
Abstract
Significant advances have allowed diffusion magnetic resonance imaging (MRI) to evolve into a powerful tool in the field of movement disorders that can be used to study disease states and connectivity between brain regions. Diffusion MRI is a promising potential biomarker for Parkinson’s disease and other forms of parkinsonism, and may allow the distinction of different forms of parkinsonism. Techniques such as tractography have contributed to our current thinking regarding the pathophysiology of dystonia and possible mechanisms of penetrance. Diffusion MRI measures could potentially assist in monitoring disease progression in Huntington’s disease, and in uncovering the nature of the processes and structures involved the development of essential tremor. The ability to represent structural connectivity in vivo also makes diffusion MRI an ideal adjunctive tool for the surgical treatment of movement disorders. We review recent studies using diffusion MRI in movement disorders research and present the current state of the science as well as future directions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although the clinical use of magnetic resonance imaging (MRI) has revolutionized the diagnosis and management of neurological diseases, its utility in neurodegenerative diseases was initially limited to the exclusion of other diagnoses [1]. During the past three decades, significant advances have been made in the field of MRI that have increased its value in the study of neurodegenerative diseases, and these advances have occurred in a time period that has largely paralleled the maturation of the field of movement disorders as a neurologic subspecialty [2]. During this time period, diffusion MRI has emerged as a powerful tool in the field of movement disorders, both in research settings and in clinical settings for evaluating white matter (WM), gray matter (GM), and connectivity.
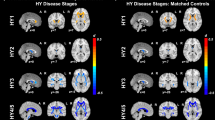
Diffusion MRI makes use of the random translational motion of molecules that occurs secondary to thermal energy and is influenced by a variety of microstructural factors, including organelles, neurofibrils, and membranes. Diffusion can be relatively directional (anisotropic) or can occur relatively equally in all directions (isotropic). The degree and direction of diffusion can be used to produce accurate contrast images, and a tensor can be calculated to estimate diffusivity in three-dimensional space [3]. From this tensor one can calculate the mean-squared displacement of molecules (mean diffusivity, MD) and the degree to which diffusion is directional (fractional anisotropy, FA, which ranges between 0 and 1). Additional scalars such as axial diffusivity and radial diffusivity can be used to estimate the magnitude of diffusion parallel and perpendicular to the principal axis of diffusion, respectively. As underlying fiber orientation can be inferred from the orientation of the longest axis of the tensor, fiber orientation in neighboring pixels can be repeatedly reconstructed to produce streamlines to reconstruct WM pathways in a process called tractography, making diffusion MRI especially useful in the analysis of WM tracts in the brain. Figure 1 shows some of the major analytic approaches that have been used, and includes region of interest (ROI) analysis, voxel-based analysis, tract-based spatial statistics (TBSS), and tractography.

Visual representations of the major diffusion magnetic resonance imaging analysis methods that are currently in use. Clockwise from top left: manual selection of regions of interest; automated tract-based spatial statistics aligns a combined fractional anisotropy map on a fractional anisotropy skeleton; tractography involves tract reconstruction based on the orientation and magnitude of diffusion, after which probabilities of connectivity can be analyzed; automated voxel-based analysis registers diffusion maps into a standard space. (Reproduced with permission from Prodoehl J et al. [4••], Zheng et al. [5], Saini et al. [6], Argyelan et al. [7], Wang et al. [8], and Zhang et al. [9])
The interpretation of diffusion MRI measures, including the specific abnormalities that these proxy measures represent and the conclusions that can be drawn from abnormal values in disease, can be controversial [10]. Results can be highly dependent on the appropriateness of the methods of acquisition and data processing [11]. With these caveats in mind, changes in diffusion MRI scalars can reveal important information about the microstructural properties of underlying tissues. FA is higher in areas of highly coherent fiber structure and is affected by myelination. Reduced axial diffusivity has been correlated with axonal injury, whereas increased radial diffusivity has been suggested to represent incomplete or damaged myelination [11]. Reduced probabilities of tractography are believed to represent compromised WM fiber integrity or a reduction in fiber myelination or number [12].
Diffusion MRI can be used to study differences in tissue properties at specific locations in the brain between individuals or groups, to look for relationships between diffusion MRI properties and other variables (such as task performance), and to investigate connectivity between GM and WM or alternatively to attempt to reconstruct specific WM pathways [10]. Recently, diffusion MRI studies have made major contributions in a variety of subdisciplines within the field of movement disorders, with wide-ranging implications for pathophysiology, differential diagnosis, surgical treatment, and the search for possible biomarkers of disease.
In this review, we discuss the evolving role of diffusion MRI in the study of movement disorders, and we emphasize the most important publications in the field within the past year. As our scope is focused across all movement disorders, this work is not intended to be exhaustive (the reader is directed to disease-specific reviews of diffusion MRI for such purposes). We do, however, hope to present the state of the science regarding the role of diffusion MRI in movement disorders research, and we will discuss diffusion MRI in the context and framework of prior research within each field.
Diffusion MRI in Parkinsonism
The study of Parkinson’s disease (PD) and parkinsonism has evolved into a multifaceted field that has many different avenues of approach, and many of these areas of interest are actively making use of diffusion MRI technology to answer research questions. Table 1 reviews the manner in which diffusion MRI has been used in the past year to study parkinsonism. In addition, we recommend a recent systematic review and meta-analysis [33••] that includes many studies that predate the studies described.
One of the most important and exciting aspects of PD research has been the quest for a biomarker of disease that can facilitate diagnosis, allow objective monitoring of disease progression, and evaluate the efficacy of potential therapeutic and neuroprotective therapies [34]. Diffusion MRI is among those modalities being investigated in this regard. Many different GM and WM structures have been investigated using diffusion MRI, and abnormalities in a variety of areas have been reported [33••]. However, given what we know about the pathogenesis of PD, it is not surprising that the substantia nigra (SN) has been the most commonly studied area. Although not all studies have found a reduction in FA in the SN [35, 36], a recent meta-analysis [33••] found a significant pooled effect size for reduction of FA in the SN across studies. One study achieved 100 % sensitivity and specificity in distinguishing early medication naive patients from controls in the ventral SN [37]. A recent follow-up study [38] demonstrated that, in normal aging, FA decreased and radial diffusivity increased in the dorsal SN but not in the ventral SN, again consistent with earlier histopathology studies. These studies further the suggestion put forth by animal models that diffusion MRI may act as a proxy for dopaminergic degeneration in the SN [39]. They also highlight the critical importance of where ROIs are defined in obtaining meaningful results [38] as well as the possible potential of diffusion MRI of the SN as a biomarker for PD [40].
Diffusion MRI is also being investigated in combination with other neuroimaging modalities. Diffusion MRI measures have been combined with inverse T2* (R2*) [41], another MRI measure that has been shown to be increased in PD patients and is thought to correlate with iron concentration, to see if the combined measures improve separation between PD and controls [42••]. Mean FA was reduced and R2* was increased in the SN of patients compared with controls, with improved discrimination between groups when the modalities were combined. Further, there was no correlation between the two measures, which the authors of the study suggested could indicate that these measures could reflect independent ongoing pathological processes in the SN. A follow-up study from the same group [17] expanded these earlier findings and showed that the decrease in FA in the SN in PD was significant early in the caudal region of the SN, whereas in the rostral SN the decrease in FA was only significant in late stages of the disease. R2* in the caudal SN also correlated with clinical scores, disease duration, and levodopa dosage.
