
Abstract
Graves’ disease (GD) is a common autoimmune disease mainly caused by thyroid-stimulating antibodies (TSAbs). Interleukin 21 (IL-21) has recently been reported to play a vital role in the production of pathogenic autoantibodies in several autoimmune diseases, but less is known about GD. This study aimed to investigate the serum levels of IL-21 in GD patients and to explore their association with disease activity. We performed a case–control association study of 152 patients with GD and 32 healthy controls. All patients were further classified into three subgroups: the GD-untreated group (n = 70), the GD-recurrence group (n = 41), and the GD-remission group (n = 41). Serum IL-21 levels were assayed with ELISA. TSAb activity was measured by an in vitro bioassay. Changes in serum IL-21 were also observed in 12 GD patients before and after treatment. Additionally, correlations among the serum IL-21 and free triiodothyronine (FT3), free thyroxine (FT4), thyrotropin (TSH), thyroperoxidase antibodies (TPOAb), thyroglobulin antibodies (TGAb), thyrotropin receptor antibody (TRAb), and TSAb were also analyzed. The serum IL-21 levels in all GD patients were significantly higher than those in the control group (P < 0.001), and specifically, both the GD-untreated and GD-recurrence groups had elevated serum IL-21 compared to the control group (P < 0.001). Moreover, serum IL-21 in newly diagnosed patients markedly decreased after treatment (P < 0.001). Additionally, the serum IL-21 levels in GD-goiter patients were higher than those of the GD-non-goiter patients (P < 0.001). However, no significant differences were found in the serum IL-21 levels in patients with or without Graves’ ophthalmopathy. Importantly, serum IL-21 positively correlated with FT3, FT4, TPOAb, TGAb, and TRAb (r = 0.5053, r = 0.3266, r = 0.1792, r = 0.2445, and r = 0.4096, respectively; all P < 0.0001), and particularly with TSAb activity (r = 0.8171, P < 0.0001), negatively correlated with TSH (r = −0.2713, P < 0.0001). Serum IL-21 levels were significantly elevated in patients with GD and decreased after treatment; moreover, IL-21 may be associated with the clinical disease activity. These observations suggest that IL-21 may play an important role in the pathogenesis of GD.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
A novel cytokine, interleukin 21 (IL-21), has recently been recognized as playing a vital role in the production of pathogenic autoantibodies that lead to end-organ damage in several autoimmune diseases [1–3]. Recent studies have shown that IL-21 is mainly produced by follicular helper T (Tfh) cells, T helper 17 cells, and natural killer (NK) T cells [4–6]. Through the JAK/STAT pathway, IL-21 exerts pleiotropic actions on the immune system [7, 8]. IL-21 can bind to its receptor (IL-21R), which is widely expressed on T cells, B cells, and NK cells, and it can enhance the proliferation of T cells, B cells, and NK cells [5, 9–11]. Specifically, IL-21 can promote the transformation of B cells into memory cells and terminally differentiated Ig-producing plasma cells [10, 11], indicating that IL-21 has an important role in the humoral immune response. Recent studies have demonstrated that IL-21 is associated with the development of multiple immune-mediated diseases, including systemic lupus erythematous (SLE) [12], rheumatoid arthritis (RA) [13], Sjogren’s syndrome [14], multiple sclerosis [15], and type 1 diabetes [3]; however, less is known about the role of IL-21 in Graves’ disease (GD). GD is a common autoimmune disease characterized by thyrotoxicosis, various degrees of diffuse goiter and ophthalmopathy [16]. Although the pathogenesis of GD is complex, the immune response plays a central role in the development of GD, which involves the production of multiple cytokines and aberrant autoantibodies [17]. The most important autoantibodies in GD are thyrotropin (TSH) receptor antibodies (TRAb), including thyroid-stimulating antibody (TSAb) and TSH-binding antibody (TSBAb) [18]. Up to now, TSAb has been considered a pathogenic autoantibody that plays a crucial role in the pathogenesis of GD [19], but the detailed mechanisms involved are not fully understood.
In this study, the serum levels of IL-21 were determined in a case–control association study of 152 patients in different phases of GD and 32 healthy controls. Moreover, changes in the serum IL-21 levels were also observed in 12 cases of the GD-untreated group before and after treatment. Additionally, for the first time, the correlations between serum IL-21, goiter, ophthalmopathy, thyroid hormones, and anti-thyroid autoantibodies, especially TSAbs, were analyzed.
