
Abstract
Purpose of Review
To summarise the advances that have been made from 2017 in dual, triple, and quadruple low-dose combination therapy for treating high blood pressure.
Recent Findings
Many people require multiple blood pressure lowering medicines to achieve target blood pressures, and initiating treatment with combination blood pressure lowering therapy is being increasingly investigated and recommended. Low-dose combinations of blood pressure lowering provide more effective blood pressure lowering, with fewer adverse events. Recent advances include listing of four dual combinations on the WHO Essential Medicines List, completion of a triple half-dose combination trial, and a pilot of quadruple quarter-dose combination, and recent cardiovascular polypill trials have included two blood pressure lowering medicines at low dose. These trials all demonstrated improvements in achieving blood pressure targets with low-dose combination therapy.
Summary
Low-dose combination therapy is a promising option for initial treatment of hypertension that appears to be safe and effective. Larger trials of triple and quadruple low-dose combination therapy in multiple locations are underway and should provide stronger evidence of efficacy as well as information on the side effect profile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High blood pressure, hypertension, remains the leading modifiable risk factor for the global burden of disease and disability [1], with significant gaps in awareness, treatment, and control in all regions and World Bank income levels [2, 3]. Despite many blood pressure lowering medicines available, with the majority being off-patent and manufactured as generics, there are significant barriers in terms of availability, affordability, and use of these medicines globally [4].
Previously, hypertension treatment guidelines have recommended initiating treatment with a single blood pressure lowering agent at standard dose, with up-titration to maximal dose before adding a second agent. However, single agents at a standard dose achieve an average reduction of 9.1 mmHg [5•], which for many is insufficient to achieve control. Globally, the PURE study found that most participants being treated are on monotherapy (69.2%), and less than a third of those treated achieve blood pressure control < 140/90 mmHg [2]. This treatment-control gap highlights the importance of initiating effective treatment that will achieve the blood pressure reduction necessary to control hypertension.
Combination therapy is an efficient method for achieving blood pressure reductions. Though historically used for those who did not meet blood pressure targets on monotherapy, there is increasing investigation of, and recommendation for, initial treatment of high blood pressure with low-dose combination therapy. This strategy involves using multiple blood pressure lowering classes at doses below the usual standard dose. Dose-response studies show that singly half-standard doses achieve approximately 80% of the efficacy of a standard dose with fewer adverse events for thiazides, beta-blockers, and calcium channel blockers and no difference for ACE inhibitors (ACE-I) and no adverse events in angiotensin II receptor blockers (ARB) [5•]. An additive effect is seen when combining agents from different classes [5•], which allows better blood pressure lowering than doubling the dose.
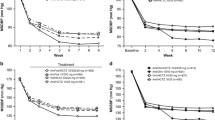
Our goal with this review is to summarise the advances that have been made from 2017 in dual, triple, and quadruple low-dose combinations for treating high blood pressure. We have followed the method described by Bennett et al. to classify standard and low doses [6]. Briefly, a standard dose was defined as the most frequently reported maintenance dose in the British National Formulary, Martindale: The Complete Drug Reference, and the Monthly Index of Medical Specialties. The World Health Organization Defined Daily Dose was used as a tiebreaker when needed. Low doses are those which are less than a standard dose. We have summarised the placebo-controlled estimates of SBP reduction (Fig. 1) from a single quarter up to dual combinations over a standard dose [5•, 6, 7••, 8, 9].

Placebo-controlled SBP lowering of combinations and doses of BP drugs. * Estimates derived from 1 RCT
* Estimates derived from 1 RCT
Recent Developments
Dual Combination
Salam et al. published a systematic review of 33 studies of initial treatment with dual combination therapy [8]. Dual low-dose combination (both components less than a standard dose) provided slightly better SBP reductions to standard dose monotherapy (− 2.8; 95% CI − 4.0 to − 1.6 mmHg), with similar effect to monotherapy on DBP (− 0.7; 95% CI − 1.5 to 0.1 mmHg). There was evidence of a dose-response in BP reduction up to dual standard dose, but higher doses did not provide additional benefit. The dual low-dose combinations also showed no greater risk of withdrawals due to adverse events (RR 0.98, 95% CI 0.45 to 2.16) nor dizziness (RR 1.02; 95% CI 0.51 to 2.04) compared with standard dose monotherapy.
The systematic review of quarter-dose therapy from Bennett et al. demonstrated that a combination of two quarter standard doses was not significantly different to a single standard dose for BP reduction (SBP 1.3 mmHg, 95% CI − 0.4 to 3.0 mmHg; DBP − 0.3 mmHg, 95% CI − 1.2 to 0.7 mmHg) but had lower risk of adverse events (RR 0.66, 95% CI 0.63 to 0.82) [6].
