
Abstract
Background
Musculoskeletal disease is a major cause of disability in the global burden of disease, yet data regarding the magnitude of this burden in developing countries are lacking. The Surgeons OverSeas Assessment of Surgical Need (SOSAS) survey was designed to measure the incidence and prevalence of surgically treatable conditions, including musculoskeletal conditions, in patients in low- and middle-income countries, and was administered in the West African nation of Sierra Leone in 2012.
Purpose
We attempted to quantify the burden of potentially treatable musculoskeletal conditions in patients in Sierra Leone.
Methods
A cross-sectional two-stage cluster-based survey was performed in Sierra Leone using the SOSAS. Two individuals from each randomly selected household underwent a verbal head to toe examination. The musculoskeletal-related questions from the SOSAS survey in Sierra Leone were analyzed to determine the prevalence of musculoskeletal problems in the study population. Prevalence is reported as the number of respondents with a musculoskeletal problem now and number of respondents with a musculoskeletal problem during the past year. Respondents had “no need” for care, they “received care”, or they faced a barrier that prevented them from receiving care.
Results
One thousand eight hundred seventy-five households were targeted, with 1843 undergoing the survey, which yielded 3645 individual respondents. Of the individual respondents, 462 (n = 3645; 12.6% of total; 95% CI, 12%–13%) had a traumatic musculoskeletal problem during the past year, and 236 (n = 3645; 6% of total; 95% CI, 5%–7%) respondents had a musculoskeletal problem of nontraumatic etiology. Of respondents with either a traumatic or nontraumatic musculoskeletal problem, 359 (n = 562; 63.9% of total; 95% CI, 59.5–68.3%) needed care but were unable to receive it with the major barrier reported as financial.
Conclusion
Resource allocation decisions in global health are made based on burden of disease data in low- and middle-income countries. The data provided here for Sierra Leone may offer some generalizable insight into the scope of the burden of musculoskeletal disease for low- and middle-income countries, especially in Sub-Saharan Africa, and provide concrete evidence that musculoskeletal health should be included in the global health discussion. However, there may be important differences across countries in this region, and further study to elucidate these differences seems critical given the large burden of disease and the limited resources available in these regions to manage it.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Musculoskeletal disease encompasses a wide range of conditions that vary from traumatic injury to congenital malformations, disabling arthritides to chronic low back pain, many of which benefit from surgical interventions. They affect a large portion of the world’s population in one form or another, with nontraumatic musculoskeletal disease estimated to account for 6.8% of all disability-adjusted life years lost according to the latest Global Burden of Disease studies [27, 37]. However this 6.8% of disability-adjusted life years does not include those lost owing to musculoskeletal trauma. Traumatic injury is estimated to cause 9% of annual deaths and accounts for 11% of global disability-adjusted life years, more than is attributed to HIV, malaria, and tuberculosis combined [27]. An estimated 70% of traumatic injuries in populations in low- and middle-income countries occur in the extremities [20, 27, 32]. These previous data indicate that musculoskeletal conditions, traumatic or nontraumatic, are a substantial contributor to the global burden of disease, and deserve attention by those who set the global health agenda [3, 6, 19]. The capacity to deal with disabling, chronic, and acute musculoskeletal conditions will be met only by increasing surgical capacity in low- and middle-income countries [6, 19, 35]. To allow for informed allocation of resources for strengthening health systems, the little data that exist must be expanded on so that the scope of the burden of musculoskeletal disease in low- and middle-income countries may be known [5, 8, 22, 38]. The epidemiology of musculoskeletal disease in Sierra Leone is presented here with the goal of encouraging the development of programs to address the burden of musculoskeletal impairment and disability in Sierra Leone and other low- and middle-income countries. By reporting on the burden of disease in Sierra Leone, decision-makers working in other low- and middle-income countries may examine the burden of musculoskeletal disease in their geographic scope and develop programs to address musculoskeletal disease.