Subjects and methods
Individuals and samples
GD patients in different stages of the disease (n = 152, 34 males and 118 females, aged 18–65 years, and mean age of 37.5 ± 13.3 years) were enrolled in this study from August 2011 to August 2012. The study was conducted at the Department of Endocrinology in the Sun Yat-Sen Memorial Hospital of Sun Yat-Sen University. The diagnosis of GD was based on clinical criteria and confirmed by thyroid function testing and thyroid antibody measurements. The clinical evaluation included the patient’s history as well as the presence of typical symptoms and signs of hyperthyroidism. The laboratory diagnosis included elevated serum free triiodothyronine (FT3) and free thyroxine (FT4) concentrations, low or undetectable serum sensitive TSH (sTSH), and positive TRAb or TSAb. The exclusion criteria were as follows: patients with other coexisting autoimmune diseases or other thyroid disease, patients with carcinoma, patients with medications that could affect the immune system (such as corticosteroids), and patients with a recent history of infectious disease within the past 6 months. Meanwhile, goiter was assessed by experienced endocrinologists and confirmed by thyroid ultrasonography; Graves’ ophthalmopathy (GO) was diagnosed by complete eye examination performed by experienced ophthalmologists [20]. All 152 GD patients were further classified into 3 subgroups, which were as follows: GD-untreated (n = 70)—newly diagnosed patients who had not received antithyroid drugs (ATD) therapy; GD-recurrence (n = 41)—patients who relapsed after the completion of a course of treatment with ATD for 18 months and, after the withdrawal of ATD, remained in the euthyroid state for at least 6 months; and GD-remission (n = 41)—GD patients were in a euthyroid state as a result of treatment with ATD for at least 6 months. Baseline clinical and lab data for all subjects were collected. Additionally, we performed follow-up analyses of 12 patients in the GD-untreated group included in this study before and after 6 months of treatment.
Simultaneously, 32 age- and sex-matched healthy volunteers (6 males and 26 females, aged 19–66 years, and mean age of 34.6 ± 15.1 years) were recruited as the control group. The exclusion criteria for the healthy controls were as follows: normal subjects with a history of thyroid or other autoimmune diseases and with abnormal thyroid function and autoantibodies [FT3, FT4, sTSH, thyroperoxidase antibodies (TPOAb), thyroglobulin antibodies (TGAb), or TRAb].
Moreover, thyroid tissue samples were obtained from six GD patients undergoing thyroidectomy, and the cultured thyrocytes were obtained and assessed for TSAb activity in the serum and for other studies.
The study protocol was approved by the Ethics Committee of Sun Yat-Sen Memorial Hospital of Sun Yat-Sen University and was registered in the Chinese Clinical Trial Registry. Informed consent was obtained from all participants before the study samples were collected.
Sample preparation
Peripheral blood samples from all subjects were collected by venipuncture in the fasting state in the morning and were processed after clotting for 30 min at room temperature. Then, serum specimens were obtained by centrifugation at 1,000×g for 10 min and were stored at −70 °C before measuring the serum levels of IL-21 and the biochemical markers. Repeated freeze–thaw was avoided. The serums FT3, FT4, sTSH, TPOAb, and TGAb were assayed by automated chemiluminescent immunoassays (Siemens ADVIA Centaur CP, MA, USA) according to the manufacturers’ protocol. The serum TRAb was measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (RSR Ltd., Cardiff, UK). The sensitivity and reference ranges of our laboratory are shown in Table 1.
The serum concentration of IL-21
The serum IL-21 concentration was tested in all 152 GD patients and 32 healthy controls using a commercially available ELISA Development kit (PeproTech, (900-K226), USA) according to the manufacturer’s instructions. Briefly, the standards and samples were incubated in a 96-well polystyrene microplate precoated with an anti-IL-21 antibody. The optical density (O.D.) at 450 nm was measured using an automated microplate reader (Wellscan MK3, Thermo labsystem, USA). The serum concentration of IL-21 was then determined by comparing the O.D. of the samples to a standard curve. All experiments were performed in duplicate.
Primary cultured human thyrocytes
Human thyrocytes were obtained from fresh thyroid tissues of GD patients undergoing thyroidectomy (who were euthyroid after previous treatment with ATD), as described previously [21]. In brief, thyroid tissue samples were dissected and minced with scissors into small pieces and incubated with type II collagenase (200 U/mL, Gibco, Carlsbad, USA) in a shaking water bath at 37 °C for 4–6 h. The thyrocytes were then suspended in RPMI 1640 (Gibco) culture medium containing 10 % fetal bovine serum (FBS) (Gibco). Finally, the cells were plated in 75 cm2 tissue culture flasks with RPMI 1640 medium containing 10 % FBS, 1 % penicillin–streptomycin, and 10 mIU/mL bovine TSH (Sigma, St Louis, MO, USA), and the samples were incubated at 37 °C in humidified air atmosphere containing 5 % CO2. After 24 h, the supernatant was removed. The medium was changed every 3 days, and cells were passaged 5–7 days later when the primary cultures of cells were 80 % confluent. Additionally, the identity of the thyrocytes was confirmed by positive immunohistochemical (IHC) staining for thyroglobulin (Maxim-Bio, Fuzhou, China) using a commercially available kit (UltraSensitiveTM Streptavidin-Peroxidase IHC Kit, Maxim-Bio, Fuzhou, China) according to the manufacturer’s instructions. The second passages of thyrocytes were used for the detection of serum TSAb activity and for additional in vitro studies.
