
Abstract
Fine needle aspiration cytology (FNAC) plays an essential role in the evaluation of thyroid nodules especially for the category of follicular neoplasms (FN) representing 25 % of all thyroid cases including different neoplastic entities. Hence, one of the most promising areas is the application of molecular tests to FNAC. Among them, microRNAs (miRNA),identified as negative (post-transcriptional) gene expression regulators involved in tumor development, are likely to discriminate among FNs. Limited data explored the use of miRNAs on FNAC as well as their role in the malignant risk stratification. We aimed to define whether liquid-based cytology (LBC) is a valid method for miRNA evaluation. From June 2014 to March 2015, we enrolled 27FNs with histological follow-up. In the same reference period, 13 benign nodules (BN) and 20 positive for malignancy (PM) were selected as controls. Histologically, FNs resulted in 14 malignancies (3 papillary thyroid carcinoma-PTC and 11 follicular variant of PTC-FVPC) and 13 follicular adenomas (FA). The 20 PMs included two FVPC, 16 PTC and two medullary thyroid carcinoma (MTC). Five miRNAs (10b, 92a, 221/222 cluster, and 375) were studied on LBC and quantified by real-time PCR. Only miR-375 was over-expressed in the FNs diagnosed as carcinomas and in the PMs. A cut-off of 12 miR-375/U6 relative ratio recognized all BNs and 95 % PMs. Specifically, in each category, FVPCs and PTCs did not show any difference while MTCs had the highest value. miR-375 shows 97.1 % sensitivity, 100 % specificity, 96.3 % negative predictive value (NPV), 100 % positive predictive value (PPV), and 98.3 % diagnostic accuracy. LBC is suitable for miRNAs evaluation. miR-375 resulted over-expressed in all malignant FNs and 95 % PMs. It may represent a valid aid in ruling out BNs and supporting PTCs and/or FVPCs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fine needle aspiration cytology (FNAC) is the first “gold standard approach” in the evaluation and diagnosis of thyroid nodules [1–4]. Numerous studies reported that more than 70 % of the thyroid FNACs are benign, 5–10 % are “malignant,” and the remaining 20–25 % of them represent the so-called “grey zone” of follicular neoplasms (FN) in which different neoplastic entities are included [5–10]. However, FN category encompasses also some cases in which an objective and consistent morphological diagnosis is not always straightforward [1–10]. In fact, deciding on both the FN nature and the consequent management (clinical and/or surgical) remains a vexing issue in several cases. In this regard, the recognized evidence that upward of 75 % of the FNs are found to be histological benign do not warrant the useless risk, costs of surgery and thyroid hormone replacement therapy. The remaining 25 % includes also cases of follicular variant of papillary thyroid carcinoma (FVPC) in which the absence of the unequivocal nuclear features of PTC may fall short of a definitive cytological diagnosis of malignancy [11–15]. Notwithstanding, the increasing knowledge of the molecular mechanisms of cancer appears to have an extremely useful role also on FNAC samples and mainly in the field of FNs. Despite the evidence that immunocytochemistry-ICC and molecular techniques (mainly through the detection of specific somatic mutations, i.e., BRAF V600E and NRAS) are highly likely to contribute to the diagnosis, prognosis, and even prediction of thyroid tumor behavior, they did not supply 100 % of the achievements especially among FNs [6, 16–23]. In this regard, some authors encouraged the role of microRNAs (miRNAs) defined as small endogenous, non-coding RNAs that mainly act as negative (post-transcriptional) regulators of coding gene expression whose deregulation is frequently associated with different human cancers [24–34].
Hence, only recently few authors demonstrated that thyroid tumors, including a broad spectrum of histotypes with different degrees of malignancy, represent a valid model for assessing that miRNA deregulation may play a role in thyroid cancer [24–28, 34–43].
Proved that, the cytological analysis of miRNAs panel may warrant its use as a novel and promising tool in order to overcome the morphological issues mainly in the “grey zone” of FNs.
To date, few authors described their yields mostly including the cytological categories of benign and malignant lesions obtained from ex vivo thyroid aspiration during thyroidectomies [24–28, 40, 41]. On the other hand, only one paper highlighted the low sensitivity and specificity obtained with the detection of miRNAs carried out on conventional FN samples [41].
Herein we display, for the first time to date, a prospective series of 60 liquid-based cytology (LBC) cases with histological follow-up, including 27 FNs with the application of a miRNA panel. Our results appraised that LBC represents an adequate and promising cytological preparation for carrying out miRNA analysis and a helpful aid for the malignant risk stratification among FNs.
