
Abstract
Volar percutaneous cannulated screw fixation of acute scaphoid waist fractures reportedly produces high rates of healing and early return to work, but the method has not been reported for treating scaphoid waist delayed unions. We therefore report the surgical results of percutaneous screw fixation in scaphoid waist delayed union in 12 patients. All patients were male with an average age of 31.1 years. Duration of injury was 12 weeks (range, 6–20 weeks). However, no patient had carpal instability, scaphoid deformity, or avascular necrosis of the proximal fracture fragment. The minimal followup was 12 months (mean, 20 months; range, 12–24 months). Preoperative radiographs showed slight bone resorption at the fracture site in five patients and cyst formation in three patients. A cannulated screw was introduced volarly under image intensifier guidance in all patients. All fractures united uneventfully. At 12 month followups, the flexion and extension arcs of the injured wrist were 94% and 93% of the uninjured wrist. Grip strength averaged 34 ± 3 kg, which was 92% of the grip strength of the uninjured hand. The Mayo Modified Wrist Score was 94 ± 6 points and the Disabilities of the Arm, Shoulder, and Hand score was 9 ± 6 points. Our experience suggests volar percutaneous screw fixation is a reliable method to treat scaphoid waist delayed union.
Level of Evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Volar percutaneous cannulated screw fixation of acute scaphoid waist fractures has been used commonly by many authors, reportedly with uniformly high union rates approaching 100%, excellent functional results, rare complications, quicker time to union, and early return to manual work [1, 3, 9, 21]. However, the use of this modality for treatment of scaphoid waist delayed union has not been addressed.
Herbert and Fisher [10] devised an alphanumeric classification system of scaphoid fractures with possible prognostic importance by combining fracture location, stability, and chronicity of injury. They classified scaphoid fractures in terms of chronicity of injury as acute fracture, delayed union, and nonunion. According to this classification, delayed union includes fractures showing signs of delayed union after 6 or more weeks wearing a plaster cast and late fractures are defined as those presenting some weeks after injury. Although they made no conclusion concerning the cutoff between delayed union and nonunion, some authors suggest 6 months postinjury as a reasonable cutoff [12, 20, 23].
In patients with delayed union of scaphoid wrist fractures, we therefore documented (1) the rate of healing of fracture, (2) the functional outcomes, and (3) the complications.
Materials and Methods
We identified 15 patients with delayed scaphoid waist unions treated from October 2004 to April 2007, and meeting our inclusion criteria. Scaphoid waist delayed union included fractures with no sign of healing after 8 weeks wearing a plaster cast and late fractures presenting between 4 weeks to 6 months after injury. We excluded patients with a tuberosity fracture, proximal pole fracture, transscaphoid perilunar dislocation, humpback deformity of the scaphoid, dorsal intercalated segment instability (DISI) deformity, osteonecrosis of the proximal scaphoid fragment, or previous wrist injury. The risks and benefits of treatment were explained to all patients. Thirteen of the 15 agreed to participate and provided written consent. All of these patients were men; they were an average age of 31.1 years (range, 19–44 years). Seven patients had an injured right hand and five had an injured left hand. The mean duration of injury was 12 weeks (range, 6–20 weeks). The minimum followup was 12 months (mean, 20 months; range, 12–24 months). One of the 13 patients was lost before 1 year of followup. Thus, 12 patients with scaphoid waist delayed unions participated in this study (Table 1). The study was approved by our institutional review board.
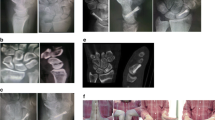
Scaphoid radiographs included the following views: posteroanterior, lateral, semipronation oblique, and semisupination oblique. Fracture location, displacement, lateral intrascaphoid angle, which is formed by lines perpendicular to the articular surface of the proximal and distal pole (Fig. 1) [26], and DISI were recorded. DISI [28] was considered present when the scapholunate angle was greater than 60° or the radiolunate angle was greater than 30°. Preoperative radiographs showed slight bone resorption at the fracture site in five patients (Fig. 1) and cyst formation in three patients (Fig. 2). The mean lateral intrascaphoid angle was 31° (range, 26°–35°). No patient had osteonecrosis of the proximal fracture fragment. Preoperatively, CT scans were performed to accurately measure lateral intrascaphoid angle and to better determine the viability of the proximal fracture fragment. Sections were made at 1.5-mm intervals and scout film was used to obtain proper longitudinal axis of the scaphoid.