TSAb activity measurement
TRAb is clinically classified into TSAb and TSBAb, and TSAb is considered to play a pivotal role in the pathogenesis of GD and is also a useful clinical indicator of disease activity[19, 22]. Therefore, it is very important to identify the TSAb from TRAb. In our study, 20 TRAb-positive sera and 20 TRAb-negative sera were randomly selected from the GD-untreated and control groups, respectively, using a random digits table. TSAb activity was measured using an in vitro bioassay that assessed the capacity of the immunoglobulin G (IgG) to stimulate the degree of cyclic adenosine monophosphate (cAMP) production in human cultured thyrocytes [23]. Briefly, the first step was to extract crude IgG, which was precipitated from 0.4 mL of serum from both patients and controls with 1.2 mL of 20 % polyethylene glycol (PEG4000, Sigma, Missouri, USA), as described in detail elsewhere [23]. Then, the crude lgG was dissolved in RPMI 1640 solution without FBS. The second step was to stimulate the production of cAMP in thyrocytes with the crude IgG. The cultured thyrocytes (2 × 105/well) isolated above were washed twice with phosphate buffer solution and incubated with 0.3 mL of the test IgG. After 5 h of stimulation at 37 °C, the supernatant was obtained to test for cAMP. The third step was the detection of the production of cAMP, which was measured using a competitive binding immunoassay using a commercial kit (R&D, Minneapolis, MN, USA) according to the manufacturer’s instructions. All experiments were performed in duplicate. The last step was calculating the TSAb activity. TSAb activity was expressed as a percentage of the mean values for normal subjects as follows: TSAb activity (%) = [a/b] × 100, where a is the cAMP generated in the presence of the patient’s IgG and b is the cAMP generated in the presence of normal IgG.
Statistical analysis
The Shapiro–Wilk test was applied to analyze the data distribution. Data following a normal distribution were expressed as the mean ± standard deviation (SD). Comparisons between the two GD groups (pre- and post-treatment) were performed using a paired t test; comparisons between the two GD groups (with- and without goiter/GO) were performed using an unpaired t test; and comparisons among more than two difference groups were performed using a one-way ANOVA with the Tukey–Kramer multiple comparison test after a comparison of the homogeneity of variance (homogeneity of variance test). Correlation analysis was determined using the Pearson correlation coefficient. P < 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS17.0 and GraphPad Prism5 software.
Results
-
1.
Baseline clinical characteristics of the study subjects: The clinical characteristics of the patients with GD and healthy volunteers are shown in Table 1. No differences in gender or age were noted between the groups according to the Pearson Chi square test (P > 0.05). However, the serum levels of thyroid hormones (FT3, FT4) and autoantibodies (TPOAb, TGAb, and TRAb) in patients with GD were significantly higher than those in the control group (P < 0.001).
-
2.
Increased TSAb activities in patients with GD: The TSAb activities of GD-untreated patients were significantly higher than those of healthy controls according to an in vitro bioassay (189.01 ± 35.20 vs. 97.47 ± 17.18 %, P < 0.001).
-
3.