Although the commonest cause of parkinsonism is PD, the syndromes of multiple system atrophy, progressive supranuclear palsy (PSP), and corticobasal degeneration, as well as a variety of other disorders, can also result in parkinsonism, and the clinical differentiation between these diseases can sometimes be difficult [43]. In addition to detecting PD, the ability of diffusion MRI to differentiate PD from atypical parkinsonism and the atypical parkinsonism disorders from each other is also being investigated. A recent study [4••] used a multitarget approach based on prior diffusion MRI studies and areas of the brain that are known to be affected by specific diseases in a population of patients with PD, multiple system atrophy, parkinsonism subtype (MSA-P), PSP, and essential tremor (ET) and healthy controls. Receiver operating characteristic analyses demonstrated an area under the curve of 0.99 (sensitivity 90 %, specificity 100 %) in distinguishing PD from atypical parkinsonism. Areas under the curves of 0.99, 0.96, and 0.97 were achieved for distinguishing PD versus MSA-P, PD versus PSP, and MSA-P versus PSP, respectively, with unique diffusion MRI measures and subcortical ROIs for each group. The study also found excellent separation between PD and ET. Given the recent finding of increased FA in the somatosensory cortex in PD [13], future analyses that include a cortical ROI may further improve classification.
In summary, diffusion MRI in the SN and in other areas of the brain is a promising potential biomarker for PD and other forms of parkinsonism. It may also provide a powerful method to distinguish PD from atypical parkinsonism and the atypical parkinsonism disorders from each other, and can possibly answer questions, such as the temporal order of structural abnormalities that occur in parkinsonism, that cannot be answered by neuropathology studies. Diffusion-related measures have been correlated with motor dysfunction and cognitive performance in domains such as executive function, language, and attention [5]. Diffusion MRI can be useful to evaluate genetic forms of disease, to study specific symptoms, and to complement other imaging and nonimaging modalities to better understand the underlying pathophysiology and network-level dysfunction.
Diffusion MRI in Other Movement Disorders
As in parkinsonism, diffusion MRI has been used to investigate the structural and network underpinnings of other movement disorders. Table 2 describes the articles published in the last year involving diffusion MRI in the study of dystonia, Huntington’s disease (HD), and ET. Additionally, the use of diffusion MRI techniques in movement disorders surgery is also described.
Dystonia
Although dystonia was traditionally considered a disease of the basal ganglia, the pathophysiology of dystonia is now thought to involve multiple levels of the neuraxis, with a loss of motor inhibition as well as disordered sensory processing, neuroplasticity, and somatotopic organization [43]. Neuroimaging studies have been crucial in the development of a broader network model of dystonia pathophysiology that includes the multiple brain regions that are likely involved in its development. Structural abnormalities giving rise to secondary dystonia have been demonstrated throughout the brain, and the results of nuclear imaging studies, functional MRI findings of brain activation patterns, and voxel-based morphometry studies of regional GM volumes have differed depending on the type of dystonia studied (for extensive reviews including diffusion MRI studies, see Neychev et al. [55•] and Zoons et al. [56•]).
Diffusion MRI has been useful in evaluating WM connectivity and integrity in hereditary and idiopathic forms of dystonia. In young-onset hereditary dystonia, the evolving notion of the disease as a neurodevelopmental disorder involving pathways of the basal ganglia, cortex, and cerebellum has been heavily influenced by diffusion MRI studies [57]. The earliest diffusion MRI study in DYT1 carriers (manifesting and nonmanifesting carriers) found decreases in FA in the WM underlying the sensorimotor cortex compared with age-matched controls [58]. Subsequent studies [59] in DYT1 and DYT6 patients confirmed this finding and expanded the reduced FA findings to the dorsal pontine brainstem. One of the most promising studies described to date [7] used probabilistic tractography to show reduced probability of connectivity in the proximal cerebellothalamic pathway near the dentate nucleus in mutation carriers, with penetrance regulated by an additional connectivity abnormality in the subrolandic WM of the thalamocortical projections. The authors of the study hypothesized that reduced penetrance in asymptomatic gene carriers may be due to a protective effect of the thalamocortical pathway disruption in altering the effect of the more caudal abnormality. This report has been further strengthened by abnormalities found in thalamocortical and cerebellocortical pathways in torsin A DYT1 knock-in mice [60•]. In addition to genetic dystonia, abnormalities in diffusion MRI measures in focal dystonias such as torticollis [61–64], writer’s cramp [65], and spasmodic dysphonia [66] have also been described in the WM connections of the pathways of the basal ganglia, cortex, and cerebellum, suggesting an important role of these areas in gene-negative primary dystonias.
In addition to the interest in the role of cerebellothalamocortical connections in hereditary dystonia described above [7], recent interest has also focused on collateralized pallidal connections to the thalamus and brainstem and hemispheric differences in diffusion MRI findings in gene-negative primary focal dystonias [12, 67, 68]. In a 2006 study, Blood et al. [68] compared patients with primary focal dystonia and healthy controls and demonstrated increased hemispheric asymmetry in FA in the WM fibers between the pallidum/putamen and the thalamus. Further, this asymmetry was no longer different from that in controls after botulinum toxin injections. Blood [67] hypothesized that these differences might represent abnormal functioning of a distributed (and possibly lateralized) postural control system that could result in dystonia. Recently, Blood et al. [12] used diffusion MRI measures (FA and MD) and probabilistic tractography to further investigate pallidal connections to the brainstem in 12 DYT1-negative patients with cervical dystonia and 12 healthy matched controls. Focusing on the bilateral pallidum and ansa lenticularis as their seed ROI, they found reduced FA in the WM near the left superior cerebellar peduncle and increased FA near the left SN. A reduced probability of connectivity was shown in the left ansa lenticularis projections to the ipsilateral brainstem in dystonia patients compared with controls, with the greatest difference demonstrated in the area between the ansa lenticularis and the region of the red nucleus and SN. In the right hemisphere, increased probability of connectivity was found in the connections between the pallidum and the brainstem.
In summary, diffusion MRI (and especially tractography) has made major contributions to our current thinking regarding the pathophysiology of dystonia, and has helped to expand our focus beyond the basal ganglia to include related connections to and between the brainstem, cerebellum, and cortex. These studies have proposed models to explain reduced penetrance, directed attention to possible hemispheric differences in the disease, and fueled hypotheses incorporating dysfunction of postural control in models of dystonia. Examination of the similarities and differences between diffusion MRI abnormalities in the various forms of dystonia may shed light on a shared pathophysiology as well as how dystonia can be focal in presentation [56•]. Diffusion MRI studies in patients treated with botulinum toxin might elucidate the manner in which the toxin exerts a central effect though motor afferent feedback, and may suggest new treatment modalities. Expanding diffusion MRI analyses to include dystonia-plus syndromes and secondary dystonias may further elucidate characteristics that are shared between and that differentiate the various dystonia subtypes.
