
Abstract
Medical nutrition therapy plays a major role in diabetes management. Macronutrient composition has been debated for a long time. However, there is increasing evidence that a modest increase in dietary protein intake above the current recommendation is a valid option toward better diabetes control, weight reduction, and improvement in blood pressure, lipid profile, and markers of inflammation. Increasing the absolute protein intake to 1.5–2 g/kg (or 20–30% of total caloric intake) during weight reduction has been suggested for overweight and obese patients with type 2 diabetes and normal kidney function. Increased protein intake does not increase plasma glucose, but increases the insulin response and results in a significant reduction in hemoglobin A1c. In addition, a higher dietary protein intake reduces hunger, improves satiety, increases thermogenesis, and limits lean muscle mass loss during weight reduction using a reduced calorie diet and increased physical activity. It is preferable to calculate protein intake for patients with diabetes as grams per kilogram of body weight and not as a fixed percentage of total energy intake to avoid protein malnutrition when a hypocaloric diet is used. The relationship between protein intake as grams per kilogram of body weight and albumin excretion rate is very weak, except in hypertensive patients and particularly in those with uncontrolled diabetes. A protein intake of 0.8–1 g/kg should be recommended only for patients with diabetes and chronic kidney disease. Other patients with diabetes should not reduce protein intake to less than 1 g/kg of body weight. This review discusses the effects of different amounts of protein intake in a diabetes meal plan. It particular, it discusses the effects of protein intake on renal function, the effects of protein content on diabetes control, and the effects of increased dietary protein on body weight.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Medical nutrition therapy is an important component of the overall diabetes management. Both the total daily caloric intake and the dietary composition have been considered to play major roles in regulating blood glucose levels, improving the lipid profile, preserving renal function, and slowing progression of vascular complications of diabetes.
Before the discovery of insulin, several diets, ranging from what would now be considered to be “fad” diets (oat cure, milk diet, potato therapy) to the “starvation diet” used by Fredrick Allen in his Physiatric Institute had been used to treat diabetes with limited success [1]. The introduction of insulin in 1922 made it possible for patients with type 1 diabetes to better utilize calories and consume diets similar to those of healthy individuals. However, the ideal dietary composition has remained a debated issue.
In the first half of the 20th century, Elliot P. Joslin and others recommended a diet composed of 40% of caloric intake from carbohydrates, 40% from fat, and 20% from protein to all patients with diabetes [2]. This dietary composition was widely accepted by health care professionals as the standard diabetes diet until the late 1970s when a concern was raised about the increased incidence of coronary artery disease among patients with diabetes, which was partially blamed on the excess calories from fat sources. This concern urged the medical community to agree on reducing fat intake to about 30% and saturated fat to less than 10% of the total daily caloric consumption. The recommended decrease in fat intake required a compensatory increase in either carbohydrate or protein intake as percentage of total calories. The legitimate fear of worsening renal function by increasing protein intake led to the final decision to increase carbohydrate content to 50–55% of the total daily caloric intake. Although it might seem harmful to recommend a higher carbohydrate intake to treat a disease principally characterized by carbohydrate intolerance, it was generally considered—at that time—as the best or the safest option compared with maintaining a high caloric intake from fat sources. These changes led to a recommended diet that contains approximately 50–55% of its caloric content from carbohydrates, 30% to 35% from fat, and 15% to 20% from protein.
Over the past several years, a debate about the optimal amount of protein in the diabetes meal plan has emerged. Several clinical trials have shown that increasing dietary protein intake is a valid alternative to increasing carbohydrate intake and could be a better option toward optimal diabetes macronutrients composition. Although many clinicians may agree that carbohydrate intake should be reduced, or at least the type of carbohydrates should be modified, the increase in protein intake remains controversial. This review discusses the effects of different amounts of protein intake in the diabetes meal plan. It particularly discusses the effects of protein intake on renal function, the effects of protein content on diabetes control, and the effects of increased dietary protein on body weight.
Current Protein Recommendation
The American Diabetes Association (ADA) proposed the following recommendations regarding protein intake [3•]:
-
1.
Patients with diabetes and normal renal function should consume between 15% and 20% of their total energy intake from protein. (E)
-
2.
Patients with diabetes and with early stages of chronic kidney disease (CKD) should limit their caloric intake to 0.8 to 1 g/kg per day. (B)
-
3.
Patients with diabetes and later stages of CKD should limit their caloric intake to 0.8 g/kg per day. (B)
-
4.