Increased serum levels of IL-21 in patients with GD: The average IL-21 serum concentration in all 152 patients with GD was higher than that of healthy controls (101.07 ± 50.97 vs. 36.72 ± 12.33 pg/mL, P < 0.001) (Table 2; Fig. 1a). Moreover, the average serum level of IL-21 in both the GD-untreated and GD-recurrence subgroups was also markedly higher than that of the control group: 134.23 ± 41.05 and 89.11 ± 42.72 versus 36.72 ± 12.33 pg/mL, respectively (all P < 0.001) (Table 2; Fig. 1b). However, the serum levels of IL-21 in the GD-untreated group were higher than the GD-recurrence group (P < 0.001). Importantly, the averages of serum levels of IL-21 in the GD-remission group were higher than that in healthy controls (56.44 ± 31.07 vs. 36.72 ± 12.33 pg/mL, P < 0.001). Additionally, the mean serum level of IL-21 in GD-goiter patients (n = 37) was also higher than that of the GD-non-goiter patients (n = 115): 144.30 ± 47.60 versus 87.07 ± 43.97 pg/mL (P < 0.001) (Table 3; Fig. 1c). Although the serum IL-21 concentration tended to be higher in GO patients, there was no statistically significant difference between the GO patients (n = 22) and GD-non-GO patients (n = 130): 98.62 ± 51.92 versus 109.9 ± 46.46 pg/mL (P = 0.34) (Table 3; Fig. 1d)
Table 2 Serum levels of IL-21 in GD patients and healthy controls (pg/mL) (X ± SD) Fig. 1 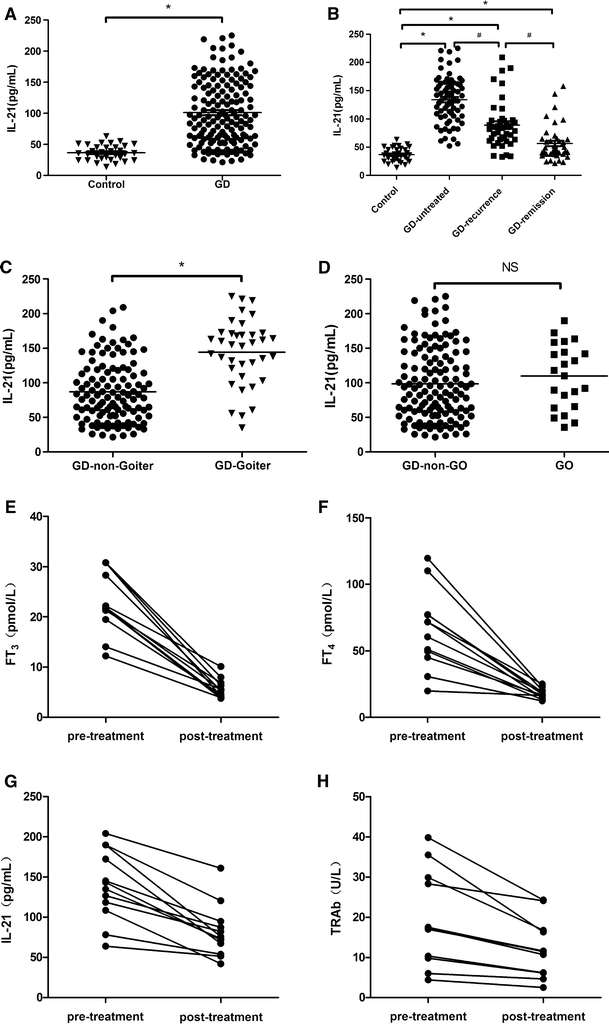
Serum levels of IL-21 in GD patients and their changes before and after treatment (pg/mL) (X ± SD). The serum IL-21 levels of patients with GD and healthy controls were measured by ELISA. GD patients had significantly higher serum IL-21 levels than the healthy controls. *P < 0.001, compared with controls; # P < 0.001, compared with GD-recurrence. a Serum levels of IL-21 in all patients with GD (n = 152) and healthy controls (n = 32). b Serum levels of IL-21 in GD-untreated group (n = 70), GD-recurrence group (n = 41), GD-remission group (n = 41), and in healthy controls (n = 32), respectively. c, d Serum levels of IL-21 in GD-with or without goiter/ophthalmopathy group. e–h, Changes in serum levels of IL-21, FT3, FT4, and TRAb in untreated GD patients (n = 12) before and after treatment for 6 months, respectively. On average, the serum levels of IL-21 were decreased by 41.4 %, FT3 decreased by 75.1 %, FT4 decreased by 72.7 %, and TRAb decreased by 37.3 % compared to the measurements before treatment. GD Graves’ disease, GO Graves’ ophthalmopathy
Table 3 Serum levels of IL-21 of 152 Graves’ disease patients with or without goiter/ophthalmopathy (X ± SD)

Subsequently, 12 GD-untreated patients were followed after ATD therapy for 6 months. The elevated serum levels of IL-21 in these patients were significantly decreased after treatment (139.62 ± 44.12 vs. 81.81 ± 32.60 pg/mL, P < 0.001). Interestingly, this decrease was accompanied by a decrease in the serum thyroid hormones and TRAb pre- and post-treatment (FT3: 22.92 ± 6.24 vs. 5.70 ± 1.89 pmol/L; FT4: 65.34 ± 29.33 vs. 17.81 ± 3.81 pmol/L; and TRAb: 19.42 ± 11.53 vs. 12.17 ± 7.1 U/L, respectively) (P < 0.001) (Table 4; Fig. 1c–f). On average, the serum levels of IL-21 pre- and post-treatment decreased by 41.4 %, TRAb decreased by 37.3 %, FT3 decreased by 75.1 %, and FT4 decreased by 72.7 %, showing that serum IL-21 and TRAb recovered slightly less than thyroid hormones.
-
4.
Correlation between the serum levels of IL-21 and clinical GD parameters: To identify possible correlations between the serum IL-21 levels and disease activity, we analyzed the serum levels of thyroid hormones (FT3, FT4, and TSH) and anti-thyroid autoantibodies (TPOAb, TGAb and TRAb) in all subjects. Statistical analysis revealed that the serum IL-21 in all subjects positively correlated with FT3, FT4, TPOAb, TGAb, and TRAb (r = 0.5053; r = 0.3266; r = 0.1792; r = 0.2445, and r = 0.4096, respectively, all P < 0.0001) (Fig. 2a, b, d–f) and that negatively correlated with TSH (r = −0.2713, P < 0.0001) (Fig. 2c). Particularly, there was a strong correlation with the TSAb activity value in 20 GD-untreated patients and 20 controls (r = 0.8171, P < 0.0001) (Fig. 2g).
