhythmic and periodic patterns, seizures, and status epilepticus. The background was categorized as follows: mild slowing (slowing of posterior dominant rhythm, intermittent background slowing), moderate slowing (loss of posterior dominant rhythm), severe slowing (predominantly 1- to 2-Hz delta activity), discontinuous, burst attenuated and/or suppressed. We used this scale to further refine the category of slow/disorganized included in many pediatric critical care EEG studies [25]. Electrographic seizures were defined as follows: abnormal, paroxysmal EEG events that were distinctly different from the background activity; longer than 10 s duration or shorter if associated with a clinical event; and episodes that had a plausible electric field with evolution in morphology and spatial distribution. Electrographic seizures included electrographic (or EEG-only seizures) as well as electroclinical seizures.
Neuroimaging data were extracted from the electronic medical record based on interpretation by board-certified neuroradiologists. Pediatric Overall Cerebral Performance Category and Pediatric Cerebral Performance Category (PCPC) were scored by KS, NP, and a research assistant based on retrospective review of patient charts.
Statistical Analysis
Cohort characteristics and clinical outcomes were summarized with percentages for categorical variables and means for numerical variables. PCPC outcome data were categorized into no change in PCPC score, increase in PCPC score, and in-hospital mortality. Seizure data were categorized into no seizures and seizures groups. We compared the associations between the EEG parameters and the clinical outcomes (PCPC and seizure) using the χ2 test or Fisher’s exact test; the corresponding p values were reported. Data were analyzed using SAS for Windows version 9.4 (SAS Institute Inc., Cary, NC). A two-sided test with a significance level of 0.05 was used throughout all the hypothesis tests.
Results
General Cohort Characteristics
Our cohort included 40 unique patients (8 with UCD, 7 with OA, 3 with MSUD, and 22 with MD) with a total of 153 PICU admissions (Table 1). Presenting symptoms included altered mental status (n = 55, 36%), seizures (n = 62, 41%), focal weakness (n = 8, 5%), and emesis (n = 41, 28%). Biochemical aberrations during admission included lactic acidosis (55%), HA (37%), and elevated leucine levels (6%). Seventy-two percent of patients had a diagnosis of epilepsy before PICU admission, and 63% of patients with epilepsy were on more than three antiseizure medications. Thirty-seven percent of patients had had a stroke-like episode at any point of time before PICU admission. Neuroimaging (magnetic resonance imaging [MRI]) was performed during 25% of admissions, revealing edema (2.4%), cortical and basal ganglia injury (20% and 2.4%, respectively), and encephalomalacia (49%). Management in the PICU followed standardized treatment recommendations for the specific disorders, including intravenous arginine for MELAS, ammonia scavenger medications and hemodialysis in HA in OA and UCD, and appropriate dietary and fluid management. The mean length of stay in the PICU was 5.11 days, and 4% of patients had in-house mortality. Only 8% of admissions had iatrogenic complications, most commonly hyperglycemia or hypotension. Mean Pediatric Overall Cerebral Performance Category and PCPC scores at discharge were 3.32 and 3.39, respectively.
EEG Background and Seizure Characteristics
EEG data were available for 52 (34%) admissions. Indications for ordering EEG were clinical paroxysmal events suspected to be seizures (n = 20, 38%), persistently altered mental status following status epilepticus (n = 11, 21%), acute supratentorial brain injury with altered mental status (n = 8, 15%), unexplained alteration of mental status without known brain injury (n = 7, 13%), intracranial pressure (ICP) monitoring (n = 2, 4%), and other indications (n = 13, 25%). Minimum duration of EEG was 2.6 h and maximum duration was 533.5 h with a median of 22.1 h (interquartile range [IQR] 13.8–56 h). For a detailed characterization of EEG findings for the cohort as a whole and for each type of disorder, see Table 2. Most EEGs showed an abnormal background, most commonly mild or moderate slowing. There appears to have been a change in the EEG background severity during at least a subset of admissions given that the distribution of background abnormalities for the worst background recorded differed from that for the best background recorded. Background asymmetry and focal slowing was associated with a higher incidence of seizures and these results were statistically significant (p = 0.01 and 0.03, respectively; Table 3). Background findings led to changes in care in several situations. For example, a 27-year-old female patient with MELAS and a history of multiple stroke-like episodes, refractory epilepsy, and intellectual disability presented with emesis and breakthrough seizures in the setting of viral infection. Urgent brain MRI could not be performed overnight, but cEEG showed left occipital sharp waves and generalized slowing. Based on clinical presentation, lactic acidosis, and EEG findings, a stroke-like episode was suspected, and intravenous arginine therapy was initiated. Brian MRI performed the next morning confirmed new diffusion-weighted imaging (DWI) changes in the left occipital lobe, and therapy was continued.