High-protein diets are not recommended as a method for weight loss at this time. The long-term effects of protein intake greater than 20% of calories on diabetes management and its complications are unknown. Although such diets may produce short-term weight loss and improved glycemia, it has not been established that these benefits are maintained long term, and long-term effects on kidney function for persons with diabetes are unknown. (E)
Readers of these guidelines should observe that the first and the last recommendations are based on expert opinions and are not on rated clinical evidence, which are usually derived from clinical trials.
Protein Intake: How High is High?
It has been confusing to determine what is the exact amount of protein that many nutrition guidelines are recommending. The percentage of protein intake of total calories has been frequently interchanged with the absolute amount of dietary protein expressed as grams per kilogram of body weight. The hazard is that using the percentage value to calculate protein intake in a restricted caloric diet may result in an unintentionally low absolute protein intake. As seen in Table 1, an individual consuming a 2000-kcal diet and weighing 70 kg may eat between 70 and 105 g of protein when absolute protein intake is calculated based on 1–1.5 g/kg of body weight. That amount is equivalent to 14–21% of the total daily calories and is approximately similar to the ADA recommendation. However, if this person uses the same percentage to calculate his protein intake in a 1500-kcal/day diet, it would result in 52–79 g of absolute protein per day. This amount decreases his intake to the moderately low protein category of 0.8–1 g/kg. Such lower absolute protein intake is similar to the ADA recommendation for patients with early CKD. This means that using a fixed percentage of total calories to calculate protein intake rather than grams per kilogram will always result in a lower absolute protein intake for people on a low calorie diet for weight management and may put them at risk for protein malnutrition.
It is logical that future recommendations should use grams per kilogram of body weight instead of using a fixed percentage of calories to calculate protein intake. In this case, if a person decides to follow a low calorie diet plan for weight reduction, the absolute amount of protein will be kept constant and may allow that individual to decrease caloric intake from other sources such as carbohydrates and fat. This may also reduce the risk of lean muscle mass loss during weight reduction and may help in maintaining higher energy expenditure.
In general, the Dietary Reference Intakes of protein among the US population are between 10% and 35% of the total energy intake. Most individuals eat protein in a range between 1 and 1.5 g/kg of body weight and usually this amount does not exceed 20% of total daily caloric intake. The valid question is whether a higher protein intake is safe or valuable for patients with diabetes and normal kidney functions. In other words, is protein intake in the moderately high range (1.5–2 g/kg/day, 20–30% of isocaloric diet) better than protein intake in the current average range (1–1.5 g/kg/day, 15–20% of isocaloric diet)?
Protein Intake and Kidney Function
Until recently, it was an undisputed practice for nephrologists to recommend restriction of protein for patients with CKD. However, the evidence behind these recommendations was generally derived from studies that were limited by small numbers, short follow-up, compliance problems, and failure to adequately assess the nutritional impact of protein restriction.
Low Protein and Progression of Kidney Disease in Diabetic Patients
In type 1 diabetes, many randomized clinical trials (RCTs) showed that reducing protein intake to 0.8 g/kg per day in patients with overt nephropathy decreases proteinuria and reduces the decline in glomerular filtration rate (GFR), the risk of renal failure, and mortality [4–6]. However, very little data are available to support this recommendation in patients with type 2 diabetes. Moreover, there is no evidence to show that increased protein intake is harmful in patients with normal kidney function or that it will induce microalbuminuria or result in a more rapid decline in GFR.
Raal et al. [4] studied the effects of 0.8 g/kg per day of protein restriction over 6 months on patients with type 1 diabetes and overt proteinuria. Proteinuria decreased and GFR stabilized on this reduction of protein intake to 50% of that of their previously unrestricted diet (> 1.6 g/kg/day).
In a meta-analysis of five RCTs of low-protein diet in patients with diabetic nephropathy or nondiabetic kidney disease, protein restriction significantly reduced the risk of kidney failure or death (RR, 0.67; 95% CI, 0.50–0.89) and delayed the need for dialysis [5].
Kasiske et al. [6] pooled 13 RCTs (n = 1919) of protein restriction (mean, 0.7 vs 1.0. g/kg/day) in both diabetic and nondiabetic kidney disease. In the diabetic subgroup, protein restriction had a greater effect on GFR than in the nondiabetic patients, where dietary protein restriction in patients with diabetes reduced the rate of GFR decline by 5.4 mL/min per year. However, the confidence interval of this value was wide (0.3–10.5 mL/min per year).