Huntington’s Disease
HD is a neurodegenerative disorder that produces progressive degeneration and volume loss of the striatum and other GM and WM structures in a process that begins well before the onset of clinical symptoms. The symptoms of HD are progressive and include motor dysfunction, cognitive decline, and neuropsychiatric disturbances [43].
As would be expected from neuropathology data, conventional and volumetric brain imaging have shown reductions in the volumes of the striatum and putamen in symptomatic and presymptomatic HD, as well as cortical GM loss and whole brain atrophy in some studies [69]. These findings of volume loss in the striatum have been confirmed in large multicenter studies such as PREDICT-HD [70] and TRACK-HD [71], and caudate volume abnormalities have been correlated with cognitive function, repeat length, and age of manifestation of clinical symptoms [51]. However, not all T1-weighted structural imaging studies have yielded consistent results [72].
A number of studies have investigated diffusion characteristics in symptomatic and preclinical HD [73–82], demonstrating microstructural changes in multiple areas of the brain (for a comprehensive review, see Esmaeilzadeh et al. [83•]). Some caution has, however, been raised that the changes in FA reported in some of these studies might be due to misregistration of images due to neurodegenerative changes [72], and diffusion MRI findings have also not been consistent across all studies [50]. Among the studies that have looked at diffusion MRI measures longitudinally, some studies [84] have found worsening abnormalities in diffusion MRI measures over time, whereas some have not [85]. Many of the diffusion MRI scalar abnormalities have been shown to correlate with clinical features [84–86]. Unified Huntington’s Disease Rating Scale score has been shown to correlate with MD in the corpus callosum in an area demonstrated by tractography to connect to premotor and supplementary motor areas, and radial diffusivity in areas of the corpus callosum projecting to the prefrontal cortices has also been demonstrated to correlate with cognition [82]. In tractography studies of presymptomatic HD patients, a reduction of streamlines directed to the caudate was demonstrated, with the degree of impairment of voluntary saccades correlating with fewer fiber tracking streamlines between the caudate and the frontal cortex [87].
The studies using diffusion MRI techniques to study HD published within the past year have spanned human and animal models of the disease, and have included established as well as new diffusion MRI techniques in a variety of different areas of the brain. The first diffusion MRI study [49] of quinolinic acid induced excitotoxicity, a commonly used lesioning model of HD in rats [88], found that diffusion MRI discriminated between rats that developed cortical lesions from those that did not secondary to lesioning. In addition, diffusion MRI measures were more sensitive than histology in detecting microstructural changes in the caudate, putamen, and internal and external capsules, complementing data from the same group [89], who presented the first diffusion MRI data in a transgenic mouse model of HD.
One study [51] combined motor and cognitive measures with diffusion MRI and volumetric analysis in patients with and without symptoms and healthy controls and found the highest level of discriminative accuracy (78 %) was attained when motor and cognitive scores were added to neuroimaging measures. This level of accuracy was slightly higher than that (76 %) found using machine learning approaches and voxel-based volumetric analysis [90]. Another study [47] found that motor and cognitive tasks were correlated with abnormal diffusion MRI measures in multiple areas of GM and WM, suggesting that dysfunction in extrastriatal areas of the brain is related to clinical manifestations in a region-specific manner. Dumas et al. [50] found more widespread diffusion MRI abnormalities in early-manifesting HD compared with premanifesting HD, with correlations between diffusion MRI and clinical measures. A study [52] that examined diffusion MRI measures in the subregions of the prefrontal cortex in presymptomatic HD patients and controls found that diffusion MRI abnormalities largely followed “disease burden” as defined by the age–CAG length calculation, and a recent tractography study [53] examined symptomatic HD patients and healthy controls and developed detailed maps and percentages of reduced inferred connectivity from the striatum to the cortex.
In summary, diffusion MRI has the potential to contribute to the study of HD on a number of different fronts. Although genetic testing generally negates the need for a biomarker for diagnosis, a quantitative method of monitoring disease progression would be useful should more effective treatment options become available [69, 91]. It could potentially allow objective investigation into the relationship between specific clinical findings and microstructural changes and function as a means of predicting the time to symptom onset and monitoring disease progression [51]. Combining diffusion MRI measures with other neuroimaging measures, as well as clinical data, might be better than diffusion MRI alone. As the sequence of pathogenic events that occur in HD remain poorly understood [92], specific measures of diffusion MRI may be useful as in vivo representations of these processes, and are being investigated as such [84]. In addition, diffusion MRI studies in animal models of disease may also be useful in developing novel connectivity-based markers of HD-related pathological processes [92].
Essential Tremor
Compared with other movement disorders, relatively few studies investigating ET with diffusion MRI have been published. The first report that used diffusion-weighted imaging to study patients with ET used an ROI approach and found no differences in MD values between ET patients and normal controls in the cerebellum, basal ganglia, and frontal WM [93]. Subsequent studies using diffusion MRI found reduced FA in areas of the cerebellum, pons, and the WM of the midbrain and cerebral cortex in a voxel-wise analysis [94] and reduced FA in the dentate nucleus and the superior cerebellar peduncle (along with increased MD), with no overlap in FA values between patients and controls in the dentate nucleus [95]. A 2011 study found an increase in MD in the red nucleus but no differences in FA among the basal ganglia, thalamus, red nucleus, and SN of ET patients compared with controls [96]. Another group the same year [97] showed increased MD in the bilateral inferior cerebellar peduncle, adjacent to the left parieto-occipital sulcus, and in bilateral frontal and parietal WM, with decreased FA in the right inferior cerebellar peduncle and a correlation between tremor scores and MD values in some WM regions in patients with ET.
Two articles have reported use of diffusion MRI techniques in the study of ET within the past year [6, 54]. The first of these [6] used TBSS and ROI analysis of specific WM tracts in 22 patients with definite or probable ET and 17 normal matched controls. TBSS showed increased asymmetric MD changes and increased axial diffusivity throughout the bilateral cortical WM, potentially suggesting axonal damage. No correlations were found between diffusion MRI measures and tremor severity or disease duration. The most recent work [54] to analyze diffusion MRI measures in ET did so as part of a study to evaluate cerebellar WM in familial cortical myoclonic tremor with epilepsy, showing that mean FA was significantly decreased in patients with familial cortical myoclonic tremor with epilepsy compared with the other groups, but FA was not different between ET patients and controls.
In summary, the body of diffusion MRI literature in ET is not as developed as in other movement disorders, which may be due to both a smaller study number and the nature of the disease. The syndrome of ET itself is likely more heterogeneous [98], and the abnormalities present in ET might be subtler and more difficult to identify. Despite these challenges, a number of useful observations have been made to guide future research. Studies that focus on the cerebellum might be best approached with ROI analysis, as involvement of these regions is guided by strong hypotheses and data from the greater literature and thus they may produce more robust results than voxelwise comparisons [97]. Laterality of tremor and handedness may also be important factors, and should be carefully considered in future studies [6], and certainly larger sample sizes are needed. Although some the findings of some reports have been interpreted as supporting the notion of ET as a neurodegenerative disease [94], it is important to consider that microstructural WM abnormalities suggested by diffusion MRI do not differentiate between changes due to a neurodegenerative process and those that might occur secondary to ongoing abnormal oscillatory activity in a tremorogenic network. Further correlation with neuropathology data might shed light on the underlying microstructural changes that the diffusion MRI abnormalities represent in the ET brain.