Materials and methods
Our series included all the 27 consecutive prospective FN samples with histological follow-up in the period between June 2014 and March 2015. In the same reference period, as control cases, we purposely chose to select a small prospective series of both 13 consecutive benign nodules (BNs) and 20 positive for malignancy (PMs) with histological follow-up. All the cases were recorded in the Division of Anatomic Pathology and Histology of the Catholic University, “Agostino Gemelli” Hospital of Rome (Italy). All FNAC were carried out under-sonographic guidance (US) mostly by surgeons and endocrinologists and processed with LBC, Thin Prep 5000™ method (Hologic Co., Marlborough, MA).
Our patients were studied with US during their thyroid check-up performed in the “Centre for Thyroid Diseases” of our hospital. The series included 24 male and 36 female patients with a median age of 27 years (range 19–73-year old, median age 44-year old) and size ranging from 0.5 to 5 cm (Table 1). All aspirations (usually two passes for each lesion) were performed with 25–27 G needles; no rapid on-site assessment of the adequacy of the material was done. All patients had been appropriately informed regarding the use of LBC method for processing their samples and a written informed consensus was signed. Our study followed the tenants of the Declaration of Helsinki and we received the institutional (Catholic University) ethical approval for the study.
The technical steps for liquid-based preparations have been clearly described in previous papers of our group [6, 22]. The resulting slide was fixed in 95 % methanol and stained with Papanicolaou, while the remaining material was stored in the Preservcyt™ solution to be possibly used for the preparation of additional slides for further investigations (including both immunocytochemistry-ICC and molecular analysis). The lower limit for the adequacy for each sample was established, according to the British RC Path classification, in six groups of thyroid follicular epithelial cells within the submitted slides, each of them with at least ten well-visualized epithelial cells [14].
The cytological cases were classified according to the New Italian Working Group SIAPEC-IAP classification [15]. The above mentioned categories are defined as follows: TIR1: inadequate and TIR1C: cystic-hemorrhagic lesions; TIR2: benign nodules-BN; TIR3A: FN (low-risk indeterminate lesions); TIR3B: FN (high-risk indeterminate lesions); TIR4: suspicious of malignancy-SM; TIR5: positive for malignant neoplasm-PM. The definition of FN included both TIR3A and TIR3B. For the reader’s convenience and with the exclusion of the definitions of TIR3A (increased cellularity with numerous microfollicular structures in a background of poor colloid amount) and TIR3B (characterized by high cellularity in a monotonous and repetitive microfollicular/trabecular arrangement, with scant or absent colloid), the remaining categories did not result in any change from the previous classification system [15]. We ruled out all the Hurthle cell nodules (belonging to the TIR3B category) as long as their morphological features can be easily recognized on FNAC samples. Furthermore, as recently published by Dettmer et al., Hurthle cell tumors show different miRNA expression patterns allowing to discriminate between Hurthle cell adenomas and carcinomas which was not the goal of the current project [44].
Although the cytological cases were classified according to the New Italian Working Group SIAPEC-IAP classification, the majority of categories overlapped with the diagnoses adopted by the Bethesda System for Reporting Thyroid Cytopathology [13]. Specifically the cytological diagnoses of BNs, SMs, and PMs share identical features in both systems while TIR3As correspond to AUS/FLUSs [atypia of undetermined significance (AUS)/follicular lesion of undetermined significance (FLUS)] and TIR3Bs to FN [13].
Our global cytological series included the following distribution of diagnoses during the reference period: 6.5 % TIR1 (non diagnostic plus cystic cases); 79 % TIR2; 4.3 % TIR3A; 6 % TIR3B; 1.7 % SM; and 2.5 % PM. All the cytological and histological samples were reviewed by two expert pathologists (EDR and GF), and those cases whose interpretation was equivocal were submitted to the diagnostic judgment of the other pathologists until a final agreement was achieved.
The molecular analysis was carried out on the material stored in the PreservCyt solution; so that they can be performed with even 2 ml remaining material eluted in 5 ml of PreservCyt solution. The percentage of disease specific cells for molecular analysis was at least 50 % in all LBC samples
In all the cases, the extraction of DNA for BRAF V600E mutation was carried out from liquid-based stored material according to our previous papers [22]. All the BN and FN cases were wild type for (wt) for BRAF V600E while only five PMs expressed BRAF mutation (diagnosed as five papillary thyroid carcinoma-PTC on histology)
Molecular analysis of miRNA
Total RNA was isolated with miRNeasy Mini Kit (Qiagen, Milan, Italy) from our LBC series following the manufacturer’s instructions. One hundred ng of total RNA was reverse transcribed to cDNA using Im-Prom™ Reverse Transcription System (Promega, Milan Italy) with 2 µl (1 μM) stem-loop RT primers for miR-375, miR-10b, miR-92a, miR-221, miR-222, and U6 snRNA.
