
Abstract
Purpose of Review
The purpose of this review is to present an overview of common sleep disturbance pathologies and their impact on chronic pain, while examining various factors that are implicit in the relationship between sleep disturbance and chronic pain, including neurobiochemistry, anatomy, and systemic mediators, and reviewing recent and landmark literature.
Recent Findings
Earlier literature reviews and studies have introduced the bidirectional relationship between sleep disturbance and chronic pain; that is, impaired sleep may worsen chronic pain, and chronic pain causes sleep disturbance. However, more recent reviews and studies seem to show a more associative, rather than causative relationship. There have been recent studies that attempt to determine mechanisms that link sleep disturbance and chronic pain; the results of these studies were more varied, ultimately concluding that there may be a separate, yet-to-be discovered mechanism that shows the causative relationship between sleep disturbance and pain.
Summary
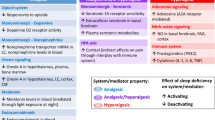
There are several neurotransmitters that are involved in the mediation of chronic pain and sleep disturbance as separate entities, and some studies have shown that there may be mechanisms that govern both chronic pain and sleep disturbance as a single unit. Other neuroendocrine substances also serve to mediate chronic pain and sleep disturbance. All these substances are found to be associated with various sleep disorders and are also associated with chronic pain symptoms as well. Inflammation plays a role in chronic pain and sleep disturbance, with an increase in inflammatory substances and mediators associated with an increase or worsening in chronic pain symptoms and sleep disorders. The HPA axis plays a role in chronic pain and sleep disorders, influencing pain and sleep pathways through stress response, inflammation, and maintenance of homeostasis. There are several variables that influence both chronic pain and sleep disturbance, and more research into these variables may further our understanding into the complex pathways governing the influence of sleep disturbance on pain, and ultimately to improve treatment for this issue.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sleep in humans is governed by complex physiological processes, and sleep itself plays a significant role in a person’s physical and mental health [1]. The prevalence of sleep disorders, such as obstructive sleep apnea (OSA), rapid eye movement (REM) sleep behavior disorder, and narcolepsy, has appeared to be increasing in recent years [2]. Still other sleep disorders, such as narcolepsy, have been noted to persist through several years [3].
Pain is defined as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [4]. Chronic pain has been newly redefined into two categories, chronic primary pain and chronic secondary pain. Chronic primary pain is defined as a pain that is anatomical in nature which persists or recurs for more than 3 months, and that this pain is associated with emotional and/or functional disability, and that the pain cannot be better explained by another pain condition. Chronic secondary primary pain is a pain that is secondary to another disease process, such as cancer, post-trauma, or neuropathy [5].
The relationship between sleep disturbance and chronic pain has been commonly regarded as bidirectional, as poor sleep can influence pain, and pain can worsen sleep [6•]. However, several recent studies have showed conflicting results on the effect of pain on sleep and vice versa [7]. In patients with chronic pain, a range of 50% to 90% reported sleep disturbance, with symptoms of insomnia reported as the most common [8•]. There have been several reviews and studies exploring the effect of sleep on several mediators of pain, including neurobiology, inflammation, endocrine systems, and psychiatric influences [8•, 9, 10•]. Other studies and reviews have attempted to identify individual sleep disturbance pathologies, behavioral characteristics, and effects of pharmacological agents on the relationship of sleep disturbance and chronic pain [11].
The aim of this review is to present several sleep disturbance pathologies and their role in chronic pain, neurochemical mechanisms and their interaction with chronic pain and sleep, systemic regulation of chronic pain and sleep, and anatomical considerations related to pain, sleep, and stress, all while presenting an overview of relevant studies and literature.
Physiology and Function of Sleep
Sleep is divided into two phases, rapid eye movement (REM) sleep and non-rapid eye movement (NREM) sleep [1]. Electroencephalography (EEG) can be used to identify specific subdivisions of sleep; for example, the N1, N2, and N3 (slow-wave sleep) phases comprise NREM sleep [1]. NREM sleep is typically associated with decreased brain activity, and while dreaming can be present in all phases of sleep, vivid dreaming is not usually a part of NREM [10•]. Dreaming during the NREM phase is thought to be more of a nonvisual thought process [10•, 12]. In addition to decreased brain activity, NREM sleep is associated with decreased sympathetic activity, including lower heart rate and blood pressure [10•, 13]. The delta waveform seen on EEG most commonly characterizes NREM sleep [14]. Delta waveforms on EEG seem to indicate restorative sleep, and as sleep continues, delta waveforms gradually decline [14]. Delta wave forms range from 1 to 4 Hz in frequency, and seem to correlate with brain activity in thalamo-cortical areas [13]. Slow oscillation waveforms, with a frequency of less than 1 Hz, are also found during the NREM phase, and correlate with intra-cortical brain activity [13]. Although it is known that sleep promotes brain and body restoration, the exact process of restoration is unknown [13]. However, the presence of slow oscillation waveforms seen on EEG has been studied extensively in the past, and these waveforms have been associated with synaptic pruning, memory consolidation, and mediation of neuroplasticity, which may represent neuro-restoration in the brain [13].
REM sleep is associated with vivid dreaming and higher levels of brain activity in comparison to NREM sleep [12]. There is a suppression of muscle tone during REM sleep, and rapid eye movement is characteristic of the REM phase [13]. Other physiological features include variability in body and brain temperature, respiration, blood pressure, and heart rate [10•, 15]. A study measuring sympathetic in the peroneal nerve at the level of the knee showed increasing activity during REM sleep, and nearly no activity during NREM sleep [13]. The first instance of REM sleep occurs after 70 to 90 min after the onset of sleep and, afterwards, will occur every 90 to 120 min [15, 16]. Waveforms seen on EEG during REM sleep are low amplitude and high frequency, and are similar to theta waves seen in the hippocampus during awake periods [15]. During sleep, hippocampal activity may be involved in memory formation and consolidation; a 2016 study showed that the selective silencing of GABA neurons found in the hippocampus decreased theta waveform activity, leading to impaired memory consolidation [15]. In addition to memory, a recent study in 2017 demonstrated pruning and maintenance of new neuronal synapses, showing that REM sleep may contribute to motor learning [15]. Although muscle activity is nearly silenced during REM sleep, occasional muscle twitches have been noted during this phase [15]. The functions of these muscle twitches are generally unknown, but recent studies have shown that these twitches may contribute to sensorimotor system development [15]. Additionally, REM sleep serves to promote cortical plasticity, increase creativity, and restore cellular and receptor functioning in cells utilizing aminergic molecules (e.g., dopamine, serotonin, and acetylcholine), and preparing the transition from sleep to wakefulness [15].