Although the evidence is convincing for patients with type 1 diabetes, there are little data to show that reducing protein intake slows progression of renal disease in patients with type 2 diabetes who have overt nephropathy. Only Pemerlalu et al. [7], in a randomized crossover trial, showed that a moderate protein intake of 0.8 g/kg per day, compared with a high protein of 2 g/kg per day, improved GFR and decreased proteinuria in patients with type 2 diabetes. However, this study included a very small number of patients. Contrary to this observation, Parving [8] showed no benefit from protein restriction in patients with type 2 diabetes and overt proteinuria.
It has been suggested that the benefit of a low-protein diet on the progression of kidney disease may be related to something other than the restriction of protein. Bellizzi et al. [9] showed a clear benefit of a very low protein diet (VLPD) containing less than 0.6 g/kg of body weight on reducing blood pressure and decreasing proteinuria in patients with end-stage renal disease (stages 4 and 5) compared with a low-protein diet containing 0.8 g/kg of body weight or an unrestricted protein. However, when they adjusted for the total sodium intake, such independent effect of a low-protein intake on blood pressure disappeared. The study concluded that in moderate to advanced CKD, VLPD has an antihypertensive effect likely due to reduction of salt intake independent of the actual protein intake. Similarly, a cross-sectional population-based study of Tasmanian adults with type 1 diabetes showed that the adjusted odds ratio (OR) for microalbuminuria for the highest quintile of energy-adjusted saturated fat intake compared with the lowest quintile was 4.9 (95% CI, 1.2, 20.0; P = 0.03), whereas the adjusted OR for microalbuminuria for the highest quintile of energy-adjusted usual protein intake compared with the lowest quintile was 0.10 (95% CI, 0.02, 0.56; P = 0.01) [10]. These observations taken together indicate that the benefit of a low-protein diet may be partially related to reduced salt intake or reduced saturated fat, as common associations, and may not be related solely to the reduced protein intake.
Effect of a High-Protein Diet on Kidney Function
The EURODIAB IDDM study provided the strongest evidence in support of the current recommendation of lowering protein intake to less than 20% of total daily calories [11]. This cross-sectional clinic-based study was designed to determine the prevalence of renal complications and putative risk factors in 2696 European individuals with type 1 diabetes from 30 centers in 16 European countries. The study examined the relationship between dietary protein intake and urinary albumin excretion rate (AER) through reviewing a standardized 3-day dietary record in relation to 24-hour urinary AER. The study found that in individuals who reported protein consumption less than 20% of total energy intake, mean AER was below 20 μg/min. In those patients whose regular protein consumption exceeded 20% of the total caloric intake, the mean AER increased. This trend was particularly pronounced in individuals with hypertension and/or poor diabetes control. The study findings supported the recommendation that protein intake for patients with diabetes should not exceed 20% of the total energy consumption. It also suggested that monitoring and adjusting dietary protein appears particularly desirable for individuals whose AER exceeds 20 μg/min (~ 30 mg/24 h), especially when arterial blood pressure is high and/or diabetes control is poor.
It may be difficult to take the conclusions of this study literally. Careful reading of this study shows that AER did not increase with increased protein intake in patients with controlled diabetes. It also did not increase in normotensive patients. But more importantly, in normotensive patients with either controlled or uncontrolled diabetes, AER also did not increase with the increased protein intake. It is only in hypertensive patients that AER was high and particularly when hypertension was associated with uncontrolled diabetes. In this respect, the study results provided a clear indication that hypertension, and not protein intake, is associated with increased AER. Interestingly, the study discussion admitted that AER is strongly associated with the presence of hypertension or higher hemoglobin A1c (HbA1c) values, whereas a weaker relationship was seen with dietary protein intake, which clearly contradicts the study conclusions. The study also clearly mentioned that the trend toward a linear relationship between protein intake and AER is not significant for vegetable protein or for absolute protein intake calculated in relation to body weight (gram per kilogram of body weight). Based on a second careful reading of this important study, the conclusion should read “There is a weaker relation between AER and dietary protein intake except in hypertensive patients, particularly in those with uncontrolled diabetes. Monitoring and adjusting of protein intake may be (as the study is cross-sectional) recommended in hypertensive individuals with AER that exceeds 20 μg/min (30 mg/24 h), especially when diabetes control is poor.”