U6 snRNA was used as an endogenous control. The mixture was incubated in a final volume of 20 µl at 75 °C for 5 min, 4 °C for 3 min, 25 °C for 5 min, 42 °C for 60 min and 70 °C for 15 min, and then held at 12 °C. After reverse transcription, real-time PCR was performed using KAPA SYBR FAST Universal qPCR Kit (KAPA BIOSYSTEMS, Milan, Italy) on CFX96 Real-Time System (Biorad, Milan, Italy), according to the user’s manual. Briefly, quantitative PCR of biological samples was done in 20 μl total volume with 2 μl RT products, 10 μl of 2× KAPA SYBR FAST Universal qPCR Kit, and 250 nM of each primer. All reactions were run in triplicate. The specificity of each PRC products was validated by melting curve analysis at the end of PCR cycles. Samples were excluded if the PCR melt curves suggested multiple products or triplicates were inconsistent.
miRNA expression was normalized to that of the U6 snRNA using the 2−ΔΔCt method. The primers used were LRT miR-375: 5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACTCACGC-3′; LRT-U6 snRNA: 5′-AAAATATGGAACGCTTCACGAATTTG-3′; LRT miR-10b: 5′-GTCGTATCCAGTGCGTGTCGTGGAGTCGGCAATTGCACTGGATACGACCACAAA-3′; LRT miR-92a: 5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACCAGGCC-3′; LRT miR-221: 5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACGAAACCC-3′; LRT miR-222: 5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACGAGACC-3′; miR-375 S 5′-CGTTTGTTCGTTCGGCTC-3′; miR-375 AS 5′-GTGCAGGGTCCGAGGT-3′; U6snRNA S 5′-CTCGCTTCGGCAGCACATATACT-3′; U6snRNA AS 5′-ACGCTTCACGAATTTGCGTGTC-3′; miR-10b S 5′-GGATACCCTGTAGAACCGAA-3′; miR-10b AS 5′-CAGTGCGTGTCGTGGAGT-3′; miR-92 S 5′-TATTGCACTTGTCCCGGCCTG-3′; miR-92 AS 5′-GTGCAGGGTCCGAGGT-3′; miR-221 S 5′-AGCTACATTGTCTGCTGG-3′; miR-221 AS 5′-GTATCCAGTGCAGGGTCC-3′; miR-222 S 5′-TACATCTGGCTACTGG-3′; miR-222 AS 5′-GTATCCAGTGCAGGGTCC-3′.
Statistical analysis
Statistical analysis was performed using GraphPad-Prism 5 software (Graph Pad Software, San Diego, CA) and MedCalc version 10.2.0.0 (MedCalc Software, Mariakerke, Belgium). Statistical comparison of continuous variables was performed by the Mann–Whitney U test or Paired t test, as appropriate. Comparison of categorical variables was performed by Chi-square statistic, using the Fisher’s exact test. p values less than 0.05 were considered as statistically significant.
Histology
All surgical specimens were fixed in 10 % buffered formaldehyde and embedded in paraffin; the five micron-thick microtomic sections were stained with hematoxylin-eosin. All the peri-thyroid adipose tissue was embedded and examined for lymph-nodes research. The diagnosis of PTC was based on both the detection of true papillary structures and the distinctive nuclear features, whereas the diagnosis of FVPC relied upon the detection of the nuclear features of PTC in multiple foci within the tumor including both diffuse and encapsulated variants [45]. The diagnosis of medullary thyroid carcinoma (MTC) was characterized by the predominance of neoplastic C-cells showing the classical features of MTC and supported by the positivity for Calcitonin and CEA and negativity for Thyroglobulin. All the cases were classified according to the seventh edition of the tumor-node-metastasis-based staging system recommended by the American Joint Commission on Cancer (AJCC) [45].
Results
The study project, first evaluating five miRNAs (10b, −92a; −221; −222; 375) in a series of 35 prospective thyroid FNACs (including 11 BN, 13 FN and 11 PM), was then expanded to 60 prospective thyroid FNACs including 27 FNs samples, 13 BNs, and 20 PMs with surgical follow-up in the reference period. As for our purpose, we analyzed the role of miRNAs in the FN category and in the two categories of BN and PMs (respectively, benign and malignant control) while we did not record any suspicious of malignancy (SM) case with histological follow-up in the study. The category of FNs, according to the New Italian Working Group SIAPEC-IAP classification, was sub-classified into nine TIR3A and 18 TIR3B (Table 1).
Table 1 shows the distribution of clinical features in our series. None of the 27 cytological diagnosis of FN resulted in the histological diagnosis of goiter, and we recognized 13 Follicular Adenomas (FA) and 14 malignancies (three classical variant of papillary thyroid cancer-PTC and 11 Follicular Variants of Papillary thyroid cancer-FVPC). The 11 FVPCs included eight encapsulated and three infiltrative FVPCs. Specifically, TIR3A category was characterized by eight FA and one encapsulated FVPC, whereas TIR3B by five FAs and 13 malignancies (seven encapsulated FVPC, three infiltrative FVPC and three PTC) (specifically detailed in Table 4). BNs resulted in 13 nodular goiters while the 20 PM were diagnosed as 16 PTC, two encapsulated FVPC and two MTC. All the clinical and pathologic features (age, gender, size) are summarized in Table 1. We did not find any statistical significant difference among the analyzed parameters.
