
Abstract
Purpose of Review
In this article, we review current understanding of the epidemiology and etiology of disparities in asthma. We also highlight current and emerging literature on solutions to tackle disparities while underscoring gaps and pressing future directions.
Recent Findings
Tailored, multicomponent approaches including the home, school, and clinician-based interventions show great promise.
Summary
Managing asthma in disadvantaged populations can be challenging as they tend to have disproportionately worse outcomes due to a multitude of factors. However, multifaceted, innovative interventions that are sustainable and scalable are key to improving outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Asthma remains a significant public health problem. In 2014, about 9% of children and 7.5% of adults reported a physician diagnosis of current asthma [1]. However, the burden of disease is higher in underrepresented minorities and low-income populations [2, 3]. The prevalence has been reported to be as high as 20–30% in some underrepresented minority communities (Blacks and certain Latino groups such as Puerto Ricans) [4,5,6]. These underrepresented minority groups are also more likely to experience higher rates of asthma morbidity, mortality, and healthcare utilization [7]. These differences have been recognized and described to a significant extent in the literature [8]. Moreover, the reasons for these differences have been investigated although more work can be done [9]. However, what is lacking are solutions to tackle these differences.
This review will highlight recent advances in the treatment and management of asthma in disadvantaged populations, with emphasis on innovative interventions in these populations.
Who and Where Is the Disadvantaged?
Before we dive into our review, it is prudent to clarify who is defined as disadvantaged, as it is a quite nebulous term.
In this review, we will define disadvantaged populations as those who have experienced barriers to self-sufficiency through lack of resources such as education, financial capital, or community support [10]. Given the historical context of the USA in regard to racial discrimination and segregation, disadvantaged communities tend to be those that are primarily low income, majority underrepresented minority, and live in rural and inner-city areas [11]. This is also in line with the NIH’s definition of disadvantaged persons [12].
However, it is important to highlight that not all disadvantaged communities with asthma reside in urban or inner-city areas [13]. Keet et al. investigated the concept of “inner city asthma” through their analysis of National Health Interview Survey data from 2009 to 2011 [14••]. They found that independent risk factors for asthma were Black race, Puerto Rican ethnicity, and low household income—not residence in poor or urban areas. They performed a similar inquiry using Medicaid claims data and found that residence in poor, urban areas was not a predictor of asthma prevalence adjusted for neighborhood poverty and race/ethnicity [15••]. However, Black race and poor neighborhood residence were risk factors for prevalent asthma. Additionally, residence in poor, urban areas was associated with emergency department visits and hospitalizations.
Mechanisms of Worse Outcomes in Disadvantaged Communities
Through mostly observational studies, worse outcomes in asthma prevalence and outcomes in disadvantaged communities have been attributed to multifactorial causes such as socioeconomic factors (namely income, education), racial/ethnic genetic variants, environmental allergen/pollutant exposures, psychosocial stressors (neighborhood violence/safety), behavioral risk factors (smoking, obesity), poor medication adherence, and/or lack of access (to medicines, quality evidence-based care) [16,17,18,19,20,21].
Beck et al. pursued the difficult task of trying to disentangle the multifactorial causes by examining several contributors to worse readmission rates in Black children compared to white children [22••]. Their analysis involved directed acyclic graphing which allows one to examine multiple variables’ effect on an outcome in one model. They found that the socioeconomic hardship variable explained 53% of the disparity, and when biologic, environmental, disease management, and access variables were added, 80% of the disparity was explained. Although this analysis further supports how the cause of racial disparities is multifactorial, it is reassuring that most of the factors could be amendable to intervention.
Another study that has attempted to further elucidate the complexity of asthma is an article recently in press by the VIDA Disparities Working Group that examined the relationship between socioeconomic status, stress, and asthma outcomes in the context of a randomized controlled trial, allowing the unique inclusion of variables, normally captured via self-report in previous studies, through objective monitoring and measurement [23••]. They found that low income was an independent risk factor for asthma treatment failures and exacerbations, regardless of factors such as race, education, perceived stress, BMI, inhaled corticosteroid dose or adherence, baseline lung function, environmental allergen sensitization, secondhand smoke exposure, and hospitalizations. The authors noted that this finding could be limited to their cohort and not generalizable, and additional research would be warranted to further clarify the relationship between low income and asthma outcomes.