Diffusion MRI in Movement Disorders Surgery
The ability to represent structural connectivity in vivo makes diffusion MRI an ideal adjunctive tool for deep brain stimulation (DBS) surgery for movement disorders, and diffusion MRI will likely be increasingly used in the planning of DBS surgical procedures in the future [11]. As DBS technology advances, the ability to target specific subregions of GM in a given individual for stimulation will be important in optimizing clinical benefit and minimizing side effects [99, 100]. Diffusion MRI is already being used to investigate interindividual variability in DBS targeting [101] in patient-specific partitioning of thalamic areas on the basis of the probability of connectivity with motor cortices [102], a concept that has been validated [103] and for which refinement of methods is continuously being sought [104]. Further, as WM tracts may sometimes be more ideal targets for neurostimulation than GM structures, diffusion MRI may allow direct targeting of WM pathways [105]. Tractography studies guided by effective DBS placement can be used as a starting point to elucidate network connectivity such as in tremor [106•].
Conclusions
Diffusion MRI has evolved into an invaluable tool in the study of movement disorders, and is used in studies of disease states, connectivity between brain regions, and brain development [3]. In a variety of disorders, diffusion MRI is showing promise as a biomarker of disease, which is encouraging since MRI is noninvasive, is widely available, and generates reproducible data that can be analyzed offline if required [107]. However, in the absence of standardized techniques, variability in methods of acquisition, image processing, and analysis can affect the reproducibility of findings. The sensitivity and specificity of potential diffusion MRI biomarkers may vary throughout the course of the disease [74], and the future role of diffusion MRI as a biomarker could be as part of a battery of tests. Future studies will help to determine the degree to which diffusion MRI measures can serve as a proxy for disease presence and progression in movement disorders.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Scherfler C, Schocke MF, Seppi K, Esterhammer R, Brenneis C, Jaschke W, et al. Voxel-wise analysis of diffusion weighted imaging reveals disruption of the olfactory tract in Parkinson's disease. Brain. 2006;129(2):538–42. doi:10.1093/brain/awh674.
Stoessl AJ, Brooks DJ, Eidelberg D. Milestones in neuroimaging. Mov Disord. 2011;26(6):868–978. doi:10.1002/mds.23679.
Mori S, Zhang J. Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron. 2006;51(5):527–39. doi:10.1016/j.neuron.2006.08.012.
•• Prodoehl J, Li H, Planetta PJ, Goetz CG, Shannon KM, Tangonan R, et al. Diffusion tensor imaging of Parkinson’s disease, atypical Parkinsonism, and essential tremor. Mov Disord. 2013. doi:10.1002/mds.25491. This study used a multitargeted approach using basal ganglia and cerebellar ROI to study the discriminative capability of diffusion MRI in patients with PD, MSA-P, PSP, and ET and healthy controls. Excellent differentiation was achieved between the differentiation of diseases from each other and from controls, and the pattern of diffusion MRI targets and measures was unique for each disease.
Zheng Z, Shemmassian S, Wijekoon C, Kim W, Bookheimer SY, Pouratian N. DTI correlates of distinct cognitive impairments in Parkinson's disease. Hum Brain Mapp. 2013. doi:10.1002/hbm.22256.
Saini J, Bagepally BS, Bhatt MD, Chandran V, Bharath RD, Prasad C, et al. Diffusion tensor imaging: tract based spatial statistics study in essential tremor. Parkinsonism Relat Disord. 2012;18(5):477–82. doi:10.1016/j.parkreldis.2012.01.006.
Argyelan M, Carbon M, Niethammer M, Ulug AM, Voss HU, Bressman SB, et al. Cerebellothalamocortical connectivity regulates penetrance in dystonia. J Neurosci. 2009;29(31):9740–7. doi:10.1523/JNEUROSCI.2300-09.2009.
Wang HC, Hsu JL, Leemans A. Diffusion tensor imaging of vascular parkinsonism: structural changes in cerebral white matter and the association with clinical severity. Arch Neurol. 2012;69(10):1340–8. doi:10.1001/archneurol.2012.633.
Zhang K, Yu C, Zhang Y, Wu X, Zhu C, Chan P, et al. Voxel-based analysis of diffusion tensor indices in the brain in patients with Parkinson's disease. Eur J Radiol. 2011;77(2):269–73. doi:10.1016/j.ejrad.2009.07.032.
Jones DK, Knosche TR, Turner R. White matter integrity, fiber count, and other fallacies: the do's and don'ts of diffusion MRI. Neuroimage. 2013;73:239–54. doi:10.1016/j.neuroimage.2012.06.081.
Soares JM, Marques P, Alves V, Sousa N. A hitchhiker's guide to diffusion tensor imaging. Front Neurosci. 2013;7:31. doi:10.3389/fnins.2013.00031.
Blood AJ, Kuster JK, Woodman SC, Kirlic N, Makhlouf ML, Multhaupt-Buell TJ, et al. Evidence for altered basal ganglia-brainstem connections in cervical dystonia. PloS One. 2012;7(2):e31654. doi:10.1371/journal.pone.0031654.
Zhan W, Kang GA, Glass GA, Zhang Y, Shirley C, Millin R, et al. Regional alterations of brain microstructure in Parkinson's disease using diffusion tensor imaging. Mov Disord. 2012;27(1):90–7. doi:10.1002/mds.23917.
Prakash BD, Sitoh YY, Tan LC, Au WL. Asymmetrical diffusion tensor imaging indices of the rostral substantia nigra in Parkinson's disease. Parkinsonism Relat Disord. 2012;18(9):1029–33. doi:10.1016/j.parkreldis.2012.05.021.
Planetta PJ, Schulze ET, Geary EK, Corcos DM, Goldman JG, Little DM, et al. Thalamic projection fiber integrity in de novo Parkinson disease. AJNR Am J Neuroradiol. 2013;34(1):74–9. doi:10.3174/ajnr.A3178.
Agosta F, Kostic VS, Davidovic K, Kresojevic N, Sarro L, Svetel M, et al. White matter abnormalities in Parkinson's disease patients with glucocerebrosidase gene mutations. Mov Disord. 2013;28(6):772–8. doi:10.1002/mds.25397.
Du G, Lewis MM, Sen S, Wang J, Shaffer ML, Styner M, et al. Imaging nigral pathology and clinical progression in Parkinson's disease. Mov Disord. 2012;27(13):1636–43. doi:10.1002/mds.25182.
Sharman M, Valabregue R, Perlbarg V, Marrakchi-Kacem L, Vidailhet M, Benali H, et al. Parkinson's disease patients show reduced cortical-subcortical sensorimotor connectivity. Mov Disord. 2013;28(4):447–54. doi:10.1002/mds.25255.