The application of the entire panel of five miRNAs in the first 35 cases did not show any significant result except for miR-375 so that we studied and analyzed the additional thyroid FNACs (for a total of 60 cases) only for miR-375. Nevertheless, we found a slightly higher expression of miR-221 and miR-222 in the malignant cases which was not statistically significant (data not tabled).
The miRNAs evaluation was carried out in all the 27 prospective FNs, even if we have to report that five cases had been previously excluded because PCR melting curves suggested multiple products (four cases) or low amount of RNA (one case).
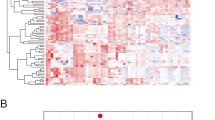
As highlighted in Fig. 1, the quantitative PCR analysis to assess the expression levels of miR-375 demonstrated an increasing and statistically significant up-regulation among the three categories (BN vs FN p = 0.0026; BN vs PM p < 0.0001 and FN vs PM p = 0.0023 respectively)

Comparison of miR-375 expression using quantitative PCR analysis in different cytological categories
Furthermore, taking all the data into account, we found that all our benign lesions and FN with benign histology were under the cut-off value of 12, determined utilizing the mean value of miR-375/U6 relative ratio in benign samples plus two standard deviation (SD). This threshold seemed to be the best value for the comparative evaluation among the cytological categories of BNs, FNs, and PMs with significantly higher value in cases with malignant outcome (including malignant FNs and PMs) than in BNs (p < 0.0001, OR 689, 95 % CI 26.6–17850, Table 2)
In fact, Table 2 highlights that this threshold recognized 100 % of benign cases and 95 % of malignant cases. Our data estimated that miR-375 had a significant over-expression in all FNs which resulted in a malignant outcome as well as in 95 % of the PMs compared with BNs. We reported a significant difference (p = 0.00011, OR 29, 95 % CI 1.565–537.2) between the category of BNs and FNs including both TIR3A and TIR3B accordingly to the new Italian classification system (Table 2). The same picture shows the significant p value between FN and PM categories (p = 0.00012, OR 0.057, 95 % CI 0.007–0.486) and also between BN and PM categories (p < 0.0001, OR 0.003, 95 % CI 0.0001–0.075).
In Table 3, we assess miR-375 mean expression among the different histological diagnoses showing its increasing expression from PTCs/FVPCs progressively up to MTCs. Moreover, when we compared encapsulated and infiltrative FVPCs, we did not appreciate any significant difference regardless of the cytological diagnoses.
When we evaluated miR-375 expression in the categories of TIR3A and TIR3B, classified according to the new Italian Classification System, we interestingly observed that the two subcategories showed a different and distinct miR-375 expression, clearly down, and up the cut-off value. As underscored in Table 4 and Fig. 2, miR-375 over-expression identified the two morphological subcategories of FNs and moreover it marked its correlation with a malignant outcome (p < 0.0001)

Comparison of miR-375 expression using quantitative PCR analysis in the category of Follicular Neoplasms (sub-classified according to the Italian Classification System) [15]
Concerning the correlation between BRAF and miR-375, none of our FNs with a malignant histology had BRAF V600E mutation also because 11 out of them resulted as FVPCs. These data are in agreement with literature inasmuch as FVPCs have a low prevalence of BRAF V600E mutation. Nonetheless, we reported five PTCs with BRAF V600 mutation (belonging to the group of our 20 PMs) and higher value of miR-375 expression. According to our results, the statistical analysis (data not tabled) for miR-375 confirmed 97.1 % sensitivity, 100 % specificity, 96.3 % negative predictive value (NPV), 100 % positive predictive value (PPV), and 98.3 % diagnostic accuracy.
Discussion
In this paper, we evaluated the reliability of analyzing a panel of five miRNAs on LBC thyroid lesions, mostly diagnosed on FNs, in order to establish whether it is possible to distinguish benign from malignant lesions providing a predictive molecular diagnosis on FNAC. In fact, despite the high diagnostic accuracy of morphology alone, several authors demonstrated that the identification of genetic mutations, frequently associated with malignancy, represents an additional valid aid especially in the “grey zone” of FNs which comprises 20–30 % of malignancies [1, 5, 6, 18, 23].
Similarly, it is not surprising that the introduction of ancillary techniques (namely ICC or DNA/RNA analysis) has been adopted over the last years on cytology in the attempt to recognize this latter malignant cohort which is frequently devoid of the unequivocal PTC nuclear features [5–10, 17, 18, 21–23].
