
Abstract
Purpose of Review
Prevalence and outcome differences between women and men with pulmonary arterial hypertension (PAH) raise questions about the role of sex hormones in disease pathobiology. This review will summarize the current understanding of sex and sex hormone pathways and their influence on heart-lung function in health and in disease.
Recent Findings
Female sex has been shown to be a risk factor for the development of PAH, but women have improved survival compared to men with PAH. These paradoxical observations are likely driven in part by complex sex hormone signaling and processing pathways and their interaction with the pulmonary vasculature and the right ventricle. These relationships may vary depending on an individual’s underlying sex, age, and/or genetic substrate.
Summary
The study of the connections between sex, sex hormones, the pulmonary circulation, and the right ventricle may improve our understanding of disease epidemiology and outcomes and lead to new treatment strategies for PAH.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Female sex is the best-established clinical risk factor for pulmonary arterial hypertension (PAH). Recent population-based studies have demonstrated that while women are more likely to develop PAH then men, men have worse outcomes compared to their opposite sex counterparts. Sex and sex hormones appear to play an important role in pulmonary hypertension (PH) pathogenesis in animal models, but with inconsistent results that vary with experimental conditions. These contradictory human and animal observations, dubbed the “estrogen paradox” of pulmonary vascular disease, have led to increased interest in the study of sexual dimorphism in PAH and right ventricular (RV) failure. Defining sex-based phenotypes and the role of sex hormones in cardiopulmonary function may lead to novel therapeutic strategies including hormonal manipulation in PAH. Here, we will review current evidence from clinical and translational studies implicating sex and sex hormones in disease epidemiology, outcomes, and key mechanisms of PAH pathobiology. Leading hypotheses, including the importance of estrogen, its aromatization (conversion of androgens into estrogens), metabolism and signaling in the pulmonary circulation, and links between sex hormone pathways and RV function will be summarized. Gaps in our understanding of the estrogen paradox and areas for future research will also be highlighted (Fig. 1).

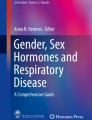
Sex hormone biosynthesis and effects in the diseased right ventricle and lung vasculature. An abbreviated biosynthetic pathway shows the key enzymes and intermediates connecting dehydroepiandrosterone (DHEA), testosterone (T), estradiol (E2), and the estrogen metabolite 16-hydroxy-estrone (16-OH-E1). Collagen and elastin staining of the fibrosis in the diseased right ventricle (left photomicrograph). The thick arrow shows abnormal accumulation of extracellular fibrosis, whereas the thin arrows illustrate capillaries within the myocytes. Original magnification, ×40. The opposing actions of DHEA and testosterone on the diseased right ventricle are illustrated (see text for supporting references); direct effects of estradiol on the diseased right ventricle seem less clear. Hematoxylin and eosin staining of a plexiform-like lesion from a diseased female rat (right photomicrograph). Original magnification, ×60. The opposing effects of DHEA and estradiol within the lung vasculature are illustrated; similarly, the direct effects of testosterone within the vasculature are also less clear. 3-β-OH-steroid-DH 3-β-hydroxysteroid dehydrogenase, 17-β-OH-steroid-DH 17-β-hydroxysteroid dehydrogenase, BMPR2 bone morphogenetic protein receptor-2, CYP1B1 cytochrome P450 1B1 (reprinted with permission of the American Thoracic Society. Copyright© 2016 American Thoracic Society. R. James White “Estrogen: Friend or Foe in Pulmonary Hypertension?” American Journal of Respiratory and Critical Care Medicine, Vol. 193, No. 10 (2016), pp. 1084–1086. The American Journal of Respiratory and Critical Care Medicine is an official journal of the American Thoracic Society.)
Sex-Based Differences in PAH Prevalence
The earliest modern description of idiopathic pulmonary arterial hypertension (IPAH) by Dresdale et al. [1] in 1951 included three young women with disease. In the 1980s, the National Institutes of Health (NIH) established the first multicenter registry before the advent of targeted PAH therapies and demonstrated a 1.7:1 female/male ratio [2]. Similar female/male biases have been noted in more recent registries throughout many parts of the world, including the USA, UK, Spain, China, and France [3–6, 7•, 8–14, 15•, 16–25] (Table 1). A large European registry which enrolled patients from 2007 to 2011 (the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension [COMPERA]) demonstrated a 1.8:1 female/male ratio; however, this female predominance was strongest among younger patients: the female/male ratio was 2.3:1 among 18–65-year-olds but just 1.2:1 in those older than 65 [7•]. This finding raises the question of whether age (and temporal changes in the hormonal milieu over the life cycle) is an important modifier of the relationship between sex and PAH risk.
The Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL), the largest US registry to date, reported a more pronounced sex bias than had been observed in other registries; 80 % of patients enrolled between 2006 and 2007 were women [15•]. Whether the observations from REVEAL signal a true change in disease biology (e.g., via epigenetic factors) and/or a significant survival bias conferred by female sex because of a predominantly prevalent (versus incident) study population is not known. In China, where targeted PAH therapies have only recently become available, their earliest registry containing incident (i.e., untreated) patients demonstrated a female/male ratio of 2.4:1 and 71 % of patients were women, similar to the US NIH registry [2, 17]. This is in contrast to a follow-up Chinese study which reported a ratio of 3.1:1 female/male patients and 76 % women from a treated/prevalent cohort, similar to REVEAL [24].
The epidemiology of heritable PAH is similar to that of IPAH, and women are roughly twice as likely to be affected as men [27]. In a large cohort of individuals with bone morphogenetic protein type II (BMPR2) receptor mutations (including those with IPAH, heritable, and drug- and toxin-induced PAH), roughly 70 % of the population were women [28]. As we discuss below, cross talk between BMPR2 (the major genetic mutation of heritable PAH) and estrogen signaling has been proposed as an important mechanistic driver responsible for female predominance in pulmonary vascular disease.
Beyond idiopathic and heritable PAH, other World Health Organization (WHO) Group 1 PAH subgroups are characterized by female predominance, including connective tissue disease (CTD) and portopulmonary hypertension-associated PAH. CTD itself occurs more commonly in women than in men; when associated with PAH, female/male ratios between 3.8:1 and 10:1 have been reported [6, 14, 15•, 24, 26]. Women with systemic sclerosis are eight times more likely than men with systemic sclerosis to be affected by PAH [29]. In patients with systemic lupus erythematosus, women are 17 times more likely to be affected with PAH than men [6].
Female sex is also a risk factor for the development of portopulmonary hypertension. The French Registry reported that 40 % of patients with portopulmonary hypertension were women [14]. Although this ratio is tipped toward male sex, it is higher than expected because the prevalence of female sex overall in portal hypertension is low. In a prospective cohort of patients with chronic liver disease, the pulmonary vascular complications of liver disease (PVCLD) investigators demonstrated that female sex is an independent risk factor for the development of portopulmonary hypertension and increases the risk nearly 3-fold (adjusted odds ratio 2.90, 95 % confidence interval [CI] 1.2–7.01, p = 0.018) [30]. This has been confirmed in other registries including the REVEAL registry [11, 14, 30]. In other conditions associated with WHO Group 1 PAH, including human immunodeficiency virus infection and congenital heart disease, sex does not appear to be a risk factor, raising the question of whether sex hormones can be implicated in all forms of PAH.
Sex-Based Differences in Outcome
Although female sex is clearly a risk factor for the development of PAH, longitudinal observations from modern registries have shown that women have increased survival as compared to men with PAH. In 2010, both the French [31•] and US REVEAL [13] registries published similar findings and found male sex to double the risk of death in PAH. This risk was shown to be independent of commonly held disease surrogates such as the 6-min walk distance (6MWD) and cardiac index [13, 20, 31•]. Updated survival data from the REVEAL registry in 2012 and 2015 continue to demonstrate an increased risk of death in men compared to women, but this finding was only in individuals aged 60 years and older [32], which suggests that age-related changes in the hormonal milieu may impact risk throughout the lifespan. The 2015 REVEAL update looked at survival 5 years from enrollment and continued to demonstrate significant differences in outcome based on sex. These differences were noted irrespective of whether the PAH diagnosis was incident or prevalent, such that 5-year survival estimates for newly diagnosed (incident) men were 53 ± 4 versus 63 ± 2 % for women and 57 ± 2 versus 68 ± 1 % for previously diagnosed (prevalent) men versus women [10]. Limited data suggests that male sex confers a higher risk of death in specific WHO Group 1 subtypes. For example, Chung et al. demonstrated an almost 4-fold increase in the risk of death (hazard ratio 3.9, 95 % CI 1.1–13.9, p = 0.03) among men as compared to women with PAH associated with systemic sclerosis [33].
Age-Sex Interaction
Hormonal changes throughout a person’s lifecycle (e.g., puberty, menarche, menopause, waning androgen levels with aging) may impact pulmonary vascular and RV function. These influences may manifest as interactions between sex, age, and epidemiologic observations in PAH. Limitations of current registries make it difficult to define the impact of age on sex-based differences in PAH prevalence, incidence, and outcome, however.