Carlesimo GA, Piras F, Assogna F, Pontieri FE, Caltagirone C, Spalletta G. Hippocampal abnormalities and memory deficits in Parkinson disease: a multimodal imaging study. Neurology. 2012;78(24):1939–45. doi:10.1212/WNL.0b013e318259e1c5.
Rae CL, Correia MM, Altena E, Hughes LE, Barker RA, Rowe JB. White matter pathology in Parkinson's disease: the effect of imaging protocol differences and relevance to executive function. Neuroimage. 2012;62(3):1675–84. doi:10.1016/j.neuroimage.2012.06.012.
Deng B, Zhang Y, Wang L, Peng K, Han L, Nie K, et al. Diffusion tensor imaging reveals white matter changes associated with cognitive status in patients with Parkinson's disease. Am J Alzheimers Dis Other Demen. 2013;28(2):154–64. doi:10.1177/1533317512470207.
Surdhar I, Gee M, Bouchard T, Coupland N, Malykhin N, Camicioli R. Intact limbic-prefrontal connections and reduced amygdala volumes in Parkinson's disease with mild depressive symptoms. Parkinsonism Relat Disord. 2012;18(7):809–13. doi:10.1016/j.parkreldis.2012.03.008.
Gallagher C, Bell B, Bendlin B, Palotti M, Okonkwo O, Sodhi A, et al. White matter microstructural integrity and executive function in Parkinson's disease. J Int Neuropsychol Soc. 2013;19(3):349–54. doi:10.1017/S1355617712001373.
Kamagata K, Motoi Y, Tomiyama H, Abe O, Ito K, Shimoji K, et al. Relationship between cognitive impairment and white-matter alteration in Parkinson's disease with dementia: tract-based spatial statistics and tract-specific analysis. Eur Radiol. 2013. doi:10.1007/s00330-013-2775-4.
Ford AH, Duncan GW, Firbank MJ, Yarnall AJ, Khoo TK, Burn DJ, et al. Rapid eye movement sleep behavior disorder in Parkinson's disease: Magnetic resonance imaging study. Mov Disord Off J Mov Disord Soc. 2013;23(7):1946–55. doi:10.1002/mds.25367.
Tsukamoto K, Matsusue E, Kanasaki Y, Kakite S, Fujii S, Kaminou T, et al. Significance of apparent diffusion coefficient measurement for the differential diagnosis of multiple system atrophy, progressive supranuclear palsy, and Parkinson's disease: evaluation by 3.0-T MR imaging. Neuroradiology. 2012;54(9):947–55.
Agosta F, Pievani M, Svetel M, Jecmenica Lukic M, Copetti M, Tomic A, et al. Diffusion tensor MRI contributes to differentiate Richardson's syndrome from PSP-parkinsonism. Neurobiol Aging. 2012;33(12):2817–26. doi:10.1016/j.neurobiolaging.2012.02.002.
Haller S, Badoud S, Nguyen D, Garibotto V, Lovblad KO, Burkhard PR. Individual detection of patients with Parkinson disease using support vector machine analysis of diffusion tensor imaging data: initial results. AJNR Am J Neuroradiol. 2012;33(11):2123–8. doi:10.3174/ajnr.A3126.
Nair SR, Tan LK, Mohd Ramli N, Lim SY, Rahmat K, Mohd Nor H. A decision tree for differentiating multiple system atrophy from Parkinson's disease using 3-T MR imaging. Eur Radiol. 2013. doi:10.1007/s00330-012-2759-9.
Whitwell JL, Xu J, Mandrekar J, Gunter JL, Jack Jr CR, Josephs KA. Imaging measures predict progression in progressive supranuclear palsy. Mov Disord. 2012;27(14):1801–4. doi:10.1002/mds.24970.
Saini J, Bagepally BS, Sandhya M, Pasha SA, Yadav R, Pal PK. In vivo evaluation of white matter pathology in patients of progressive supranuclear palsy using TBSS. Neuroradiology. 2012;54(7):771–80. doi:10.1007/s00234-011-0983-7.
Lu CF, Soong BW, Wu HM, Teng S, Wang PS, Wu YT. Disrupted cerebellar connectivity reduces whole-brain network efficiency in multiple system atrophy. Mov Disord. 2013;28(3):362–9. doi:10.1002/mds.25314.
•• Cochrane CJ, Ebmeier KP. Diffusion tensor imaging in Parkinsonian syndromes: a systematic review and meta-analysis. Neurology. 2013;80(9):857–64. doi:10.1212/WNL.0b013e318284070c. This systematic review and meta-analysis describes many of the important diffusion MRI studies that predated those described in Table 1 and describes a significant effect size for decreased FA in the SN in PD patients compared with controls.
Sherer TB. Biomarkers for Parkinson's disease. Sci Transl Med. 2011;3(79):79ps14. doi:10.1126/scitranslmed.3002488.
Menke RA, Scholz J, Miller KL, Deoni S, Jbabdi S, Matthews PM, et al. MRI characteristics of the substantia nigra in Parkinson's disease: a combined quantitative T1 and DTI study. Neuroimage. 2009;47(2):435–41. doi:10.1016/j.neuroimage.2009.05.017.
Menke RA, Jbabdi S, Miller KL, Matthews PM, Zarei M. Connectivity-based segmentation of the substantia nigra in human and its implications in Parkinson's disease. Neuroimage. 2010;52(4):1175–80. doi:10.1016/j.neuroimage.2010.05.086.
Vaillancourt DE, Spraker MB, Prodoehl J, Abraham I, Corcos DM, Zhou XJ, et al. High-resolution diffusion tensor imaging in the substantia nigra of de novo Parkinson disease. Neurology. 2009;72(16):1378–84. doi:10.1212/01.wnl.0000340982.01727.6e.
Vaillancourt DE, Spraker MB, Prodoehl J, Zhou XJ, Little DM. Effects of aging on the ventral and dorsal substantia nigra using diffusion tensor imaging. Neurobiol Aging. 2012;33(1):35–42. doi:10.1016/j.neurobiolaging.2010.02.006.
Boska MD, Hasan KM, Kibuule D, Banerjee R, McIntyre E, Nelson JA, et al. Quantitative diffusion tensor imaging detects dopaminergic neuronal degeneration in a murine model of Parkinson's disease. Neurobiol Dis. 2007;26(3):590–6. doi:10.1016/j.nbd.2007.02.010.
Skorpil M, Soderlund V, Sundin A, Svenningsson P. MRI diffusion in Parkinson’s disease: using the technique’s inherent directional information to study the olfactory bulb and substantia nigra. J Park Dis. 2012;2(2):171–80. doi:10.3233/JPD-2012-12091.
Martin WR, Wieler M, Gee M. Midbrain iron content in early Parkinson disease: a potential biomarker of disease status. Neurology. 2008;70(16 Pt 2):1411–7. doi:10.1212/01.wnl.0000286384.31050.b5.
•• Du G, Lewis MM, Styner M, Shaffer ML, Sen S, Yang QX, et al. Combined R2* and diffusion tensor imaging changes in the substantia nigra in Parkinson's disease. Mov Disord. 2011;26(9):1627–32. doi:10.1002/mds.23643. This study combined diffusion MRI with R2* imaging and showed abnormalities in both measures in the SN, with combined measures showing the greatest sensitivity and specificity in distinguishing patients from controls. Further, the two measures were not correlated, suggesting they might represent different pathological processes in PD.