More recent studies have evaluated the role of asthma phenotypes, social determinants of health including discrimination as playing a role in asthma morbidity. For example, phenotypic analysis of children from low-income urban areas is lacking which would potentially help tailor management approaches. Zoratti et al. performed a cluster analysis from participants enrolled in nine inner-city asthma consortium centers and were receiving guidelines-based asthma management [24]. Five cluster phenotypes identified distinguished by asthma and rhinitis severity, pulmonary physiology, atopy, and allergic inflammation. The most severe phenotype was highly atopic with high total serum IgE levels, serum eosinophilia, and allergen sensitizations. However, there was a phenotype that was highly symptomatic but with little atopy and allergic inflammation.
Examination of the physical environment and social context contribution to asthma morbidity has been quite revealing. Material hardship and home ownership were recently examined as a contributor to disparities by Hughes et al. [25••]. They analyzed the 2011 American Housing Survey and found that poor housing quality was associated with asthma diagnosis and emergency department visits. Home ownership was associated with lower odds of an asthma emergency department visit. These findings emphasize the multifaceted nature of socioeconomic status and the need for it to be captured using multiple measures. The stress of caregivers of students enrolled in the school inner-city asthma study was associated with worse asthma outcomes [26•]. Participants with caregivers with very high stress (PSS-4 > =8) had two times increased odds of haying a symptom day and 2.1 more symptom days over a 2-week period compared to participants with normal stress. Level of caregiver stress was not associated with differences in child anxiety, inhaled corticosteroid use, medication adherence, and secondhand smoke exposure, calling attention to the need for additional research to elucidate the mechanism is necessary.
The role of perceived discrimination in asthma status and outcomes of Latino and Black asthmatics aged 8–21 years of age in the GALA II and SAGE II studies was investigated by Thakur et al. Blacks reporting any severity of discrimination had 78% increased odds of having asthma and 97% increased odds of poor asthma control. Mexican subjects with a low socioeconomic status (measured by a composite of education, income, and insurance status) had a 65% increased odds of having asthma [27••]. These findings highlight those efforts to improve asthma outcomes in disadvantaged populations should not only entail interventions within our healthcare system, but also include integration with social supports and services [28].
Recent Solutions to Addressing Disparities in Disadvantaged Communities
Indoor Environmental Remediation
Over the past two decades, the role of the indoor environment in asthma management has come under attention [29••, 30•, 31]. However, questions persist regarding indoor environment remediation’s role in asthma management as there is publication bias—where there is less publication of unsuccessful environmental interventions. Despite this, appropriately tailored, multicomponent (e.g., physical and education) interventions appear to be most effective [29••, 32••].
Environmental Remediation at Home
The inner-city asthma study (ICAS) was one of the most successful intervention studies consisting of a home remediation conducted by families and tailored to the child’s sensitizations that lead to reductions in home dust mite and cockroach levels and asthma symptom days [33]. Benefits lasted 12 months and were cost-effective. ICAS and other early studies have led to numerous trials investigating how to balance comprehensive remediation while maintaining cost and efficacy. We will focus on new studies published in the past year given the brevity of this article.
The Mouse Allergen and Asthma Intervention Trial (MAAIT) evaluated if professionally delivered integrated pest management (IPM) and pest management education compared to pest management education alone—targeting mouse allergen alone—was associated with improved asthma outcomes [34]. The study authors found no difference in maximal symptom days, lung function, health care utilization, and short-acting β-agonist use. Interestingly, there was no statistically significant difference in the proportion of subjects with large decreases of mouse allergen (except for one airborne measure) between the two groups. It is possible that this lack of significance could be because the intervention was not blinded, leading to biased results.