In a large study (n = 1211) of patient-level pooled data from 11 clinical trials in PAH, we examined the associations between sex and baseline hemodynamic measures (which are markers of disease burden tied to survival) and found that women with idiopathic and CTD-associated PAH had more favorable hemodynamic indices (lower right atrial pressure [RAP], lower pulmonary vascular resistance [PVR], higher cardiac index) as compared to men with idiopathic and CTD-associated PAH [34]. Younger men had higher mean pulmonary arterial pressure (mPAP) than younger women, but this difference was attenuated after age 45 years. In both men and women with idiopathic PAH, hemodynamic burden tended to decrease with age.
Similar observations have been made in the COMPERA registry, which demonstrated a strong female predominance among younger patients with PAH that dissipated after age >65 [7•]. As in our study, in REVEAL, male sex was associated with higher RAP and mPAP at diagnosis and overall men had worse survival, especially in older age [13, 32]. Benza et al. identified age >60 years in males as a significant negative predictor of outcome in REVEAL, which was then validated as part of a risk stratification equation [13]. In a follow-up study, Shapiro and colleagues stratified the REVEAL cohort by age at enrollment and found poorer 2-year survival among older males (>60 years of age) and worse hemodynamics in men in general [32]. While there are some inconsistencies across studies, these results support the theory that sex hormones may play a role in PAH pathogenesis and that changes in the hormonal milieu caused by aging may impact disease epidemiology.
Differences in Right Ventricular Function by Sex
Since the RV is the proximate cause of death in PAH, sex- or sex hormone-driven influences on RV function may explain why more women develop PAH yet have improved survival as compared to men. Until recently, there have been significant knowledge gaps in our understanding of RV structure and function in both health and disease. Studying the RV in health may inform studies in PAH (and other causes of right heart failure) and our understanding of changes in RV adaptation during different stages of disease and across the lifespan.
Multi-Ethnic Study of Atherosclerosis (MESA)-RV is the largest population-based, cardiovascular disease-free cohort with available RV indices measured via cardiac magnetic resonance imaging, the gold standard for assessment of the RV. Female sex was associated with higher right ventricular ejection fraction (RVEF), lower RV mass, and smaller RV volumes after adjustment for multiple comorbid factors and body size in MESA-RV [34, 35]. These sex-based differences in RVEF and volumes were recently recapitulated in the Framingham Heart Study Offspring cohort [36]. Both the MESA and Framingham studies have shown age to be an important modifier of the relationships between sex and measures of RV morphology [34–36].
Sex appears to be a unique determinant of RV structure and function in health, which begs the question whether sex hormone pathways are associated with RV phenotype. Higher estradiol (E2) levels were associated with higher RVEF and lower RV end-systolic volume in post-menopausal women using hormone therapy in MESA-RV, but this relationship did not persist in non-hormone therapy users or men [37]. In men, higher levels of testosterone were associated with higher RV stroke volume and greater RV mass and higher dehydroepiandrosterone (DHEA) levels tracked with greater volumes and mass in both sexes [37]. Using this same study population, we demonstrated that genetic variation in CYP1B1 (the major enzyme responsible for E2 metabolism) was associated with increased RVEF in post-menopausal women [38•]. This polymorphism was tightly linked to variants that increase the risk of PAH in BMPR2 carriers [39•] and angioinvasion in cancer [40–43]. In men from MESA-RV, two polymorphisms in the androgen receptor gene were associated with RV end-diastolic volume and mass and these relationships were dependent on circulating testosterone levels, indicating that these variants may have biological relevance [38•]. Taken together, these observations lend support to the hypothesis that sex hormones may have pleiotropic effects on the pulmonary circulation and RV that may change based on an individual’s sex, age, and/or genetic predisposition, giving rise to unique sex-based phenotypes in pulmonary vascular disease.
The RV has not been robustly studied in PAH, and less is known about sex-based differences in the RV response to increased pulmonary afterload. Changes in RV structure and function with PAH therapies are strongly tied to survival in PAH, more so than changes in PVR [44–46]. Kawut et al. demonstrated that male sex was associated with lower RVEF (measured by radionuclide angiography) in PAH [47]. Among a cohort of 101 patients with idiopathic, heritable, or anorexigen-associated PAH, men and women had similar reductions in PVR but RVEF declined in men and improved in women over time with PAH therapies. A significant proportion (39 %) of the transplant-free survival difference seen between men and women was explained by treatment-related improvements in RVEF [48•], suggesting the survival bias conferred by female sex in PAH may be explained by sex- or sex hormone-mediated effects on the RV.
