
Abstract
Invasive device-based therapies for drug-resistant hypertension are undergoing active clinical investigation. The two approaches are 1) permanent implantation of a carotid baroreceptor pacemaker and 2) radiofrequency catheter ablation of the renal nerves. Both are designed to reduce the sympathetic nervous system component of drug-resistant hypertension. Several excellent comprehensive articles have reviewed each of these devices separately. In contrast, this brief article aims to provide a conceptual framework for evaluating the premise, promise, and potential limitations of both invasive antihypertensive therapies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Invasive device-based therapy for clinical hypertension has created much new buzz, even before receiving US Food and Drug Administration (FDA) approval. Two different approaches are under active clinical investigation: 1) permanent implantation of a carotid baroreceptor pacemaker [1••, 2–5] and 2) radiofrequency (RF) catheter ablation of the renal nerves [6•, 7••]. The recent publications have captured the attention of invasive cardiologists, vascular surgeons, and entrepreneurs who previously have had less interest in hypertension management. The new research also has rekindled scientific interest in neural mechanisms of hypertension as viable therapeutic targets for hypertension—especially drug-resistant hypertension.
Several excellent comprehensive articles have reviewed each of these devices separately [3, 8–12]. In contrast, this brief article aims to provide a conceptual framework for evaluating the premise, promise, and potential limitations of both invasive antihypertensive therapies. We will focus solely on clinical hypertension, discussing none of the preclinical data, and base our comments on peer-reviewed published data to date [13–15].
For decades, the sympathetic nervous system has been the “stepchild” of clinical hypertension. Sympathetic neural activity is too hard to measure in routine clinical practice. The measurement techniques require specialized training and research infrastructure, which are not widely available. Also, anti-adrenergic drugs are not first- or second-line therapy for uncomplicated hypertension because they have undesirable side-effect profiles and have performed poorly in treatment trials [16–18]. Standard β blockers are far less effective than other classes of antihypertensives in lowering central blood pressure and thus offer little if any stroke protection [19, 20]. They can cause diabetes, depression, and fatigue, and precipitate asthma or heart block in predisposed patients. α Blockers can precipitate heart failure in patients with asymptomatic left ventricular dysfunction [16, 17]. Central sympatholytics cause fatigue, depression, and rebound hypertension.
However, there now is overwhelming evidence that sympathetic overactivity constitutes a major factor in the pathogenesis and progression of human hypertension. The best evidence comes from radiotracer measurements of regional norepinephrine (NE) spillover [21, 22] and microelectrode measurements of postganglionic sympathetic nerve activity, the proximate neural stimulus to NE release [23, 24]. The former shows that sympathetic outflow is typically increased to the heart and kidneys in patients with primary hypertension. The increased cardiac NE spillover is thought to promote the development of left ventricular hypertrophy [25, 26]. The increased renal NE spillover is thought to promote the development and progression of hypertension by at least three mechanisms: renal vasoconstriction, renin secretion, and reduced sodium renal excretion [8]. The nerve recordings show that patients with primary hypertension typically have a sustained increase in the basal firing rate of sympathetic nerves innervating the skeletal muscle vasculature, one of the main beds determining total systemic vascular resistance and blood pressure (as well as insulin-mediated glucose disposal) [27].
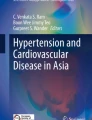
Figure 1 shows the major central and reflex mechanisms thought to drive sympathetic overactivity in human hypertension. These include, among others, resetting of the baroreceptors and activation of renal afferents. The figure also shows the specific mechanisms that are targeted by the device-based therapies and those that are not.