More than half of the EEGs showed sporadic epileptiform discharges, and almost half had a rhythmic or periodic pattern and/or seizures. Twenty-three admissions during which EEG monitoring was performed were complicated by seizures, including eight (35%) manifesting as status epilepticus (seven nonconvulsive and one convulsive). Ten such admissions (43%) were complicated by both clinical and subclinical seizures, and 22 (96%) were complicated by subclinical seizures and/or nonconvulsive status epilepticus. One admission that did not include EEG monitoring was complicated by clinical seizures. Seizures were < 5 min in duration (n = 21, 91%) and focal (n = 14, 61%) in most patients who had seizures. The number of seizures per patient ranged from 1 to 201, with a median of 13.5 (IQR 5.3–77.5), and seizure minutes in the worst hour ranged from 1 to 60 min, with a median of 5 (IQR 3–14.5) minutes. Of note, both asymmetry (p = 0.01) and focal slowing (p = 0.03) on EEG were associated with the presence of seizures. No other background EEG features were associated with seizures. New seizure medications were started in 18 (78%) patients who underwent EEG monitoring and had seizures. The most frequently used medications were phenytoin in 11 (21%) patients and phenobarbital in 9 (17%) patients monitored on EEG. Midazolam infusion was required in 21% of these admissions per the status epilepticus protocol in our PICU, suggesting the refractory nature of seizures during acute metabolic crisis in a subset of these patients. Statistical comparison of seizure and EEG characteristics across the four groups of disorders was not feasible because of the small number of patients with OA, UCD, and MSUD monitored on EEGs who also had seizures.
EEG Features Associated with Outcome
Patient outcomes were assessed at discharge. Among those patients monitored on EEG with a known outcome at discharge (n = 51), 4 (8%) died, 3 (6%) experienced a worsening of their PCPC score as compared to admission, and 44 (86%) had no change (or improvement) in their PCPC score during admission. EEG features associated with outcome included the best background category (p = 0.01), reactivity (p = 0.03), and amplitude (p = 0.04) (Table 4). No other EEG background feature, including rhythmic and periodic patterns or seizures, was significantly associated with outcome. The association results are made based on univariate analysis; because of the limitation of sample size, no covariates/cofounders are included.
Discussion
The study shows a high incidence of seizures, especially subclinical seizures, in intoxication type and energy deficiency IEMs. Asymmetry and focal slowing of the EEG background were associated with an increased risk for seizures. In addition to subclinical seizures, our neuromonitoring data also revealed a high incidence of encephalopathy during metabolic crisis as characterized by background slowing, lack of state change, and lack of reactivity. EEG features associated with outcome included the best background category during the first 24 h of recording, reactivity, and voltage.
Almost half of the admissions for acute metabolic crisis in our cohort were characterized by seizures, and a significant subset showed subclinical seizures. Twenty-three admissions were complicated by seizures, including eight manifesting as status epilepticus (seven nonconvulsive and one convulsive). Ten admissions were complicated by both clinical and subclinical seizures, 22 were complicated by subclinical seizures and/or nonconvulsive status epilepticus, and one was complicated by clinical seizures not captured on EEG. Our data also suggest that asymmetry (p = 0.01) and focal slowing (p = 0.03) of the EEG background are associated with seizures. Close attention to asymmetry and focal slowing may help identify patients who are at increased risk for seizures. Asymmetry and focal slowing in patients with IEMs may predict metabolic brain injury and should prompt consideration for neuroimaging. As demonstrated in the case of the patient with MELAS who presented with breakthrough seizures, EEG background and focal sharp waves led to changes in inpatient management by initiation of appropriate therapy, and ischemic injury was identified on MRI subsequently. It is of utmost importance to identify patients who are at increased risk of seizures because seizures lead to a vicious cycle of increased cerebral metabolism, oxidative stress, and further mitochondrial dysfunction [26,27,28]. For example, HA is associated with status epilepticus, coma, respiratory failure, and death [29]. Verma et al. reported that EEG abnormalities can be seen in HA and that subclinical seizures are common during acute metabolic crisis [30]. In an ornithine transcarbamylase (OTC) murine model, the etiology of seizures was attributed to desynchronized Ca2+ signaling and impaired K+ buffering [31]. The higher incidence of focal seizures in patients with MELAS and other MDs is not unexpected given the injury caused by stroke-like episodes is often focal, leading to cortical irritability. Seizures in a patient with MELAS should be considered a sign of a potential stroke-like episode and not as a breakthrough seizure even if they have a known history of epilepsy [15, 16]. The incidence of acute provoked seizures and development of long-term epilepsy in OA have not been studied systematically. In a cohort reported by Jiang et al. [32], seizures were reported in 14.64% and 14.50% of hospitalized patients with methylmalonic acidemia and propionic acidemia, respectively.