The New Orleans roach elimination study (NO-Roach) was a randomized trial to examine the effect of cockroach insecticidal bait, a component of integrated pest management (IPM) on asthma symptom days [35]. The control group had a greater median level of cockroaches, number of symptom days, and ED/unscheduled visits. The control group also had 5.74 times higher odds of a FEV1 of < 80% predicted. The effect of the intervention was also more notable depending on cockroach sensitization. Cockroach sensitized children in the control group also had a significantly higher number of missed school days in addition to more symptom days and healthcare utilization.
DiMango et al. conducted a randomized trial of an individualized home environmental remediation—delivered by intervention counselors—to investigate the ability to “step-down” asthma therapy in children and adults with optimally treated and controlled asthma in New York City [36]. The remediation targeted all home allergens. The intervention group had a significant reduction in all mean allergen levels, and interestingly, the control group had a significant reduction in kitchen cockroach and bedroom dust and mouse allergen levels. Both groups could step down their asthma therapy, and there was no statistical significant difference between the two groups. There was also no difference in the mean number of days with symptoms, nighttime awakenings, or rescue medication use. The authors attributed the lack of difference due to control subjects preparing for home visits, subjects having regular follow-up and access to free medicines. The authors also noted that there was a post-hoc analysis suggesting that subjects who had significant reduction in kitchen mouse allergen had a significant stepping down of their asthma therapy, regardless of treatment arm, compared to those who did not have a significant reduction.
Some of the major criticisms of these home intervention studies is how will they translate to the “real world setting” and if they truly associate with improved outcomes. A recent review of the effectiveness of home environmental remediation studies examined the compliance of participants in these studies. Compliance was related to study design features such as the Hawthorne effect; however, there were participant factors. Notably, resources of the participants and interventions requiring behavioral change were associated with less compliance of study recommendations [32••]. The health outcome measures used in studies have been varied with very, mixed results—lung function, bronchial hyperresponsiveness, medication usage, absenteeism, health care utilization, and functional limitations [32••]. This inconsistency in results has been attributed to the following: study design such as the use of self-reported measures or seasonality, sample size, and inadequate environmental changes. This latter issue of inadequate environmental changes highlights an important issue regarding “how much” does an allergen or pollutant need to be decreased to improve a health outcome, particularly if the intervention is targeting only one allergen.
Environmental Remediation at School
There has been recent interest in conducting interventions in the school setting as children spend most of their time in school, and numerous studies have demonstrated considerable allergen and pollutant levels present in schools [37••, 38]. There is less comprehensive data on school-based environmental interventions and health outcomes, as most studies to date have been small, cross-sectional and have not controlled for home environmental exposures [39].
One recent study examining school allergen and pollution is the school inner-city asthma study (SICAS-1), which is a 5-year-cohort study following asthma outcomes and classroom aeroallergen exposures of urban, elementary age children over 1 year [37••, 40]. Mouse allergen had the highest rate of detection in homes and schools but was significantly higher in schools. Mouse allergen exposure, independent of sensitization and home allergen exposure, was significantly associated with an increased number of asthma symptom days and decreased FEV1% predicted [37••].
The same research team conducted a randomized pilot study to examine the role of high efficiency particulate air (HEPA) cleaners in elementary school classrooms in reducing indoor particulate pollutant and improving asthma morbidity outcomes [41]. They also assessed the feasibility of a partial-integrated pest management intervention in these schools. Classroom-based HEPA cleaners were associated with significant reduction of fine particulate matter (PM2.5) and black carbon (BC). The intervention group had a greater improvement in PEF compared to the control group [41]. However, they did not measure classroom ventilation which is a significant contributor to indoor pollution.
The team has now embarked on a randomized, blinded sham controlled environmental trial, built on SICAS-1 and this recent pilot, which is called the school inner-city asthma intervention study (SICAS-2). Schools will be randomized to receive integrated pest management versus control and classrooms within these schools to receive either air purifiers or sham control [42].