The World Health Organization Essential Medicines List (EML) also now includes a square box listing for four types of single-pill dual combinations, lisinopril plus amlodipine, lisinopril plus hydrochlorothiazide, telmisartan plus amlodipine, and telmisartan plus hydrochlorothiazide [10, 11••]. This square box listing indicates that class substitutions for both components are recognised as having similar efficacy and safety, highlighting the importance of dual therapy for achieving greater blood pressure reductions. Many governments rely on the EML to guide their purchases to care for their populations, and so this is an important step to improving access to effective treatment.
Triple Combination
A recent addition to the evidence of low-dose combinations for initial treatment is the TRIUMPH study, a trial of a fixed-dose triple versus usual care [12]. The key characteristics of the TRIUMPH study population were that it included 700 people from Sri Lanka with a mean age of 56 years, mean baseline SBP/DBP 154/90, 29% with diabetes and 59% not on BP lowering therapy prior to randomisation. Follow-up was completed in 2017, and the triple pill increased the proportion achieving target blood pressure at 6 months (70% vs 55%). In line with the overall result, those with initial treatment with the triple pill were more likely to experience BP control at 6 months compared with those with usual care (RR 1.25; 95% CI 1.08 to 1.44). More trials of low-dose triple pills are underway, so there may be more information about their use in initial treatment of high blood pressure in the coming 3 years.
Quadruple Combination
The publication of the quadpill double-blind placebo-controlled crossover trial provided new evidence of the benefit of quadruple quarter-dose combination for initial treatment of high blood pressure. Twenty-one people with newly diagnosed hypertension were randomly allocated to quadpill then placebo or placebo followed by quadpill with a fortnight washout between treatments. The quadpill effectively reduced BP with a difference of 22.4 mmHg office SBP (95% CI 16.5 to 28.3 mmHg) and 13.1 mmHg DBP (95% CI 8.9 to 17.3) between the active and placebo periods [7••]. All participants achieved blood pressure control with active treatment. Additional studies of ultra-low dose quadruple combination in comparison with best-practice usual care are underway in Australia and the USA and may provide further insights into the efficacy and safety (Australian New Zealand Clinical Trials Registry ACTRN12616001144404; clinicaltrials.gov NCT03640312).
Cardiovascular Polypill
The recently published cardiovascular polypill studies have included low-dose combinations of blood pressure lowering medicines. Most recently, the polypill versus usual care trial in people without cardiovascular disease from Muñoz et al. included three blood pressure lowering agents all at half-standard dose [13]. This study was conducted in a federally qualified community health centre in AL, USA. Ninety-six percent of participants were black, and three quarters reported annual income below $15,000 (USD; below poverty threshold for a 2-person household). Mean baseline blood pressure was 140/83 mmHg. The polypill group’s mean SBP was 7 mmHg lower than the control group [13]. PolyIran was a cluster randomised controlled trial conducted in 236 villages in the Golestan Province of Iran. Half the participants were female, and 95% never smoked. The investigators compared a polypill versus minimal care in people with and without cardiovascular disease [14••]. The initial polypill contained a half-dose thiazide plus quarter-dose ACE-I, with participants experiencing cough swapped to a second polypill with half-dose thiazide plus half-dose ARB. Mean blood pressure at baseline was 131/79 mmHg. At 24 months, the polypill group’s mean SBP was 3.05 mmHg lower than the minimal care group, and at 60 months, no significant difference remained [14••].
Individual participant data meta-analysis from the SPACE collaboration, including 3140 people from the UK, Ireland, the Netherlands, India, Australia, and New Zealand participating in three trials, showed that the polypill recipients were more likely to achieve target blood pressure (using 2016 ESC guidelines) at 12 months than those receiving usual care (RR 1.08; 95% CI 1.02–1.05) [15]. Prescribing physicians had a choice of two polypills, one had dual half-dose combination of ACE-I and thiazide and the other a half-dose ACE-I and standard dose beta-blocker. Mean baseline blood pressure was139/79 mmHg. Mean SBP was 2.5 mmHg lower in the polypill group versus usual care at 12 months [16].
Observations and Controversies
What Should Be in the Combination?
A common question is why a particular drug was used, or not used, in the combination being tested. There are different schools of thought, but many would now support the notion that in the common drug classes, ACE/ARB, CCBs, thiazides, and BBs, the drugs within class have similar blood pressure lowering efficacy and side effect profiles, though drugs within a class may differ on some pharmacodynamic properties, e.g. half-life. Most recent hypertension drug combination studies start with a base of an ARB. It seems common that local preferences drive the choice of components in the studies originating from various countries. That is, there are different preferences for particular blood pressure lowering medicines within each class in different countries, and so the components of a combination, which may appear ideal in one location and population, may not be the best option elsewhere. The dynamics of a particular drug also come into play such as a longer half-life which is desirable to enable once a day dosing, and there are also stability considerations of mixing components.