In the field of thyroid oncology, BRAF mutation represents the most recent hallmark of thyroid carcinoma mainly harbored in 49–70 % of the PTCs; however, the majority of FNs do not harbor any somatic mutation including BRAF V600E or they do not express specific ICC markers without a concrete contribution to the correct diagnosis of a high percentage of FNs [6–12, 18, 22, 23]. As a result, the decision about the diagnosis and management of FNs remains a vexing question and a difficult challenge, which warrants the introduction of miRNA analysis on cytological material for improving some shortcomings of DNA methods as reported by Diggans [8].
In this perspective, thyroid lesions with their broad spectrum of neoplasms (from benign to malignant entities) pioneers the possibility of studying and identifying specific subsets of different up-and down-regulated miRNAs in each different entity [24–40]. Pallante et al. demonstrated the role of miRNAs in tumor cell transformation as well as the up-regulation of a specific miRNA panel in a cohort of 30 PTCs versus ten benign lesions on histological samples. In the same way, Dettmer et al. confirmed the correlation between miRNA levels and well-differentiated thyroid malignant histotypes without any significant discrimination between different malignant variants (specifically PTC and FVPC) [30, 43].
However, despite the unequivocal demonstration that aberrant expression of miRNAs is frequently recognized as a clue to thyroid cancers, few papers have applied the evaluation of miRNAs on thyroid FNAC. In detail, the majority of published case studies are based on conventional cytological samples mainly performed ex vivo during thyroidectomies [24–29, 41, 42]. Hence, in these papers, the authors mainly aimed at the validation of miRNA analysis on cytological samples obtained from ex vivo PTCs during frozen exams, without specific investigation into the “complex” category of FNs [30–36, 42]. To the best of our knowledge, our study is the first prospective thyroid series analyzing miRNAs in FNs on LBC while two previous papers by Keutgen et al. and Agretti et al. studied miRNA expression in 29 ex vivo FNs and in 53 FNs on conventional cytology, respectively [29, 41].
We designed this research to rule out malignancies from the “nightmare” category of FNs and for this reason, we selected five miR-375: miR-221, miR-222, miR-10b, and miR-92a, which are recognized to be up-regulated in malignancies with metastatic behavior and in follicular thyroid carcinomas [40].
In contrast with existing literature, our data suggest that four out of five miRNAs (including 10b, 92a, 221, and 222) exhibited a slightly higher expression among the malignancies; however, no significant difference was noted among the analyzed cytological categories. On the other hand, as also observed by Dettmer, miR-375 seemed to be a novel highly up-regulated marker in thyroid malignancies specifically in both PTCs and FVPCs [43]. The assessment of adequacy for miR-375 on LBC, supported by the evidence of U6 snRNA expression as an endogenous control for RNA adequacy, led us to the conclusion that contrasting results for the four miRNAs may be ascribed to different selections of patients, study designS, cytological categories of the samples, and/or mutational status as demonstrated by Nikiforova et and Chou rather than the use of LBC preparation. Specifically in their series, they proved that miR-221 and miR-222 are mostly up-regulated with two-fold over-expression in tumors carrying out BRAF mutation [26, 36, 46, 47]. Nevertheless, in our series, the category of FN did not harbor any BRAF V600E mutated cases which is in agreement with the statement that this category mainly includes cases with a histological diagnosis of FVPC, notoriously associated with a low BRAF V600E prevalence. Although the bias of our limited figures, the data are in agreement with Nikiforova et and Chou et al., since five out of our 20 PMs, diagnosed as PTC on histology, expressed BRAF V600E mutation and showed higher values of miR-221, 222, and miR-375.
Whereas Hudson et al. found up-regulation of miR-375 in medullary carcinoma, Dettmer et al. demonstrated that miR-375 was also over-expressed in well-differentiated carcinomas (i.e., PTCs and FVPCs). Taking into account this latter evidence, we analyzed its possible application on thyroid cytology for a stratification of malignant risk especially among thyroid cases and/or categories [38, 43]. In fact, data from our current study indicate that miR-375 expression on thyroid LBC may help in suggesting a malignant outcome among FNs. According to the new Italian Classification Thyroid System, our study utilized the subdivision of FNs into TIR3A and TIR3B for the purpose of establishing that the two distinct subsets of lesions (TIR3A and TIR3B) can be correctly matched with different risks of malignancy (TIR3A vs TIR3B; p value <0.0001) [15]. In detail, our data documented that in the TIR3A category we had only one case with the miR-375 value higher than the cut-off level which was correctly associated to the malignant outcome. In the same way, the TIR3B category highlighted a perfect correlation between the histological outcome and miR-375 expression.