Chronic Pain
In 2020, the International Association for the Study of Pain (IASP) published a revised definition for pain [4]. The reasoning for this was due to a better understanding and advancement in the study of pain, especially given that pain can have a multifactorial etiology [4]. The revised definition of pain is now “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [4]. The definition of chronic pain has also been recently revised in 2019, with the term chronic pain divided into chronic primary pain and chronic secondary pain [5]. According to the IASP, chronic primary pain is a pain that is primarily a disease, whereas chronic secondary pain is a symptom of another disease [5]. Chronic primary pain encompasses chronic widespread pain (CWP), complex regional pain syndrome (CRPS), chronic primary headache and orofacial pain, chronic primary visceral pain, and chronic primary musculoskeletal pain [5]. Chronic secondary pain syndromes include chronic cancer-related pain, chronic postsurgical and posttraumatic pain, chronic neuropathic pain, chronic secondary headache and orofacial pain, chronic secondary visceral pain, and chronic secondary musculoskeletal pain [5]. The IASP states that the diagnosis of chronic primary or secondary pain may be difficult [5]. Chronic pain is diagnosed when the duration exceeds beyond 3 to 6 months of healing [10•].
The Institute of Medicine (IOM) estimates that chronic pain has impacted at least 116 million adults in the USA in a 2011 report [17]. The prevalence of pain is expected to increase, according to the IOM, due to five reasons: an aging US population, increasing prevalence of obesity and its chronic comorbidities, improved medical care for people with injuries who would have otherwise died, post-surgical changes, and greater understanding of chronic pain syndromes causing people to seek care for their pain [17]. Worldwide, chronic pain may affect nearly 20% of people [10•]. The IOM estimates that $635 billion is spent on healthcare costs related to chronic pain [17].
Sleep Disorders and Chronic Pain
The International Classification of Sleep Disorders (ICSD) defines seven categories of sleep disorders, including insomnia, sleep-related breathing disorders, central disorders of hypersomnolence, circadian rhythm sleep–wake disorders, parasomnias, sleep-related movement disorders, and other sleep disorders [18]. In the USA, about 31% of adults 18 years and over get insufficient sleep [19]. This insufficient sleep duration is defined as less than 7 h of sleep during a 24-h period [20].
A common sleep disorder is insomnia, with general consensus estimating nearly 30% of adults reporting one or more symptoms of insomnia [21]. Insomnia is further categorized into short-term, chronic, and other (does not meet criteria for the other two types of insomnia) [18]. In general, insomnia is defined as a difficulty with falling asleep, staying asleep, and impairment of daytime function [21]. Insomnia has been reported to persist as far as 20 years, with persistence rates estimated to range from 40 to 69% in patient follow-up [22]. Women are more affected by insomnia than are men, and the elderly more affected than the younger [22].
In an investigation to determine the association between sleeping problems and development of neck, shoulder, and lumbar pain, results seem to suggest that symptoms of insomnia were associated with the development of musculoskeletal pain over a 12-month period [23]. This study also reports that one in 15 to 20 cases of newly diagnosed chronic pain can be attributed to poor sleep quality [23]. In another study estimating the prevalence of insomnia in chronic pain patients, the researchers found that slightly more than half of chronic pain patients were found to have symptoms associated with insomnia, as scored by questionnaires measuring sleep [24]. The data also showed that insomnia severity was significantly positively correlated with pain intensity, sensory pain ratings, and affective pain ratings [24]. Affective pain, defined as the emotional aspect of pain, was found to be a significant predictor of insomnia severity [24]. In early studies to establish the directionality of relationship between chronic pain and insomnia, sleep deprivation was found to be associated with muscular tenderness and increased hyperalgesia to heat, cold, and blunt pressure, in addition to increased pain sensitivity to pinprick [22]. An earlier review of the directionality between chronic pain and insomnia noted that in one study, restorative sleep was associated with resolution of chronic widespread pain [25]. In a 2017 study of chronic pain and insomnia, insomnia was found to be a significant predictor of chronic pain incidence over 6 years [21].
Obstructive sleep apnea (OSA) is defined as obstructive apnea or hypopnea of the upper airway with arousal during sleep [7]. Patients report symptoms such as poor sleep that is not restorative, snoring, daytime sleepiness, and morning headaches [7, 26]. OSA is more common in males, in African Americans, older ages, obesity, and people with craniofacial or upper airway abnormalities [27,28,29,30,31]. There have been several studies documenting the relationship between chronic pain syndromes and OSA, including chronic craniofacial pain, pain related to psoriasis, fibromyalgia, and chronic widespread pain [32,33,34,35].
A 2017 study on the relationship between OSA and fibromyalgia found that as much as 50% of patients with fibromyalgia were found to have OSA [34]. In this study, the authors found a negative correlation between fibromyalgia and mean oxygen saturation during sleep and a positive correlation with desaturation time (defined as the period of time when oxygen saturation is below 90%) [34]. Although this study showed features linking OSA and fibromyalgia, this study was flawed as it did not evaluate treatment of OSA and its relationship with fibromyalgia, and subsequent studies on the relationship between OSA and fibromyalgia would stand to benefit from the inclusion of treatment strategies for both OSA and fibromyalgia [35]. Temporomandibular joint disorders (TMD) have been found to be associated with OSA, and OSA symptoms have been found to predict the incidence of initial TMD and chronic TMD. In this review, patients suffering from TMD did not awaken from sleep, but did report increased muscle tenderness upon awakening. A further subset of TMD patients with myofascial pain syndrome had significantly poorer sleep than patients only with TMD [32]. Another longitudinal study reported OSA symptoms were precedent to and predictive of the development of pain secondary to chronic TMD [36]. This study also proposes that chronic pain may occur via central sensitization and pain amplification through baroreceptor pathways [36]. An earlier experiment has shown that increased inspiratory resistance reduces baroreceptor reflexes, which has been implicated in TMD [37]. In a 2013 study of nocturnal intermittent hypoxia and its relationship with pain, the authors found that low arterial oxygen saturation nearly double the odds of developing pain, ultimately concluding that nocturnal hypoxemia may be a risk factor for pain [38•]. This study hypothesized that sleep-related pain may be secondary to hypoxia via systemic inflammation and oxidative stress [38•].
Narcolepsy is a sleep disorder characterized by daytime sleepiness, and may feature cataplexy (muscle weakness secondary to strong emotions), hypnagogic (prior to sleep onset) and hypnopompic (after awakening) visual hallucinations, and REM sleep dysfunction [18, 39, 40]. Narcolepsy has two types, with type 1 featuring cataplexy and type 2 without cataplexy [41].