Others have emphasized that school-centered health partnerships between school nurses, patients, families, primary care physicians, and asthma specialists are key to improving outcomes and reducing disparities [43, 44]. The American Academy of Allergy, asthma and immunology have advocated utilizing the school-based asthma management program (SAMPRO) framework to coordinate care for children with asthma. The program entails communication network between all stakeholders, complete asthma management plan, asthma education plan for school personnel, and remediation of asthma triggers at school [45•, 46].
Community Interventions Targeting Social Determinants of Health
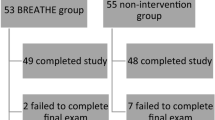
Other interventions have focused in improving adherence to asthma guidelines and increased detection of worsening asthma severity. The Easy Breathing program consists of decision support tools to help clinicians diagnose and manage asthma utilizing the EPR-3 asthma guidelines during office visits. The program has been associated with 35% reduction in admissions and 30% reduction in emergency department visits in Medicaid-insured children [47].
Bradley et al. conducted a pilot of a collaborative asthma management program between a community pharmacy and pediatric primary care center (serving a largely publicly insured population) to improve outcomes in children with high-risk asthma [48]. The partnership formed a medication therapy management (MTM) service to improve transition of care of high-risk pediatric patients with asthma from physician offices to the pharmacy. The MTM session was designed as a 20-min intervention integrated into the pharmacy workflow, follow-up with the caregiver approximately 1 month later, and recommendations to the prescriber. The number, type, and acceptance of recommendations to caregivers/patients, and prescribers were evaluated. Prescriber recommendations were usually directed toward orders for rescue inhalers, anti-allergy medications, nebulizers, humidifiers, and spacers. There was 100% acceptance of the medication recommendations by primary care providers.
As mentioned above, rural communities can also be significantly affected by worse asthma outcomes. The Regional Asthma Disease Management Program (RADMP) was designed to improve outcomes in children at least 12 years old by providing asthma education and environmental education and remediation, in rural western North Carolina [49]. There was a significant reduction in asthma-related emergency department visit and admissions, improved lung function and reduction in school absences. The healthcare cost avoided 1-year post-intervention was about $882,021.
The Merck Childhood Asthma Network (MCAN) conducted a study to assess the effectiveness of pediatric asthma care coordination in four underserved urban areas. The care coordination intervention varied slightly amongst the sties but mainly consisted of an asthma care coordinator providing education, home visits, and care linkages with clinical providers. At 12-month follow-up, intervention participants had fewer symptom days and nights per month versus a simulated comparison group [50].
Patient Centered Outcomes Research Institute (PCORI) recently funded multicomponent interventions to improve patient-centered outcomes for underrepresented minorities with uncontrolled asthma. Many of the projects are specifically investigating patient and other stakeholder-centered approaches to improving adherence to guidelines. For example, one study is examining the role of caregiver/patient adjustment of medication compared to guideline-physician-based adjustment. Another study is investigating the role of enhanced clinic care, community home worker visits, provider education, and a health plan intervention in several community health centers [51••].
Previous studies have shown that community health workers have been instrumental in improving health outcomes through education and home visits [31]. Bryant-Stephens et al. recently reaffirmed the significance of the home visit in better understanding what low-income minority patients with asthma need to have better outcomes. In this study, community health workers were used to recruit and follow subjects to help with patient portal access [52]. They observed extremely poor housing conditions and lack of social resources for many of the subjects. The authors suggested that interventions should entail understanding and removal of barriers to optimal management. This and the other featured PCORI funded studies are ongoing at this time [51••, 53].
Future Directions and Conclusion
Asthma continues to be a significant cause of morbidity and mortality in low-income underrepresented minority communities. However, recent research has shown great promise of improved outcomes when tailored, multifaceted approaches that include home, school, clinician-based interventions are implemented. These interventions entail dealing with reducing/eliminating allergen or pollutant exposure, educational and empowerment support for patients, and decision support tools and resources for providers.