Even though we are aware that this new classification system needs to be validated and confirmed by large multi-center studies, for the first time, we found a reliable match between TIR3A or TIR3B morphology and molecular results among the 27 FNs. Therefore, it is interesting to point out that these results of miRNAs may represent an effective aid inasmuch as these two subcategories (TIR3A and TIR4B) required different clinical management (follow-up versus surgery, respectively).
Comparing our results with the scant literature about miRNAs in FNs, we found significantly higher diagnostic accuracy, sensitivity and specificity than those reported by Agretti et al. in their 53 FNs or Shen et al. in their cases with AUS [25, 40]. When we worked out the comparative analysis between FNs and PMs, we found a significant p value (p = 0.00012) with only one false-negative case in the latter category compared to the 16 false-positive and six false-negative cases found by Agretti et al. [41].
Most interestingly, the analysis of the BN and PM categories highlighted that all the BNs with benign histology had a significantly low miR-375 value while 95 % of the PMs were up-regulated and showing also an increasing expression from well-differentiated hystotypes (PTC/FVPC) to MTCs as previously underlined by Dettmer [43]. Moreover, despite the lack of statistical significance, we found slightly lower expression of miR-375 in our encapsulated FVPCs reflecting the new scientific debate about whether the definition of carcinoma is warranted as suggested in recent meetings and studies [48]
Another interesting point to underline is that, to the best of our knowledge, this is the first report assessing the reliable and feasible application of miRNAs on thyroid LBC-stored material.
In our experience, the use of LBC for molecular techniques is feasible and highly reproducible; this molecular application on LBC provides high yields of good quality with the remaining material stored in the preservative solution even some months after FNACs [19, 22, 23]. In fact, the high quality of DNA/RNA extracted from LBC, even after a long period of storage, is comparable and even better than that from conventional preparation [19]. Along similar considerations, Chen et al. underlined that miRNA-based assay is well suited using both ex vivo FNACs (during thyroidectomy) and preoperative in vivo FNAC samples, though they found lower RNA levels and poorer quality than those from the paraffin-embedded group [33]. In spite of the bias of our series, we yielded reliable results on LBC and we reported only a minimal number of cases (7.6 %) which had been excluded because of altered melting curves or an inadequate RNA amount.
We are conscious that the major limit of our series can be attributed to the small cohort of patients, even though this is the largest prospective series of FNs with miR-375 evaluation on LBC with feasible results. In summary, we showed that miR-375 is over-expressed in 100 % of the FNs with a malignant outcome and in 95 % of the PMs. Furthermore, the high sensitivity (97.1 %) and positive predictive value (100 %) in the FNs may suggest its role as a promising marker in the preoperative discrimination between benign and malignant thyroid FNs.
In conclusion, we underline the valuable role of LBC in maximizing the role of cytology and we suggest processing cytological samples with miRNAs (in our experience miR-375) for the purpose of obtaining significant information for the clinical management of patients with thyroid nodules, mainly in the FN category.
Take home message
Our paper deals with the analysis and detection of a miRNA panel applied on liquid-based cytology of thyroid lesions with a specific focus on the challenging category of FN.
miR-375 resulted over-expressed in all malignant FNs and 95 % of the PMs. miR-375 over-expression shows 97.1 % sensitivity, 100 % specificity, 96.3 % negative predictive value (NPV), 100 % positive predictive value (PPV), and 98.3 % diagnostic accuracy. LBC is suitable for miRNAs evaluation and this analysis may represent a valid aid in ruling out BNs and supporting PTCs and/or FVPCs
Authors’ contributions
EDR, LML, MM, TB, GF, SC, and TC carried out the molecular genetic studies, participated in the sequence alignment, and drafted the manuscript. SC, DS, MB, and TC carried out and participated in the sequence alignment. EDR, LML, MM, and TB participated in the design of the study and performed the statistical analysis. EDR, and LML conceived of the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.”