(A) Slight bone resorption at the fracture site is a common finding in scaphoid waist delayed unions. (B) The lateral intrascaphoid angle (α) is 33°. (C) Healing was achieved 12 weeks after volar percutaneous screw insertion.

(A) Cyst formation at the fracture site sometimes is observed with scaphoid waist delayed unions. (B) Sagittal scaphoid alignment is not disturbed despite cystic bone resorption. (C) Bone union was achieved 14 weeks after surgery.
Surgery was performed with patients under general or regional anesthesia. Before starting surgery, we used a C-arm image intensifier to identify the scaphoid axis and determine the guide wire entry point. A towel roll was used under the supinated wrist to allow adequate wrist extension. A 1.1-mm guide wire of an Acutrak® screw (Acumed, Hillsboro, OR) then was introduced volarly. An image intensifier was used to confirm the wire was placed along the longitudinal axis of the scaphoid and across the fracture site. We determined screw length indirectly using a second guide wire. An antirotation wire then was placed parallel to the first guide wire such that it crossed the fracture site and was distanced from the initial guide wire to prevent interfering with drilling or screwing procedures. We then made a minimal incision around the initial guide wire to allow drill and screw passage. Blunt dissection around the guide wire was accomplished using a fine hemostat, and the scaphoid then was drilled for the prescribed distance along the guide pin. The 3.3-mm Acutrak® screw was placed, and the quality of the fracture reduction and screw position were determined under image intensifier guidance. We then removed the guide and antirotation wires and closed the wound with a nylon suture. Finally, a well-padded short-arm thumb spica plaster splint was applied.
Ten to 14 days after surgery, we removed the stitch and applied a short-arm thumb spica cast, which allowed free motion of the interphalangeal joint of the thumb. Four weeks postoperatively, casts were replaced by removable custom-fabricated thumb spica braces, which were worn for another month during work and recreation to avoid adventurous insults.
All patients were reevaluated at 2-week intervals after surgery until the fracture united. At each followup, the wrist was examined for snuffbox tenderness, and four radiographic views of the scaphoid (posteroanterior, lateral, semipronation oblique, and semisupination oblique) were taken. Union was considered to have occurred when there was no tenderness at the fracture site and there was evidence of trabeculae crossing it on at least three views [21]. CT scanning was done to confirm the union when union was considered.
Once union was documented, the patients revisited the clinic at 6 months, 1 year, and 2 years postoperatively. Clinical assessments were performed based on grip strength, range of motion (ROM) of the wrist, Mayo Modified Wrist Score (MMWS) [5], and Disabilities of the Arm, Shoulder, and Hand (DASH) score [11]. Grip strength was measured using a Jamar® dynamometer (Sammons Preston, Bolingbrook, IL) with elbows flexed at 90° and forearms in neutral rotation. ROM of the wrist (extension, flexion) was measured using a goniometer. These parameters were presented as percentages of the corresponding contralateral measurements. The MMWS is scored on a scale of 0 to 100, where 100 represents normal wrist function and is based on separate ratings of pain (25 points), ROM (25 points), grip strength (25 points), and functional status (25 points). The DASH questionnaire consists of 30 items, including 21 regarding the ability to perform specified activities and nine regarding symptoms. The DASH score ranges from 0 to 100 and a higher numeric score indicates greater disability.
One of the authors (SYL), who was not involved in surgical treatment, evaluated the radiographs for postoperative osteoarthritis and osteonecrosis. Osteoarthritis was graded as follows: (1) Stage I, affecting the radial styloid-scaphoid junction; (2) Stage II, affecting the entire radioscaphoid joint; (3) Stage III, affecting the entire radioscaphoid joint and capitolunate joint; and (4) Stage IV, affecting the radiocarpal and intercarpal joints [29]. Osteonecrosis was considered present when we observed increased absolute or relative density in the proximal pole of the scaphoid [26].