Central and reflex mechanisms involved in the neural control of blood pressure. Bold boxes and “X” marks show target areas for invasive therapeutic devices for the treatment of hypertension, including carotid baroreceptor pacemakers and radiofrequency (RF) catheter ablation of the renal afferent and efferent nerves. Dotted arrows represent inhibitory neural influences and solid arrows represent excitatory neural influences on sympathetic outflow. Ach acetylcholine, Ang II angiotensin II, EPI epinephrine; NE norepinephrine, NTS nucleus tractus solitaries. (Modified from Victor and Shafiq [28])
Carotid Sinus Pacemaker
The Premise
Baroreceptors are pressure-sensitive nerve endings located in the adventitia of the carotid sinuses and aortic arch [23, 28]. With each cardiac cycle, they fire during each systole and are silent during each diastole. The baroreceptors buffer acute increases in blood pressure as with emotional or physical stress. When blood pressure rises suddenly, increased baroreceptor firing sends inhibitory signals to the nucleus tractus solitarius (Fig. 1). This triggers a reflex increase in vagal efferent activity—slowing sinus rate—and a reflex decrease in sympathetic efferent activity to multiple vascular beds—decreasing vascular resistance and thus blood pressure.
The baroreceptors are thought to play a permissive role in chronic hypertension [23, 28]. They reset to defend a higher level of blood pressure, and the reflex gain can be attenuated. This attenuation is due in part to stiffening of the vessel walls in which pressure-sensitive nerve endings are embedded: a given increase in blood pressure causes less mechanical deformation of their receptive fields.
The proof-of-concept studies for carotid baroreceptor pacing dates back to the 1950s when this approach was used to treat angina and hypertension [29, 30]. Despite some short-term success, the approach was abandoned due to technical limitations—electrode contact with the carotid sinus nerve deteriorated over time due to seepage of tissue juice—and the advent of β blockers [29, 30]. Over 50 years later, the premise behind the Rheos system (CVRx, Minneapolis, MN) is a technological advance allowing durable electrode contact.
The Rheos Baroreflex Hypertension System consists of an internal programmable pulse generator and electrode leads for bilateral carotid nerve stimulation [31]. Following neck incision under general anesthesia, electrodes are placed around both carotid bifurcations. The stimulation protocol in the operating room involves changing the placement of the electrodes until optimal blood pressure response to acute electrical stimulation is found. The pacemaker itself is placed in a subcutaneous pocket and then turned off until the patient returns for a follow-up visit 1 month after the surgery.
The Promise
The appropriate initial target patient population is drug-resistant hypertension, which is said to represent as many as 1 in 5 hypertensive patients [32]. Even if a substantial portion of such patients have pseudoresistance, the actual target population in the United States alone could be 2 to 7 million Americans.
What is clear from the published data so far is that in chronically implanted patients with drug-resistant hypertension, acute activation of the baroreceptor pacemaker for 10 min evokes voltage-dependent decreases in blood pressure, with parallel decreases in heart rate and muscle sympathetic nerve activity [1••, 2–5]. These parameters return to baseline levels when the stimulation is turned off. For example, one study of 12 patients showed peak drops in blood pressure of 32/15 mm Hg (from baseline blood pressure 193/94 mm Hg), heart rate of 5 bpm, and sympathetic nerve activity of 9% in 12 patients [1••].
What is yet to be determined is whether long-term carotid baroreflex stimulation is effective antihypertensive therapy. To date, there are two multicenter trials of Rheos for drug-resistant hypertension—one in Europe (DEBuT-HT trial [Device Based Therapy in Hypertension Extension Trial]; clinicaltrials.gov identifier NCT00710294) and the other in the United States (Rheos Pivotal trial; clinical trials.gov identifier NCT00442286). The European DEBuT-HT trial is a single-arm, open-label trial with end points of safety and blood pressure at 1 year post surgery with an enrollment goal of 50 patients. Forty-five patients have been enrolled with a baseline blood pressure of 179/105 mm Hg. The recently published results show that office blood pressures dropped by 21/12 mm Hg at 3 months (n = 37), 30/20 mm Hg at 1 year (n = 26), and 33/22 mm Hg at 2 years (n = 17). In a subset of patients, ambulatory blood pressures dropped 6/4 mm Hg at 3 months, 13/8 mm Hg at 1 year, and 24/13 mm Hg at 2 years [33••]
The US Pivotal trial was designed as a randomized, controlled, double-blind trial with end points of safety and blood pressure reduction at 1 year and an enrollment goal of 300 patients: 322 patients were enrolled. One month following pacemaker implantation, patients were randomized to an active intervention arm in which the pacemaker was turned on for the full 12 months or a comparison arm in which the pacemaker was off for the first 6 months and turned on for the final 6 months. An interim analysis by the Data Safety Monitoring Board found that the 6-month efficacy and 30-day safety endpoints were unlikely to be met [34].