Fig. 2 
The correlations between the serum levels of IL-21 and thyroid function and anti-thyroid autoantibodies in all subjects. The correlations between the serum IL-21 and thyroid function (FT3, FT4, TSH) and anti-thyroid autoantibodies (TPOAb, TPGAb, TRAb, and TSAb) in all subjects (including 152 GD patients and 30 controls). a, b, d–f Serum IL-21 positively correlated with FT3, FT4, TPOAb, TGAb, and TRAb (r = 0.5053; r = 0.3266; r = 0.1792; r = 0.2445, and r = 0.4096, respectively, all P < 0.0001); c negatively correlated with TSH (r = −0.2713, P < 0.0001). g Serum IL-21 positively correlated with TSAb activities in 20 patients with untreated-GD and 20 healthy controls (r = 0.8171, P < 0.0001). GD Graves’ disease, TRAb thyrotropin receptor antibody, TPOAb thyroperoxidase antibody, TGAb thyroglobulin antibody, TSAb and thyroid-stimulating antibody

Discussion
In this case–control association study, we assessed the serum levels of IL-21 in patients with GD and the association of serum IL-21 with disease activity in GD. Our results indicate that GD patients had significantly higher serum levels of IL-21 than those in the control group and that these levels decreased after ATD therapy. To the best of our knowledge, our series of analyses establishes for the first time that the IL-21 serum levels positively correlate with FT 3 , FT 4 , TPOAb, TGAb, TRAb, and especially with TSAb in untreated GD patients, negatively with TSH. These results extend a previous study from Jia [24], showing that the IL-21 serum levels are increased in GD patients and providing additional evidence about the association of IL-21 levels with disease activity and changes after treatment. Jia demonstrated that the IL-21 gene single-nucleotide polymorphism rs907715 was significantly associated with GD, and similar results in Chinese Cantonese population were also demonstrated in our group (Genetic Testing and Molecular Biomarkers 2013, unpublished observations); additionally, Jia’s study showed that the IL-21 serum levels increased in a relatively small group of 40 GD patients, but his paper did not describe an association between IL-21 and the levels of thyroid hormones and autoantibodies. Another study from Zhu recently reported that the percentages of circulating Tfh cells and the levels of IL-21 in CD4+T cell were also increased in ten GD patients [25]. Because Tfh cells are the main source of IL-21 [1], an increase in the Tfh cells may account for the increasing levels of IL-21 in GD. These findings indicate that IL-21 may play a vital role in the development of GD. Our results reinforce those from previous studies, and we provide additional clinical evidence that the increased levels of IL-21 correlate with increased TSAb activities more than thyroid hormones. This strongly suggests that the overexpression of IL-21 in GD patients may participate in the pathogenesis of GD by enhancing TSAb production. However, further exploration of this mechanism is needed.
Our data also show that GD patients with goiter have higher serum IL-21 than patients without goiter. Because our data indicate that increased serum levels of IL-21 correlate with increased TSAb in untreated-GD patients, we speculate that enhanced levels of IL-21 might be associated with the presence of thyroid gland hyperplasia and lymphocytes infiltrate as well as the production of TSAb. Previous studies have shown that in GD thyroid tissues lymphocytic infiltrates and ectopic follicles or germinal centers are affected by disorders of autoimmunity [26, 27]. More recently, it has become clear that IL-21 plays a critical role in a variety of regulatory effects on immune responses, particularly the induction of B proliferation and differentiation of immunoglobulin (Ig)-producing plasma cells [10, 11, 28]. Furthermore, IL-21 is also essential in Tfh cell development and GC formation, and it serves as an autocrine amplification loop for its own production and for CD4+ T cell proliferation and survival [1, 6, 28]. TSAbs are all correlated with the formation of thyroid goiter [29], and our data showed that the serum levels of IL-21 in GD are increased and associated with TSAb. Thus, we suppose that the overexpression of IL-21 may directly activate T cells and promote the differentiation of B cells to Ig-secreting plasma cells, which then excrete multiple autoantibodies (specifically TSAbs). In this way, TSAbs could compete with TSH for binding to the thyrotropin receptor and enhance cAMP production, which imitates the biological effects of TSH. The result is the acceleration of the proliferation of thyroid follicles, thereby stimulating synthesis and releasing more thyroid hormones, which in turn gives rise to a series of hyperthyroid symptoms including thyroid gland hyperplasia [16]. However, the detailed role of IL-21 in GD requires further research. Conversely, our results also showed that there were no significant differences in the serum IL-21 levels in patients with and without GO, though GO had a trend toward increased IL-21; these results are similar to those of Jia et al. [24]. It is likely that our sample size is small, which could have impacted the results. Further studies are needed to confirm this preliminary result.