Results
All fractures united successfully with no additional procedures.
At the 12-month followup, the flexion arc of the injured wrist averaged 69° ± 3° versus 74° ± 2° for the uninjured wrist (94%), and the extension arc of the injured wrist averaged 67° ± 3° versus 71° ± 3° for the uninjured wrist (93%). Grip strength averaged 34 ± 3 kg, which was 92% of the grip strength of the uninjured hand (37 ± 2 kg). The mean MMWS was 94 ± 6 points and the mean DASH score was 9 ± 6 points (Table 2).
There were no perioperative complications. No patient showed stiffness of the fingers or thumb, nor did they experience complex regional pain syndrome. None of the patients showed radiographic signs of posttraumatic osteoarthritis or osteonecrosis of the scaphoid at the 12-month followup.
Discussion
Volar percutaneous cannulated screw fixation of acute scaphoid waist fractures uniformly produces high rates of union and early return to work [1, 3, 9, 21], and some authors have suggested delayed union may heal with rigid fixation alone without bone graft [7, 10, 18]. However, volar percutaneous screw fixation had not been addressed in scaphoid waist delayed unions. Therefore, in this study we used the volar percutaneous screw for treatment of scaphoid waist delayed unions to document healing of fractures, functional outcomes, and complications.
This study had several limitations. First, our study sample is small, as a scaphoid waist delayed union is relatively rare. Although only 12 cases were included in this study, we believe the study has meaning because consistent findings were observed in all cases. Second, there was no control group. However, the advantages of percutaneous screw fixation compared with open reduction with or without bone graft are theoretically clear as long as the union rates are compatible between two surgical methods. Numerous authors use surgical treatment in cases of scaphoid delayed union because times to union are much delayed and nonunion rates are quite high when scaphoid delayed unions are treated nonoperatively. Third, we did not assess the time to union. Although we took serial radiographs of all patients at 2-week intervals and confirmed union using CT when we judged union clinically and radiographically, judging early union is difficult and prone to interobserver variability. Therefore, we report the immobilization period rather than time to union, a clinically important parameter used in other studies [1, 21].
Several studies [6, 17, 20] that used cast immobilization for scaphoid delayed union had incidences of nonunion ranging from 19% to 88% and much longer immobilization periods (Table 3). Because the scaphoid resides intracapsularly, completely covered by cartilage, and possesses an odd undulating shape, it requires primary union for fracture healing. This form of union has strict requirements, including motionless contact between fragments. But some delay in detecting the fracture and slight fracture displacement or angulation can lead to delayed union. When nonoperative treatment is used on scaphoid delayed union, prolonged immobilization is necessary. However, prolonged immobilization temporarily, and sometimes permanently, disrupts hand function [14]. There is a need for rapid return to work in young male patients who are prone to scaphoid injury, which leads surgeons and patients to propose and accept surgical treatment.
When surgical treatment was considered for scaphoid waist delayed unions, surgeons have traditionally used internal fixation and bone graft, and 91% to 100% of their patients achieved union [8, 12, 15, 19]. However, some have used screw fixation alone, ie, without bone graft, for scaphoid delayed unions and bony union was achieved by 91% to 100% of their patients [7, 10, 18]. Subsequently it seemed reasonable to presume delayed unions might heal with rigid fixation alone. Through the development of the headless cannulated compression screw, strong fixation of the scaphoid can be achieved by the percutaneous approach. Moreover, preparative reaming of the scaphoid for a screw provides an opportunity to establish a bleeding bone surface [25]. By fixing the scaphoid waist delayed union using headless cannulated compression screw alone, all fractures successfully united.
Advantages of percutaneous fixation are minimal disturbance of local biology, minimal skin scarring, and reduced risk of osteonecrosis [13]. Since the first reported surgical technique for percutaneous screw fixation for an acute scaphoid fracture, the majority of patients have been operated on via the volar approach with successful outcomes [13]. The volar approach has several advantages. It is technically less demanding and simplifies guide wire insertion and placement because the guide wire does not cross the radiocarpal joint during fluoroscopic evaluation [4, 13]. The wrist extension, which is the wrist position during the volar approach, makes the scaphoid fracture stable and there is no risk of injuring the extensor tendon. However, the advantages of the dorsal approach are exact targeting of the central axis of the scaphoid and avoiding injury to the trapezioscaphoid joint [4, 13]. Central placement of the percutaneous screw is considered an important factor for successful healing of scaphoid fractures [27], and there is no difference in central placement of the screw between the volar and dorsal approaches when it is used in the proximal or waist region of the scaphoid [4]. A recent comparative study reported no difference in functional outcome and bone union between the volar and the dorsal approaches in acute B2 scaphoid fractures [13].