Some studies of the burden of musculoskeletal disease have been performed in high-income countries, with few population-based studies in low- and middle-income countries [2, 39]. Atijosan et al. [2] reported that the prevalence of musculoskeletal impairment in the population in Rwanda was 5.2%, with an estimated 814,000 treatments and 184,000 operations required by the Rwandese population of 8.4 million. To our knowledge, their study is the only available population-based study of musculoskeletal disease in a low-income country. Some published data are extrapolated from hospital-based surveys, however these data have limited generalizability owing to various factors that prevent access to care such as cost, transportation, and availability [12, 24]. In a health system that does not provide effective coverage to an entire population, the most accurate method of determining disease prevalence and burden is via cross-sectional studies using population-based sampling methods [7].
We therefore undertook a population-based survey to estimate the musculoskeletal burden of disease for the small, West African nation of Sierra Leone using the Surgeons OverSeas Assessment of Surgical Need (SOSAS) survey [10], which was developed to evaluate the burden of surgically treatable conditions in low- and middle-income countries.
Methods
Setting
The full study methods were described previously, therefore the following is a condensed description [11]. Sierra Leone, a small country in West Africa, ranks 177 of 187 nations [36] on the United Nations Development Index. Life expectancy at birth is 48 years, an estimated 185.3 per 1000 children die before they are 5 years old, and the maternal mortality rate was 890 per 100,000 live births, the third highest in the world in 2010 [34]. Surgeons OverSeas has had a long-standing collaboration with the Ministry of Health and Sanitation of Sierra Leone, and therefore chose Sierra Leone as the pilot country for implementing the SOSAS survey [11, 18].
Study Design
A cluster randomized survey study design was used. Sierra Leone’s smallest administration unit is called an enumeration area, and 75 of 9671 enumeration areas were randomly selected to be study clusters. These were chosen in two stages, first with stratification for districts and urban and rural population distributions, then with a probability proportional to population size. Weighting was achieved via random selection of 25 households in each cluster [4]. The principles outlined for achieving random selection of households for countries without population registries were used which includes an initial structure count (house count) with subsequent randomization using a random number generator [4, 13].
Data were gathered between January and February 2012. A questionnaire was administered to the head of household regarding socioeconomic and demographic information of all household members [33](Appendix 1. Supplemental material is available with the online version of CORR®). Two members of each household then were chosen at random to respond to a questionnaire designed to collect information regarding problems potentially requiring surgical consultation, including all musculoskeletal problems. Each respondent was asked whether they had experienced a musculoskeletal problem now or during the past year. If they responded affirmatively, a full questionnaire designed to elicit the body region, type of problem, and treatment received was conducted. All interviews were conducted verbally in the appropriate local language.
Demographic Data
Data were collected and analyzed from 1843 of the 1875 targeted households which yielded 3645 respondents, yielding a response rate of 98%. The population sampled was a representative sample, as the demographic composition of the study population is similar to the most recent Sierra Leone Demographic Health Survey (2008) [31]. Of the 3645 individual respondents, the mean (SD) age of respondents was 25 years (19.7 years) and the median age was 20 years (range, 0–100 years), with 36% younger than 15 years, 59% between 15 and 65 years, and only 5% older than 65 years. Age information was missing for 42 respondents. Males comprised 46% of the sample population. A greater percentage of respondents lived in rural (61%) as compared with urban areas (39%) (Table 1).
Statistical Analysis
Respondents were stratified by age groups; children, 0 to 14 years old; adults, 15 to 65 years old; and elderly, older than 65 years. Proportions were compared between groups using a chi-square test. Logistic regression analyses were conducted using ProcSurvey Logistic (SAS 9.3, Cary, NC, USA) to generate the odds of having a musculoskeletal problem while adjusting for potential confounders. Probability values of 0.05 or less were considered statistically significant.
Ethical Clearance
Ethical approval was obtained from the Ethics and Scientific Review Committee of Sierra Leone, and the Research Ethics Committee of the Royal Tropical Institute in Amsterdam. Written informed consent was obtained from all respondents, and if younger than 18 years, the respondent and his or her parent or guardian. For respondents younger than 12 years, a parent or guardian responded for the child or assisted with the interview.