Conversely, among 1624 individuals in the Nurses’ Health Study [12], high-protein intake was not significantly associated with a change in estimated GFR in women with normal renal function (defined as an estimated GFR ≥ 80 mL/min/1.73 m2) . Change in estimated GFR in this subgroup was 0.25 mL/min per 10-g increase in protein intake over an 11-year period (the change in estimated GFR was 1.14 mL/min after measurement error adjustment for protein intake). In women with mild renal insufficiency (defined as an estimated GFR ≥ 55 mL/min/1.73 m2 but < 80 mL/min/1.73 m2), protein intake was significantly associated with a change in estimated GFR of −1.69 mL/min per 10-g increase in protein intake. After measurement error adjustment, the change in estimated GFR was −7.72 mL/min per 10-g increase in protein intake, an association of borderline statistical significance. The study concluded that high-protein intake was not associated with decline in renal function in women with normal renal function. However, high total protein intake, particularly high intake of nondairy animal protein, may accelerate renal function decline in women with mild renal insufficiency. It is worth mentioning that the highest quintile of protein intake in this study was 86.5–163.7 g/day.
Does Type of Protein Matter?
There is some evidence that fish protein reduces progression to microalbuminuria in patients with type 1 diabetes. Möllsten et al. [13], in a nested case control study of 1150 patients with diabetes duration greater than 5 years, reported that a high intake of fish protein and fish fat showed a reduction in the risk of microalbuminuria (OR, 0.22 and 0.31, respectively; 95% CI, 0.09–0.56 and 0.13–0.76, respectively). When fish protein and fat were adjusted for each other, a high intake of fish protein but not of fish fat was still significantly associated with decreased risk of microalbuminuria. Soy protein was also shown to be associated with significant improvement in proteinuria and urinary creatinine among patients with type 2 and diabetic nephropathy [14•].
Protein Intake and Glucose Control
Amino acids derived from protein are converted to glucose in the liver and kidney through gluconeogenesis. As early as 1915, Janney [15] reported that 3.5 g of glucose could be produced from 6.25 g of ingested meat protein. Thus, theoretically, every 100 g of ingested meat protein produces 56 g of glucose. For other proteins the range of glucose production is between 50 and 84 g/100 g.
To study the effect of protein intake on blood glucose, in 1924 MacLean [16] gave 250 g of beef, which contains about 50 g of protein (equivalent to ~ 25 g of glucose), to a subject with type 2 diabetes whose fasting glucose concentration was about 280 mg/dL. He observed that blood glucose did not change for 5 h. When the same subject was given 25 g of glucose—the amount of glucose that theoretically could have been produced from the 50 g of protein in the 250 g of meat—the blood glucose concentration increased to nearly 600 mg/dL.
It was later demonstrated that when normal subjects ingest 50 g of protein, the plasma glucose concentration remains stable during the following 4 h [17]. But when patients with type 2 diabetes ingest the same amount of protein, their blood glucose does not remain stable, but decreases after 2 h [18]. It was shown that the insulin response to protein intake is relatively higher in patients with diabetes compared with normal healthy subjects. In normal subjects, the increase in insulin production was only 30% of the insulin production in response to 50 g of glucose, but in patients with type 2 diabetes, insulin production was equivalent in response to either 50 g of protein or 50 g of glucose. In addition, ingestion of 50 g of beef protein had very little effect on plasma glucose concentration either in normal subjects [19] or in people with type 2 diabetes [20]. From these studies and others, it was concluded that dietary protein is a potent insulin secretagogue in patients with type 2 diabetes. Subsequently, it has been demonstrated that dietary protein acts synergistically with ingested glucose to increase insulin secretion and reduces blood glucose response to the ingested glucose in patients with type 2 diabetes [21].
Gannon et al. [22] studied the effect of substituting protein for carbohydrate in mixed meals over an extended period of time in 12 subjects with untreated type 2 diabetes in a randomized crossover study. Investigators increased protein content from 15% in the control diet to 30% in the test diet. To compensate for the increase in percentage protein, they decreased the carbohydrate content from 55% in the control diet to 40% in the test diet. The fat content remained about 30% in both diets. Both diets were isocaloric to maintain constant body weight. Each diet was consumed for 5 weeks with a washout period in between. The study results showed that integrated 24-hour plasma glucose area was reduced by 38% on the high-protein diet. In spite of the lower integrated glucose area, the integrated insulin area response was increased by 18% when compared with the control (15% protein) diet results. Moreover, with the 30% protein diet, the percentage total glycohemoglobin decreased from 8.1% to 7.3% (Δ = 0.8), whereas it decreased from 8.0% to 7.7% during by the control (15% protein) diet (Δ = 0.3). The difference was statistically significant by week 2.