Potential Limitations
Potential limitations of a carotid baroreceptor pacemaker for hypertension involve 1) challenges of clinical trial methodology, 2) surgical skill, and 3) conceptual issues. Because the first two issues are common to both devices, they will be discussed later in the paper.
Conceptually, the key question is whether sustained electrical stimulation of the carotid sinus nerves can cause sustained reductions in blood pressure or whether there will be partial blood pressure escape. To test for escape or adaptation, it first would be necessary to show that electrode contact with the nerve does not deteriorate over time. If so, the next key issue is potential compensation from many other blood pressure control mechanisms, especially from aortic baroreceptors that are not being paced. With carotid baroreceptor pacing, the fall in blood pressure should be sensed by the aortic baroreceptors, evoking reflex increases in sympathetic activity that would be expected to at least partially offset the desired blood pressure reduction. Moreover, previous research suggested that in normotensive humans the aortic baroreceptors are dominant in the baroreflex control of sympathetic activity, vascular resistance, and blood pressure, whereas the carotid baroreceptors are dominant in the vagal control of heart rate [35]. The acute stimulation studies with Rheos in hypertensive individuals may call the earlier conclusion into question.
A large body of research has shown that baroreflex control of vagal activity (heart rate) is attenuated with even mild hypertension [36], whereas baroreflex control of sympathetic activity (vascular resistance and blood pressure) is preserved until much later in the hypertensive process—until stage 2 hypertension associated with left ventricular hypertrophy [37, 38]. Thus, in some patients with advanced hypertension in the Rheos trials, the carotid pacemaker may be driving an attenuated reflex.
Radiofrequency Ablation of the Renal Nerves
The Premise
The kidney is richly innervated by sympathetic nerve terminals. The renal sympathetic nerves have long been considered one of the most important regional sympathetic outflows in long-term blood pressure regulation [39]. Renal sympathetic nerves cause renal vasoconstriction and hypertrophy via α1 receptors, stimulate renin release via β1 receptors, and enhance renal sodium and water reabsorption via α1 receptors [39].
The kidney is also a sensory organ, innervated by a rich supply of sensory afferents that signal the brain of changes in the chemical composition of the urine and mechanical changes in the renal pelvis [14, 40, 41]. Some of these afferents have inhibitory effects on sympathetic outflow [14, 40] but most seem to evoke sympathetic excitation [41]. Chemosensitive renal afferents can be activated by ischemic metabolites such as adenosine and uremic metabolites such as urea; they have been implicated in triggering reflex sympathetic activation and thus contributing to the pathogenesis and progression of hypertension in chronic kidney disease, renovascular hypertension, and cyclosporine A–induced hypertension [42, 43]. The renal nerves also have been implicated in the progression of hypertensive chronic kidney disease [44, 45].
The proof-of-concept studies for this invasive antihypertensive therapy began as early as the 1930s, when complete surgical sympathectomy was used to reduce blood pressure in patients with hypertension [46]. These methods were abandoned because they were associated with high perioperative morbidity and mortality. In contrast, the RF catheter allows selective, nonsurgical ablation of the renal sympathetic nerves.
The catheter (Symplicity; Ardian, Palo Alto, CA) is used for hopefully complete and permanent ablation of both renal nerves, both efferents and afferents [47]. The procedure is performed under conscious sedation because patients will experience transient renal colic with the ablation (renal afferent nerve activation). The catheter is inserted into the femoral artery and then advanced to each renal artery under the guidance of renal angiography. The premise is that the renal nerves, which are located on the adventitial surface of the renal arteries, are destroyed by application of an RF current via the intraluminal catheter. An advantage of this approach is that this is a one-time procedure, and there is no implanted hardware.