Fahn S, Jankovic J, Hallett M. Principles and practice of movement disorders. 2nd ed. Edinburgh: Saunders; 2011.
Horovitz SG, Ford A, Najee-Ullah MA, Ostuni JL, Hallett M. Anatomical correlates of blepharospasm. Transl Neurodegener. 2012;1(1):12. doi:10.1186/2047-9158-1-12.
van der Meer JN, Beukers RJ, van der Salm SM, Caan MW, Tijssen MA, Nederveen AJ. White matter abnormalities in gene-positive myoclonus-dystonia. Mov Disord. 2012;27(13):1666–72. doi:10.1002/mds.25128.
Cheng FB, Wan XH, Feng JC, Ma LY, Hou B, Feng F, et al. Subcellular distribution of THAP1 and alterations in the microstructure of brain white matter in DYT6 dystonia. Parkinsonism Relat Disord. 2012;18(8):978–82. doi:10.1016/j.parkreldis.2012.05.008.
Delmaire C, Dumas EM, Sharman MA, van den Bogaard SJ, Valabregue R, Jauffret C, et al. The structural correlates of functional deficits in early Huntington's disease. Hum Brain Mapp. 2012;34(9):2141–53. doi:10.1002/hbm.22055.
Di Paola M, Luders E, Cherubini A, Sanchez-Castaneda C, Thompson PM, Toga AW, et al. Multimodal MRI analysis of the corpus callosum reveals white matter differences in presymptomatic and early Huntington's disease. Cereb Cortex. 2012;22(12):2858–66. doi:10.1093/cercor/bhr360.
Van Camp N, Blockx I, Camon L, de Vera N, Verhoye M, Veraart J, et al. A complementary diffusion tensor imaging (DTI)-histological study in a model of Huntington's disease. Neurobiol Aging. 2012;33(5):945–59. doi:10.1016/j.neurobiolaging.2010.07.001.
Dumas EM, van den Bogaard SJ, Ruber ME, Reilman RR, Stout JC, Craufurd D, et al. Early changes in white matter pathways of the sensorimotor cortex in premanifest Huntington's disease. Hum Brain Mapp. 2012;33(1):203–12. doi:10.1002/hbm.21205.
Georgiou-Karistianis N, Gray MA, Dominguez DJ, Dymowski AR, Bohanna I, Johnston LA, et al. Automated differentiation of pre-diagnosis Huntington's disease from healthy control individuals based on quadratic discriminant analysis of the basal ganglia: the IMAGE-HD study. Neurobiol Dis. 2013;51:82–92. doi:10.1016/j.nbd.2012.10.001.
Matsui JT, Vaidya JG, Johnson HJ, Magnotta VA, Long JD, Mills JA, et al. Diffusion weighted imaging of prefrontal cortex in prodromal Huntington's disease. Hum Brain Mapp. 2013. doi:10.1002/hbm.22273.
Marrakchi-Kacem L, Delmaire C, Guevara P, Poupon F, Lecomte S, Tucholka A, et al. Mapping cortico-striatal connectivity onto the cortical surface: a new tractography-based approach to study Huntington disease. PloS One. 2013;8(2):e53135. doi:10.1371/journal.pone.0053135.
Buijink AW, Caan MW, Tijssen MA, Hoogduin JM, Maurits NM, van Rootselaar AF. Decreased cerebellar fiber density in cortical myoclonic tremor but not in essential tremor. Cerebellum. 2013;12(2):199–204. doi:10.1007/s12311-012-0414-2.
• Neychev VK, Gross RE, Lehericy S, Hess EJ, Jinnah HA. The functional neuroanatomy of dystonia. Neurobiol Dis. 2011;42(2):185–201. doi:10.1016/j.nbd.2011.01.026. This review describes current thinking regarding the neuroanatomic substrates of dystonia, and provides as a critical appraisal of the evidence from pathology, imaging (including diffusion MRI), and physiologic studies.
• Zoons E, Booij J, Nederveen AJ, Dijk JM, Tijssen MA. Structural, functional and molecular imaging of the brain in primary focal dystonia—a review. Neuroimage. 2011;56(3):1011–20. doi:10.1016/j.neuroimage.2011.02.045. This extensive review focuses on the role of neuroimaging specifically in focal dystonia, and includes descriptions of many of the important studies published prior to those listed in Table 2.
Niethammer M, Carbon M, Argyelan M, Eidelberg D. Hereditary dystonia as a neurodevelopmental circuit disorder: evidence from neuroimaging. Neurobiol Dis. 2011;42(2):202–9. doi:10.1016/j.nbd.2010.10.010.
Carbon M, Kingsley PB, Su S, Smith GS, Spetsieris P, Bressman S, et al. Microstructural white matter changes in carriers of the DYT1 gene mutation. Ann Neurol. 2004;56(2):283–6. doi:10.1002/ana.20177.
Carbon M, Kingsley PB, Tang C, Bressman S, Eidelberg D. Microstructural white matter changes in primary torsion dystonia. Mov Disord. 2008;23(2):234–9. doi:10.1002/mds.21806.
• Ulug AM, Vo A, Argyelan M, Tanabe L, Schiffer WK, Dewey S, et al. Cerebellothalamocortical pathway abnormalities in torsinA DYT1 knock-in mice. Proc Natl Acad Sci U S A. 2011;108(16):6638–43. doi:10.1073/pnas.1016445108. This animal model of dystonia study is important because it demonstrated cerebellothalamic diffusion MRI changes in mutants compared with controls that correlated with measures of cortical metabolic activity, somewhat similar to the findings of Argyelan et al. [27].
Colosimo C, Pantano P, Calistri V, Totaro P, Fabbrini G, Berardelli A. Diffusion tensor imaging in primary cervical dystonia. J Neurol Neurosurg Psychiatry. 2005;76(11):1591–3. doi:10.1136/jnnp.2004.056614.
Fabbrini G, Pantano P, Totaro P, Calistri V, Colosimo C, Carmellini M, et al. Diffusion tensor imaging in patients with primary cervical dystonia and in patients with blepharospasm. Eur J Neurol. 2008;15(2):185–9. doi:10.1111/j.1468-1331.2007.02034.x.
Bonilha L, de Vries PM, Vincent DJ, Rorden C, Morgan PS, Hurd MW, et al. Structural white matter abnormalities in patients with idiopathic dystonia. Mov Disord. 2007;22(8):1110–6. doi:10.1002/mds.21295.
Bonilha L, de Vries PM, Hurd MW, Rorden C, Morgan PS, Besenski N, et al. Disrupted thalamic prefrontal pathways in patients with idiopathic dystonia. Parkinsonism Relat Disord. 2009;15(1):64–7. doi:10.1016/j.parkreldis.2008.01.018.
Delmaire C, Vidailhet M, Wassermann D, Descoteaux M, Valabregue R, Bourdain F, et al. Diffusion abnormalities in the primary sensorimotor pathways in writer's cramp. Arch Neurol. 2009;66(4):502–8. doi:10.1001/archneurol.2009.8.