Differences in Response to PAH Treatments by Sex
Limited evidence suggests that treatment response to targeted PAH therapies may vary according to sex. Major molecular pathways implicated in PAH and targeted by available PAH therapies (e.g., nitric oxide [NO], endothelin) are influenced by sex and sex hormones. For example, women have greater levels of NO biosynthesis compared to men, while men have higher levels of circulating endothelin-1 (ET-1) and greater ET-1-mediated vasoconstriction compared to women [49–51]. Sex hormones have also been shown to directly modulate NO signaling pathways and circulating ET-1 levels [52–54]. A patient-level pooled analyses of six randomized placebo-controlled trials of endothelin receptor antagonists (ERAs) showed that women had a 30-m greater improvement in 6MWD on active treatment as compared to men treated with ERAs [55]. Conversely, Mathai et al. showed that men treated with tadalafil, a phosphodiesterase type 5 inhibitor targeting the NO pathway, were more likely to meet the minimally important difference in 6MWD and improve the physical component of a health-related quality-of-life score than women treated with tadalafil [56]. While these studies raise interesting questions about potential treatment response heterogeneity according to sex, further studies are needed to confirm these observations and to understand the mechanisms that may explain these findings.
Sex Hormones and Disease Pathobiology
Numerous experimental studies in various PH models have implicated sex and sex hormones in pulmonary vascular disease pathobiology. While beyond the scope of this discussion, these preclinical studies are discussed in depth in a recent review by Lahm et al. [57•]. Current proposed hypotheses to explain the estrogen paradox of PAH include mechanisms related to sex hormone metabolism, aromatization, and receptor signaling and their interaction with an individual’s genetic substrate, the BMPR2 pathway, and the RV.
Few clinical studies have tied estrogen (and other hormones) to known mechanistic pathways in PAH. Mutations in BMPR2, a member of the transforming growth factor [TGF]-β family, are present in 70–80 % of families with PAH and roughly 25 % of patients with IPAH [58, 59]. These mutations are transmitted in an autosomal dominant fashion with incomplete penetrance, and with a significant female predominance. TGF-β signaling including the BMPR2 pathway is felt to play a major role in disease pathogenesis.
Only recently have we come to understand the relationships between BMPR2 signaling and sex hormones. E2 is metabolized by cytochrome P4501B1 to two major metabolites (2-hydroxyestrone [2-OHE]) and 16α-hydroxysterone [16α-OHE1]) which have different effects on inflammation and mitogenesis and have previously been implicated in cancer of the gonadal organs [60]. Austin and colleagues discovered alterations in E2 metabolism in heritable PAH and demonstrated that a CYP1B1 polymorphism increased the risk of PAH penetrance in female, but not male, BMPR2 carriers [39•]. This polymorphism is linked to the variant associated with RV function in healthy women from MESA [38•]. In addition, the presence of the CYP1B1 mutation in PAH patients was associated with a more mitogenic E2 metabolite profile as measured in the urine [39•, 61, 62]. This same group described direct estrogen receptor alpha binding to the BMPR2 promoter, which leads to reduced BMPR2 gene expression in females [61]. This important connection may be a major driver underlying the female predominance of idiopathic and heritable PAH, but more work is needed to understand the contributions of estrogen receptors (and signaling of other sex hormones) in disease pathogenesis.
Roberts et al. demonstrated that genetic variation in sex hormone pathways is associated with an increased risk of portopulmonary hypertension in patients with severe liver disease (the PVCLD cohort) [63]. Polymorphisms in genes encoding for estrogen receptor 1 and aromatase (the enzyme responsible for testosterone to E2 conversion) were associated with the odds of developing portopulmonary hypertension. Moreover, biologic activity of the aromatase variants was suggested by a correlation between increased circulating E2 levels and genotype [63]. More recently, we have demonstrated that men with idiopathic, heritable, or CTD-associated PAH have higher levels of E2 and lower levels of DHEA-sulfate compared to age- and body mass index-matched healthy controls [64•]. High E2 and low DHEA-sulfate levels were associated with the risk of PAH, such that a 1-unit increase in E2 increased the risk of PAH 50-fold, and this hormone profile was associated with markers of disease severity. Specifically, higher E2 levels were associated with shorter 6MWD (p = 0.03), whereas higher levels of DHEA-sulfate were associated with lower RAP (p = 0.02) and PVR (p = 0.01) in men with PAH [64•]. These studies strongly implicate sex hormone processing and signaling in pulmonary vascular disease risk.