Results
Prevalence of Musculoskeletal Problems
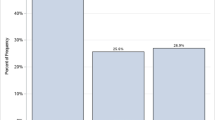
A total of 921 (25%; n = 3645) respondents reported a musculoskeletal problem at some point in their lives, 698 (19%; n = 3645) had a musculoskeletal problem during the past year, and 515 (14%; n = 3645) had a musculoskeletal problem at the time of the survey. Problems then were categorized as traumatic or nontraumatic. A total of 256 (7%; n = 3645) respondents reported a nontraumatic musculoskeletal problem during their lifetime, 236 (6%; n = 3645) had a nontraumatic musculoskeletal problem during the past year, and 209 (6%; n = 3645) had a nontraumatic musculoskeletal problem at the time of the survey. One respondent answered that he/she had a musculoskeletal problem, but did not answer the question regarding traumatic or nontraumatic, therefore the data for 920 respondents are provided (Table 2). These problems are defined as “complaints/symptoms significant enough to warrant medical attention if it was available”. The likelihood of having a nontraumatic musculoskeletal problem was greater among adults (odds ratio [OR], 2.65; 95% CI, 1.88–3.73) and elderly individuals (OR, 9.38; 95% CI, 5.69–15.47) than in children (Table 3). Females were equally likely to have a nontraumatic musculoskeletal problem as males (OR, 0.89; 95% CI, 0.68–1.16). Rural residency as opposed to urban residency was associated with a greater likelihood of having a nontraumatic musculoskeletal problem (OR, 1.44; 95% CI, 1.08–1.92).
The odds of having a nontraumatic musculoskeletal problem were greater among nonfarmers (OR, 2.04; 95% CI, 1.45–2.87) and farmers (OR, 3.40; 95% CI, 2.46–4.71) compared with unemployed respondents. Having a primary education was associated with a decreased odds of having a nontraumatic musculoskeletal problem (OR, 0.49; 95% CI, 0.34–0.72), although having a secondary or tertiary education did not change the results.
Types of Musculoskeletal Problems
For children with nontraumatic musculoskeletal problems (n = 49), 36% were attributable to congenital deformity, 28% to a mass or a growth, 22% to an acquired deformity, 8% to a wound not associated with an injury, and 2% were categorized as recurrent drainage (Table 4). Acquired deformity was significantly (p < 0.001) less common in children than in adults or the elderly. Congenital deformities were significantly (p < 0.001) more common in children than in adults, and were not seen in the elderly. For adults with nontraumatic musculoskeletal problems (n = 185), 46% were attributable to acquired deformities, 28% to a mass or a growth, 16% to a wound not associated with injury, 7% to recurrent drainage, and 5% to a congenital deformity. Of the nontrauma-associated musculoskeletal problems in the elderly (n = 38), 73% were attributable to acquired deformity, 22% to a mass or a growth, and 8% to wounds not associated with injury. No statistically significant differences in types of musculoskeletal problems were noted between sexes in all categories.
Affected Body Parts
The back was the most affected part of the body, with 33% (97 of 293) of all reported nontraumatic musculoskeletal problems (Table 5). The elderly were most affected by back problems, which accounted for 49% of all musculoskeletal problems in the elderly (18 of 44), followed by 35% of adults (70 of 198), and 18% of children (nine of 51) (p = 0.0115). Back problems accounted for 38% of all problems in males (49 of 139) and 30% in females (48 of 154), with no significant differences found. Back problems accounted for 39% of problems in farmers (42 of 112), 28% in nonfarm workers (30 of 94), and 33% in unemployed persons (25 of 86), with no statistical differences seen among the groups (Table 6). Foot problems accounted for 14% of problems in the elderly (five of 44), 19% in adults (34 of 198), and 28% in children (15 of 51). They were present in 21% of males (25 of 139) and 19% of females (29 of 154) reporting problems. The lower leg caused 24% of problems in the elderly (nine of 44), 15% of problems in adults (27 of 198), and 28% in children (14 of 51) (p = 0.047), with males having a significantly different incidence (24% of problems [29 of 139] versus 15% of problems [21 of 154]) than females (p = 0.03). The upper leg caused problems in 19% of elderly respondents (seven of 44), 14% of adults (24 of 198), and 12% of children (six of 51), with no differences noted between the sexes. Upper arm problems accounted for 5% of problems in the elderly (two of 44), 8% in adults (15 of 198), and 4% in children (two of 51), with no difference between the sexes. No differences were found for lower arm problems between the age or gender groups. Hand problems were seen in 4% of adults (eight of 198), and there were no problems among children or the elderly. No differences in the incidence of hand problems were seen between males or females.