How Can I Deliver This for My Patients?
While research studies have examined combinations of common drugs which are available in some form on many markets, currently in most parts of the world it is difficult to find existing products that meet the single-pill low-dose combination therapy concepts tested in trials [17,18,19]. In some parts of the world, low-dose dual combinations are on the market and have been available for some time [20]. Single-pill dual therapies of standard doses are more available in some markets, and its expected costs will reduce as a flow-on from listing on the EML. Some pharmacies provide over-encapsulation services for individuals to deliver personalised medicine, but this can be costly. Providing low-dose combination therapy as multiple low-dose or split tablets is a simpler option to prescribe and may be provided by some pharmacies in dose administration aids but can face higher costs and increased pill burden for patients.
How Do I Up-Titrate Medications If They Are on Multiple Drug Low-Dose Combination?
Concern is often raised about up-titration when patients are on low-dose combination. If using multiple low-dose or split tablets to achieve combination therapy, prescribing a higher dose of one component is straight forward. If using a single-pill combination, up-titration could be achieved either through increasing the dose prescribed (i.e. going from dual quarter-dose therapy to dual half-dose therapy) or adding a second tablet.
How Will I Know Which Medication Is Causing Side Effects If They Are on Multi-Drug Combinations?
Side effect symptoms can be drug-specific, such as a cough commonly associated with ACE-I. It can be difficult to attribute to a specific drug, and it may require switching to the components of medications and withdrawing one component at a time to determine this.
What If I Need to Stop Some Components of the Combination and Not Others?
If using a single-pill combination, this could be achieved swapping to another option without that specific component, for example, swapping from an ACE-I plus calcium channel blocker to an ARB plus calcium channel blocker combination. If using multiple tablets, you would follow your usual process for stopping components.
What Time of the Day Should Low-Dose Combination Therapy Be Taken?
The best time of day to take low-dose combination therapy is the time that will facilitate adherence; this will be different for different people. Integrating new medicines into existing routine can ensure that they are taken regularly. Components of low-dose combination therapy are often selected for longer half-life to ensure efficacy across the day. Although there has been recent discussion of bedtime versus morning dosing and reduction of cardiovascular event risk, further research is needed to determine if there is true benefit.
Is There a First Dose Effect?
A first dose effect has not been reported in existing low-dose combination studies.
What About Using Divided Doses?
The benefit of a single-pill combination is the simplicity for dosing and adherence, and dividing doses provides more opportunity for doses to be missed.
Conclusion
Low dose combination therapy is a promising option for initial treatment of hypertension. It is an approach that in recent studies appears to be both effective and safe in the short and longer term management of hypertension. The increased efficacy of low-dose combination is appealing, but the ability to demonstrate a better side effect profile compared with existing approaches could be the clincher. Meta-analysis of dual low-dose combination shows that it is slightly more effective than single standard dose on SBP reduction, with no difference on adverse events [8]. Low-dose triple combination was more effective than usual care for blood pressure control for initial treatment in one study in Sri Lanka [12]. Another Australian study of quadruple quarter-dose combination therapy showed it to be effective [7••]. However larger trials of triple and quadruple low-dose combination therapy in multiple locations are underway and should provide stronger evidence of efficacy as well as information on side effect profile.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Gakidou E, Afshin A, Abajobir AA, Abate KH, Abbafati C, Abbas KM, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. 2017 2017/09/16/;390(10100):1345–1422.
Chow CK, Teo KK, Rangarajan S, Islam S, Gupta R, Avezum A, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310(9):959–68.
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–50.
Khatib R, McKee M, Shannon H, Chow C, Rangarajan S, Teo K, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries: an analysis of the PURE study data. Lancet. 2016;387(10013):61–9.
• Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427 Law (2003) an impactful publication at the turn of the century which has been key to the development of low-dose combination trials.
Bennett A, Chow CK, Chou M, Dehbi H-M, Webster R, Salam A, et al. Efficacy and safety of quarter-dose blood pressure–lowering agents. Hypertension. 2017;70(1):85–93.
•• Chow CK, Thakkar J, Bennett A, Hillis G, Burke M, Usherwood T, et al. Quarter-dose quadruple combination therapy for initial treatment of hypertension: placebo-controlled, crossover, randomised trial and systematic review. The Lancet. 2017;389(10073):1035–42 Chow (2017) and Bennett (2017) the Quadpill trial and quarter-dose systematic review have further opened a promising line of research into quadruple combinations of quarter doses which is being pursued through ongoing trials in Australia and USA.