Although this study included a small number of patients, its results clearly indicate that increasing dietary protein from 15% to 30% of the total energy intake at the expense of carbohydrate may result in an increased 24-hour integrated insulin concentration, a decreased 24-hour integrated glucose concentration, and a decreased HbA1c.
Protein Intake and Weight Reduction
Available data indicate that short-term weight reduction of 7–10% in patients with type 2 diabetes improves insulin sensitivity, endothelial function, and diabetes control and reduces many other risk factors for coronary artery disease [23, 24]. Substantial weight loss (23.4% at 2 years and 16.1% at 10 years after bariatric surgery) has been shown to be associated with diabetes remission in 72% of patients after 2 years and in 36% after 10 years [25].
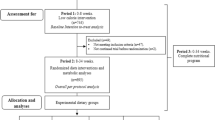
High protein-low carbohydrate energy–restricted diets have started to emerge as an effective tool for weight management in patients with diabetes. In the Why WAIT (Weight Achievement and Intensive Treatment) Program, developed at the Joslin Diabetes Center for diabetes weight management in clinical practice [26••], a high protein-low carbohydrate (30% protein [1.5–2 g/kg] and 40% carbohydrates) energy–restricted diet was tried within a multidisciplinary diabetes weight management program for 12 weeks [27•]. Patients who completed the program lost an average 24.6 ± 10.9 lb (−10.3%, P < 0.001) of their initial body weight. Their waist circumference decreased by 3.6 ± 2.2 in. (P < 0.001) and their HbA1c decreased from 7.5% ± 1.3% to 6.6% ± 0.99% (P < 0.001). Almost 82% achieved the target HbA1c of less than 7% and approximately 70% were able to reduce their HbA1c to less than 6.5%. After approximately 1 year, weight remained lower by 18.2 ± 10.6 lb (−7.6%, P < 0.001) from baseline. Fifty-five percent of participants continued to lose weight and maintained the significantly decreased HbA1c. The remainder 45% gained back more than 5 lb, but their final weight remained lower than baseline by −2%. Systolic and diastolic blood pressure were reduced significantly at both 12 weeks and 1 year (P < 0.01). Other metabolic changes can be seen in Table 2.
At the same degree of weight loss, a high-protein weight-reduction diet may have, in the long term, a more favorable effect on the cardiovascular risk profile than a low-protein weight-reduction diet in patients with type 2 diabetes. Brinkworth et al. [28] studied the long-term weight reduction and health outcomes at 1 year following a 12-week intensive intervention with two diets, which differed in protein content; a low-protein (15% protein, 55% carbohydrate) versus high-protein diet (30% protein, 40% carbohydrate). At week 64, weight reductions compared with baseline were −2.2 ± 1.1 kg (low protein) and −3.7 ± 1.0 kg (high protein) (P < 0.01). At week 12, both diets reduced systolic and diastolic blood pressure by 6 and 3 mm Hg, respectively, but blood pressure increased more with weight regain during follow-up in the low-protein group (P < 0.05). At week 64, both diets significantly increased high-density lipoprotein cholesterol and lowered C-reactive protein concentrations.
Parker et al. [29] compared a high-protein diet (28% protein, 42% carbohydrate, 28% fat [8% saturated fatty acids, 12% monounsaturated fatty acids, 5% polyunsaturated fatty acids]) versus a low-protein diet (16% protein, 55% carbohydrate, 26% fat [8% saturated fatty acids, 11% monounsaturated fatty acids, 5% polyunsaturated fatty acids]) in 54 obese men and women with type 2 diabetes during 8 weeks of energy restriction (1600 kcal) and 4 weeks of energy balance. Although weight loss was achieved independent of the diet composition, women on the high-protein diet lost significantly more total (−5.3 vs −2.8 kg; P = 0.009) and abdominal (−1.3 vs −0.7 kg; P = 0.006) fat compared with those on the low-protein diet. Reduction in low-density lipoprotein (LDL) cholesterol was significantly greater with the high-protein diet (−5.7%) than with the low-protein diet (−2.7%; P < 0.01).