Additionally, we observed the changes of serum levels of IL-21 of all GD patients in different stages as well as clinical parameters. Statistical analysis of the serum IL-21 in different phases of GD revealed that the serum levels of IL-21 in the GD-untreated group were higher than those observed in the GD-recurrence group. One possible explanation is a difference in baseline levels of thyroid hormones (FT3, FT4) and autoantibodies (TRAb) between the two groups; the patients who relapsed were perhaps diagnosed earlier than those who were newly diagnosed. Importantly, elevated serum levels of IL-21 were identified in relapsing GD patients, indicating that the increase in IL-21 is most likely related to disease recurrence. We will conduct additional follow-up to assess the dynamic follow-up of the serum IL-21 level in the same patient with and without disease relapse. As mentioned earlier, though the serum IL-21 levels in the GD-remission patients were decreased after treatment, they were still higher than those of the healthy controls. Therefore, these remission patients, who are euthyroid and TRAb positive, persist to have elevated IL-21, suggesting that the autoimmune disorders are still present and that they should continue ATD therapy, though their thyroid hormones under control. These data indicate that serum IL-21 was associated with the autoimmune status more than thyroid hormones. Similarly, in our study of 12 newly diagnosed patients, the serum level of IL-21 was significantly decreased after treatment, accompanied by decreases in thyroid hormones and TRAb. However, serum IL-21 and TRAb recovered slightly less than thyroid hormones. These findings further suppose that patients with higher serum IL-21, who were euthyroid after treatment, had their autoimmune disorder suppressed in part. Thus, those patients remain in an abnormal immune state rather than in remission, suggesting that they may be at higher risk of relapsing if drugs are withdrawn earlier. Therefore, the persistent high level of IL-21 may be a useful predictor of disease activity. Additional follow-up of our study patients is needed to assess the changes in IL-21 during the course of disease, and there is still much to learn about the related mechanisms.
Our results also showed that TSAb activity was increased in GD-untreated patients and that TSAb is positively correlated with serum IL-21 in untreated-GD patients. TSAb is a useful clinical indicator of disease activity and a predictor of relapse after the cessation of treatment [30–32]. However, detection of TSAb activity in an in vitro bioassay has been restricted because of the expense, technical expertise, and time required. To date, the independent measurement of TSAb and TSBAb in GD serum remains difficult in our clinical diagnostic laboratories [22]. Two types of assays are used in the clinic: an assay measuring TSHRAb binding to the TSHR without functional discrimination, now termed TRAb (including TSAb and TSBAb), and bioassays measuring the functional activity of TSHRAb (TSAb) [33]. Moreover, TRAbs in patients with GD are functionally heterogeneous; they include mainly TSAb and occasionally TSBAb [18]. When crude IgG is extracted from GD patients, it can bind to the TSHR of thyrocytes and then activate TSHR to release cAMP; the varying degrees of cAMP release are indirectly reflective of the TSAb activity. Conversely, though TRAb detection is in common use, TRAb detection still fails to distinguish TSAb from TSBAb in our clinical tests. Thus, the clinical significance of these results is improved in combination with our results above that IL-21 might be one of the useful markers for monitoring the degree of disease activity in GD patients. Similarly, other reports have shown that IL-21 is associated with markers of B cell activation and disease activity in early RA [13, 34].
On the other hand, as regard serum IL-21, it was more related with TSAb than TRAb, TPOAb, or TGAb, the possible reason is that though they are all pathological antibodies produced by B cell in GD, the differences should be caused by different antigens in immune disorder. In addition, several recent papers suggested a potential role of vitamin D deficiency in the pathogenesis and disease activity of GD [35]. In female patients with newly onset GD, serum vitamin D levels are decreased and significantly associated with thyroid volume [36]. Since vitamin D has potent immunomodulatory effects in various autoimmune diseases which inhibit the production of some inflammatory cytokines [37, 38], but it is not known whether vitamin D has a potential modulation of IL-21, and further study would be necessary to conclude. Interestingly, recent studies have focused on the therapeutic potential of targeting IL-21 in autoimmune disease [39, 40]. In an animal model of RA, blocking the IL-21 pathway via the administration of a fusion protein (IL-21R.Fc) ameliorated disease severity [41]; similar results were reported in the mice with SLE [42]. Furthermore, regarding the treatment of GD, existing therapies do not include immunomodulatory drugs; therefore, blocking the IL-21/IL-21R pathway may be a target for GD treatment in the future.
Conclusion
In conclusion, the serum levels of IL-21 were significantly higher in patients with GD than in healthy individuals, and the levels decreased after treatment. Serum levels of IL-21 were correlated with disease activity in GD patients, suggesting that IL-21 participates in the pathogenesis of GD and could potentially be used as a marker of disease activity.