The most common indications for ordering EEG were paroxysmal events concerning for seizures or altered mental status following prolonged seizures. Moderate slowing or worse was noted in 75% of EEGs. Change in EEG background and increase in interburst intervals can predict worsening in metabolic failure, such as HA and lactic acidosis [33]. Previous studies have shown that the EEG background in UCD and OA complicated by HA comprises low voltage slow waves with asymmetric delta and theta waves and may reveal burst suppression [5]. A case series from our center describing eight neonates with HA demonstrated that all patients lacked state changes on EEG, and there was correlation between interburst interval duration and degree of HA [34].
Consideration can also be given to using EEG as a noninvasive means of monitoring for increased ICP secondary to cerebral edema from HA, hyperleucinemia, or other metabolic brain injury when more invasive modalities are not an option. In our cohort, ICP monitoring was noted to be the reason for ordering an EEG in a small subset of patients (4%). For example, acute suppression ratio on quantitative EEG can be used to predict and monitor raised ICP. Sansevere et al. [35] published a retrospective review of 13 patients with clinical or neuroimaging signs of raised ICP who were monitored on cEEG. They noted a median time of 3.12 h from an increase in the suppression ratio on quantitative EEG to signs of raised ICP on examination or neuroimaging. Based on these findings, quantitative EEG may be a useful tool for management of acute crises in IEMs. The disorders included in that publication included epileptic encephalopathy and cardiac arrest, and therefore whether these results are applicable to patients with IEMs remains to be determined.
We also identified EEG features associated with outcome in our population. The best background category, reactivity, and voltage were associated with a PCPC score at discharge that was the same as or improved compared to the baseline PCPC score. A normal or mildly abnormal background, the presence of reactivity, and a normal voltage background are all more likely to be seen in patients without new brain injury. This is keeping with prior studies that have examined the association of EEG background features with outcome after pediatric cardiac arrest [17] and traumatic brain injury [18]. EEG background features may be used to screen for new metabolic injury and/or to identify patients at high risk of metabolic injury for targeted neuroprotective and other therapeutic measures.
There are several limitations to this study. First, this was a single-center retrospective study with a relatively small number of patients. Therefore, a comparison of seizure and EEG characteristics across the four groups of disorders was not statistically feasible. Furthermore, the χ2 test or Fisher’s exact test was used to test for the associations between EEG features and clinical outcomes. However, our conclusion is made based on the univariate analysis without adjusting any covariates because of the small sample size. In addition, many patients were intubated and sedated, which could have played a confounding role on the EEG background. Moreover, there were multiple EEG readers, and our analysis relied on EEG reports rather than rereview of the recordings.
We aim to use the data from this article to form a formal neuromonitoring protocol for acute crisis in IEMs [21]. The results of our study suggest that EEG should be considered when these patients are being managed for acute metabolic crisis, regardless of occurrence of clinical seizures because identification of subclinical seizures as well as background abnormalities can lead to changes in care. However, risk/benefit analysis and a thorough review of clinical data are indispensable because cEEG monitoring may not be easily available at some centers that are not tertiary care children’s hospitals. At most centers, medical geneticists take the lead in management of acute metabolic crisis in patients with IEMs. Our study reiterates that early consultation with a pediatric neurology team and collaborative care models can lead to improvement in neuromonitoring, which may contribute to better outcomes. Further studies are required to understand the importance of neuromonitoring in IEMs and to meaningfully improve the survival and long-term outcomes. Understanding the biochemical basis of brain injury in these IEMs will help in establishing tailor-made neuromonitoring protocols and improving the outcomes in this patient population. For instance, seizures were noted to be extremely common during stroke-like episodes in MELAS; therefore, consideration should be given to monitoring these patients on cEEG throughout their management. On the other hand, seizures are not very common during metabolic crisis in MSUD, but EEG may be invaluable in monitoring ICP using the acute suppression ratio or other similar measures.