In a 2018 study of narcolepsy and its association with chronic pain, researchers found that patients with both type 1 and type 2 narcolepsy had a higher frequency of chronic pain in comparison to control subjects [41]. In addition, while previous studies have showed that patients with type 1 narcolepsy had a higher frequency of chronic pain that those with type 2 narcolepsy, this study was the first to show increased frequency of type 2 narcolepsy patients with chronic pain [41]. In a separate study, researchers found that chronic low back pain was comorbid with narcolepsy [42]. Other studies regarding pain and narcolepsy have reported the development of headache disorders and other pain conditions in patients with narcolepsy, but failed to definitely conclude the bidirectional relationship between narcolepsy and chronic pain; that is, whether pain was an association of narcolepsy, or if narcolepsy caused the pain itself [43, 44]. Therefore, future studies should establish a treatment protocol to determine causation of narcolepsy on pain.
Neurobiology of Pain and Sleep
There have been several studies in determining neurological mechanisms between the interaction of sleep and pain, including the study of neurotransmitters and other endogenous substances, neuroanatomy, and inflammation [8•, 45•, 46]. Several neurotransmitters such as dopamine, serotonin, and norepinephrine have played roles in sleep and chronic pain pathways [8•, 10•]. Endogenous substances, including melatonin, vitamin D, and orexin also play a role in the interaction between sleep and pain [10•]. It is known that inflammation mediates pain, and a focus on a variety of substances related to inflammation, including pro-inflammatory cytokines and free radicals, have been studied to understand the role of inflammation on sleep and chronic pain [47,48,49]. Finally, specific areas of the brain have been identified to potentially link sleep disturbance and chronic pain, such as alterations of the hypothalamic–pituitary–adrenal axis, thalamus, and cortical areas [8•, 10•, 11, 50].
Dopamine is a neurotransmitter with a variety of functions in humans, playing roles in reward pathways, movement, psychiatric disease, hemodynamics, and also pain [51, 52]. Dopamine is also known to participate in sleep, with dopaminergic pathways located in the ventral tegmental area and nucleus accumbens implicated in sleep and wake regulation in recent studies [53]. Increased dopamine is associated with an awake state, and lower dopamine levels are associated with a sleep state [10•]. A 2016 study has shown that dopaminergic neurons were responsible for releasing dopamine after physical pain was experienced, and it has been hypothesized that chronic pain leads to decreased dopamine levels, which can lead to an impaired dopaminergic pathway in the mesolimbic reward system [54]. In sleep research, decreased dopamine receptor activity has been associated with acute sleep deprivation in animal models [55]. A 2013 review showed dopamine is associated with symptoms of insomnia and chronic pain, specifically with dysfunction in mesolimbic dopaminergic systems [56]. Additionally, further research has hypothesized that pain-mediated dopamine signaling in the raphe nucleus of the brainstem may play a role in regulating sleep and wake [46, 57].
Serotonin, also known as 5-hydroxytryptamine (5-HT), may play a role in the relationship between chronic pain and insomnia [8•]. There has been thorough research on serotonin and its interaction with chronic pain, and there is belief that serotonin mediates pain through specific peripheral and central receptors [58•]. In some animal models, administration of serotonin in peripheral areas resulted in increased excitability of cell membranes of nociceptive nerve fibers, while serotonergic agonists injected intradermally produced hyperalgesia, indicating that serotonin receptor activation may play a role in mediating pain [59, 60]. Later studies with serotonin receptor antagonists have also showed an attenuation in pain response in animal models, and in human studies, serotonin injected peripherally caused pain, with attenuation of pain serotonin-induced hyperalgesia when serotonin receptor antagonists were injected [61, 62]. In a study on pain secondary to peripheral nerve injury, there was found to be lower levels of serotonin in the brainstem, increased expression of serotonin receptors in the brainstem. After low-intensity exercise, brainstem serotonin levels were found to be increased, as well as increased serotonin receptor expression, which produced an attenuation in pain [63]. Other earlier studies have found that the spinal release of serotonin induced analgesia [58•]. While serotonin receptor agonists may have promising potential in treating chronic migraines, the mechanism of serotonin in mediating chronic pain has yet to be fully elucidated [58•, 64]. In sleep, serotonin is involved in the preparation and maintenance of sleep [65]. In another study, one night of total sleep deprivation was associated with a significant increase in serotonin receptor binding in various cortical regions of the brain, showing an important role of serotonin in sleep regulation [66]. While serotonin plays individual roles in both sleep–wake regulation and pain mediation, there have been no studies formally linking serotonin changes as a causal, rather than associative, relationship with pain and sleep.
Norepinephrine is a catecholamine neurotransmitter that is responsible for bodily functions, including maintenance of hemodynamics, sleep, arousal, and more recently, effects on pain [67]. In recent studies on animal models, the inhibition of norepinephrine reuptake in the spinal cord has been seen to directly inhibit neuropathic pain through alpha-2 receptor activation [67]. Selective serotonin and norepinephrine reuptake inhibitors (SNRIs) have been used for the treatment of chronic pain, and both these neurotransmitters play a role in descending pain pathways [68]. In animal models for sleep research, the reduction of norepinephrine activity in the locus coeruleus seems to mediate unresponsiveness during sleep, and increased activity results in awakening [69]. In humans, plasma levels of norepinephrine are higher during an awake state and lower during sleep [70]. Several studies have showed that sleep deprivation in both animals and humans have resulted in higher levels of circulating norepinephrine [71, 72]. There have been minimal studies relating the effect of norepinephrine on sleep disturbance and chronic pain, and it is difficult to establish a conclusion for the directionality of chronic pain and sleep. In an animal model examining the role of norepinephrine in pain and sleep, results suggested that experimentally induced neuropathic pain increased norepinephrine release stimulated by neurons in the locus coeruleus, leading to a decrease in NREM sleep and increased wakefulness [73]. However, this study did not establish the reverse relationship; that is, an increase in sleep deprivation worsening pain. In addition, given the previous knowledge of the analgesic effect of norepinephrine in the brainstem, the findings of the previous study call for further research into the effect of increased norepinephrine secondary to sleep disturbance and pain.
Melatonin is a hormone that is secreted by the pineal gland and is involved in sleep regulation, with increased secretion levels in the dark and decreased levels with light exposure [74]. Melatonin has been also studied for analgesic purposes in acute and chronic pain environments; however, research has been inconclusive in the acute and chronic pain settings [74, 75]. While it is still too early to definitely identify melatonin as an analgesic agent, there have been studies showing melatonin’s effect on inflammatory, analgesic, anxiolytic mechanisms [6•, 10•, 74]. Melatonin acts on the MT1 and MT2 receptors in the thalamus, hypothalamus, dorsal horns of the spinal cord, spinal trigeminal tract, and trigeminal nerve nucleus to mediate its analgesic effect [75]. In animal studies on neuropathic pain, MT2 receptor agonists were seen to mediate analgesic effect through a descending nociceptive pathway in the brainstem [75, 76]. The mechanism of melatonin and analgesia has not been fully identified, but several studies have reported mechanisms via GABA receptors, opioid receptors, and possible anti-inflammatory pathways [77, 78, 79•]. Melatonin is well known for its regulation of sleep, and low melatonin production during the night has been associated with insomnia in older patients [80]. The administration of melatonin in sleep disorders, such as insomnia, has been widely studied, and in a meta-analysis of melatonin studies, it was seen to significantly improve sleep in primary sleep disorders in comparison to placebo [81]. It has been reported that melatonin administration in chronic pain patients improved the quality of sleep, and conversely, in a separate review, melatonin maintained the quality of sleep, leading to decreased pain levels [77, 82•].