Abbreviations
- cAMP:
-
Cyclic adenosine monophosphate
- CV:
-
Coefficient of variation
- ELISA:
-
Enzyme-linked immunosorbent assay
- FBS:
-
Fetal Bovin Serum
- FT3 :
-
Free T3
- FT4 :
-
Free thyroxine
- GC:
-
Germinal center
- GD:
-
Graves’ disease
- Ig:
-
Immunoglobulin
- IL-21:
-
Interleukin-21
- OD:
-
Optical density
- PBS:
-
Phosphate buffer solution
- RA:
-
Rheumatoid arthritis
- SD:
-
Standard deviation
- SLE:
-
Systemic lupus erythematous
- SNPs:
-
Single nucleotide polymorphismsin
- s-TSH:
-
Sensitive thyrotropin
- Tfh:
-
T follicular helper
- TGAb:
-
Thyroglobulin antibody
- Th17:
-
T helper 17
- TPOAb:
-
Thyroperoxidase antibody
- TRAb:
-
TSH receptor antibody
- TSAb:
-
Thyroid stimulatory antibody
References
R. Spolski, W.J. Leonard, IL-21 and T follicular helper cells. Int. Immunol. 22(1), 7–12 (2010)
R. Liu, Q. Wu, D. Su et al., A regulatory effect of IL-21 on T follicular helper-like cell and B cell in rheumatoid arthritis. Arthr. Res. Ther. 14(6), R255 (2012)
R. Spolski, M. Kashyap, C. Robinson et al., IL-21 signaling is critical for the development of type I diabetes in the NOD mouse. Proc. Natl. Acad. Sci. USA 105(37), 14028–14033 (2008)
J. Parrish-Novak, S.R. Dillon, A. Nelson et al., Interleukin 21 and its receptor are involved in NK cell expansion and regulation of lymphocyte function. Nature 408(6808), 57–63 (2000)
J.M. Coquet, K. Kyparissoudis, D.G. Pellicci et al., IL-21 is produced by NKT cells and modulates NKT cell activation and cytokine production. J. Immunol. 178(5), 2827–2834 (2007)
A. Vogelzang, H.M. Mcguire, D. Yu et al., A fundamental role for interleukin-21 in the generation of T follicular helper cells. Immunity 29(1), 127–137 (2008)
B.J. Dien, P. Gelebart, M. Anand et al., IL-21 contributes to JAK3/STAT3 activation and promotes cell growth in ALK-positive anaplastic large cell lymphoma. Am. J. Pathol. 175, 825–834 (2009)
S. Crotty, Follicular helper CD4 T cells (TFH). Annu. Rev. Immunol. 29, 621–663 (2011)
W.J. Leonard, R. Spolski, Interleukin-21: a modulator of lymphoid proliferation, apoptosis and differentiation. Nat. Rev. Immunol. 5(9), 688–698 (2005)
D. Konforte, N. Simard, C.J. Paige, IL-21: an executor of B cell fate. J. Immunol. 182(4), 1781–1787 (2009)
K. Brandt, P.B. Singh, S. Bulfone-Paus et al., Interleukin-21: a new modulator of immunity, infection, and cancer. Cytokine Growth Factor Rev. 18(3–4), 223–232 (2007)
S. Dolff, W.H. Abdulahad, J. Westra et al., Increase in IL-21 producing T-cells in patients with systemic lupus erythematosus. Arthr. Res. Ther. 13(5), R157 (2011)
J.E. Gottenberg, J.M. Dayer, C. Lukas et al., Serum IL-6 and IL-21 are associated with markers of B cell activation and structural progression in early rheumatoid arthritis: results from the ESPOIR cohort. Ann. Rheum. Dis. 71(7), 1243–1248 (2012)
R.H. Scofield, IL-21 and Sjogren’s syndrome. Arthr. Res. Ther. 13(6), 137 (2011)
J.S. Tzartos, M.J. Craner, M.A. Friese et al., IL-21 and IL-21 receptor expression in lymphocytes and neurons in multiple sclerosis brain. Am. J. Pathol. 178(2), 794–802 (2011)
A.P. Weetman, Graves’ disease. N. Engl. J. Med. 343(17), 1236–1248 (2000)
D. Pan, Y.H. Shin, G. Gopalakrishnan et al., Regulatory T cells in Graves’ disease. Clin. Endocrinol. (Oxf) 71(4), 587–593 (2009)
B. Rapoport, G.D. Chazenbalk, J.C. Jaume et al., The thyrotropin (TSH) receptor: interaction with TSH and autoantibodies. Endocr. Rev. 19(6), 673–716 (1998)
B. Rapoport, S.M. Mclachlan, Thyroid autoimmunity. J. Clin. Invest 108(9), 1253–1259 (2001)
M.P. Mourits, L. Koornneef, W.M. Wiersinga et al., Clinical criteria for the assessment of disease activity in Graves’ ophthalmopathy: a novel approach. Br. J. Ophthalmol. 73(8), 639–644 (1989)
W.E. Hinds, N. Takai, B. Rapoport et al., Thyroid-stimulating immunoglobulin bioassay using cultured human thyroid cells. J. Clin. Endocrinol. Metab. 52(6), 1204–1210 (1981)
K. Tan, T.P. Loh, S. Sethi, Lack of standardized description of TRAb assays. Endocrine 43(3), 732–733 (2013)
Y. Ochi, K. Yamashiro, N. Takasu et al., Sensitive assay to detect thyroid stimulating antibody (TSAb) in the presence of thyroid stimulation blocking antibody (TSBAb) in serum. Horm. Metab. Res. 33(2), 115–120 (2001)
H.Y. Jia, Z.G. Zhang, X.J. Gu et al., Association between interleukin 21 and Graves’ disease. Genet. Mol. Res. 10(4), 3338–3346 (2011)