References
J.A. Sosa, J.W. Hanna, K.A. Robinson et al., Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States. Surgery 154, 1420–1426 (2013)
C.M. Kiernan, J.T. Broome, C.C. Solozano, The Bethesda system for reporting thyroid cytopathology: a single-center experience over 5 years. Ann. Surg. Oncol. 21, 3522–3527 (2014)
S. Ali, Thyroid cytopathology: Bethesda and beyond. Acta Cytol. 55, 4–12 (2011)
H.H. Wang, Reporting thyroid fine-needle aspiration: literature review and a proposal. Diagn. Cytopathol. 34, 67–76 (2000)
D.N. Poller, A.K. Ibrahim, M.H. Cummings et al., Fine-needle aspiration of the thyroid. Importance of an indeterminate diagnostic category. Cancer Cytopathol. 90, 239–244 (2000)
G. Fadda, E.D. Rossi, M. Raffaelli et al., Follicular thyroid neoplasms can be classified as low and high risk according to HBME-1 and Galectin 3 expression on liquid based fine needle cytology. Eur. J. Endocrinol. 165, 447–453 (2011)
F. Pagni, M. Prada, P. Goffredo et al., ‘Indeterminate for malignancy’ (TIR3/Thy3 in the Italian and British systems for classification) thyroid fine needle aspiration (FNA) cytology reporting: morphological criteria and clinical impact. Cytopathol 25, 170–176 (2014)
J. Diggans, S.Y. Kim, Z. Hu et al., Machine learning from concept to clinic: reliable detection of BRAFV600E DNA mutations in thyroid nodules using high-dimensional RNA expression data. Pac. Symp. Biocomput. 20, 371–382 (2015)
J.F. Krane, P.A. Vanderlaan, W.C. Faquin et al., The atypia of undetermined significance/follicular lesion of undetermined significance:malignant ratio. Cancer Cytopathol. 120, 111–116 (2012)
A.S. Ho, E.E. Sarti, K.S. Jain et al., Malignancy rate in thyroid nodules classified as Bethesda category III (AUS/FLUS). Thyroid 24, 832–839 (2014)
H. Chen, I. Izevbaye, F. Chen et al., Recent advances in follicular variant of papillary thyroid carcinoma. N. Am. J. Med. Sci. 5, 212–216 (2012)
Walts AE, Mirocha JM, Bose S. Follicular variant of papillary thyroid carcinoma (FVPTC): histological features, BRAF V600E mutation, and lymph node status. J. Cancer Res. Clin. Oncol. 141, 1749–1756 (2015). doi:10.1007/s00432-015-1939-9
E.S. Cibas, S.Z. Ali, The Bethesda system for reporting thyroid cytopathology. Thyroid 19, 1159–1165 (2009)
British Thyroid Association, Royal College of Physicians Guidelines for the management of thyroid cancer, 3rd edn. (RCP, London, 2014)
F. Nardi, F. Basolo, A. Crescenzi et al., Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Invest. 37, 593–599 (2014)
B.C.G. Freitas, J.M. Cerutti, Genetic markers differentiating follicular thyroid carcinoma from benign lesions. Mol. Cell. Endocrinol. 321, 77–85 (2010)
H.G. Correia-Rodrigues, A.A. Nogueira De Pontes, L.F.F. Adan, Use of molecular markers in samples obtained from preoperative aspiration of thyroid. Endocr. J. 59, 417–424 (2012)
M.N. Nikiforova, Y. Nikiforov, Molecular diagnostics and predictors in thyroid cancer. Thyroid 19, 1351–1361 (2009)
G. Fadda, E.D. Rossi, Liquid based cytology in fine needle aspiration biopsies of the thyroid gland. Acta Cytol. 55, 389–400 (2011)
D. Dabbs, C.S. Abendroth, R.T. Grenko et al., Immunocytochemistry on the Thin-prep processor. Diagn. Cytopathol. 17, 388–392 (1997)
A. Longatto-Filho, A.E. Goncalves, O. Martinho et al., Liquid based cytology in DNA-based molecular research. Anal. Quant. Cytol. Histol. 31, 395–400 (2009)
E.D. Rossi, M. Martini, S. Capodimonti et al., Diagnostic and prognostic value of immunocytochemistry and BRAF mutation analysis on liquid based biopsies of thyroid neoplasms suspicious for carcinoma. Eur. J. Endocrinol. 168, 853–859 (2013)
Y.E. Nikiforov, D.L. Steward, T.M. Robinson-Smith et al., Molecular testing for mutations in improving the fine needle aspiration diagnosis of thyroid nodules. J. Clin. Endocrinol. Metab. 94, 2092–2098 (2009)
H. Mazeh, I. Mizrahi, D. Halle et al., Development of a microRNA-based molecular assay for the detection of papillary thyroid carcinoma in aspiration biopsy samples. Thyroid 21, 111–118 (2011)
R. Shen, S. Liyanarachchi, W. Li et al., MicroRNA signature in thyroid fine needle aspiration cytology applied to “atipia of undetermined significance” cases. Thyroid 22, 9–16 (2012)
M.N. Nikiforova, S.I. Chiosea, Y.E. Nikiforov, MicroRNA expression profiles in thyroid microRNAs in thryoid fine needle aspiration biopsy samples. Thyroid 22, 285–291 (2012)
M.N. Nikiforova, G.C. Tseng, D. Steward et al., MicroRNA expression profiling of thyroid tumors: biological significance and diagnistic utility. J. Clin. Endocrinol. Metab. 93, 1600–1608 (2008)