Vitamin D can be generated from exposure to sunlight (specifically, ultraviolet B radiation) or obtained from dietary sources, and deficiency of vitamin D can lead to musculoskeletal, neurological, autoimmune, and infectious pathologies, and more recently, sleep–wake regulation and pain [83•]. A few studies evaluating the role of vitamin D in chronic pain demonstrated that a deficiency in vitamin D was associated with patients with chronic musculoskeletal pain [84, 85]. Another study looking into pain and poor sleep showed that in patients with chronic musculoskeletal pain and sleep disorders, vitamin D deficiency was prevalent [86]. Patients in this study were found to have chronic pain symptoms incidentally, and the authors concluded that chronic musculoskeletal pain may be a symptom of a vitamin D deficiency [86]. In a separate study analyzing the effects of vitamin D administration to patients with chronic pain and vitamin D deficiency, patient’s pain levels were reported to be significantly decreased, the amount of pain medication use overall decreased, and overall sleep was improved [87]. The mechanism of vitamin D has been thought to be related to its anti-inflammatory effects as a neuroactive steroid, upregulation of endogenous substances to provide a neuroprotective function, inhibiting prostaglandin action thus attenuating neuropathic pain, inhibition of nitric oxide production decreasing pain central sensitization, and downregulation of some immune cells to decrease inflammatory mediators [88,89,90,91,92,93,94,95,96]. In a study analyzing the effect of vitamin D and day time sleepiness in patients who reported chronic pain disrupting their sleep, the authors posited that vitamin D deficiency could contribute to sleepiness via inflammatory mediators including TNF-alpha and NF-kappa-B, of which the latter is associated with OSA [97]. In addition, the authors report that a vitamin D deficiency is correlated with factors that increase the risk of OSA, including chronic rhinitis, tonsillar hypertrophy, and nonspecific myopathy [97].
Orexin, also known as hypocretin, is an endogenous neuropeptide that is primarily secreted by neurons in the hypothalamus [98, 99]. Orexin plays a role in mediating the awake-sleep cycle, and orexinergic neurons are found to be activated during awake periods and inhibited during sleep [100]. There are two types of orexin receptors, both of which are involved in regulating the sleep–wake cycle, and two types of orexin compounds, orexin-1 and orexin-2, of which orexin-1 seems to be a more potent effector of analgesia [10•, 100]. Orexinergic neurons interact with the brainstem to regulate the sleep–wake cycle [100]. Orexin deficiency is closely associated with narcolepsy, and the number of nerve fibers that contain orexin receptors is significantly decreased in patients with narcolepsy [99]. In a study determining the relationship between pain and narcolepsy, pain was found to be more intense and more frequent in patients with narcolepsy in comparison to the control group [101]. In a study to analyze the mechanism of orexin-mediated analgesia, orexin was found to activate orexin-1 receptors in the periaqueductal gray and produce analgesia through an endocannabinoid pathway disinhibiting the output of the periaqueductal gray [102].
Inflammation and inflammatory molecules are well-known and widely studied as a mediator of chronic pain, and more recent studies have linked sleep disturbance with an increase in inflammatory substances [103,104,105,106,107]. A recent review has shown that sleep disturbance, but not short sleep duration, was associated with increased inflammatory markers [108]. A study performed on healthy volunteers to analyze the effects of sleep deprivation and markers of inflammation found that levels of interleukin-6 (IL-6), a proinflammatory cytokine, serum C-reactive protein, and urinary prostaglandin metabolites were increased after sleep deprivation [109]. This study suggested that sleep disturbance may mediate chronic pain via inflammatory pathways [109]. Inflammatory substances have demonstrated an ability to activate central nervous system glial cells, which themselves release proinflammatory cytokines [110]. This overall increases pain responsivity, which is hypothesized to result in chronic pain [110]. Other studies on sleep disorders and inflammation have shown that a pro-inflammatory cytokine, tumor necrosis factor alpha (TNF-alpha), and IL-6 were increased in OSA [111]. In a recent systematic review to determine the relationship between OSA and pain, while OSA was associated with increased pain intensity or a decreased tolerance to pain, results were variable due to patient characteristics and OSA phenotype (nocturnal hypoxemia or sleep fragmentation). The review also demonstrated an improvement in chronic pain with the use of CPAP [112•]. In a recent study on patients with insomnia, IL-6 levels were found to decrease with improvements in insomnia symptoms, and overall the study suggested that inflammatory pathways were related to symptoms of insomnia and chronic pain [113•].
The hypothalamic–pituitary–adrenal (HPA) axis plays a major role in stress response, as well as regulation of the circadian and immunological systems, and overall homeostasis [114,115,116]. It is known that sleep causes a decrease in cortisol, a glucocorticoid hormone that acts as a signaling molecule to allow the body to adapt to a variety of stressors [114, 117]. Subsequently, the administration of glucocorticoids has been studied extensively, generally causing sleep disturbance [118]. A recent review has shown that possible mechanisms into glucocorticoid-induced sleep disturbance occur via glucocorticoid receptors in the dorsal raphe with serotonin depletion in the suprachiasmatic nucleus, and decrease in neurotransmitter activity in the suprachiasmatic nucleus from the effect of glucocorticoids on various organs [119•]. Corticotropin-releasing hormone (CRH) is made in the paraventricular nucleus of the hypothalamus, and serves to regulate the HPA axis [118]. Adrenocorticotropic hormone (ACTH) is a hormone secreted by the anterior pituitary in response to stimulation from CRH, which subsequently leads to the secretion of glucocorticoids in the adrenal cortex [116]. In a recent study, short-term severe sleep restriction was found to be associated with altered function of the HPA axis, increased spontaneous activity, and decreased response and recovery to external stress. The authors propose that the irregular HPA function may contribute to the effect of sleep disturbance on conditions such as obesity, diabetes, infection, and psychiatric pathologies [120]. Disrupted HPA function has been found in patients with OSA, with increased secretion duration of ACTH and cortisol. In this study, patients that were treated with CPAP were found to have a normalized HPA activity in comparison to untreated patients [121]. As previously mentioned, inflammation plays a role in the relationship between chronic pain and sleep disturbance. Several animal studies have showed that a hyperactive HPA axis, secondary to induced inflammatory states, disrupted circadian systems [116]. There have been a paucity of human studies related to inflammation, HPA function, and circadian rhythm, but the few studies have showed possible evidence that an inflammatory state, such as rheumatoid arthritis, may be associated with circadian disruption [116]. In a study of chronic pain patients, researchers found that patients had decreased levels of ACTH, cortisol, and dehydroepiandrosterone (DHEA)/dehydroepiandrosterone sulfate (DHEAS), of which the latter two are steroidal hormones produced by the adrenal gland and are transformed to other biologically active hormones [122]. The researchers posited that chronic pain affects HPA activity and leads to psychiatric, neurological, and inflammatory co-morbidities [122]. In separate studies on the effects of chronic pain on the HPA axis, decreased sensitivity of glucocorticoid receptors secondary to HPA axis dysfunction caused by chronic pain may play a role in an elevated inflammatory state, which is associated with chronic pain [8•]. In normal sleep, slow wave sleep was found to inhibit the HPA axis and decreased cortisol secretion, and this dysfunction of the HPA axis, along with increased cortisol secretion, can be found in patients with chronic pain, amongst other comorbidities.