The Promise
Once again, the appropriate initial target patient population is drug-resistant hypertension. The ongoing safety and proof-of-principle cohort study is being performed at five medical centers in Australia and Europe (clinicaltrials.gov identifiers NCT00483808 and NCT00664638). The study is designed as an uncontrolled, open-label, single-group assignment study to assess the safety and feasibility of the interventional treatment in patients with 1) blood pressure of 160 mm Hg or higher, 2) treatment with three or more antihypertensives, 3) no known secondary cause of hypertension, and 4) glomerular filtration rate of 45 mL/min/1.73 m2 or more. To date, 50 patients have been enrolled, and recruitment is ongoing.
What has been published in the peer-review literature so far is the initial results of this phase 1 study [6•] and a multicenter, prospective, randomized trial [7••]. After bilateral RF renal nerve ablation, renal NE spillover fell by 47.5%. Office blood pressure fell (from a baseline of 177/101 mm Hg) by 24/10 mm Hg in 39 patients at 3 months of follow-up and by 29/16 mm Hg in the first nine patients followed for 12 months [6•]. However, measured reductions in blood pressure by 24-hour ambulatory monitoring were much smaller: -11 mm Hg (vs −27 mm Hg for office blood pressure in the same 12 patients at 1 month). In the absence of a control group, the precise effect size remains unclear.
In the multicenter Symplicity HTN-2 trial, office blood pressure fell by 32/12 mm Hg from a baseline of 178/96 mm Hg in 49 patients six months following renal denervation, but not in the control group [7••]. Home-based blood pressure measurements and 24-hour blood pressure monitoring confirmed these findings.
Potential Limitations
As with the carotid sinus nerve pacemaker, potential limitations of RF renal nerve ablation for resistant hypertension involve 1) challenges of clinical trial methodology, 2) operator skill, and 3) conceptual issues.
Besides patient safety issues of early and late procedural complications, which are being actively investigated, the main unresolved conceptual concerns are the completeness of renal denervation and possible reinnervation over time. Efficient protocols for quantifying renal denervation and long-term follow-up studies are needed. An RF catheter placed at the level of the renal nerves almost certainly will not destroy all urogenital afferents, which arise densely throughout the renal pelvis as well as the genitofemoral regions; the afferent inputs may exert highly redundant effects on sympathetic outflow.
Continuing with the concept of redundancy, the renal efferents are by no means the only regional sympathetic nerves involved in blood pressure regulation. Major roles have been implicated for the muscle and splanchnic sympathetic nerves [48], which obviously will not be ablated by the procedure. A key question is whether renal afferent denervation causes global decreases in sympathetic nerve activity to multiple vascular beds. The advent of the RF catheter should shed important new light on this topic.
Limitations Common to Both Devices
As mentioned earlier, clinical trial methodology and operator skill complicate the evaluation of both invasive techniques. Standard clinical trial methodology is designed for evaluating drug therapy and is an imperfect fit for evaluating device-based therapy of any kind. Antihypertensive drug trials typically randomize tens of thousands of patients with stage 1 to 2 hypertension to new therapy versus an active comparator arm and are powered to detect a greater benefit of the new therapy on hard outcomes over 5 years. By contrast, the initial device-based trials have a sample size of only 50 to 300 patients mainly because of the much stricter inclusion criteria, starting with drug-resistant hypertension. Due to sample size, the primary outcome is restricted to blood pressure reduction rather than hard outcomes. The ability to detect and measure a treatment effect on blood pressure reduction is complicated by background noise from the inherent variability of blood pressure and changing multidrug blood pressure regimens. Ambulatory blood pressure monitoring will help with the former but not the latter issue.