Recent work has shown that aromatase (which accounts for most of the estrogen production in post-menopausal women and men) is produced in the smooth muscle cells of the small muscular pulmonary arteries of both experimental PH and women with PAH [65, 66]. Administration of the aromatase inhibitors anastrozole and metformin reduced pulmonary arterial pressures, pulmonary vascular changes, and indices of RV hypertrophy in animal models [65–67]. A recently completed randomized, double-blind, placebo-controlled trial demonstrated a significant reduction in circulating E2 levels with anastrozole treatment versus placebo but no effect on echocardiographic RV measures at 12 weeks in 18 subjects with WHO Group 1 PAH [68•]. Active treatment also resulted in an improvement in 6MWD (+26 m) compared to placebo (−12 m) (median % change from baseline was +8 versus −2 %, respectively [p = 0.042]), and there were no adverse events. This pilot study demonstrates the feasibility of hormonal manipulation as a treatment strategy in PAH, but larger and longer studies are needed to confirm these results.
Conclusions
While there has been much progress in our understanding of the sex paradox of PAH, there are continued major knowledge gaps. Unmet needs in the field include defining how age impacts epidemiologic observations and how temporal changes in sex hormones across the life cycle and stages of disease affect the cardiopulmonary interaction. Better characterization of sex- or sex hormone-based phenotypes may guide prognosis as well as more precise treatment regimens with currently available agents (e.g., PDE5i and ERAs, based on sex-based treatment responses) or future treatments that impact the hormonal milieu or the RV response directly. While the focus thus far has been on the study of women (and female sex hormones), future work should elucidate the role of androgens in pulmonary vascular and RV dysfunction and include men with PAH, who may represent a more severe phenotype from whom we can gain further insights. Finally, additional mechanisms of sexual dimorphism should be explored, such as the role of inflammation and immune function regulation (known to be regulated by sex hormones) in PAH and RV failure.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Dresdale DT, Schultz M, Michtom RJ. Primary pulmonary hypertension: I. Clinical and hemodynamic study. Am J Med. 1951;11(6):688–705.
Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Primary pulmonary hypertension. Ann Intern Med. 1987;107(216–223).
Olsson KM, Delcroix M, Ghofrani HA, Tiede H, Huscher D, Speich R, et al. Anticoagulation and survival in pulmonary arterial hypertension: results from the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA). Circulation. 2014;129(1):57–65.
Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JS, et al. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension: results from the pulmonary hypertension registry of the United Kingdom and Ireland. Am J Respir Crit Care Med. 2012;186(8):790–6.
Frost AE, Badesch DB, Barst RL, Elliott CG, Farber HW, Krichman A, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest. 2011;139(1):128–37.
Chung L, Liu J, Parsons L, Hassoun PM, McGoon M, Badesch DB, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138(6):1383–94.
• Hoeper MM, Huscher D, Ghofrani HA, Delcroix M, Distler O, Schweiger C, et al. Elderly patients diagnosed with idiopathic pulmonary arterial hypertension: results from the COMPERA registry. Int J Cardiol. 2013;168(2):871–80. This registry raises interesting questions regarding how age plays a role in the interaction between sex hormones and PAH. The female:male ratio was 2.3:1 among 18–65 year olds but nearly even 1.2:1 among those older than 65.
Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30(1):104–9.
Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest. 2012;142(2):448–56.
Farber HW, Miller DP, Poms AD, Badesch DB, Frost AE, Muros-Le Rouzic E, et al. Five-year outcomes of patients enrolled in the REVEAL Registry. Chest. 2015;148(4):1043–54.
Krowka MJ, Miller DP, Barst RJ, Taichman D, Dweik RA, Badesch DB, et al. Portopulmonary hypertension: a report from the US-based REVEAL Registry. Chest. 2012;141(4):906–15.
Lee WT, Ling Y, Sheares KK, Pepke-Zaba J, Peacock AJ, Johnson MK. Predicting survival in pulmonary arterial hypertension in the UK. Eur Respir J. 2012;40(3):604–11.
Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010;122(2):164–72.
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023–30.
• Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137(2):376–87. This is the largest US PAH registry to date and reported a more pronounced sex bias than other registries. This raises the question whether there has been a true change in disease biology or whether the predominantly prevalent study population skews the bias, especially given a survival bias conferred by female sex.
McGoon MD, Benza RL, Escribano-Subias P, Jiang X, Miller DP, Peacock AJ, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(25 Suppl):D51–9.
Jing ZC, Xu XQ, Han ZY, Wu Y, Deng KW, Wang H, et al. Registry and survival study in Chinese patients with idiopathic and familial pulmonary arterial hypertension. Chest. 2007;132(2):373–9.