Controlled energy intake, in association with a moderately elevated protein intake, may represent an effective and practical weight loss strategy. Potential beneficial outcomes associated with protein ingestion in patients with diabetes include increased satiety [30], which facilitates reduction in energy consumption under ad libitum dietary conditions; increased thermogenesis and thermic effect of food [31], which also influences satiety and augments energy expenditure (in the longer term, increased thermogenesis contributes to the relatively low-energy efficiency of protein); and enhanced stimulatory effect on muscle protein anabolism, favoring the retention of lean muscle mass [32] while improving metabolic profile. The satiety associated with a higher protein diet may be partially explained by increased concentrations of glucagon-like peptide 1 in response to high protein [33].
Considering kidney function during a high-protein weight-reduction diet, it was observed that both blood urea nitrogen and serum creatinine did not change after 1 year of the Why WAIT intervention [27•]. Meanwhile, albumin/creatinine ratio decreased after 12 weeks and remained significantly lower than baseline after 1 year (P < 0.001) (Fig. 1). Such improvement may be explained by the significant reduction of the blood pressure. However, a recent study showed that the long-term improvement in renal function after weight reduction may not be related to the improvement in GFR, but rather is attributable to the decrease in body mass index and to the improvement of other weight-related metabolic factors [34]. It has been shown that moderate changes in dietary protein intake cause adaptive alterations in renal size and function without adverse effects [35].

Changes in microalbumin/creatinine ratio after 12 weeks and 1 year of intervention using the Why WAIT Program in the diabetes clinical practice
In a 1-year RCT, a high-protein weight-reduction diet was found to have a more favorable cardiovascular risk profile than a low-protein diet with similar weight reduction in people with type 2 diabetes [36]. In the Why WAIT program, C-reactive protein and other markers of inflammation, coagulation, and endothelial dysfunction such as tumor-necrosis factor-α, interleukin-6, plasminogen-activator inhibitor-1, intravascular and intercellular adhesion molecules, and E-selectin were all reduced significantly and adiponectin was nearly doubled. These changes in circulating cytokines indicate a possible reduction in cardiovascular risk [37].
Twenty-one percent of the Why WAIT patients on short-acting insulin were able to stop insulin completely by the end of the program. In the remaining patients on insulin therapy, the daily dose of long-acting analogue insulins was reduced by an average of 55% and the short-acting analogue insulins by 54%. Almost two-thirds of the patients on sulfonylureas were able to stop them, whereas the remaining participants reduced their dose by 35–41%. The average cost saving on diabetes medications was −$561 over a year.
Conclusions
There is strong evidence that a modest increase in dietary protein intake above the current recommended level is a valid option to achieve the optimal dietary macronutrient composition for patients with type 2 diabetes and normal kidney function. Higher protein intake does not increase plasma glucose, but increases the insulin response and results in a reduction in HbA1c. Meanwhile, higher dietary protein reduces hunger, improves satiety, and increases thermogenesis. It also enhances weight reduction while maintaining lean muscle mass, when combined with a reduced calorie diet. It is also associated with reduction in total serum cholesterol, LDL cholesterol, triglycerides, blood pressure, and markers of inflammation. It is preferable to calculate protein intake for patients with diabetes based on grams per kilogram of body weight. The use of a fixed percentage of total energy intake may result in low absolute protein intake when total caloric intake is restricted for weight reduction. Increasing protein intake to 1.5–2 g/kg (or 20–30% of total caloric intake) in association of a low caloric diet and increased physical activity may enhance weight loss, reduce blood pressure, improve lipid profile, and reduce HbA1c. Such increase in protein consumption was not associated with deterioration of renal function in patients with diabetes and normal renal function. The relationship between protein intake as grams per kilogram of body weight and AER is very weak except in hypertensive patients, particularly in those with uncontrolled diabetes. A protein intake of 0.8–1 g/kg should be reserved only for patients with diabetes and CKD. Other patients with diabetes should not reduce protein intake to less than 1 g/kg of body weight. There may be value in recommending VLPDs for patients with overt kidney disease. The beneficial effects of these diets may be related, in part, to other factors including a reduced intake of salt or saturated fat. Protein restriction may be valuable in patients with stages 4 and 5 CKD, but carries the risk of protein malnutrition and hypoalbuminemia.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Hockaday, T.D.R. (1981). Should the diabetic diet be based on carbohydrate or fat restriction? In M. Turner & B. Thomas (eds.). Nutrition and Diabetes. London : Libbey, 1981. pp23–32
Todhunter EN. Biographical notes from the history of nutrition: Elliott Proctor Joslin-June 6,1869–January 28,1962. J Am Diet Assoc. 1965;46:150.