Access to Care
A total of 78% of the respondents (143 of 183) with nontraumatic musculoskeletal problems who desired care were not able to access that care. The major barriers were lack of money for care, which affected 69% of respondents (98 of 143), followed by lack of skilled health providers in the area, which affected 15.4% (Table 7).
Discussion
Musculoskeletal problems are a substantial contributor to the global burden of disease, yet the scale of their contribution in the developing world is not fully known. By separating traumatic musculoskeletal problems from nontraumatic, better insight into the health needs of a population can be achieved. A previous study of musculoskeletal disease in low- and middle-income countries focused on disability attributable to musculoskeletal problems [2], which may capture short-term problems such as injury. The capacity to deal with disabling, chronic, and acute musculoskeletal conditions will be met only by increasing surgical capacity in low- and middle-income countries [6, 19, 35]. To allow informed allocation of resources for strengthening health systems, the scope of the problem must be known [5, 8, 22, 38]. The estimated prevalence of nontraumatic musculoskeletal problems is 5.7%, with an estimated yearly prevalence of 6.4%. Of the respondents with nontraumatic musculoskeletal problems that occurred during the past year, 78% (143 of 183) desired evaluation by a healthcare provider, yet only 22% (40 of 183) of the respondents desiring care actually received it. These data indicate a large burden of debilitating nontraumatic musculoskeletal disease that remains untreated and likely has a substantial effect on the lives and livelihoods of the population in Sierra Leone. When the prevalence is extrapolated to the general population, approximately 246,000 persons in Sierra Leone each year have a problem with their musculoskeletal system unrelated to trauma for which they desire evaluation. With trauma included, this number increases to approximately 890,000 persons of a population of 5.9 million persons [40] desiring evaluation for a musculoskeletal problem.
This study had numerous limitations. First, the study relied on self-reporting by respondents, which owing to recall bias, may result in certain problems being underestimated. No physical examinations were performed to validate the accuracy of self-reporting, however this study design probably has less underreporting than hospital-based studies, which exclude all of the population who cannot access health services. This was approximately 50% in our study. The survey attempted to parse out the individuals who had problems for which they did not think they needed to see a doctor via the access to care questions; however the study was not validated via physical examination and diagnostic testing, and thus depends solely on patient reporting. The lack of a physical examination also may affect estimates of what types of musculoskeletal conditions are reported. The survey was designed to capture the prevalence of surgically treatable conditions, therefore musculoskeletal conditions that are not amenable to surgery may be underreported. The validity of the survey has not been evaluated in a population with a known prevalence of musculoskeletal problems. However, to our knowledge, there are no published reports of a validated survey in a population with a known prevalence of musculoskeletal conditions in a low-income country. We think that our data, although not perfect, are the best estimates available of the burden of musculoskeletal conditions in a low-income country.
The demand in Sierra Leone for musculoskeletal care appears to be great when compared with estimates from previously published population-based and extrapolative studies [2, 27, 30]; however we are aware of only one other population-based survey of musculoskeletal problems in a developing country [2]. Atijosan et al. [2] measured musculoskeletal impairment in Rwanda as 5.2% overall prevalence using a standardized survey, history, and physical examination by a trained physiotherapist. Their results focus specifically on long-term problems related to physical impairments of the musculoskeletal system in an effort to contribute to data for calculation of disability. The numbers in our study reflect self-identified musculoskeletal problems, many of which would benefit from evaluation, and may represent short-term or long-term problems. The WHO Global Burden of Disease study was used to extrapolate an 8.4% global prevalence of musculoskeletal disease after excluding rheumatoid arthritis, osteoarthritis, gout, and low back or neck pain [30]. However, much of these data are based on extrapolations from nonpopulation-based surveys, thereby excluding patients who do not have access to care. Smith et al. [30] were not able to find any suitable data in Sub-Saharan Africa for inclusion in their estimate on the burden of musculoskeletal disease worldwide.