Conclusions
We report the largest study to date investigating seizure characteristics and EEG attributes of patients with neurometabolic disorders admitted to the PICU. This study identified a high prevalence of seizures, especially subclinical seizures, for patients presenting with metabolic decompensation. Three quarters of EEGs showed moderate slowing or worse, and asymmetry and focal slowing were both associated with seizures. There are currently no standardized guidelines for neuromonitoring in IEMs. These data can serve to establish standardized protocols to improve the recognition, stabilization, and recovery of patients with IEMs. This study also emphasizes the importance of collaborative clinical care between intensivists, pediatric neurologists, and biochemical geneticists for this patient population. Lastly, we advocate for a multicenter registry for patients with IEMs where features of EEG and other advanced neuromonitoring techniques can be researched and studied systematically.
References
Ferreira CR, van Karnebeek CD. Inborn errors of metabolism. Handb Clin Neurol. 2019;162:449–81.
Saudubray JM, Garcia-Cazorla À. Inborn errors of metabolism overview: pathophysiology, manifestations, evaluation, and management. Pediatr Clin N Am. 2018;65(2):179–208.
Gropman AL. Patterns of brain injury in inborn errors of metabolism. Semin Pediatr Neurol. 2012;19(4):203–10.
Ah Mew N, Simpson KL, Gropman AL, Lanpher BC, Chapman KA, Summar ML, et al. Urea cycle disorders overview. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, et al., editors. GeneReviews. Seattle: University of Washington; 2003.
Sen K, Whitehead M, Castillo Pinto C, Caldovic L, Gropman A. Fifteen years of urea cycle disorders brain research: looking back, looking forward. Anal Biochem. 2022;636:114343.
Häberle J, Chakrapani A, Ah Mew N, Longo N. Hyperammonaemia in classic organic acidaemias: a review of the literature and two case histories. Orphanet J Rare Dis. 2018;13(1):219.
Jafari P, Braissant O, Zavadakova P, Henry H, Bonafé L, Ballhausen D. Brain damage in methylmalonic aciduria: 2-methylcitrate induces cerebral ammonium accumulation and apoptosis in 3D organotypic brain cell cultures. Orphanet J Rare Dis. 2013;8(1):4.
Wajner M, Coelho JC. Neurological dysfunction in methylmalonic acidaemia is probably related to the inhibitory effect of methylmalonate on brain energy production. J Inherit Metab Dis. 1997;20(6):761–8.
Sen K, Burrage LC, Chapman KA, Ginevic I, Mazariegos GV, Graham BH; ACMG Therapeutics Committee. Solid organ transplantation in methylmalonic acidemia and propionic acidemia: a points to consider statement of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2023;25(2):100337.
Sen K, Gropman A, Harrar D. In-hospital mortality from cerebral edema in MSUD during newborn screening era: What are we missing and what more can we do? Pediatr Neurol. 2022;135:61–2.
Zinnanti WJ, Lazovic J. Interrupting the mechanisms of brain injury in a model of maple syrup urine disease encephalopathy. J Inherit Metab Dis. 2012;35(1):71–9.
Amaral AU, Wajner M. Pathophysiology of maple syrup urine disease: focus on the neurotoxic role of the accumulated branched-chain amino acids and branched-chain α-keto acids. Neurochem Int. 2022;157:105360.
Strauss KA, Carson VJ, Soltys K, Young ME, Bowser LE, Puffenberger EG, et al. Branched-chain α-ketoacid dehydrogenase deficiency (maple syrup urine disease): treatment, biomarkers, and outcomes. Mol Genet Metab. 2020;129(3):193–206.
Gropman AL. Neuroimaging in mitochondrial disorders. Neurotherapeutics. 2013;10(2):273–85.
Set KK, Sen K, Huq AH, Agarwal R. Mitochondrial disorders of the nervous system: a review. Clin Pediatr (Phila). 2019;58(4):381–94.
Gropman AL. The neurological presentations of childhood and adult mitochondrial disease: established syndromes and phenotypic variations. Mitochondrion. 2004;4(5–6):503–20.
Bach AM, Kirschen MP, Fung FW, Abend NS, Ampah S, Mondal A, et al. Association of EEG background with diffusion-weighted magnetic resonance neuroimaging and short-term outcomes after pediatric cardiac arrest. Neurology. 2024;102(5):e209134.
Xie J, Burrows BT, Fox Kensicki J, Adelson PD, Appavu B. early electroencephalographic features predicting cerebral physiology and functional outcomes after pediatric traumatic brain injury. Neurocrit Care. 2023;38(3):657–66.
Harrar DB, Sun LR, Segal JB, Lee S, Sansevere AJ. Neuromonitoring in children with cerebrovascular disorders. Neurocrit Care. 2023;38(2):486–503.