Despite this, there are still gaps that should be examined to reduce the burden of disease in disadvantaged communities. There is still a need to have a better understanding of the role of indoor environmental remediation of chemical pollutants and its role in health outcomes and what is the adequate “dose” of an environmental intervention to see improved outcomes. Moreover, it is unclear from the multicomponent environmental remediation interventions which component was the effective piece. This may require more innovative study designs such as factorial designs to better delineate the most effective pieces of multifaceted interventions. Another possibility is that the synergy of components that lead to improved outcomes and that teasing out the relative contributions may not be feasible or even warranted.
More research is also needed in developing more innovative approaches in settings outside of the clinical setting, such as telemedicine and Breathmobiles [54, 55]. Additionally, we need a better understanding of what leads to sustainable and scalable interventions in real-world settings. Lastly, the complex intersection between the social determinants of health and asthma must continue to be examined with a particular emphasis on the role of policy in supporting these intervention efforts [56].
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Control CfD, Prevention. Most recent asthma data. External link available at: http://www.cdc.gov/asthma/most_recent_data.htm. 2015. Accessed 04 Apr 2016.
Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. NCHS data brief. 2012;94(94):1–8.
Togias A, Fenton MJ, Gergen PJ, Rotrosen D, Fauci AS. Asthma in the inner city: the perspective of the National Institute of Allergy and Infectious Diseases. J Allergy Clin Immunol. 2010;125(3):540–4.
McLaughlin T, Maljanian R, Kornblum R, Clark P, Simpson J, McCormack K. Evaluating the availability and use of asthma action plans for school‐based asthma care: a case study in Hartford, Connecticut. J Sch Health. 2006;76(6):325–8.
Nicholas SW, Jean-Louis B, Ortiz B, Northridge M, Shoemaker K, Vaughan R, et al. Addressing the childhood asthma crisis in Harlem: the Harlem children’s zone asthma initiative. Am J Public Health. 2005;95(2):245–9.
Szentpetery SE, Forno E, Canino G, Celedón JC. Asthma in Puerto Ricans: lessons from a high-risk population. J Allergy Clin Immunol. 2016;138(6):1556–8.
Gold DR, Wright R. Population disparities in asthma. Annu Rev Public Health. 2005;26:89–113. doi:10.1146/annurev.publhealth.26.021304.144528.
Litonjua AA, Carey VJ, Weiss ST, Gold DR. Race, socioeconomic factors, and area of residence are associated with asthma prevalence. Pediatr Pulmonol. 1999;28(6):394–401.
Wright RJ, Subramanian SV. Advancing a multilevel framework for epidemiologic research on asthma disparities. Chest. 2007;132(5 Suppl):757S–69S. doi:10.1378/chest.07-1904.
Mayer SE. What is a “disadvantaged group”? rainbow research. 1980.
Massey DS. Segregation and stratification. Du Bois Review. 2004;1(1):7–25.
Individuals from Disadvantaged Backgrounds. In: Diversity in extramural programs. National Institutes of Health. https://extramural-diversity.nih.gov/diversity-matters/disadvantaged-backgrounds. 2017. Accessed 6/27/2017.
Berube A, Institution B. The continuing evolution of American poverty and its implications for community development. Investing in What Works for America’s Communities 2012:59.
•• Keet CA, McCormack MC, Pollack CE, Peng RD, McGowan E, Matsui EC. Neighborhood poverty, urban residence, race/ethnicity, and asthma: rethinking the inner-city asthma epidemic. J Allergy Clin Immunol. 2015;135(3):655–62. doi:10.1016/j.jaci.2014.11.022. Utilizing nationally collected survey data this group demonstrated that the prevalence of asthma was not high in all inner-city areas, and that Black race, Puerto Rican ethnicity and income were independent risk factors for current asthma.
•• Keet CA, Matsui EC, McCormack MC, Peng RD. Urban residence, neighborhood poverty, race/ethnicity, and asthma morbidity among children on Medicaid. J Allergy Clin Immunol. 2017. Utilizing Medicaid claims data, this group showed that inner-city residence and non-Hispanic black race was associated with increased healthcare utilization in asthma.