H. Mazeh, Y. Levy, I. Mizrahi et al., Differentiating benign from malignant thyroid nodules using micro ribonucleic acid amplification in residual cells obtained by fine needle aspiration biopsy. J. Surg. Res. 180, 216–221 (2013)
X.M. Keutgen, F. Filicori, M.J. Crowley et al., A panel of four miRNAs accurately differentiates malignant from benign indeterminate thyroid lesions on fine needle aspiration. Clin. Cancer Res. 18, 2032–2038 (2012)
P. Pallante, R. Visone, M. Ferracin et al., MircoRNA deregulation in human thyroid papillary carcinomas. Endocr. Relat. Cancer 13, 497–508 (2006)
F. Weber, R.E. Teresi, C.E. Broelsch et al., A limited set of human microRNA is deregulated in follicular thyroid carcinoma. J. Clin. Endocrinol. Metab. 91, 3584–3591 (2006)
M.T. Tetzlaff, A. Liu, X. Xu, S.R. Master et al., Differential Expression of miRNAs in papillary thyroid carcinoma compared to multinodular goiter using formalin fixed paraffin embedded tissues. Endocr. Pathol. 18, 163–173 (2007)
Y.T. Chen, N. Kitabayashi, X.K. Zhou et al., MicroRNA analysis as a potential diagnostic tool for papillary thyroid carcinoma. Mod. Pathol. 21, 1139–1146 (2008)
S.Y. Sheu, F. Grabellus, S. Schwertheim et al., Differential miRNA expression profiles in variants of papillary thyroid carcinoma and encapsulated follicular thyroid tumors. Br. J. Cancer 102, 376–382 (2010)
Y. Peng, C. Li, D.C. Luo et al., Expression profile and clinical significance of microRNAs in papillary thyroid carcinoma. Molecules 19, 11586–11599 (2014)
C.K. Chou, R.F. Chen, F.F. Chou et al., miR-146 is highly expressed in adult papillary thyroid carcinoma with high risk features including extrathyroidal invasion and the BRAF (V600E) mutation. Thyroid 20, 489–494 (2010)
L. Yip, L. Kelly, Y. Shuai et al., MicroRNA signature distinguishes the degree of aggressiveness of papillary thyroid carcinoma. Ann. Surg. Oncol. 18, 2035–2041 (2011)
J. Hudson, E. Duncavage, A. Tamburrino et al., Over expression of miR-10a and miR-375 and down regulation of YAP1 in medullary thyroid carcinoma. Exp. Mol. Pathol. 95, 62–67 (2013)
J.W. Yan, J.S. Lin, X.X. He, The emerging role of miR-375 in cancer. Int. J. Cancer 135, 1011–1018 (2013)
T. Jikuzono, M. Kawamoto, H. Yoshitake et al., The miR-221/222 custer, miR-10B and miR-92a are highly upregulated in metastatic minimally invasive follicular thyroid carcinoma. Int. J. Oncol. 42, 1858–1868 (2013)
P. Agretti, E. Ferrarini, T. Rago et al., MicroRNA expression profile help to distinguish benign nodules from papillary thyroid carcinomas starting from cells of fine needle aspiration. Eur. J. Endocrinol. 167, 393–400 (2012)
Y. Zhang, Q. Zhong, X. Chen et al., Diagnostic value of microRNAs in discriminating malignant thyroid nodules from benign ones on fine needle aspiration samples. Tumor Biol. 35, 9343–9353 (2014)
M. Dettmer, A. Perren, H. Moch et al., Comprehensive microRNA expression profiling identifies novel markers in follicular variant of papillary thyroid carcinoma. Thyroid 23, 1383–1389 (2013)
M. Dettmer, A. Vogetseder, M.B. Durso et al., MicroRNA expression array identifies novel diagnostic markers for conventional and oncocytic follicular thyroid carcinomas. J. Clin. Endocrinol. Metab. 98, E1–E7 (2013)
American Joint Commission on Cancer (AJCC) Cancer Staging Atlas, 2nd edn. (2013)
M. Xing, BRAF mutationin papillary thyroid cancer: pathogenic role, molecular bases and clinical implications. Endocr. Rev. 28, 742–762 (2007)
T.H. Kim, Y.J. Park, J.A. Lim et al., The association of the BRAFV600E mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer. Cancer 118, 1764–1773 (2012)
M. Drage, B. Howitt, J. Krane, J. Barletta et al., Fine needle aspiration diagnoses of non-infiltrative, non-invasive follicular variant of papillary thyroid carcinoma. Mod. Pathol. 28, S-134A (2015)
Acknowledgments
The authors thank Mrs. Elisabeth Boyle for the invaluable support with the English language.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial, or not-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interests
Additional information
The abstract was prized as the best oral presentation during the 39th European congress of cytology held in Milan September 2015.
Rights and permissions
About this article

Cite this article
Rossi, E.D., Bizzarro, T., Martini, M. et al. The evaluation of miRNAs on thyroid FNAC: the promising role of miR-375 in follicular neoplasms. Endocrine 54, 723–732 (2016). https://doi.org/10.1007/s12020-016-0866-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-016-0866-0