• American Diabetes Association, Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, Hoogwerf BJ, Lichtenstein AH, Mayer-Davis E, Mooradian AD, Wheeler ML. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31 Suppl 1:S61–78. This article describes the position statement of the American Diabetes Association regarding nutrition for patients with diabetes.
Raal FJ, Kalk WJ, Lawson M et al. Effect of moderate dietary protein restriction on the progression of overt diabetic nephropathy: a 6-month prospective study. American Journal of Clinical Nutr 1994; 60: 579–85.
Pedrini MT, Levey AS, Lau J et al. The effect of dietary protein restriction on the progression of diabetic and non-diabetic renal diseases: a meta analysis. Ann Intern Med 1996; 124: 627–32.
Kasiske BL, Lakatua JD, Ma JZ et al. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am J Kidney Dis 1998; 31: 954–61.
Pemerlalu J, Berdy M, Garrel ER et al. Effect of protein intake and glycaemic control on renal function in type 2 diabetes mellitus. Diabetology 1993; 36: 829–39.
Parving HH. Renoprotection in diabetes: genetic and non-genetic risk factors and treatment. Diabetologia 1998; 41: 745–59.
Bellizzi V et al. Very low protein diet supplemented with ketoanalogs improves blood pressure control I chronic kidney disease. Kidney Int. 2007;71(3):245–51
Riley MD, Dwyer T. Microalbuminuria is positively associated with usual dietary saturated fat intake and negatively associated with usual dietary protein intake in people with insulin-dependent diabetes mellitus. Am J Clin Nutr. 1999;69(1):153.
Toelle M, Buyken A, Heitkamp G, Brämswig S, Mann J, Milne R, Gries FA, Keen H. Protein intake and urinary albumin excretion rates in the EURODIAB IDDM Complications Study. Diabetologia. 1997;40(10):1219–26.
Knight EL, Stampfer MJ, Hankinson SE, Spiegelman D, Curhan GC. The impact of protein intake on renal function decline in women with normal renal function or mild renal insufficiency. Ann Intern Med. 2003;138(6):460–7
Möllsten AV, Dahlquist GG, Stattin EL, Rudberg S.Higher intakes of fish protein are related to a lower risk of microalbuminuria in young Swedish type 1 diabetic patients. Diabetes Care. 2001;24(5):805–10.
• Azadbakht L, Atabak S, Esmaillzadeh A. Soy protein intake, cardiorenal indices, and C-reactive protein in type 2 diabetes with nephropathy: a longitudinal randomized clinical trial. Diabetes Care. 2008;31(4):648–54. This longitudinal randomized trial shows the effect of plant protein on cardiorenal indices.
Janney, NW. The metabolic relationship of the proteins to glucose. J Biol Chem. 1915;20:321–350.
MacLean, H. Modern Methods in the Diagnosis and Treatment of Glycosuria and Diabetes. 2nd edition. London, Constable & Co. Ltd.; 1924. pp. 1–52.
Krezowski, PA; Nuttall, FQ; Gannon, MC; Bartosh, NH. The effect of protein ingestion on the metabolic response to oral glucose in normal individuals. Am J Clin Nutr. 1986;44:847–856.
Nuttall, FQ; Mooradian, AD; Gannon, MC; Billington, CJ; Krezowski, PA. Effect of protein ingestion on the glucose and insulin response to a standardized oral glucose load. Diab Care. 1984;7:465–470.
Khan, MA; Gannon, MC; Nuttall, FQ. Glucose appearance rate following protein ingestion in normal subjects. J Am Coll Nutr. 1992;11:701–706.
Gannon, MC; Nuttall, JA; Damberg, G; Gupta, V; Nuttall, FQ. Effect of protein ingestion on the glucose appearance rate in subjects with type 2 diabetes. J Clin Endo & Metab. 2001;86:1040–1047. doi: 10.1210/jc.86.3.1040.
Gannon, MC; Nuttall, FQ; Neil, BJ; Westphal, SA. The insulin and glucose responses to meals of glucose plus various proteins in Type II diabetic subjects. Metabolism. 1988;37:1081–1088. doi: 10.1016/0026-0495(88)90072-8.
Gannon, MC; Nuttall, FQ; Saeed, A; Jordan, K; Hoover, K. An increase in dietary protein improves the blood glucose response in people with type 2 diabetes. Amer J Clin Nutr. 2003;78:734–741.