Conclusion
The relationship between sleep disturbance and chronic pain is complex. There have been many studies analyzing the effects of sleep disturbance and related sleep pathologies in chronic pain patients, and a foray into the biological mechanisms of chronic pain and its effect on sleep. This relationship has been labeled as bidirectional, meaning that pain negatively impacts sleep, and sleep disturbance negatively impacts pain. However, some studies have shown that variable results, emphasizing that alternative pathways must exist in the relationship between sleep and pain. These results have yet to be elucidated, and further research is required. This is particularly evident in the norepinephrine and serotonergic systems governing sleep and pain, demonstrating associative, rather than causal relationship between the two. Still other recent studies and reviews seem to support the fact that sleep disturbance causes worsening pain, rather than the bidirectional relationship seen in earlier studies [10•]. In conclusion, we have described sleep disturbance pathologies and chronic pain, and how neurochemical, anatomical, and physiologic mechanisms interplay between the two. Given the extent of disruption and damage that sleep disturbance and chronic pain cause from an individual to a global level, continued investigation of the relationship and mechanisms, along with novel treatment and diagnosis using emerging technologies, will help further develop our understanding of this complex issue.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Dijk D-J, Landolt H-P. Sleep physiology, circadian rhythms, waking performance and the development of sleep-wake therapeutics. In: Landolt H-P, Dijk D-J, editors. Sleep-wake neurobiology and pharmacology. Cham: Springer International Publishing; 2019. p. 441–81.
Acquavella J, Mehra R, Bron M, Suomi JM-H, Hess GP. Prevalence of narcolepsy and other sleep disorders and frequency of diagnostic tests from 2013–2016 in insured patients actively seeking care. J Clin Sleep Med. 2020;16:1255–63.
Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, persistence, and remission rates of insomnia over 5 years. JAMA Netw Open. 2020;3:e2018782.
Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161:1976–82.
Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160:19–27.
• Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacol. 2020;45:205–16. Review describing various factors that contribute to the bidirectional relationship between sleep disturbance and chronic pain.
Andersen ML, Araujo P, Frange C, Tufik S. Sleep disturbance and pain. Chest. 2018;154:1249–59.
• Boakye PA, Olechowski C, Rashiq S, Verrier MJ, Kerr B, Witmans M, et al. A critical review of neurobiological factors involved in the interactions between chronic pain, depression, and sleep disruption. Clin J Pain. 2016;32:327–36. Reviews the neurobiochemistry mechanisms between chronic pain and sleep disturbance.
Evans S, Djilas V, Seidman LC, Zeltzer LK, Tsao JCI. Sleep quality, affect, pain, and disability in children with chronic pain: is affect a mediator or moderator? J Pain. 2017;18:1087–95.
• Herrero Babiloni A, De Koninck BP, Beetz G, De Beaumont L, Martel MO, Lavigne GJ. Sleep and pain: recent insights, mechanisms, and future directions in the investigation of this relationship. J Neural Transm. 2020;127:647–60. Provides a broad overview of the current status of chronic pain and sleep disturbance, while also providing potential targets for future study.
Generaal E, Vogelzangs N, Penninx BWJH, Dekker J. Insomnia, Sleep Duration, Depressive Symptoms, and the Onset of Chronic Multisite Musculoskeletal Pain. Sleep. 2017;40(1):zsw030. https://doi.org/10.1093/sleep/zsw030
McCarley RW. Neurobiology of REM and NREM sleep. Sleep Med. 2007;8:302–30.
Onton JA, Kang DY, Coleman TP. Visualization of whole-night sleep EEG from 2-channel mobile recording device reveals distinct deep sleep stages with differential electrodermal activity. Front Hum Neurosci. 2016. https://doi.org/10.3389/fnhum.2016.00605.
Campbell IG. EEG recording and analysis for sleep research. Curr Protoc Neurosci. 2009. https://doi.org/10.1002/0471142301.ns1002s49.
Peever J, Fuller PM. The biology of REM sleep. Curr Biol. 2017;27:R1237–48.
Zolovska B, Shatkin JP. Key differences in pediatric versus adult sleep. In: Encyclopedia of sleep. Elsevier; 2013. pp. 573–578.
Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. National Academies Press; 2011:13172. https://doi.org/10.17226/13172
Sateia MJ. International classification of sleep disorders-third edition. Chest. 2014;146:1387–94.
Black LI, Nugent CN, Adams PF. Tables of adult health behaviors, sleep: National Health Interview Survey, 2011–2014. 2016.
Consensus Conference Panel, Watson NF, Badr MS, et al. Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: Methodology and discussion. Sleep. 2015;38:1161–83.
Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007. https://doi.org/10.5664/jcsm.26929.
McBeth J, Wilkie R, Bedson J, Chew-Graham C, Lacey RJ. Sleep disturbance and chronic widespread pain. Curr Rheumatol Rep. 2015;17:1.
Canivet C, Östergren P-O, Choi B, Nilsson P, Sillén UA, Moghadassi M, et al. Sleeping problems as a risk factor for subsequent musculoskeletal pain and the role of job strain: results from a one-year follow-up of the Malmö shoulder neck study cohort. Int J Behav Med. 2008;15:254–62.
Tang NKY, Wright KJ, Salkovskis PM. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J Sleep Res. 2007;16:85–95.