Massey SL, Weinerman B, Naim MY. Perioperative neuromonitoring in children with congenital heart disease. Neurocrit Care. 2024;40(1):116–29.
Castillo-Pinto C, Sen K, Gropman A. Neuromonitoring in rare disorders of metabolism. Yale J Biol Med. 2021;94(4):645–55.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Herman ST, Abend NS, Bleck TP, Chapman KE, Drislane FW, Emerson RG, et al.; Critical Care Continuous EEG Task Force of the American Clinical Neurophysiology Society. Consensus statement on continuous EEG in critically ill adults and children, part I: indications. J Clin Neurophysiol. 2015;32(2):87–95.
Hirsch LJ, Fong MW, Leitinger M, LaRoche SM, Beniczky S, Abend NS, et al. American Clinical Neurophysiology Society’s standardized critical care EEG terminology: 2021 version. J Clin Neurophysiol. 2021;38(1):1–29.
Abend NS, Gutierrez-Colina A, Zhao H, Guo R, Marsh E, Clancy RR, et al. Interobserver reproducibility of electroencephalogram interpretation in critically ill children. J Clin Neurophysiol. 2011;28(1):15–9.
Posner JB, Plum F, Van Poznak A. Cerebral metabolism during electrically induced seizures in man. Arch Neurol. 1969;20(4):388–95.
Ingvar M. Cerebral blood flow and metabolic rate during seizures. Relationship to epileptic brain damage. Ann N Y Acad Sci. 1986;462(1):194–206.
Patel M. Mitochondrial dysfunction and oxidative stress: cause and consequence of epileptic seizures. Free Radic Biol Med. 2004;37(12):1951–62.
Sen K, Anderson AA, Whitehead MT, Gropman AL. Review of multi-modal imaging in urea cycle disorders: the old, the new, the borrowed, and the blue. Front Neurol. 2021;12:632307.
Verma NP, Hart ZH, Kooi KA. Electroencephalographic findings in urea-cycle disorders. Electroencephalogr Clin Neurophysiol. 1984;57(2):105–12.
Qureshi IA, Rao KV. Sparse-fur (spf) mouse as a model of hyperammonemia: alterations in the neurotransmitter systems. Adv Exp Med Biol. 1997;420:143–58.
Jiang YZ, Shi Y, Shi Y, Gan LX, Kong YY, Zhu ZJ, et al. Methylmalonic and propionic acidemia among hospitalized pediatric patients: a nationwide report. Orphanet J Rare Dis. 2019;14(1):292.
McGowan M, Ferreira C, Whitehead M, Basu SK, Chang T, Gropman A. The application of neurodiagnostic studies to inform the acute management of a newborn presenting with sarbamoyl shosphate synthetase 1 deficiency. Child Neurol Open. 2021;8:2329048X20985179.
Wiwattanadittakul N, Prust M, Gaillard WD, Massaro A, Vezina G, Tsuchida TN, et al. The utility of EEG monitoring in neonates with hyperammonemia due to inborn errors of metabolism. Mol Genet Metab. 2018;125(3):235–40.
Sansevere AJ, DiBacco ML, Pearl PL, Rotenberg A. Quantitative electroencephalography for early detection of elevated intracranial pressure in critically ill children: case series and proposed protocol. J Child Neurol. 2022;37(1):5–11.
Acknowledgements
The authors would like to thank Grace Johnson, neurogenetics research assistant, for assistance with data collection.
Funding
This study was funded by Children’s National Board of Visitors/Founders Auxiliary Board Grant (FY 2021 CHB Award 9 6005920) awarded to KS and the O’Malley Family Foundation Grant awarded to AG.
Author information
Authors and Affiliations
Contributions
Dr. Sen is the Co-Director of Neurogenetics Clinic at Children’s National Hospital and conceptualized the project and wrote the initial manuscript. Drs. Gropman and Harrar were the senior authors who contributed to the discussion and review of literature. Dr. Pariseau, Ms. Keenan, and Ms. Tucker completed data collection and constructed figures. Dr. Zhang was the biostatistician and did statistical analyses on the data.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts of interest.
Ethical Approval/Informed Consent
The study was approved by the Institutional Review Board of Children’s National Hospital (Pro0001495). Consent was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sen, K., Harrar, D., Pariseau, N. et al. Seizure Characteristics and EEG Features in Intoxication Type and Energy Deficiency Neurometabolic Disorders in the Pediatric Intensive Care Unit: Single-Center Experience Over 10 Years. Neurocrit Care (2024). https://doi.org/10.1007/s12028-024-02073-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12028-024-02073-4