We found a higher frequency of musculoskeletal problems during the past year with increasing age, similar to patterns observed in developed countries [39]. Individuals living in rural areas were more likely to have musculoskeletal problems than were individuals living in urban areas. Lacerations and crush injuries typically are the most common causes of extremity problems in individuals in these areas, but sequelae of distant trauma, such as posttraumatic arthritis and deformities, also are likely in a population with high incidences of injury [1, 23, 26, 32]. In addition to injuries, back and lower extremity problems are common among farmers, which would be expected owing to the physically difficult nature of the work [16]. The rural population also has decreased access to care through decreased ability to pay and fewer providers in the area, thereby exacerbating any musculoskeletal problems needing care, (ie, turning a fracture into an acquired deformity via malunion or nonunion, or mild osteoarthritis into debilitating osteoarthritis). The patterns of disease in the rural versus urban populations will likely be similar to those of other countries with similar economies and population structures, especially in the same geographic region.
The major barrier to care identified was the lack of money to pay for care. The costs of care have been proven to be a major deterrent for those needing treatment for injuries and surgical problems [9, 12, 21, 24], therefore it is not surprising that this is the major obstacle in the provision of care in Sierra Leone with a per capita gross national income of USD 830 [34]. When looking at the barriers to care, there is a trend showing increased difficulty with accessing care for the population with nontraumatic musculoskeletal problems. This would make sense in the context of a low-income country, as trauma care generally is more available than primary or surgical musculoskeletal care (ie, if you have a fracture, typically family or friends will transport patients to hospitals for treatment). Without an acute injury however, access to care could depend more on financial or local medical resources. One study showed that treatment was deferred at more district or tertiary hospitals until the patient has accumulated enough money by saving, borrowing, or selling [17]. The costs of seeking treatment were either too great or outweighed the benefits of staying and working at home, but the root causes of this in our study are unclear. The lack of providers was identified as a barrier to care, although this is to be expected in a country with a population of 5.8 million and only 0.2 physicians and 1.7 nurses per 100,000 of the population [40].
There have been calls for international help in funding of population, policy, and implementation research on scaling up interventions for noncommunicable diseases and injuries [14]. Approximately 11% of recent economic growth in low- and middle-income countries is attributable to reductions in mortality [14]. The logical progression to addressing these problems involves defining the scope of the problem, identifying interventions that are implementable and cost-effective, and then studying the effect of those interventions. There are many possible interventions, some of which are easier to implement than others. Interventions can take the form of training rural providers, be they traditional healers or trained in Western medicine, to treat patients with the conditions they can, and to recognize patients with what types of conditions to send to tertiary centers [28], training taxi drivers to administer basic first aid [15], implementing new types of equipment or implants and training local surgeons to use them [29], training providers at tertiary centers, creating partnerships with international institutions to try to foster local research or educational exchange [25], or advocate for funding from governments or international funding sources for these types of programs.
There is lack of research regarding the prevalence of musculoskeletal problems requiring treatment in developing nations. When attempting to improve the health of a population in a nation such as Sierra Leone, musculoskeletal health needs to be included in the disease categories to be targeted, and therefore deserves a place in the global health discussion. Future studies should examine regional variations in musculoskeletal health, such as the differences between musculoskeletal problems seen in individuals in urban versus rural areas in low-income countries, and variations between continents and subcontinents (for example, does the epidemiology of musculoskeletal disease vary substantially among countries in Sub-Saharan Africa?). Additionally, further study of the severity of musculoskeletal problems, musculoskeletal-related disability, and economic effect of that disability should be done to emphasize the importance of allocating money and resources to address a significant deficit in health infrastructure in low- and middle-income countries. The data presented here add credence to the argument that musculoskeletal health and injury should be a funding priority for global health-funding organizations, and readers concerned with international musculoskeletal health should be familiar with the magnitude of the problem.
References
Angoules AG, Lindner T, Vrentzos G, Papakostidis C, Giannoudis PV. Prevalence and current concepts of management of farmyard injuries. Injury. 2007;38(suppl 5):S27–34.
Atijosan O, Rischewski D, Simms V, Kuper H, Linganwa B, Nuhi A, Foster A, Lavy C. A national survey of musculoskeletal impairment in Rwanda: prevalence, causes and service implications. PLoS One. 2008;3:e2851.