Simonyan K, Tovar-Moll F, Ostuni J, Hallett M, Kalasinsky VF, Lewin-Smith MR, et al. Focal white matter changes in spasmodic dysphonia: a combined diffusion tensor imaging and neuropathological study. Brain. 2008;131(2):447–59. doi:10.1093/brain/awm303.
Blood AJ. New hypotheses about postural control support the notion that all dystonias are manifestations of excessive brain postural function. Biosci Hypotheses. 2008;1(1):14–25. doi:10.1016/j.bihy.2008.01.006.
Blood AJ, Tuch DS, Makris N, Makhlouf ML, Sudarsky LR, Sharma N. White matter abnormalities in dystonia normalize after botulinum toxin treatment. Neuroreport. 2006;17(12):1251–5. doi:10.1097/01.wnr.0000230500.03330.01.
Georgiou-Karistianis N, Scahill R, Tabrizi SJ, Squitieri F, Aylward E. Structural MRI in Huntington's disease and recommendations for its potential use in clinical trials. Neurosci Biobehav Rev. 2013;37(3):480–90. doi:10.1016/j.neubiorev.2013.01.022.
Paulsen JS, Langbehn DR, Stout JC, Aylward E, Ross CA, Nance M, et al. Detection of Huntington's disease decades before diagnosis: the Predict-HD study. J Neurol Neurosurg Psychiatry. 2008;79(8):874–80. doi:10.1136/jnnp.2007.128728.
Tabrizi SJ, Reilmann R, Roos RA, Durr A, Leavitt B, Owen G, et al. Potential endpoints for clinical trials in premanifest and early Huntington's disease in the TRACK-HD study: analysis of 24 month observational data. Lancet Neurol. 2012;11(1):42–53. doi:10.1016/S1474-4422(11)70263-0.
Kloppel S, Henley SM, Hobbs NZ, Wolf RC, Kassubek J, Tabrizi SJ, et al. Magnetic resonance imaging of Huntington's disease: preparing for clinical trials. Neuroscience. 2009;164(1):205–19. doi:10.1016/j.neuroscience.2009.01.045.
Rosas HD, Koroshetz WJ, Chen YI, Skeuse C, Vangel M, Cudkowicz ME, et al. Evidence for more widespread cerebral pathology in early HD: an MRI-based morphometric analysis. Neurology. 2003;60(10):1615–20.
Mascalchi M, Lolli F, Della Nave R, Tessa C, Petralli R, Gavazzi C, et al. Huntington disease: volumetric, diffusion-weighted, and magnetization transfer MR imaging of brain. Radiology. 2004;232(3):867–73. doi:10.1148/radiol.2322030820.
Reading SA, Yassa MA, Bakker A, Dziorny AC, Gourley LM, Yallapragada V, et al. Regional white matter change in pre-symptomatic Huntington's disease: a diffusion tensor imaging study. Psychiatry Res. 2005;140(1):55–62. doi:10.1016/j.pscychresns.2005.05.011.
Rosas HD, Tuch DS, Hevelone ND, Zaleta AK, Vangel M, Hersch SM, et al. Diffusion tensor imaging in presymptomatic and early Huntington's disease: selective white matter pathology and its relationship to clinical measures. Mov Disord. 2006;21(9):1317–25. doi:10.1002/mds.20979.
Seppi K, Schocke MF, Mair KJ, Esterhammer R, Weirich-Schwaiger H, Utermann B, et al. Diffusion-weighted imaging in Huntington's disease. Mov Disord. 2006;21(7):1043–7. doi:10.1002/mds.20868.
Magnotta VA, Kim J, Koscik T, Beglinger LJ, Espinso D, Langbehn D, et al. Diffusion tensor imaging in preclinical Huntington's disease. Brain Imaging Behav. 2009;3(1):77–84. doi:10.1007/s11682-008-9051-2.
Stoffers D, Sheldon S, Kuperman JM, Goldstein J, Corey-Bloom J, Aron AR. Contrasting gray and white matter changes in preclinical Huntington disease: an MRI study. Neurology. 2010;74(15):1208–16. doi:10.1212/WNL.0b013e3181d8c20a.
Rosas HD, Lee SY, Bender AC, Zaleta AK, Vangel M, Yu P, et al. Altered white matter microstructure in the corpus callosum in Huntington's disease: implications for cortical "disconnection". Neuroimage. 2010;49(4):2995–3004. doi:10.1016/j.neuroimage.2009.10.015.
Muller HP, Glauche V, Novak MJ, Nguyen-Thanh T, Unrath A, Lahiri N, et al. Stability of white matter changes related to Huntington's disease in the presence of imaging noise: a DTI study. PLoS Curr. 2011;3, RRN1232. doi:10.1371/currents.RRN1232.
Bohanna I, Georgiou-Karistianis N, Sritharan A, Asadi H, Johnston L, Churchyard A, et al. Diffusion tensor imaging in Huntington's disease reveals distinct patterns of white matter degeneration associated with motor and cognitive deficits. Brain Imaging Behav. 2011;5(3):171–80. doi:10.1007/s11682-011-9121-8.
• Esmaeilzadeh M, Ciarmiello A, Squitieri F. Seeking brain biomarkers for preventive therapy in Huntington disease. CNS Neurosci Ther. 2011;17(5):368–86. doi:10.1111/j.1755-5949.2010.00157.x. This review highlights the neuroimaging literature (including diffusion MRI) and details the findings of previous studies aimed at developing imaging-based potential biomarkers for HD, and includes an interesting figure highlighting potential biomarkers according to each period of disease progression.
Weaver KE, Richards TL, Liang O, Laurino MY, Samii A, Aylward EH. Longitudinal diffusion tensor imaging in Huntington's disease. Exp Neurol. 2009;216(2):525–9. doi:10.1016/j.expneurol.2008.12.026.
Sritharan A, Egan GF, Johnston L, Horne M, Bradshaw JL, Bohanna I, et al. A longitudinal diffusion tensor imaging study in symptomatic Huntington's disease. J Neurol Neurosurg Psychiatry. 2010;81(3):257–62. doi:10.1136/jnnp.2007.142786.
Della Nave R, Ginestroni A, Tessa C, Giannelli M, Piacentini S, Filippi M, et al. Regional distribution and clinical correlates of white matter structural damage in Huntington disease: a tract-based spatial statistics study. AJNR Am J Neuroradiol. 2010;31(9):1675–81. doi:10.3174/ajnr.A2128.
Kloppel S, Draganski B, Golding CV, Chu C, Nagy Z, Cook PA, et al. White matter connections reflect changes in voluntary-guided saccades in pre-symptomatic Huntington's disease. Brain. 2008;131(1):196–204. doi:10.1093/brain/awm275.
Tan L, Yu JT, Tan L. The kynurenine pathway in neurodegenerative diseases: mechanistic and therapeutic considerations. J Neurol Sci. 2012;323(1–2):1–8. doi:10.1016/j.jns.2012.08.005.