We believe selection of the candidate in whom to use volar percutaneous screw fixation is important when treating scaphoid waist delayed unions. We excluded patients with humpback deformity of the scaphoid, DISI deformity, and osteonecrosis of the proximal scaphoid fragment. Humpback deformity of the scaphoid can be detected by measuring the lateral intrascaphoid angle on sagittal CT scans [28]. The lateral intrascaphoid angle is less than 35° in patients with a normal scaphoid, and an angle of greater than 45° is believed to promote pain, stiffness, and posttraumatic arthritis [2, 16, 26]. A scapholunate angle greater than 60° or a radiolunate angle greater than 30° on plain radiographs indicates a DISI deformity. If a DISI deformity is present, it can be difficult to correct alignment of the scaphoid and the normal scaphoid-lunate relationship [28]. To correct these deformities, we believe some kinds of wedge bone graft should be applied by open procedure. Although MRI scans are considered the gold standard to detect osteonecrosis of the proximal scaphoid fragment, a recently published report indicated preoperative longitudinal CT scanning is also valuable for identifying osteonecrosis [26]. Vascularized bone grafting should be considered in patients with osteonecrosis of the proximal scaphoid fragment.
Slade et al. [25] reported good results for Acutrak® screw fixation in cases of scaphoid fibrous union or nonunion with minimal sclerosis through the dorsal percutaneous approach and suggested the times to union are substantially less in fractures treated within 6 months of injury than in fractures treated greater than 6 months after injury. However, they proposed percutaneous bone grafts to treat scaphoid nonunions with bone resorption or cyst formation [24]. Bone resorption or cyst formation at the fracture site often is observed in scaphoid delayed unions [8, 18, 22]. In our series, eight of 12 patients had slight bone resorption or cyst formation. Nevertheless, all achieved healing using volar percutaneous screw fixation alone. Therefore, results of our study indicate the presence of bone resorption or cyst formation at the scaphoid fracture site is not a contraindication of percutaneous screw fixation alone in scaphoid waist delayed union as long as it is not so severe as to disturb the scaphoid or the carpal alignment.
We found volar percutaneous screw fixation was a reliable method for patients to achieve bony union with high functional scores and without major complications, provided it was used in scaphoid waist delayed union without scaphoid or carpal malalignment.
References
Adolfsson L, Lindau T, Arner M. Acutrak screw fixation versus cast immobilisation for undisplaced scaphoid waist fractures. J Hand Surg Br. 2001;26:192–195.
Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP 3rd, Linscheid RL. Scaphoid malunion. J Hand Surg Am. 1989;14:679–687.
Bond CD, Shin AY, McBride MT, Dao KD. Percutaneous screw fixation or cast immobilization for nondisplaced scaphoid fractures. J Bone Joint Surg Am. 2001;83:483–488.
Chan KW, McAdams TR. Central screw placement in percutaneous screw scaphoid fixation: a cadaveric comparison of proximal and distal techniques. J Hand Surg Am. 2004;29:74–79.
Cooney WP, Linscheid RL, Dobyns JH. Triangular fibrocartilage tears. J Hand Surg Am. 1994;19:143–154.
Eddeland A, Eiken O, Hellgren E, Ohlsson NM. Fractures of the scaphoid. Scand J Plast Reconstr Surg. 1975;9:234–239.
Gasser H. Delayed union and pseudarthrosis of the carpal navicular: treatment by compression-screw osteosynthesis; a preliminary report on twenty fractures. J Bone Joint Surg Am. 1965;47:249–266.
Gupta A, Risitano G, Crawford RJ, Burke FD. The ununited scaphoid: prognostic factors in delayed and nonunions of the scaphoid. Hand Surg. 1999;4:11–19.