Kattan M, Mitchell H, Eggleston P, Gergen P, Crain E, Redline S, et al. Characteristics of inner-city children with asthma. Pediatr Pulmonol. 1997;24:253–62.
Koinis-Mitchell D, McQuaid EL, Seifer R, Kopel SJ, Esteban C, Canino G, et al. Multiple urban and asthma-related risks and their association with asthma morbidity in children. J Pediatr Psychol. 2007;32(5):582–95.
Crain EF, Kercsmar C, Weiss KB, Mitchell H, Lynn H. Reported difficulties in access to quality care for children with asthma in the inner city. Arch Pediatr Adolesc Med. 1998;152(4):333–9.
Wade S, Weil C, Holden G, Mitchell H, Evans R, Kruszon‐Moran D, et al. Psychosocial characteristics of inner‐city children with asthma: a description of the NCICAS psychosocial protocol. Pediatr Pulmonol. 1997;24(4):263–76.
Kopel LS, Gaffin JM, Ozonoff A, Rao DR, Sheehan WJ, Friedlander JL, et al. Perceived neighborhood safety and asthma morbidity in the school inner-city asthma study. Pediatr Pulmonol. 2015;50(1):17–24. doi:10.1002/ppul.22986.
Williams DR, Sternthal M, Wright RJ. Social determinants: taking the social context of asthma seriously. Pediatrics. 2009;123(Supplement 3):S174–S84.
•• Beck AF, Huang B, Auger KA, Ryan PH, Chen C, Kahn RS. Explaining racial disparities in child asthma readmission using a causal inference approach. JAMA Pediatr. 2016;170(7):695–703. Using directed acyclic graphing (DAG) or causal inference modeling in an observational cohort, this group examined the association between disease management, environmental, biological, access to care, socioeconomic status variables and unmeasured variables; and pediatric asthma readmissions.
•• Cardet JC, Louisias M, King TS, Castro M, Codispoti CD, Dunn R, et al. Income is an independent risk factor for worse asthma outcomes. J Allergy Clin Immunol. 2017. Secondary analysis of a randomized controlled asthma trial that found low income as a risk factor for asthma morbidity independent of race, education, perceived stress and adherence.
Zoratti EM, Krouse RZ, Babineau DC, Pongracic JA, O'Connor GT, Wood RA, et al. Asthma phenotypes in inner-city children. J Allergy Clin Immunol. 2016;138(4):1016–29.
•• Hughes HK, Matsui EC, Tschudy MM, Pollack CE, Keet CA. Pediatric asthma health disparities: race, hardship, housing, and asthma in a national survey. Acad Pediatr. 2017;17(2):127–34. Secondary analysis of American Housing Survey demonstrating that material hardship such as poor housing quality or lack of household amenities is associated with worse asthma morbidity.
• Kopel LS, Petty CR, Gaffin JM, Sheehan WJ, Baxi SN, Kanchongkittiphon W, et al. Caregiver stress among inner-city school children with asthma. J Allergy Clin Immunol Pract. 2017. Longitudinal study of urban children with asthma where caregiver stress was examined in relation to asthma morbidity. High caregiver stress scores were associated with worse asthma morbidity outcomes.
•• Thakur N, Barcelo NE, Borrell LN, Singh S, Eng C, Davis A, et al. Perceived discrimination associated with asthma and related outcomes in minority youth: the GALA II and SAGE II studies. Chest. 2017;151(4):804–12. This group examined the association between asthma prevalence and outcomes and perceived discrimination using a modified validated questionnaire, in a case-control study group. Perceived discrimination was associated with worse asthma control and odds of asthma.
Heiman HJ, Artiga S. Beyond health care: the role of social determinants in promoting health and health equity. Health. 2015;20(10)
•• Gold DR, Adamkiewicz G, Arshad SH, Celedón JC, Chapman MD, Chew GL, et al. NIAID, NIEHS, NHLBI, and MCAN workshop report: the indoor environment and childhood asthma—implications for home environmental intervention in asthma prevention and management. J Allergy Clin Immunol. 2017. Report from a workshop of international experts, that reviews and provides recommendations on current research on environmental remediation to prevent or control asthma.