Davies KA, Macfarlane GJ, Nicholl BI, Dickens C, Morriss R, Ray D, et al. Restorative sleep predicts the resolution of chronic widespread pain: results from the EPIFUND study. Rheumatology. 2008;47:1809–13.
Russell MB, Kristiansen HA, Kværner KJ. Headache in sleep apnea syndrome: epidemiology and pathophysiology. Cephalalgia. 2014;34:752–5.
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5.
Redline S, Tishler PV, Hans MG, Tosteson TD, Strohl KP, Spry K. Racial differences in sleep-disordered breathing in African-Americans and Caucasians. Am J Respir Crit Care Med. 1997;155:186–92.
Young T, Palta M, Dempsey J, Peppard PE, Nieto FJ, Hla KM. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ. 2009;108:246–9.
Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006–14.
Young T. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013.
Almoznino G, Benoliel R, Sharav Y, Haviv Y. Sleep disorders and chronic craniofacial pain: Characteristics and management possibilities. Sleep Med Rev. 2017;33:39–50.
Gupta MA, Simpson FC, Gupta AK. Psoriasis and sleep disorders: A systematic review. Sleep Med Rev. 2016;29:63–75.
Köseoğlu Hİ, İnanır A, Kanbay A, Okan S, Demir O, Çeçen O, et al. Is there a link between obstructive sleep apnea syndrome and fibromyalgia syndrome? Turk Thorac J. 2017;18:40–6.
Aytekin E, Demir SE, Komut EA, Okur SC, Burnaz O, Caglar NS, et al. Chronic widespread musculoskeletal pain in patients with obstructive sleep apnea syndrome and the relationship between sleep disorder and pain level, quality of life, and disability. J Phys Ther Sci. 2015;27:2951–4.
Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;92:S70–7.
Maixner W, Fillingim R, Kincaid S, Sigurdsson A, Harris MB. Relationship between pain sensitivity and resting arterial blood pressure in patients with painful temporomandibular disorders. Psychosom Med. 1997;59:503–11.
• Doufas AG, Tian L, Davies MF, Warby SC. Nocturnal intermittent hypoxia is independently associated with pain in subjects suffering from sleep-disordered breathing. Anesthesiology. 2013;119:1149–62. A retrospective review of patients with obstructive sleep apnea showed that nocturnal oxyhemoglobin desaturation was independently associated with pain that disturbed sleep.
Scammell TE, Arrigoni E, Lipton JO. Neural circuitry of wakefulness and sleep. Neuron. 2017;93:747–65.
Dauvilliers Y, Billiard M, Montplaisir J. Clinical aspects and pathophysiology of narcolepsy. Clin Neurophysiol. 2003;114:2000–17.
Cremaschi RC, Hirotsu C, Tufik S, Coelho FM. Chronic pain in narcolepsy type 1 and type 2 – an underestimated reality. J Sleep Res. 2019;28:e12715.
Cohen A, Mandrekar J, St. Louis EK, Silber MH, Kotagal S. Comorbidities in a community sample of narcolepsy. Sleep Med. 2018;43:14–8.
Suzuki K, Miyamoto M, Miyamoto T, et al. The prevalence and characteristics of primary headache and dream-enacting behaviour in Japanese patients with narcolepsy or idiopathic hypersomnia: a multi-centre cross-sectional study. PLoS ONE. 2015;10:e0139229.
Dahmen N, Kasten M, Wieczorek S, Gencik M, Epplen J, Ullrich B. Increased frequency of migraine in narcoleptic patients: a confirmatory study. Cephalalgia. 2003;23:14–9.
• Schuh-Hofer S, Wodarski R, Pfau DB, Caspani O, Magerl W, Kennedy JD, et al. One night of total sleep deprivation promotes a state of generalized hyperalgesia: A surrogate pain model to study the relationship of insomnia and pain. Pain. 2013;154:1613–21. A trial of sleep deprivation in healthy subjects showed the development of hyperalgesia to cold and pinprick.
Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14:1539–52.
Kukushkin ML, Poluektov MG. Current views on chronic pain and its relationship to the state of sleep. Neurosci Behav Physi. 2019;49:13–9.
Matsuda M, Huh Y, Ji R-R. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth. 2019;33:131–9.
Nijs J, Loggia ML, Polli A, Moens M, Huysmans E, Goudman L, et al. Sleep disturbances and severe stress as glial activators: key targets for treating central sensitization in chronic pain patients? Expert Opin Ther Targets. 2017;21:817–26.
Lavigne GJ, Sessle BJ. The neurobiology of orofacial pain and sleep and their interactions. J Dent Res. 2016;95:1109–16.
Wood PB. Role of central dopamine in pain and analgesia. Expert Rev Neurother. 2008;8:781–97.
Amenta F. Peripheral dopamine pathophysiology. Boca Raton, FL: CRC Press; 2019.
Oishi Y, Lazarus M. The control of sleep and wakefulness by mesolimbic dopamine systems. Neurosci Res. 2017;118:66–73.
Taylor AMW, Becker S, Schweinhardt P, Cahill C. Mesolimbic dopamine signaling in acute and chronic pain: implications for motivation, analgesia, and addiction. Pain. 2016;157:1194–8.
Volkow ND, Tomasi D, Wang G-J, Telang F, Fowler JS, Logan J, et al. Evidence that sleep deprivation downregulates dopamine D2R in ventral striatum in the human brain. J Neurosci. 2012;32:6711–7.
Finan PH, Smith MT. The comorbidity of insomnia, chronic pain, and depression: Dopamine as a putative mechanism. Sleep Med Rev. 2013;17:173–83.
Kapur S, Remington G. Serotonin-dopamine interaction and its relevance to schizophrenia. Am J Psychiatry. 1996;153:466–76.
• Bravo L, Llorca-Torralba M, Berrocoso E, Micó JA. Monoamines as drug targets in chronic pain: focusing on neuropathic pain. Front Neurosci. 2019;13:1268. Various neurotransmitters, such as dopamine, norepinephrine, and serotonin may play roles in chronic pain pathways. Some neurotransmitters, such as serotonin, still have undiscovered mechanisms in pain.
Lang PM, Moalem-Taylor G, Tracey DJ, Bostock H, Grafe P. Activity-dependent modulation of axonal excitability in unmyelinated peripheral rat nerve fibers by the 5-HT(3) serotonin receptor. J Neurophysiol. 2006;96:2963–71.
Taiwo YO, Heller PH, Levine JD. Mediation of serotonin hyperalgesia by the cAMP second messenger system. Neuroscience. 1992;48:479–83.
Godínez-Chaparro B, Barragán-Iglesias P, Castañeda-Corral G, Rocha-González HI, Granados-Soto V. Role of peripheral 5-HT4, 5-HT6, and 5-HT7 receptors in development and maintenance of secondary mechanical allodynia and hyperalgesia. Pain. 2011;152:687–97.