Benza RL, Gomberg-Maitland M, Miller DP, Frost A, Frantz RP, Foreman AJ, et al. The REVEAL Registry risk score calculator in patients newly diagnosed with pulmonary arterial hypertension. Chest. 2012;141(2):354–62.
Barst RJ, McGoon MD, Elliott CG, Foreman AJ, Miller DP, Ivy DD. Survival in childhood pulmonary arterial hypertension: insights from Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management. Circulation. 2012;125:113–22.
Humbert M, Sitbon O, Yaici A, Montani D, O’Callaghan DS, Jais X, et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur Respir J. 2010;36(3):549–55.
D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115(5):343–9.
Thenappan T, Shah SJ, Rich S, Tian L, Archer SL, Gomber-Maitland M. Survival in pulmonary arterial hypertension: a reappraisal of the NIH risk stratification equation. Eur Respir J. 2010;35(5):1079–87.
Escribano-Subias P, Blanco I, Lopez-Meseguer M, Lopez-Guarch CJ, Roman A, Morales P, et al. Survival in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir J. 2012;40(3):596–603.
Zhang R, Dai LZ, Xie WP, Yu ZX, Wu BX, Pan L, et al. Survival of Chinese patients with pulmonary arterial hypertension in the modern treatment era. Chest. 2011;140(2):301–9.
Walker AM, Langleben D, Korelitz JJ, Rich S, Rubin LJ, Strom BL, et al. Temporal trends and drug exposures in pulmonary hypertension: an American experience. Am Heart J. 2006;152(3):521–6.
Kane GC, Maradit-Kremers H, Slusser JP, Scott CG, Frantz RP, McGoon MD. Integration of clinical and hemodynamic parameters in the prediction of long-term survival in patients with pulmonary arterial hypertension. Chest. 2011;139(6):1285–93.
Loyd JE, Butler MG, Foroud TM, Conneally PM, Phillips JA, Newman JH. Genetic anticipation and abnormal gender ratio at birth in familial primary pulmonary hypertension. Am J Respir Crit Care Med. 1995;152:93–7.
Evans JD, Girerd B, Montani D, Wang XJ, Galiè N, Austin ED, et al. BMPR2 mutations and survival in pulmonary arterial hypertension: an individual participant data meta-analysis. Lancet Respir Med. 2016;4(2):129–37.
Chung L, Farber HW, Benza R, Miller DP, Parsons L, Hassoun PM, et al. Unique predictors of mortality in patients with pulmonary arterial hypertension associated with systemic sclerosis in the REVEAL registry. Chest. 2014;146(6):1494–504.
Kawut SM, Krowka MJ, Trotter JF, Roberts KE, Benza RL, Badesch DB. Clinical risk factors for portopulmonary hypertension. Hepatology. 2008;48(1):196–203.
• Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122(2):156–63. This study demonstrated male sex to be a risk factor for death within a population of idiopathic, familial, and anorexigen-associated PAH patients in the French PAH registry.
Shapiro S, Traiger GL, Turner M, McGoon MD, Wason P, Barst RJ. Sex differences in the diagnosis, treatment, and outcome of patients with pulmonary arterial hypertension enrolled in the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management. Chest. 2012;141(2):363–73.
Chung L, Domsic RT, Lingala B, Alkassab F, Boster M, Csuka ME, et al. Survival and predictors of mortality in systemic sclerosis-associated pulmonary arterial hypertension: outcomes from the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma Registry. Arthritis Care Res. 2014;66(3):489–95.
Kawut SM, Barr RG, Lima JA, Praestgaard A, Johnson WC, Chahal H, et al. Right ventricular structure is associated with the risk of heart failure and cardiovascular death: the Multi-Ethnic Study of Atherosclerosis (MESA)–Right Ventricle Study. Circulation. 2012;126(14):1681–8.
Kawut SM, LIma JA, Barr RG, Chanal H, Jain A, Tandri H, et al. Sex and race differences in right ventricular structure and function: the Multi-Ethnic Study of Atherosclerosis-Right Ventricle Study. Circulation. 2011;123(22):2542–51.
Foppa M, Arora G, Gona P, Ashrafi A, Salton CJ, Yeon SB, et al. Right ventricular volumes and systolic function by cardiac magnetic resonance and the impact of sex, age, and obesity in a longitudinally followed cohort free of pulmonary and cardiovascular disease: The Framingham Heart Study. Circ Cardiovasc Imaging. 2016;9(3):e003810.
Ventetuolo CE, Ouyang P, Bluemke DA, Tandri H, Barr RG, Bagiella E, et al. Sex hormones are associated with right ventricular structure and function: the MESA-Right Ventricle Study. Am J Respir Crit Care Med. 2011;183(5):659–67.