With the carotid sinus pacemaker, “sham” pacing is a reasonable short-term control, but for ethical reasons, patients cannot be randomized to sham RF renal nerve ablation. In the absence of comparator arms, the expected Hawthorne effect and regression to the mean will lead to overestimation of treatment effects (of both trials).
Operator skill is another uncontrolled variable in these multicenter trials of relatively small numbers of study patients. This will become an even larger issue in the clinical practice setting if FDA approval is obtained. Objective, highly standardized, intermediate end points need to be developed and measured repeatedly to establish in each patient the extent to which the intervention was delivered as intended, both initially and over time. Both devices would be expected to have a larger treatment effect when there is a large sympathetic component to the hypertension, which may or may not be the case in individual patients with drug-resistant hypertension. Finally, the total numbers of patients with truly drug-resistant hypertension will need to be re-evaluated with the increasing use of excellent cost-effective fourth- and fifth-line generic drugs for difficult hypertension, such as vasodilating β blockers and aldosterone antagonists [32].
Conclusions
Device-based therapy is a fascinating new area of clinical research in hypertension. Any firm conclusions at this point would be premature pending publication of final outcome data from the current multicenter trials. Much more research is needed to identify subsets of patients who stand to benefit the most—not only for hypertension but potentially also for treatment of heart failure and chronic kidney disease. Formal long-term cost-effectiveness simulations will be key in the era of health care reform.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
•• Heusser K, Tank J, Engeli S et al. Carotid baroreceptor stimulation, sympathetic activity, baroreflex function, and blood pressure in hypertensive patients. Hypertension 2010, 55:619–626. This study reports data showing decreases in blood pressure, heart rate, and sympathetic nerve activity following acute activation of a chronically implanted carotid baroreceptor pacemaker in 12 patients with drug-resistant hypertension.
Illig KA, Levy M, Sanchez L et al. An implantable carotid sinus stimulator for drug-resistant hypertension: surgical technique and short-term outcome from the multicenter phase II Rheos feasibility trial. J Vasc Surg 2006, 44:1213–1218.
Mohaupt MG, Schmidli J, Luft FC: Management of uncontrollable hypertension with a carotid sinus stimulation device. Hypertension 2007, 50:825–828.
Tordoir JH, Scheffers I, Schmidli J et al. An implantable carotid sinus baroreflex activating system: surgical technique and short-term outcome from a multi-center feasibility trial for the treatment of resistant hypertension. Eur J Vasc Endovasc Surg 2007, 33:414–421.
Wustmann K, Kucera JP, Scheffers I et al. Effects of chronic baroreceptor stimulation on the autonomic cardiovascular regulation in patients with drug-resistant arterial hypertension. Hypertension 2009, 54:530–536.
• Krum H, Schlaich M, Whitbourn R et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 2009, 373:1275–1281. This study reports initial safety and efficacy data from a phase 1 trial investigating blood pressure decreases following RF catheter ablation of the renal nerves. The study reports 3-month follow-up data in 39 patients and 12-month follow-up data in nine patients being treated for drug-resistant hypertension.
•• Esler MD, Krum H, Sobotka PA et al. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 trial): randomised controlled trial. Lancet 2010. doi:10.1016/s0140-6736(10)62039-9. This study reports data from a multicenter, prospective, randomized trial investigating blood pressure decreases following RF catheter ablation of the renal nerves. The study reports 6-month efficacy data in 106 patients being treated for drug-resistant hypertension,49 of which underwent RF catheter ablation of the renal nerves and 52 who were randomized to control treatment alone.
Dibona GF and Esler M: Translational medicine: the antihypertensive effect of renal denervation. Am J Physiol Regul Integr Comp Physiol 2010, 298:R245–R253.
Doumas M, Faselis C, Papademetriou V: Renal sympathetic denervation and systemic hypertension. Am J Cardiol 2010, 105:570–576.
Mancia G, Parati G, Zanchetti A: Electrical carotid baroreceptor stimulation in resistant hypertension. Hypertension 2010, 55:607–609.