• Gergen PJ, Teach SJ, Togias A, Busse WW. Reducing exacerbations in the inner city: lessons from the inner-city asthma consortium (ICAC). J Allergy Clin Immunol Pract. 2016;4(1):22–6. Great summary of the outcomes and lessons learned from the Inner-City Asthma Consortium studies.
Gergen PJ, Mortimer KM, Eggleston PA, Rosenstreich D, Mitchell H, Ownby D, et al. Results of the national cooperative inner-city asthma study (NCICAS) environmental intervention to reduce cockroach allergen exposure in inner-city homes. J Allergy Clin Immunol. 1999;103(3):501–6.
•• Le Cann P, Paulus H, Glorennec P, Le Bot B, Frain S, Gangneux JP. Home environmental interventions for the prevention or control of allergic and respiratory diseases: what really works. J Allergy Clin Immunol Pract. 2017;5(1):66–79. Comprehensive review of home environmental remediation and what are the most effective approaches.
Morgan WJ, Crain EF, Gruchalla RS, O'Connor GT, Kattan M, Evans R III, et al. Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;351(11):1068–80.
Matsui EC, Perzanowski M, Peng RD, Wise RA, Balcer-Whaley S, Newman M, et al. Effect of an integrated pest management intervention on asthma symptoms among mouse-sensitized children and adolescents with asthma: a randomized clinical trial. JAMA. 2017;317(10):1027–36.
Rabito FA, Carlson JC, He H, Werthmann D, Schal C. A single intervention for cockroach control reduces cockroach exposure and asthma morbidity in children. J Allergy Clin Immunol. 2017.
DiMango E, Serebrisky D, Narula S, Shim C, Keating C, Sheares B, et al. Individualized household allergen intervention lowers allergen level but not asthma medication use: a randomized controlled trial. J Allergy Clin Immunol Pract. 2016;4(4):671–9. e4
•• Sheehan WJ, Permaul P, Petty CR, Coull BA, Baxi SN, Gaffin JM, et al. Association between allergen exposure in inner-city schools and asthma morbidity among students. JAMA Pediatr. 2017;171(1):31–8. First longitudinal study in the United States examining the association between allergen exposure in urban schools and asthma outcomes. Mouse allergen exposure was associated with more asthma symptoms and decreased lung function.
Kay Bartholomew L, Sockrider MM, Abramson SL, Swank PR, Czyzewski DI, Tortolero SR, et al. Partners in school asthma management: evaluation of a self‐management program for children with asthma. J Sch Health. 2006;76(6):283–90.
Huffaker M, Phipatanakul W. Introducing an environmental assessment and intervention program in inner-city schools. J Allergy Clin Immunol. 2014;134(6):1232–7.
Phipatanakul W, Bailey A, Hoffman EB, Sheehan WJ, Lane JP, Baxi S, et al. The school inner-city asthma study: design, methods, and lessons learned. J Asthma. 2011;48(10):1007–14.
Jhun I, Gaffin JM, Coull BA, Huffaker MF, Petty CR, Sheehan WJ, et al. School environmental intervention to reduce particulate pollutant exposures for children with asthma. J Allergy Clin Immunol Pract. 2017;5(1):154–9. e3
Phipatanakul W, Koutrakis P, Coull BA, Kang C-M, Wolfson JM, Ferguson ST, et al. The school inner-city asthma intervention study: design, rationale, methods, and lessons learned. Contemp Clin Trials. 2017;60:14–23.
David S, Gerald LB, Jenkins I, Clemens C, Brown MA, Billheimer D, et al. School-based asthma management programs could provide a source of care for children who otherwise lack access. b94. reducing health disparities for children with asthma. Am Thoracic Soc. 2015. P. A3630-A.
Bruzzese J-M, Evans D, Kattan M. School-based asthma programs. J Allergy Clin Immunol. 2009;124(2):195–200.