• Ventetuolo CE, Mitra N, Wan F, Manichaikul A, Barr RG, Johnson C, et al. Oestradiol metabolism and androgen receptor genotypes are associated with right ventricular function. Eur Respir J. 2016;47(2):553–63. This is the first and only genotype-phenotype association study for the right ventricle. Polymorphisms in estradiol metabolism were tied to right ventricular function in healthy post-menopausal women, while genetic variation in the androgen receptor was associated with right heart morphology in healthy men from the Multi-Ethnic Study of Atherosclerosis cohort.
• Austin ED, Cogan JD, West JD, Hedges LK, Hamid R, Dawson EP, et al. Alterations in oestrogen metabolism: implications for higher penetrance of familial pulmonary arterial hypertension in females. Eur Respir J. 2009;34(5):1093–9. This study is the first to link genetic variation in sex hormone genes (CYP1B1, the major enzyme responsible for estradiol metabolism), to penetrance in heritable PAH.
Diergaarde B, Potter JD, Jupe ER, Manjeshwar S, Shimasaki CD, Pugh TW, et al. Polymorphisms in genes involved in sex hormone metabolism, estrogen plus progestin hormone therapy use, and risk of postmenopausal breast cancer. Cancer Epidemiol Biomarkers Prev. 2008;17(7):1751–9.
Kato I, Cichon M, Yee CL, Land S, Korczak JF. African American-preponderant single nucleotide polymorphisms (SNPs) and risk of breast cancer. Cancer Epidemiol. 2009;33(1):24–30.
Paracchini V, Raimondi S, Gram IT, Kang D, Kocabas NA, Kristensen VN, et al. Meta- and pooled analyses of the cytochrome P-450 1B1 Val432Leu polymorphism and breast cancer: a HuGE-GSEC review. Am J Epidemiol. 2007;165(2):115–25.
Wenzlaff AS, Cote ML, Bock CH, Land SJ, Santer SK, Schwartz DR, et al. CYP1A1 and CYP1B1 polymorphisms and risk of lung cancer among never smokers: a population-based study. Carcinogenesis. 2005;26(12):2207–12.
van de Veerdonk MC, Kind T, Marcus JT, Mauritz GJ, Heymans MW, Bogaard HJ, et al. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol. 2011;58(24):2511–9.
van Wolferen SA, van de Veerdonk MC, Mauritz GJ, Jacobs W, Marcus JT, Marques KM, et al. Clinically significant change in stroke volume in pulmonary hypertension. Chest. 2011;139(5):1003–9.
van Wolferen SA, Marcus JT, Boonstra A, Marques KM, Bronzwaer JG, Spreeuwenberg MD, et al. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur Heart J. 2007;28(10):1250–7.
Kawut SM, Al-Naamani N, Agerstrand C, Rosenzweig EB, Rowan C, Barst RJ, et al. Determinants of right ventricular ejection fraction in pulmonary arterial hypertension. Chest. 2009;135(3):752–9.
• Jacobs W, Van de Veerdonk MC, Trip P, de Man F, Heymans MW, Marcus JT, et al. The right ventricle explains sex differences in survival in idiopathic pulmonary arterial hypertension. Chest. 2014;145(6):1230–6. This study demonstrates that PAH treatment-induced changes in right ventricular ejection fraction explain a significant proportion of the survival differences between men and women with PAH.
Forte P, Kneale BJ, Milne E, Chowienczyk PJ, Johnston A, Benjamin N, et al. Evidence for a difference in nitric oxide biosynthesis between healthy women and men. Hypertension. 1998;32(4):730–4.
Miyauchi T, Yanagisawa M, Lida K, Ajisaka R, Suzuki N, Fujino M, et al. Age- and sex-related variation of plasma endothelin-1 concentration in normal and hypertensive subjects. Am Heart J. 1992;123(4):1092–3.
Stauffer BL, Westby CM, Greiner JJ, Van Guilder GP, Desouza CA. Sex differences in endothelin-1-mediated vasoconstrictor tone in middle-aged and older adults. Am J Physiol Regul Integr Comp Physiol. 2010;298(2):R261–5.
Billon-Gales A, Fontaine C, Filipe C, Douin-Echinard V, Fouque MJ, Flouriot G, et al. The transactivating function 1 of estrogen receptor alpha is dispensable for the vasculoprotective actions of 17beta-estradiol. Proc Natl Acad Sci U S A. 2009;106(6):2053–8.