Schlaich MP, Sobotka PA, Krum H et al. Renal denervation as a therapeutic approach for hypertension: novel implications for an old concept. Hypertension 2009, 54:1195–1201.
Schlaich MP, Krum H, Sobotka PA: Renal sympathetic nerve ablation: the new frontier in the treatment of hypertension. Curr Hypertens Rep 2010, 12:39–46.
Campese VM and Kogosov E: Renal afferent denervation prevents hypertension in rats with chronic renal failure. Hypertension 1995, 25:878–882.
Kopp UC, Jones SY, Dibona GF: Afferent renal denervation impairs baroreflex control of efferent renal sympathetic nerve activity. Am J Physiol Regul Integr Comp Physiol 2008, 295:R1882–R1890.
Zucker IH, Hackley JF, Cornish KG et al. Chronic baroreceptor activation enhances survival in dogs with pacing-induced heart failure. Hypertension 2007, 50:904–910.
Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). ALLHAT Collaborative Research Group. JAMA 2000, 283:1967–1975.
Diuretic versus alpha-blocker as first-step antihypertensive therapy: final results from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Hypertension 2003, 42:239–246.
Cushman WC: Are there benefits to specific antihypertensive drug therapy? Am J Hypertens 2003, 16:31S–35S.
Bangalore S, Kamalakkannan G, Messerli FH: Beta-blockers: no longer an option for uncomplicated hypertension. Curr Cardiol Rep 2007, 9:441–446.
Lindholm LH, Carlberg B, Samuelsson O: Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005, 366:1545–1553.
Esler M, Jennings G, Biviano B et al. Mechanism of elevated plasma noradrenaline in the course of essential hypertension. J Cardiovasc Pharmacol 1986, 8 Suppl 5:S39–S43.
Schlaich MP, Lambert E, Kaye DM et al. Sympathetic augmentation in hypertension: role of nerve firing, norepinephrine reuptake, and Angiotensin neuromodulation. Hypertension 2004, 43:169–175.
Guyenet PG: The sympathetic control of blood pressure. Nat Rev Neurosci 2006, 7:335–346.
Julius S, Krause L, Schork NJ et al. Hyperkinetic borderline hypertension in Tecumseh, Michigan. J Hypertens 1991, 9:77–84.
Schlaich MP, Kaye DM, Lambert E et al. Relation between cardiac sympathetic activity and hypertensive left ventricular hypertrophy. Circulation 2003, 108:560–565.
Schlaich MP, Kaye DM, Lambert E et al. Angiotensin II and norepinephrine release: interaction and effects on the heart. J Hypertens 2005, 23:1077–1082.
Esler M, Rumantir M, Wiesner G et al. Sympathetic nervous system and insulin resistance: from obesity to diabetes. Am J Hypertens 2001, 14:304S–309S.
Victor RG and Shafiq MM: Sympathetic neural mechanisms in human hypertension. Curr Hypertens Rep 2008, 10:241–247.
Epstein SE, Beiser GD, Goldstein RE et al. Circulatory effects of electrical stimulation of the carotid sinus nerves in man. Circulation 1969, 40:269–276.
Richter DW, Keck W, Seller H: The course of inhibition of sympathetic activity during various patterns of carotid sinus nerve stimulation. Pflugers Arch 1970, 317:110–123.
Welcome to CVRx, Inc. Available at http://www.cvrx.com. Accessed June 2010.
Calhoun DA, Jones D, Textor S et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension 2008, 51:1403–1419.
•• Scheffers IJM, Kroon AA, Schmidli J et al., Novel baroreflex activation therapy in resistant hypertension. J Am Coll Cardiol 2010, 56:1254–1258. This study presents 3-month, 1-year, and 2-year follow-up data from the DEBuT-HT trial showing decreases in blood pressure following activation of a chronically implanted carotid baroreceptor pacemaker in 45 patients with drug-resistant hypertension.