Hamdy O, Ledbury S, Mullooly C, et al.: Lifestyle modification improves endothelial function in obese subjects with the insulin resistance syndrome. Diabetes Care 2003, 26:2119–2125.
Pi-Sunyer X, Blackburn G, Brancati FL, et al.: Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the look AHEAD trial. Diabetes Care. 2007, 30:1374–1383.
Sjöström CD, Lissner L, Wedel H, Sjöström L. Reduction in incidence of diabetes, hypertension and lipid disturbances after intentional weight loss induced by bariatric surgery: the SOS Intervention Study. Obes Res. 1999;7(5):477–84.
•• Hamdy O, Carver C. The Why WAIT Program: Improving Clinical Outcomes through Weight Management in Type 2 Diabetes. Curr Diab Rep. 2008; 8(5):413–20. This review describes several novel methods used for diabetes weight management in clinical practice.
• Hamdy, O, Goebel-Fabbri A, Carver C, Arathuzik G, Shahar J, Capelson R, Beaton J, O’Donnell S, Elsayed N, Mitri J, Mentzelopoulos V, Abrahamson MJ. Why WAIT Program: A Novel Model for Diabetes Weight Management in Routine Clinical Practice. Obesity Management 2008;4(4):176–83. This study describes the results of the Why WAIT program for diabetes weight management in clinical practice that implemented a high protein dietary composition.
Brinkworth GD, Noakes M, Parker B, Foster P, Clifton PM.Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-loss diet, in obese adults with type 2 diabetes: one-year follow-up of a randomised trial. Diabetologia. 2004;47(10):1677–86.
Parker B, Noakes M, Luscombe N, Clifton P Effect of a high-protein, high-monounsaturated fat weight loss diet on glycemic control and lipid levels in type 2 diabetes. Diabetes Care. 2002;25(3):425–30.
Paddon-Jones D, Westman E, Mattes RD, Wolfe RR, Astrup A, Westerterp-Plantenga M. Protein, weight management, and satiety. Am J Clin Nutr. 2008;87(5):1558S–1561S.
Luscombe ND, Clifton PM, Noakes M, Parker B, Wittert G.Effects of energy-restricted diets containing increased protein on weight loss, resting energy expenditure, and the thermic effect of feeding in type 2 diabetes. Diabetes Care. 2002;25(4):652–7.
Leidy HJ, Carnell NS, Mattes RD, Campbell WW.Higher protein intake preserves lean mass and satiety with weight loss in pre-obese and obese women. Obesity 2007;15(2):421–9.
Lejeune MP, Westerterp KR, Adam TC, Luscombe-Marsh ND, Westerterp-Plantenga MS. Ghrelin and glucagon-like peptide 1 concentrations, 24-h satiety, and energy and substrate metabolism during a high-protein diet and measured in a respiration chamber. Am J Clin Nutr. 2006;83(1):89–94.
Navarro-Diaz M, Serra A, Romero R, Bonet J, Bayés B, Homs M, Pérez N, Bonal J. Effect of drastic weight loss after bariatric surgery on renal parameters in extremely obese patients: Long-term follow-up. J Am Soc Nephrol. 2006;17(12 Suppl 3):S213–217.
Skov AR, Toubro S, Bulow J, Krabbe K, Parving HH, Astrup A. Changes in renal function during weight loss induced by high vs lowprotein low-fat diets in overweight subjects. Int J Obes Relat Metab Disord. 1999;23:1170–1177.
Brinkworth GD, Noakes M, Parker B, Foster P, Clifton PM. Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-loss diet, in obese adults with type 2 diabetes: One-year follow-up of a randomised trial. Diabetologia. 2004;47:1677–1686.
Hamdy O, Elshebini A, Morsi A, Aboushady M, Mitri J, Elsayed N, Mentzelopoulos V, Abrahamson MJ. The Anti-Inflmmatory Effect of Weight Reduction in Obese Diabetic Patients after an Innovative 12-Week of Intensive Lifestyle Intervention. Diabetes (supplement 2). 2009; 731-P
Disclosure
Conflicts of interest: O. Hamdy: was on the advisory board of Abbott Nutrition; E.S. Horton: none.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hamdy, O., Horton, E.S. Protein Content in Diabetes Nutrition Plan. Curr Diab Rep 11, 111–119 (2011). https://doi.org/10.1007/s11892-010-0171-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11892-010-0171-x