Ernberg M, Lundeberg T, Kopp S. Effect of propranolol and granisetron on experimentally induced pain and allodynia/hyperalgesia by intramuscular injection of serotonin into the human masseter muscle. Pain. 2000;84:339–46.
Bobinski F, Ferreira TAA, Córdova MM, et al. Role of brainstem serotonin in analgesia produced by low-intensity exercise on neuropathic pain after sciatic nerve injury in mice. Pain. 2015;156:2595–606.
Negro A, Koverech A, Martelletti P. Serotonin receptor agonists in the acute treatment of migraine: a review on their therapeutic potential. J Pain Res. 2018;11:515–26.
Cespuglio R. Serotonin: its place today in sleep preparation, triggering or maintenance. Sleep Med. 2018;49:31–9.
Elmenhorst D, Kroll T, Matusch A, Bauer A. Sleep deprivation increases cerebral serotonin 2A receptor binding in humans. Sleep. 2012;35:1615–23.
Obata H. Analgesic mechanisms of antidepressants for neuropathic pain. IJMS. 2017;18:2483.
Marks D, Shah M, Patkar A, Masand P, Park G-Y, Pae C-U. Serotonin-norepinephrine reuptake inhibitors for pain control: premise and promise. Curr Neuropharmacol. 2009;7:331–6.
Hayat H, Regev N, Matosevich N, et al. Locus coeruleus norepinephrine activity mediates sensory-evoked awakenings from sleep. Sci Adv. 2020;6:eaaz4232.
Meerlo P, Sgoifo A, Suchecki D. Restricted and disrupted sleep: Effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med Rev. 2008;12:197–210.
Everson CA, Bergmann BM, Rechtschaffen A. Sleep deprivation in the rat: III. Total sleep deprivation. Sleep. 1989;12:13–21.
Irwin M, Thompson J, Miller C, Gillin JC, Ziegler M. Effects of sleep and sleep deprivation on catecholamine and interleukin-2 levels in humans: clinical implications. J Clin Endocrinol Metab. 1999;84:1979–85.
Koh K, Hamada A, Hamada Y, et al. Possible involvement of activated locus coeruleus–noradrenergic neurons in pain-related sleep disorders. Neurosci Lett. 2015;589:200–6.
Yousaf F, Seet E, Venkatraghavan L, Abrishami A, Chung F, Warner DS. Efficacy and safety of melatonin as an anxiolytic and analgesic in the perioperative period. Anesthesiology. 2010;113:968–76.
Danilov A, Kurganova J. Melatonin in chronic pain syndromes. Pain Ther. 2016;5:1–17.
Kaur T, Shyu B-C. Melatonin: a new-generation therapy for reducing chronic pain and improving sleep disorder-related pain. In: Shyu B-C, Tominaga M (eds) Advances in Pain Research: Mechanisms and Modulation of Chronic Pain. Springer Singapore, Singapore; 2019. pp. 229–251.
Wilhelmsen M, Amirian I, Reiter RJ, Rosenberg J, Gögenur I. Analgesic effects of melatonin: a review of current evidence from experimental and clinical studies: Analgesic effects of melatonin. J Pineal Res. 2011;51:270–7.
Chen C. Antinociceptive effects of novel melatonin receptor agonists in mouse models of abdominal pain. WJG. 2014;20:1298.
• Chaudhry SR, Stadlbauer A, Buchfelder M, Kinfe TM. Melatonin moderates the triangle of chronic pain, sleep architecture and immunometabolic traffic. Biomedicines. 2021;9:984. Melatonin may cause analgesia via GABA and opioid receptors, as well as possible antiinflammatory pathways.
Leger D, Laudon M, Zisapel N. Nocturnal 6-sulfatoxymelatonin excretion in insomnia and its relation to the response to melatonin replacement therapy. Am J Med. 2004;116:91–5.
Ferracioli-Oda E, Qawasmi A, Bloch MH. Meta-analysis: melatonin for the treatment of primary sleep disorders. PLoS ONE. 2013;8:e63773.
• Xie S, Fan W, He H, Huang F. Role of melatonin in the regulation of pain. J Pain Res. 2020;13:331–43. Review of melatonin and its relationship with pain. Melatonin is known to attenuate hyperalgesia and allodynia in animal models, and this review presents several mechanisms on this effect. However, mechanisms are not fully understood.
• de Oliveira DL, Hirotsu C, Tufik S, Andersen ML. The interfaces between vitamin D, sleep and pain. J Endocrinol. 2017;234:R23–36. Systematic review of vitamin D levels and the association with chronic pain and sleep disturbance; pain conditions have been inversely correlated with vitamin D levels and the administration of vitamin D may contribute to good sleep hygiene.
Heidari B, Shirvani JS, Firouzjahi A, Heidari P, Hajian-Tilaki KO. Association between nonspecific skeletal pain and vitamin D deficiency: Vitamin D deficiency and skeletal pain. Int J Rheum Dis. 2010;13:340–6.
Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78:1463–70.
McCarty DE, Reddy A, Keigley Q, Kim PY, Cohen S, Marino AA. Nonspecific pain is a marker for hypovitaminosis D in patients undergoing evaluation for sleep disorders: a pilot study. Nat Sci Sleep. 2013;5:37-42. https://doi.org/10.2147/nss.s42641
Huang W, Shah S, Long Q, Crankshaw AK, Tangpricha V. Improvement of pain, sleep, and quality of life in chronic pain patients with vitamin D supplementation. Clin J Pain. 2013;29:341–7.
Brewer LD, Thibault V, Chen K-C, Langub MC, Landfield PW, Porter NM. Vitamin D hormone confers neuroprotection in parallel with downregulation of L-type calcium channel expression in hippocampal neurons. J Neurosci. 2001;21:98–108.
Brown J, Bianco JI, McGrath JJ, Eyles DW. 1,25-Dihydroxyvitamin D3 induces nerve growth factor, promotes neurite outgrowth and inhibits mitosis in embryonic rat hippocampal neurons. Neurosci Lett. 2003;343:139–43.
Feldman D, Krishnan A, Moreno J, Swami S, Peehl DM, Srinivas S. Vitamin D inhibition of the prostaglandin pathway as therapy for prostate cancer. Nutr Rev. 2008;65:S113–5.
Moalem G, Tracey DJ. Immune and inflammatory mechanisms in neuropathic pain. Brain Res Rev. 2006;51:240–64.
Deluca HF, Cantorna MT. Vitamin D: its role and uses in immunology 1. FASEB J. 2001;15:2579–85.
Cury Y, Picolo G, Gutierrez VP, Ferreira SH. Pain and analgesia: The dual effect of nitric oxide in the nociceptive system. Nitric Oxide. 2011;25:243–54.