C. Zhu, J. Ma, Y. Liu et al., Increased frequency of follicular helper T cells in patients with autoimmune thyroid disease. J. Clin. Endocrinol. Metab. 97(3), 943–950 (2012)
G. Aust, D. Sittig, L. Becherer et al., The role of CXCR5 and its ligand CXCL13 in the compartmentalization of lymphocytes in thyroids affected by autoimmune thyroid diseases. Eur. J. Endocrinol. 150(2), 225–234 (2004)
B.S. Iwona, S.S. Jadwiga, K. Elzbieta et al., Lymphocytes in peripheral blood and thyroid tissue in children with Graves’ disease. World J. Pediatr. 4(4), 274–282 (2008)
K. Ozaki, R. Spolski, C.G. Feng et al., A critical role for IL-21 in regulating immunoglobulin production. Science 298(5598), 1630–1634 (2002)
Y. Abe, Apoptosis in the pathogenesis of autoimmune thyroid disease. Nihon Rinsho 57(8), 1717–1722 (1999)
D. Sinclair, Clinical and laboratory aspects of thyroid autoantibodies. Ann. Clin. Biochem. 43(Pt 3), 173–183 (2006)
M. Schott, W.B. Minich, H.S. Willenberg et al., Relevance of TSH receptor stimulating and blocking autoantibody measurement for the prediction of relapse in Graves’ disease. Horm. Metab. Res. 37(12), 741–744 (2005)
N. Takasu, M. Matsushita, Changes of TSH-stimulation blocking antibody (TSBAb) and thyroid stimulating antibody (TSAb) over 10 years in 34 TSBAb-positive patients with hypothyroidism and in 98 TSAb-positive Graves’ patients with hyperthyroidism: reevaluation of TSBAb and TSAb in TSH-receptor-antibody (TRAb)-positive patients. J. Thyr. Res. 2012, 182176 (2012)
B. Rapoport, S. Filetti, N. Takai et al., Studies on the cyclic AMP response to thyroid stimulating immunoglobulin (TSI) and thyrotropin (TSH) in human thyroid cell monolayers. Metabolism 31(11), 1159–1167 (1982)
T.K. Rasmussen, T. Andersen, M. Hvid et al., Increased interleukin 21 (IL-21) and IL-23 are associated with increased disease activity and with radiographic status in patients with early rheumatoid arthritis. J. Rheumatol. 37(10), 2014–2020 (2010)
M. Rotondi, L. Chiovato, Vitamin D deficiency in patients with Graves’ disease: probably something more than a casual association. Endocrine 43(1), 3–5 (2013)
T. Yasuda, Y. Okamoto, N. Hamada et al., Serum vitamin D levels are decreased in patients without remission of Graves’ disease. Endocrine 43(1), 230–232 (2013)
T. Yasuda, Y. Okamoto, N. Hamada et al., Serum vitamin D levels are decreased and associated with thyroid volume in female patients with newly onset Graves’ disease. Endocrine 42(3), 739–741 (2012)
F. Baeke, T. Takiishi, H. Korf et al., Vitamin D: modulator of the immune system. Curr. Opin. Pharmacol. 10(4), 482–496 (2010)
H. Sondergaard, K. Skak, IL-21: roles in immunopathology and cancer therapy. Tissue Antigens 74(6), 467–479 (2009)
G. Monteleone, F. Pallone, T.T. Macdonald, Interleukin-21 as a new therapeutic target for immune-mediated diseases. Trends Pharmacol. Sci. 30(8), 441–447 (2009)
A.K. Andersson, M. Feldmann, F.M. Brennan, Neutralizing IL-21 and IL-15 inhibits pro-inflammatory cytokine production in rheumatoid arthritis. Scand. J. Immunol. 68(1), 103–111 (2008)
J.A. Bubier, S.M. Bennett, T.J. Sproule et al., Treatment of BXSB-Yaa mice with IL-21R-Fc fusion protein minimally attenuates systemic lupus erythematosus. Ann. N. Y. Acad. Sci. 1110, 590–601 (2007)
Acknowledgments
We would like to thank the participation of the patients and healthy volunteers. We also thank Honghao Li, MiaoYun Long, and Mingqing Huang (Department of Thyroid Surgery); Feng Li, Jiuyin Tang, Na Li, and Xiaoyi Wang (Department of Endocrinology) for excellent technical assistance, valuable suggestions, and/or critical comments. Clinical Trial Registration Number: ChiCTR-OCC-11001462
Conflict of interest
None of the authors have any conflicts of interest to declare in connection with this manuscript.
Funding
This work supported by Guangdong Provinces Science and Technology Project (Grant no. 2011B031800162), and Guangdong medical science and technology research foundation (Grant no. A2010166).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Jin Zhang and Hua Zeng have contributed equally to this work.
Rights and permissions
About this article
Cite this article
Zhang, J., Zeng, H., Ren, M. et al. Interleukin-21 is associated with disease activity in patients with Graves’ disease. Endocrine 46, 539–548 (2014). https://doi.org/10.1007/s12020-013-0105-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-013-0105-x