Georgakopoulos D, Little WC, Abraham WT, et al. Chronic baroreflex activation: a potential therapeutic approach to heart failure with preserved ejection fraction. J Cardiac Fail 2010. doi:10.1016/j.cardfail.2010.09.004.
Sanders JS, Ferguson DW, Mark AL: Arterial baroreflex control of sympathetic nerve activity during elevation of blood pressure in normal man: dominance of aortic baroreflexes. Circulation 1988, 77:279-288.
Esler M: The sympathetic system and hypertension. Am J Hypertens 2000, 13:99S–105S.
Grassi G, Seravalle G, Quarti-Trevano F et al. Sympathetic and baroreflex cardiovascular control in hypertension-related left ventricular dysfunction. Hypertension 2009, 53:205–209.
Mancia G, Grassi G, Parati G et al. The sympathetic nervous system in human hypertension. Acta Physiol Scand Suppl 1997, 640:117–121.
Dibona GF: Physiology in perspective: The Wisdom of the Body. Neural control of the kidney. Am J Physiol Regul Integr Comp Physiol 2005, 289:R633–R641.
Kopp UC and Buckley-Bleiler RL: Impaired renorenal reflexes in two-kidney, one clip hypertensive rats. Hypertension 1989, 14:445–452.
Dibona GF and Kopp UC: Neural control of renal function. Physiol Rev 1997, 77:75–197.
Katholi RE, Whitlow PL, Hageman GR et al. Intrarenal adenosine produces hypertension by activating the sympathetic nervous system via the renal nerves in the dog. J Hypertens 1984, 2:349–359.
Ryuzaki M, Stahl LK, Lyson T et al. Sympathoexcitatory response to cyclosporin A and baroreflex resetting. Hypertension 1997, 29:576–582.
Klein IH, Ligtenberg G, Oey PL et al. Sympathetic activity is increased in polycystic kidney disease and is associated with hypertension. J Am Soc Nephrol 2001, 12:2427–2433.
Klein IH, Ligtenberg G, Neumann J et al. Sympathetic nerve activity is inappropriately increased in chronic renal disease. J Am Soc Nephrol 2003, 14:3239–3244.
Morrissey DM, Brookes VS, Cooke WT: Sympathectomy in the treatment of hypertension; review of 122 cases. Lancet 1953, 1:403–408.
Ardian, Inc. http://www.ardian.com/medical-professionals/system.shtml. Accessed June 2010.
Osborn JW and Fink GD: Region-specific changes in sympathetic nerve activity in angiotensin II-salt hypertension in the rat. Exp Physiol 2010, 95:61–68.
Disclosure
Conflicts of interest: E.A. Martin: none; R.G. Victor: has received grants from the following companies: Pfizer, National Institutes of Health, Muscular Dystrophy Association, NicOx, and Novartis; has received research support from the Lincy Foundation and the Donald W. Reynolds Foundation; is on the Advisory Board for St. Jude’s and CVRx; has been on the External Advisory Board for Emory University (Cardiology Training Grant program) and the University of Iowa (Clinical Translational Science award); and has been on the speakers’ bureau for Pfizer, GlaxoSmithKline, and Novartis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Martin, E.A., Victor, R.G. Premise, Promise, and Potential Limitations of Invasive Devices to Treat Hypertension. Curr Cardiol Rep 13, 86–92 (2011). https://doi.org/10.1007/s11886-010-0156-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11886-010-0156-z
Keywords
- Hypertension
- Carotid baroreceptor pacemaker
- Radiofrequency catheter ablation
- Antihypertensive therapies
- Sympathetic nervous system
- Parasympathetic nervous system
- Sympathetic overactivity
- Norepinephrine
- Renal vasoconstriction
- Renin
- Sodium
- Vascular resistance
- Blood pressure
- Blood flow
- Heart rate
- Efferent renal nerves
- Afferent renal nerves
- Kidney disease
- Renal disease
- Heart failure
- Left ventricular dysfunction
- Innervation
- Denervation
- Electrical stimulation