Takahashi K, Nakayama Y, Horiuchi H, Ohta T, Komoriya K, Ohmori H, et al. Human neutrophils express messenger RNA of vitamin D receptor and respond to 1 α, 25-dihydroxyvitamin D 3. Immunopharmacol Immunotoxicol. 2002;24:335–47.
Kalueff AV, Tuohimaa P. Neurosteroid hormone vitamin D and its utility in clinical nutrition. Curr Opin Clin Nutr Metab Care. 2007;10:12–9.
Shipton EA, Shipton EE. Vitamin D and pain: vitamin D and its role in the aetiology and maintenance of chronic pain states and associated comorbidities. Pain Res Treat. 2015;2015:1–12.
McCarty DE, Reddy A, Keigley Q, Kim PY, Marino AA. Vitamin D, race, and excessive daytime sleepiness. J Clin Sleep Med. 2012;08:693–7.
Carrive P. Orexin, orexin receptor antagonists and central cardiovascular control. Front Neurosci. 2013. https://doi.org/10.3389/fnins.2013.00257.
Ahmadi-Soleimani SM, Mianbandi V, Azizi H, Azhdari-Zarmehri H, Ghaemi-Jandabi M, Abbasi-Mazar A, et al. Coregulation of sleep-pain physiological interplay by orexin system: An unprecedented review. Behav Brain Res. 2020;391:112650.
Sakurai T. The neural circuit of orexin (hypocretin): maintaining sleep and wakefulness. Nat Rev Neurosci. 2007;8:171–81.
Dauvilliers Y, Bayard S, Shneerson JM, Plazzi G, Myers AJ, Garcia-Borreguero D. High pain frequency in narcolepsy with cataplexy. Sleep Med. 2011;12:572–7.
Chen Y-H, Lee H-J, Lee MT, Wu Y-T, Lee Y-H, Hwang L-L, et al. Median nerve stimulation induces analgesia via orexin-initiated endocannabinoid disinhibition in the periaqueductal gray. Proc Natl Acad Sci USA. 2018;115:E10720–9.
Hysing E-B, Smith L, Thulin M, Karlsten R, Bothelius K, Gordh T. Detection of systemic inflammation in severely impaired chronic pain patients and effects of a multimodal pain rehabilitation program. Scand J Pain. 2019;19:235–44.
Lisowska B, Lisowski A, Siewruk K. Substance P and Chronic Pain in Patients with Chronic Inflammation of Connective Tissue. PLoS ONE. 2015;10:e0139206.
Ji R-R, Chamessian A, Zhang Y-Q. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354:572–7.
Mullington JM, Simpson NS, Meier-Ewert HK, Haack M. Sleep loss and inflammation. Best Pract Res Clin Endocrinol Metab. 2010;24:775–84.
Leys LJ, Chu KL, Xu J, Pai M, Yang HS, Robb HM, et al. Disturbances in slow-wave sleep are induced by models of bilateral inflammation, neuropathic, and postoperative pain, but not osteoarthritic pain in rats. Pain. 2013;154:1092–102.
Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiat. 2016;80:40–52.
Haack M, Sanchez E, Mullington JM. Elevated inflammatory markers in response to prolonged sleep restriction are associated with increased pain experience in healthy volunteers. Sleep. 2007;30:1145–52.
Watkins LR, Maier SF. Immune regulation of central nervous system functions: from sickness responses to pathological pain. J Intern Med. 2005;257:139–55.
Kheirandish-Gozal L, Gozal D. Obstructive sleep apnea and inflammation: proof of concept based on two illustrative cytokines. IJMS. 2019;20:459.
• Charokopos A, Card ME, Gunderson C, Steffens C, Bastian LA. The association of obstructive sleep apnea and pain outcomes in adults: a systematic review. Pain Med. 2018;19:S69–75. Systematic review that showed that obstructive sleep apnea was associated with increased pain intensity and an improvement in pain with the use of a CPAP machine.
• Heffner KL, France CR, Ashrafioun L, Quiñones M, Walsh P, Maloney MD, et al. Clinical pain-related outcomes and inflammatory cytokine response to pain following insomnia improvement in adults with knee osteoarthritis. Clin J Pain. 2018;34:1133–40. This study showed that improvement in insomnia symptoms resulted in a decrease of inflammatory markers, as well as suggesting that inflammatory pathways were involved in insomnia symptoms and chronic pain.
Spencer RL, Deak T. A users guide to HPA axis research. Physiol Behav. 2017;178:43–65.
Dumbell R, Matveeva O, Oster H. Circadian clocks, stress, and immunity. Front Endocrinol. 2016. https://doi.org/10.3389/fendo.2016.00037.
Lightman SL, Birnie MT, Conway-Campbell BL. Dynamics of ACTH and cortisol secretion and implications for disease. Endocr Rev. 2020;41:470–90.
Weitzman ED, Zimmerman JC, Czeisler CA, Ronda J. Cortisol secretion is inhibited during sleep in normal man. J Clin Endocrinol Metab. 1983;56:352–8.
Nicolaides NC, Vgontzas AN, Kritikou I, Chrousos G. HPA axis and sleep. Endotext. 2000.
• Szmyd B, Rogut M, Białasiewicz P, Gabryelska A. The impact of glucocorticoids and statins on sleep quality. Sleep Med Rev. 2021;55:101380. A systematic review on glucocorticoids and the effect on sleep disturbance; in particular, glucocorticoid receptors in the brain and subsequent serotonin depletion seem to mediate this effect.
Guyon A, Morselli LL, Balbo ML, Tasali E, Leproult R, L’Hermite-Balériaux M, et al. Effects of insufficient sleep on pituitary-adrenocortical response to CRH stimulation in healthy men. Sleep. 2017. https://doi.org/10.1093/sleep/zsx064.
Henley DE, Russell GM, Douthwaite JA, Wood SA, Buchanan F, Gibson R, et al. Hypothalamic-pituitary-adrenal axis activation in obstructive sleep apnea: the effect of continuous positive airway pressure therapy. J Clin Endocrinol Metab. 2009;94:4234–42.
Aloisi AM, Buonocore M, Merlo L, Galandra C, Sotgiu A, Bacchella L, et al. Chronic pain therapy and hypothalamic-pituitary-adrenal axis impairment. Psychoneuroendocrinology. 2011;36:1032–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no relevant financial or non-financial interests to disclose.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Alternative Treatments for Pain Medicine
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, M.T., Robinson, C.L., Ruan, Q.Z. et al. The Influence of Sleep Disturbance on Chronic Pain. Curr Pain Headache Rep 26, 795–804 (2022). https://doi.org/10.1007/s11916-022-01074-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11916-022-01074-2