Blockx I, Van Camp N, Verhoye M, Boisgard R, Dubois A, Jego B, et al. Genotype specific age related changes in a transgenic rat model of Huntington's disease. Neuroimage. 2011;58(4):1006–16. doi:10.1016/j.neuroimage.2011.07.007.
Rizk-Jackson A, Stoffers D, Sheldon S, Kuperman J, Dale A, Goldstein J, et al. Evaluating imaging biomarkers for neurodegeneration in pre-symptomatic Huntington's disease using machine learning techniques. Neuroimage. 2011;56(2):788–96. doi:10.1016/j.neuroimage.2010.04.273.
Bohanna I, Georgiou-Karistianis N, Hannan AJ, Egan GF. Magnetic resonance imaging as an approach towards identifying neuropathological biomarkers for Huntington's disease. Brain Res Rev. 2008;58(1):209–25. doi:10.1016/j.brainresrev.2008.04.001.
Ross CA, Tabrizi SJ. Huntington's disease: from molecular pathogenesis to clinical treatment. Lancet Neurol. 2011;10(1):83–98. doi:10.1016/S1474-4422(10)70245-3.
Martinelli P, Rizzo G, Manners D, Tonon C, Pizza F, Testa C, et al. Diffusion-weighted imaging study of patients with essential tremor. Mov Disord. 2007;22(8):1182–5. doi:10.1002/mds.21287.
Shin DH, Han BS, Kim HS, Lee PH. Diffusion tensor imaging in patients with essential tremor. AJNR Am J Neuroradiol. 2008;29(1):151–3. doi:10.3174/ajnr.A0744.
Nicoletti G, Manners D, Novellino F, Condino F, Malucelli E, Barbiroli B, et al. Diffusion tensor MRI changes in cerebellar structures of patients with familial essential tremor. Neurology. 2010;74(12):988–94. doi:10.1212/WNL.0b013e3181d5a460.
Jia L, Jia-Lin S, Qin D, Qing L, Yan Z. A diffusion tensor imaging study in essential tremor. J Neuroimaging. 2011;21(4):370–4. doi:10.1111/j.1552-6569.2010.00535.x.
Klein JC, Lorenz B, Kang JS, Baudrexel S, Seifried C, van de Loo S, et al. Diffusion tensor imaging of white matter involvement in essential tremor. Hum Brain Mapp. 2011;32(6):896–904. doi:10.1002/hbm.21077.
Elble RJ. What is essential tremor? Curr Neurol Neurosci Rep. 2013;13(6):353. doi:10.1007/s11910-013-0353-4.
Brunenberg EJ, Moeskops P, Backes WH, Pollo C, Cammoun L, Vilanova A, et al. Structural and resting state functional connectivity of the subthalamic nucleus: identification of motor STN parts and the hyperdirect pathway. PloS One. 2012;7(6):e39061. doi:10.1371/journal.pone.0039061.
Sedrak M, Gorgulho A, Frew A, Behnke E, DeSalles A, Pouratian N. Diffusion tensor imaging and colored fractional anisotropy mapping of the ventralis intermedius nucleus of the thalamus. Neurosurgery. 2011;69(5):1124–9. doi:10.1227/NEU.0b013e3182296a42. discussion 1129-30.
Kincses ZT, Szabo N, Valalik I, Kopniczky Z, Dezsi L, Klivenyi P, et al. Target identification for stereotactic thalamotomy using diffusion tractography. PloS One. 2012;7(1):e29969. doi:10.1371/journal.pone.0029969.
Pouratian N, Zheng Z, Bari AA, Behnke E, Elias WJ, Desalles AA. Multi-institutional evaluation of deep brain stimulation targeting using probabilistic connectivity-based thalamic segmentation. J Neurosurg. 2011;115(5):995–1004. doi:10.3171/2011.7.JNS11250.
Elias WJ, Zheng ZA, Domer P, Quigg M, Pouratian N. Validation of connectivity-based thalamic segmentation with direct electrophysiologic recordings from human sensory thalamus. Neuroimage. 2012;59(3):2025–34. doi:10.1016/j.neuroimage.2011.10.049.
Sudhyadhom A, McGregor K, Okun MS, Foote KD, Trinastic J, Crosson B, et al. Delineation of motor and somatosensory thalamic subregions utilizing probabilistic diffusion tractography and electrophysiology. J Magn Reson Imaging. 2013;37(3):600–9. doi:10.1002/jmri.23861.
Henderson JM. "Connectomic surgery": diffusion tensor imaging (DTI) tractography as a targeting modality for surgical modulation of neural networks. Front Integr Neurosci. 2012;6:15. doi:10.3389/fnint.2012.00015.
• Klein JC, Barbe MT, Seifried C, Baudrexel S, Runge M, Maarouf M, et al. The tremor network targeted by successful VIM deep brain stimulation in humans. Neurology. 2012;78(11):787–95. doi:10.1212/WNL.0b013e318249f702. This study used probabilistic tractography to demonstrate structural connectivity between effective thalamic stimulation sites and areas of the brain known to be part of a tremor-generating network. This network was consistent across patients and was consistent with prior functional imaging studies and animal models.
Weir DW, Sturrock A, Leavitt BR. Development of biomarkers for Huntington's disease. Lancet Neurol. 2011;10(6):573–90. doi:10.1016/S1474-4422(11)70070-9.
Acknowledgments
Christopher W. Hess has received fellowship funding from the Parkinson’s Disease Foundation. Michael S. Okun has received research grants from the National Institutes of Health, the National Parkinson Foundation, the Michael J. Fox Foundation, the Parkinson Alliance, the Smallwood Foundation, the Bachmann-Strauss Dystonia & Parkinson Foundation, the Tourette Syndrome Association, the Dystonia Medical Research Foundation, and the University of Florida Foundation. David E. Vaillancourt has received grant support from the National Institutes of Health, the Michael J. Fox Foundation, the Bachmann-Strauss Dystonia & Parkinson Foundation, and Tyler’s Hope for a Dystonia Cure.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Christopher W. Hess, Edward Ofori, and Umer Akbar declare that they have no conflict of interest.
Michael S. Okun serves as a consultant for the National Parkinson Foundation. He has received royalties for publications with Demos, Manson, Amazon, and Cambridge University Press (movement disorders books). He has participated in continuing medical education activities on movement disorders sponsored by the University of South Florida’s continuing medical education office, PeerView, and Vanderbilt University. The institution and not Michael Okun receives grants from Medtronic and ANS/St. Jude, and Michael Okun has no financial interest in these grants. He has participated as a site principal investigator and/or co-investigator for several National Institutes of Health, foundation, and industry sponsored trials over the years, but has not received honoraria.
David E. Vaillancourt consults for projects at the University of Texas Southwestern Medical Center, the University of Illinois, and Great Lakes NeuroTechnologies.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Neuroimaging
Rights and permissions
About this article
Cite this article
Hess, C.W., Ofori, E., Akbar, U. et al. The Evolving Role of Diffusion Magnetic Resonance Imaging in Movement Disorders. Curr Neurol Neurosci Rep 13, 400 (2013). https://doi.org/10.1007/s11910-013-0400-1
Published:
DOI: https://doi.org/10.1007/s11910-013-0400-1