Polderman KH, Stehouwer CD, van Kamp GJ, Dekker GA, Verheugt FW, Gooren LJ. Influence of sex hormones on plasma endothelin levels. Ann Intern Med. 1993;118(6):429–32.
Russell KS, Haynes MP, Sinha D, Clerisme E, Bender JR. Human vascular endothelial cells contain membrane binding sites for estradiol, which mediate rapid intracellular signaling. Proc Natl Acad Sci U S A. 2000;97(11):5930–5.
Gabler NB, French B, Strom BL, Liu Z, Palevsky HI, Taichman DB, et al. Race and sex differences in response to endothelin receptor antagonists for pulmonary arterial hypertension. Chest. 2012;141(1):20–6.
Mathai SC, Hassoun PM, Puhan MA, Zhou Y, Wise RA. Sex differences in response to tadalafil in pulmonary arterial hypertension. Chest. 2015;147(1):188–97.
• Lahm T, Tuder RM, Petrache I. Progress in solving the sex hormone paradox in pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2014;307(1):L7–26. This review article details the preclinical evidence linking sex hormones to pulmonary vascular disease pathobiology.
Deng Z, Morse JH, Slager SL, Cuervo N, Moore KJ, Venetos G, et al. Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-II gene. Am J Hum Genet. 2000;67(3):737–44.
Soubrier F, Chung WK, Machado R, Grunig E, Aldred M, Geraci M, et al. Genetics and genomics of pulmonary arterial hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D13–21.
Dubey RK, Jackson EK, Gillespie DG, Rosselli M, Barchiesi F, Krust A, et al. Cytochromes 1A1/1B1- and catechol-O-methyltransferase-derived metabolites mediate estradiol-induced antimitogenesis in human cardiac fibroblast. J Clin Endocrinol Metab. 2005;90(1):247–55.
Austin ED, Hamid R, Hemnes AR, Loyd JE, Blackwell T, Yu C, et al. BMPR2 expression is suppressed by signaling through the estrogen receptor Biol Sex Differ. 2012;3(1).
White K, Johansen AK, Nilsen M, Ciuclan L, Wallace E, Paton L, et al. Activity of the estrogen-metabolizing enzyme cytochrome P450 1B1 influences the development of pulmonary arterial hypertension. Circulation. 2012;126(9):1087–98.
Roberts KE, Fallon MB, Krowka MJ, Brown RS, Trotter JF, Peter I, et al. Genetic risk factors for portopulmonary hypertension in patients with advanced liver disease. Am J Respir Crit Care Med. 2009;179(9):835–42.
• Ventetuolo CE, Baird GL, Barr RG, Bluemke DA, Fritz JS, Hill NS, et al. Higher estradiol and lower dehydroepiandrosterone-sulfate levels are associated with pulmonary arterial hypertension in men. Am J Respir Crit Care Med. 2016;193(10):1168–75. This is the first study to demonstrate that sex hormone levels are associated with the risk of PAH in men. Surprisingly, high estradiol levels in men (and low dehydroepiandrosterone-sulfate levels) conferred an increased risk of PAH and greater disease severity.
Mair KM, Wright AF, Duggan N, Rowlands DJ, Hussey MJ, Roberts S, et al. Sex-dependent influence of endogenous estrogen in pulmonary hypertension. Am J Respir Crit Care Med. 2014;190(4):456–67.
Wright AF, Ewart MA, Mair K, Nilsen M, Dempsie Y, Loughlin L, et al. Oestrogen receptor alpha in pulmonary hypertension. Cardiovasc Res. 2015;106(2):206–16.
Dean A, Nilsen M, Loughlin L, Salt IP, MacLean MR. Metformin reverses development of pulmonary hypertension via aromatase inhibition. Hypertension. 2016;68(2):446–54.
• Kawut SM, Archer-Chicko CL, Dimichele A, Fritz JS, Klinger RJ, Ky B, et al. Anastrozole in pulmonary arterial hypertension (AIPH): a randomized, double-blind placebo-controlled trial. Am J Respir Crit Care Med. 2016. This randomized control trial showed that anastrazole significantly reduced estradiol levels and improved 6MWD. Although a pilot study, it demonstrates the feasibility of hormonal manipulation as a treatment strategy in PAH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Pulmonary Hypertension
Rights and permissions
About this article

Cite this article
Foderaro, A., Ventetuolo, C.E. Pulmonary Arterial Hypertension and the Sex Hormone Paradox. Curr Hypertens Rep 18, 84 (2016). https://doi.org/10.1007/s11906-016-0689-7
Published:
DOI: https://doi.org/10.1007/s11906-016-0689-7