Bae JY, Groen RS, Kushner AL. Surgery as a public health intervention: common misconceptions versus the truth. Bull World Health Organ. 2011;89:394.
Bennett S, Woods T, Liyanage WM, Smith DL. A simplified general method for cluster-sample surveys of health in developing countries. World Health Stat Q. 1991;44:98–106.
Debas HT, Gosselin R, McCord C, Thind A. Surgery. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, Jha P, Mills A, Musgrove P, eds. Disease Control Priorities in Developing Countries. Washington DC: The International Bank for Reconstruction and Development/The World Bank Group; 2006.
Farmer PE, Kim JY. Surgery and global health: a view from beyond the OR. World J Surg. 2008;32:533–536.
Gordis L. Epidemiology. 4th ed. Philadelphia, PA: Saunders; 2008.
Gosselin RA, Thind A, Bellardinelli A. Cost/DALY averted in a small hospital in Sierra Leone: what is the relative contribution of different services? World J Surg. 2006;30:505–511.
Grimes CE, Bowman KG, Dodgion CM, Lavy CB. Systematic review of barriers to surgical care in low-income and middle-income countries. World J Surg. 2011;35:941–950.
Groen RS, Samai M, Petroze RT, Kamara TB, Yambasu SE, Calland JF, Kingham TP, Guterbock TM, Choo B, Kushner AL. Pilot testing of a population-based surgical survey tool in Sierra Leone. World J Surg. 2012;36:771–774.
Groen RS, Samai M, Stewart KA, Cassidy LD, Kamara TB, Yambasu SE, Kingham TP, Kushner AL. Untreated surgical conditions in Sierra Leone: a cluster randomised, cross-sectional, countrywide survey. Lancet. 2012;380:1082–1087.
Hang HM, Byass P. Difficulties in getting treatment for injuries in rural Vietnam. Public Health. 2009;123:58–65.
Henderson RH, Sundaresan T. Cluster sampling to assess immunization coverage: a review of experience with a simplified sampling method. Bull World Health Organ. 1982;60:253–260.
Jamison DT, Summers LH, Alleyne G, Arrow KJ, Berkley S, Binagwaho A, Bustreo F, Evans D, Feachem RGA, Frenk J, Ghosh G, Goldie SJ, Guo Y, Gupta S, Horton R, Kruk ME, Mahmoud A, Mohohlo LK, Ncube M, Pablos-Mendez A, Reddy KS, Saxenian H, Soucat A, Ulltveit-Moe KH, Yamey G. Global health 2035: a world converging within a generation. Lancet. 2013;382:1898–1955.
Jayaraman S, Mabweijano JR, Lipnick MS, Caldwell N, Miyamoto J, Wangoda R, Mijumbi C, Hsia R, Dicker R, Ozgediz D. Current patterns of prehospital trauma care in Kampala, Uganda and the feasibility of a lay-first-responder training program. World J Surg. 2009;33:2512–2521.
Kirkhorn S, Greenlee RT, Reeser JC. The epidemiology of agriculture-related osteoarthritis and its impact on occupational disability. WMJ. 2003;102:38–44.
Kowalewski M, Mujinja P, Jahn A. Can mothers afford maternal health care costs? User costs of maternity services in rural Tanzania. Afr J Reprod Health. 2002;6:65–73.
Kushner AL, Kamara TB, Groen RS, Fadlu-Deen BD, Doah KS, Kingham TP. Improving access to surgery in a developing country: experience from a surgical collaboration in Sierra Leone. J Surg Educ. 2010;67:270–273.
Kushner AL, Kingham TP, Nwomeh BC. Medicine and surgery: the yin and yang of health systems. Lancet. 2012;379:1488.
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128.
Macharia WM, Njeru EK, Muli-Musiime F, Nantulya V. Severe road traffic injuries in Kenya, quality of care and access. Afr Health Sci. 2009;9:118–124.
McCord C, Chowdhury Q. A cost effective small hospital in Bangladesh: what it can mean for emergency obstetric care. Int J Gynaecol Obstet. 2003;81:83–92.
Mock C, Acheampong F, Adjei S, Koepsell T. The effect of recall on estimation of incidence rates for injury in Ghana. Int J Epidemiol. 1999;28:750–755.