Salam A, Kanukula R, Atkins E, Wang X, Islam S, Kishore SP, et al. Efficacy and safety of dual combination therapy of blood pressure-lowering drugs as initial treatment for hypertension: a systematic review and meta-analysis of randomized controlled trials. J Hypertens. 2019.
Wald DS, Morris JK, Wald NJ. Randomized polypill crossover trial in people aged 50 and over. PLoS One. 2012;7(7):e41297.
World Health Organisation. WHO Model List of Essential Medicines. 21st ed ed2019 [cited 18 Sep 2019]. Available.
•• Salam A, Kanukula R, Esam H, Bahiru E, Sharma A, Heller D, et al. An application to include blood pressure lowering drug fixed dose combinations to the model list of essential medicines lists for the treatment of essential hypertension in adults2019: Available from: https://www.who.int/selection_medicines/committees/expert/22/s12_FDC-antihypertensives-28Jan.pdf.Salam(2019) this application and subsequent listing of dual-combination therapies on the WHO EML will help facilitate access, and affordability, and help close treatment-control gaps globally.
Webster R, Salam A, de Silva H, et al. Fixed low-dose triple combination antihypertensive medication vs usual care for blood pressure control in patients with mild to moderate hypertension in Sri Lanka: a randomized clinical trial. JAMA. 2018;320(6):566–79.
Muñoz D, Uzoije P, Reynolds C, Miller R, Walkley D, Pappalardo S, et al. Polypill for cardiovascular disease prevention in an underserved population. N Engl J Med. 2019;381(12):1114–23.
•• Roshandel G, Khoshnia M, Poustchi H, Hemming K, Kamangar F, Gharavi A, et al. Effectiveness of polypill for primary and secondary prevention of cardiovascular diseases (PolyIran): a pragmatic, cluster-randomised trial. The Lancet. 2019;394(10199):672–83 Muñoz (2019) and Roshandel (2019) two major polypill studies which highlight the utility and efficacy of single-pill combinations in low-resource settings. Whilst the US study showed reductions in LDL-C and SBP at 12 months, PolyIran followed participants for 5 years to demonstrate reductions in major cardiovascular events.
Selak V, Webster R, Stepien S, Bullen C, Patel A, Thom S, et al. Reaching cardiovascular prevention guideline targets with a polypill-based approach: a meta-analysis of randomised clinical trials. Heart. 2019;105(1):42–8.
Webster R, Patel A, Selak V, Billot L, Bots ML, Brown A, et al. Effectiveness of fixed dose combination medication (‘polypills’) compared with usual care in patients with cardiovascular disease or at high risk: a prospective, individual patient data meta-analysis of 3140 patients in six countries. Int J Cardiol. 2016;205:147–56.
Salam A, Atkins ER, Hsu B, Webster R, Patel A, Rodgers A. Efficacy and safety of triple versus dual combination blood pressure-lowering drug therapy: a systematic review and meta-analysis of randomized controlled trials. J Hypertens. 2019.
Volpe M, Gallo G, Tocci G. New approach to blood pressure control: triple combination pill. Trends Cardiovasc Med. 2020 2020/02/01/;30(2):72–77.
NPS MedicineWise. New dual and triple antihypertensive combinations PBS listed — be aware of potential confusion. RADAR. 2010: Available from: https://www.nps.org.au/radar/articles/new-dual-and-triple-antihypertensive-combinations-pbs-listed-be-aware-of-potential-confusion#.
U.S. Food and Drug Administration. FDA-Approved Drugs: NDA 020186. 2020 [2020 Apr 14]. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=020186
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Atkins reports grants from National Heart Foundation Australia, during the conduct of the study; grants from National Heart Foundation Australia, outside the submitted work; and George Health Enterprises Pty Ltd. (GHE) and its subsidiary, George Medicines Pty Ltd., and has received investment funds to develop fixed-dose combination products, including combinations of blood pressure-lowering drugs. GHE is the social enterprise arm of Dr. Atkins’ employer, The George Institute for Global Health. Dr. Chow reports grants from NHMRC, during the conduct of the study. In addition, Dr. Chow has a patent compositions for the treatment of hypertension pending.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Antihypertensive Agents: Mechanisms of Drug Action
Rights and permissions
About this article

Cite this article
Atkins, E.R., Chow, C.K. Low-Dose Combination Therapy for Initial Treatment of Hypertension. Curr Hypertens Rep 22, 65 (2020). https://doi.org/10.1007/s11906-020-01069-7
Published:
DOI: https://doi.org/10.1007/s11906-020-01069-7