• Kakumanu S, Antos N, Szefler SJ, Lemanske RF Jr. Building school health partnerships to improve pediatric asthma care: the school-based asthma management program. Curr Opin Allergy Clin Immunol. 2017;17(2):160–6. Review of SAMPRO, recent initiative of the Academy of Allergy, Asthma and Immunology and the National Association of School Nurses, which is a framework for coordinated school asthma partnerships.
Lemanske RF, Kakumanu S, Shanovich K, Antos N, Cloutier MM, Mazyck D, et al. Creation and implementation of SAMPRO™: a school-based asthma management program. J Allergy Clin Immunol. 2016;138(3):711–23.
Cloutier MM. Asthma management programs for primary care providers: increasing adherence to asthma guidelines. Curr Opin Allergy Clin Immunol. 2016;16(2):142–7.
Bradley CL, Luder HR, Beck AF, Bowen R, Heaton PC, Kahn RS, et al. Pediatric asthma medication therapy management through community pharmacy and primary care collaboration. J Am Pharm Assoc. 2016;56(4):455–60.
Shuler MS, Yeatts KB, Russell DW, Trees AS, Sutherland SE. The regional asthma disease management program (RADMP) for low income underserved children in rural western North Carolina: a national asthma control initiative demonstration project. J Asthma. 2015;52(9):881–8.
Janevic MR, Baptist AP, Bryant-Stephens T, Lara M, Persky V, Ramos-Valencia G, et al. Effects of pediatric asthma care coordination in underserved communities on parent perceptions of care and asthma-management confidence. J Asthma. 2017;54(5):514–9.
•• Anise A, Hasnain-Wynia R. Patient-centered outcomes research to improve asthma outcomes. J Allergy Clin Immunol. 2016;138(6):1503–10. Describes eight PCORI funded comparative effectiveness programs to improved patient-centered outcomes in Black and Latino patients with uncontrolled asthma. It highlights how these projects are overcoming evidence gaps and utilizing multicomponent research strategies to reduce disparities.
Bryant-Stephens T, Reed-Wells S, Canales M, Perez L, Rogers M, Localio AR, et al. Home visits are needed to address asthma health disparities in adults. J Allergy Clin Immunol. 2016;138(6):1526–30.
Kramer CB, LeRoy L, Donahue S, Apter AJ, Bryant-Stephens T, Elder JP, et al. Enrolling African-American and Latino patients with asthma in comparative effectiveness research: lessons learned from 8 patient-centered studies. J Allergy Clin Immunol. 2016;138(6):1600–7.
Portnoy JM, Waller M, De Lurgio S, Dinakar C. Telemedicine is as effective as in-person visits for patients with asthma. Ann Allergy Asthma Immunol. 2016;117(3):241–5.
Scott L, Li M, Thobani S, Nichols B, Morphew T, Kwong KY-C. Asthma control and need for future asthma controller therapy among inner-city Hispanic asthmatic children engaged in a pediatric asthma disease management program (the Breathmobile program, mobile asthma care for kids network). J Asthma. 2016;53(6):629–34.
Tschudy MM, Cheng TL. The “black box” of racial disparities in asthma. JAMA Pediatr. 2016;170(7):644–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Funding Information
Dr. Louisias was supported by NIH grant K12HS022986. Dr. Phipatanakul received funds from NIAID K24AI 106822 U01 AI 110397 U01 AI 126614.
Additional information
Data sources: A literature search was performed in PubMed. Studies focusing on inner-city populations
This article is part of the Topical Collection on Allergies and the Environment
Rights and permissions
About this article

Cite this article
Louisias, M., Phipatanakul, W. Managing Asthma in Low-Income, Underrepresented Minority, and Other Disadvantaged Pediatric Populations: Closing the Gap. Curr Allergy Asthma Rep 17, 68 (2017). https://doi.org/10.1007/s11882-017-0734-x
Published:
DOI: https://doi.org/10.1007/s11882-017-0734-x