Mock CN, nii-Amon-Kotei D, Maier RV. Low utilization of formal medical services by injured persons in a developing nation: health service data underestimate the importance of trauma. J Trauma. 1997;42:504–511; discussion 511–513.
Morshed S, Shearer DW, Coughlin RR. Collaborative partnerships and the future of global orthopaedics. Clin Orthop Relat Res. 2013;471:3088–3092.
Moshiro C, Heuch I, Astrøm AN, Setel P, Hemed Y, Kvåle G. Injury morbidity in an urban and a rural area in Tanzania: an epidemiological survey. BMC Public Health. 2005;5:11.
Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez M-G, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabé E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fèvre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FG, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gonzalez-Medina D, Gosselin R, Grainger R, Grant B, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Laden F, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Levinson D, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR, Mitchell PB, Mock C, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O’Donnell M, O’Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA 3rd, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leòn FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiebe N, Wiersma ST, Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh PH, Zaidi AK, Zheng Z-J, Zonies D, Lopez AD, Al Mazroa MA, Memish ZA. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223.
Omololu AB, Ogunlade SO, Gopaldasani VK. The practice of traditional bonesetting: training algorithm. Clin Orthop Relat Res. 2008;466:2392–2398.
Sekimpi P, Okike K, Zirkle L, Jawa A. Femoral fracture fixation in developing countries: an evaluation of the Surgical Implant Generation Network (SIGN) intramedullary nail. J Bone Joint Surg Am. 2011;93:1811–1818.
Smith E, Hoy DG, Cross M, Vos T, Naghavi M, Buchbinder R, Woolf AD, March L. The global burden of other musculoskeletal disorders: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73:1462–1469.
Statistics Sierra Leone, Ministry of Health and Sanitation, ICF Macro. Sierra Leone demographic and health survey 2008. Available at: http://dhsprogram.com/pubs/pdf/FR225/FR225.pdf. Accessed April 16, 2013.
Stewart KA, Groen RS, Kamara TB, Farahzad MM, Samai M, Cassidy LD, Kushner AL, Wren SM. Traumatic injuries in developing countries: report from a nationwide cross-sectional survey of Sierra Leone. JAMA Surg. 2013; 148:463–469.
Surgeons OverSeas. Surgeons OverSeas Assessment of Surgical Need (SOSAS) Version 3.0. Available at: http://www.surgeonsoverseas.org/resources.html. Accessed August 1, 2014.
The World Bank. Data, Sierra Leone. Available at: Available from: http://data.worldbank.org/country/sierra-leone. Accessed June 29, 2013.
Tollefson TT, Larrabee WF Jr. Global surgical initiatives to reduce the surgical burden of disease. JAMA. 2012;307:667–668.
UN Development Program. Human Development Reports. Sierra Leone. Available at: http://hdr.undp.org/en/countries/profiles/SLE. Accessed April 1, 2013.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basanez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabe E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196.
Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, Gawande AA. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–144.
Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646–656.
World Health Organization. Global Health Observatory, Sierra Leone, Health Profile. Available at: http://www.who.int/gho/countries/sle.pdf. Accessed April 1, 2013.
Acknowledgments
We thank the Sierra Leone Ministry of Health and Sanitation, Sierra Leone College of Medicine and Allied Health Sciences, and Connaught Hospital, who assisted with local transport and administrative issues. We thank personnel from Statistics Sierra Leone for sharing their expertise, the enumerators and field supervisors for their fine work ethic and enthusiasm, and Lucie Blok of the Royal Tropical Institute for a final look at the survey-questionnaire.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funding for logistics was provided by Surgeons OverSeas with a donation from the Thompson Family Foundation.
Ethical approval was obtained from the Ethics and Scientific Review Committee of Sierra Leone and the Research Ethics Committee of the Royal Tropical Institute in Amsterdam.
This study was performed in Sierra Leone in association with Connaught Hospital, Freetown, Sierra Leone.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Elliott, I.S., Groen, R.S., Kamara, T.B. et al. The Burden of Musculoskeletal Disease in Sierra Leone. Clin Orthop Relat Res 473, 380–389 (2015). https://doi.org/10.1007/s11999-014-4017-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-4017-8