Haddad FS, Goddard NJ. Acute percutaneous scaphoid fixation: a pilot study. J Bone Joint Surg Br. 1998;80:95–99.
Herbert TJ, Fisher WE. Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br. 1984;66:114–123.
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29:602–608.
Inaparthy PK, Nicholl JE. Treatment of delayed/nonunion of scaphoid waist with Synthes cannulated scaphoid screw and bone graft. Hand (N Y). 2008;3:292–296.
Jeon IH, Kochhar H, Lee BW, Kim SY, Kim PT. Percutaneous screw fixation for scaphoid nonunion in skeletally immature patients: a report of two cases. J Hand Surg Am. 2008;33:656–659.
Karantana A, Downs-Wheeler MJ, Webb K, Pearce CA, Johnson A, Bannister GC. The effects of scaphoid and Colles casts on hand function. J Hand Surg Br. 2006;31:436–438.
Korkala OL, Antti-Poika IU. Late treatment of scaphoid fractures by bone grafting and compression staple osteosynthesis. J Hand Surg Am. 1989;14:491–495.
Kozin SH. Incidence, mechanism, and natural history of scaphoid fractures. Hand Clin. 2001;17:515–524.
Langhoff O, Andersen JL. Consequences of late immobilization of scaphoid fractures. J Hand Surg Br. 1988;13:77–79.
Leyshon A, Ireland J, Trickey EL. The treatment of delayed union and non-union of the carpal scaphoid by screw fixation. J Bone Joint Surg Br. 1984;66:124–127.
Little CP, Burston BJ, Hopkinson-Woolley J, Burge P. Failure of surgery for scaphoid non-union is associated with smoking. J Hand Surg Br. 2006;31:252–255.
Mack GR, Wilckens JH, McPherson SA. Subacute scaphoid fractures: a closer look at closed treatment. Am J Sports Med. 1998;26:56–58.
McQueen MM, Gelbke MK, Wakefield A, Will EM, Gaebler C. Percutaneous screw fixation versus conservative treatment for fractures of the waist of the scaphoid: a prospective randomised study. J Bone Joint Surg Br. 2008;90:66–71.
Rennie WJ, Finlay DB. Posttraumatic cystlike defects of the scaphoid: late sign of occult microfracture and useful indicator of delayed union. AJR Am J Roentgenol. 2003;180:655–658.
Simonian PT, Trumble TE. Scaphoid nonunion. J Am Acad Orthop Surg. 1994;2:185–191.
Slade JF 3rd, Dodds SD. Minimally invasive management of scaphoid nonunions. Clin Orthop Relat Res. 2006;445:108–119.
Slade JF 3rd, Geissler WB, Gutow AP, Merrell GA. Percutaneous internal fixation of selected scaphoid nonunions with an arthroscopically assisted dorsal approach. J Bone Joint Surg Am. 2003;85(suppl 4):20–32.
Smith ML, Bain GI, Chabrel N, Turner P, Carter C, Field J. Using computed tomography to assist with diagnosis of avascular necrosis complicating chronic scaphoid nonunion. J Hand Surg Am. 2009 May 14. [Epub ahead of print].
Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid: treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am. 1996;78:1829–1837.
Trumble TE, Salas P, Barthel T, Robert KQ 3rd. Management of scaphoid nonunions. J Am Acad Orthop Surg. 2003;11:380–391.
Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007;32:725–746.
Acknowledgments
We thank Ji Young Hwang, MD, Department of Diagnostic Radiology, for help and advice in analysis of radiographic images.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he has no commercial association (eg, consultancies, stock ownership, equity interest, patent/licensing arrangement, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved the reporting of these cases, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participating in the study was obtained.
This work was performed at Department of Orthopedic Surgery, Medical Research Institute, School of Medicine, Ewha Womans University.
About this article
Cite this article
Kim, J.K., Kim, J.O. & Lee, S.Y. Volar Percutaneous Screw Fixation for Scaphoid Waist Delayed Union. Clin Orthop Relat Res 468, 1066–1071 (2010). https://doi.org/10.1007/s11999-009-1032-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-009-1032-2