
Abstract
Prevention of occupational asthma related to a work-sensitizing agent ideally would be achieved by avoidance of exposures that cause immunologic sensitization and subsequent asthma. There are a few examples in which a sensitizing agent has been removed from a work process and others in which exposure has been significantly changed or reduced with associated reduced rates of sensitization and disease. Additional measures include containment, use of robots, ventilation measures, exposure monitoring, and use of respiratory protective devices. Secondary prevention includes medical surveillance, which may involve periodic respiratory questionnaires, spirometry, and immunologic tests aiming to detect sensitization or disease early to allow intervention and improve outcomes. Education measures for workers to understand the meaning of work-related respiratory symptoms and appropriate workplace safety measures have not been formally evaluated but may also be expected to enhance protective measures and lead to earlier diagnosis. Tertiary prevention includes medical management and workers’ compensation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Occupational asthma (OA) has been reported to be the most common chronic occupational disease in many developed countries [1, 2], and as with other occupational lung diseases, it is potentially preventable. It refers to de novo asthma or recurrence of previously quiescent asthma (ie, asthma as a child or in the distant past that has been in remission) induced by sensitization to a specific substance (eg, an inhaled protein [high molecular weight] or a chemical at work [low molecular weight], termed sensitizer-induced OA) or by exposure to an inhaled irritant at work, termed irritant-induced OA [3]. This is distinct from the other form of work-related asthma, work-exacerbated asthma, which refers to preexisting asthma (or coincidental onset of asthma at work) that is not caused by work but is exacerbated by work exposures [3]. This is not included in this review.
Epidemiologic studies consistently show a high occupational contribution to the burden of asthma. A 2007 publication estimated population attributable risk for adult asthma due to occupational exposures to be 10% to 25% [4], using a definition of new-onset asthma and exposure to work substances recognized to cause asthma from an exposure matrix. This was very similar to earlier estimates [5] and to the estimate of 16.5% from a systematic review in 2009 [6]. OA has been reported in up to 16% of snow crab workers [7] and in 6% of apprentice bakers after 2 years [8]. However, findings suggest a reduction in prevalence and incidence of OA in recent years among animal workers [9] and a fall in incidence from exposure to agents such as diisocyanates and natural rubber latex (NRL) [10, 11, 12•, 13, 14], suggesting benefit from preventive measures. Indirect evidence from compensated OA claims in Ontario, Canada, also shows declines in yearly numbers of OA since the late-1990s compared with earlier periods [15, 16].
Recent epidemiologic studies have suggested the importance of less traditional causes of OA. In New Zealand, printers and sawmill laborers also were among those with the strongest risks [17], and the European Community Respiratory Health Survey [4] has shown the highest risks among cleaners and nurses. Although the latter findings are supported by other studies [12•, 18, 19], the causative agents and mechanisms are not clear at this time.
Irritant-induced OA accounts for a minority of OA in most case series. In the most definitive form, reactive airways dysfunction syndrome, it generally relates to an unexpected and accidental very high respiratory irritant exposure. Prevention may include good occupational hygiene and safety measures at work, with education of workers to react appropriately in the event of an accident to minimize their exposure. An example in which asthma and airway disease might have been prevented, at least in some workers, is the exposure of firefighters and other workers at the New York World Trade Center collapse, which resulted in an exposure-related significant increase in asthma from the highly alkaline dust exposure [20], when most workers were not routinely wearing the available respiratory protective equipment at the site [21]. Following an accidental exposure of workers, medical management of those who develop irritant-induced OA is similar to that for non-work-related asthma to reduce impairment [3].
The remainder of this article addresses prevention of sensitizer-induced OA, and as for other occupational diseases, it is considered in terms of primary, secondary, and tertiary prevention.
Primary Prevention
Primary prevention is the ideal form of prevention (ie, workers do not become sensitized to agents that can cause asthma). It involves taking measures to avoid exposure of workers to agents that can cause asthma (Table 1). Although sensitizers often cannot be completely removed from workplaces, it is often possible to reduce exposures to levels that are protective.
Changes to digital imaging in radiography, and use of digital photography illustrate how technological advances can result in primary prevention of OA. In these examples, digital imaging removes the need for photographic processing and developing chemicals (which include sensitizers and irritants) in settings that previously were associated with OA [22]. Another change in many hospital areas is from the use of glutaraldehyde for sterilization (eg, of endoscopes) to other agents, such as ortho-phthalaldehyde; although it is also a sensitizer [23], it appears to be less potent in causing OA. Less volatile products may reduce exposure (eg, methyl-diphenyl diisocyanate, for which production has increased relative to the much more volatile toluene diisocyanate). However, methyl-diphenyl diisocyanate, when heated or sprayed, can result in exposures that can lead to sensitization and OA. Changes in diisocyanate formulation in products, such as spray paint, with greater use of polymeric forms would be expected to result in these products having lower potency as sensitizers. It is unclear whether and to what extent the apparent decline in diisocyanate asthma [10, 16] may relate to such changes compared with other preventive measures.
Another example of complete avoidance of a sensitizer is the replacement of unnecessary NRL gloves with vinyl gloves for food handlers and cleaners/hospital housekeepers, preventing their risk of sensitization to NRL.
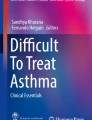
When sensitizers cannot be completely removed from the workplace, evidence supports the importance of reducing exposure. For many occupational sensitizers, the risk of sensitization (and asthma) relates partly to the level of exposure (in addition to host factors such as atopy and genetic factors). Changes in production methods for NRL gloves to increase leaching of proteins from gloves (resulting in lower glove protein) and reduce powder in the gloves (to reduce airborne carriage of NRL proteins) with other preventive measures have been associated with a marked decline in rates of NRL allergy and asthma among health care workers (Fig. 1) [13, 14, 24].

Reduction of compensated claims for natural rubber latex in health care workers in Ontario after introduction of preventive measures. Arrows refer to dates of interventions. aIntervention measures at the largest Ontario hospital included changes to low-protein, low-powder, nonsterileb, and sterilec gloves. WSIB Workplace Safety and Insurance Board. (Adapted from Liss and Tarlo [13]; with permission.)
Similarly, encapsulation of enzymes markedly reduced exposure and risks of sensitization in detergent production workers [25]. Reduced allergen exposure similarly might explain the apparent reduced rates of OA in laboratory animal workers [9] as occupational hygiene measures that effectively reduce air concentrations of animal allergens have been well-described, such as negative pressure in cages, local exhaust during cage changing, and appropriate use of respirators [26].
Other methods to reduce exposures to sensitizing agents at work include use of robotics in enclosed settings (eg, polyurethane foam manufacturing plants using diisocyanates). Spray painting with paints containing diisocyanates should be performed with use of an air-supplied respirator in a spray booth with negative pressure ventilation and separate exhaust in order to limit exposure to the worker and to others outside the booth. Exposure monitoring to ensure that levels are within allowable ranges is mandated in some jurisdictions. These measures may have contributed to relative declines in OA from diisocyanates.
When the environmental exposure cannot be reduced sufficiently, use of respiratory protective equipment is recommended (although this is lower on the hierarchy of primary prevention measures). Unfortunately, respirators can be uncomfortable, especially if they need to be worn for prolonged periods, and they are only effective if the correct protective device is provided, if it fits the face correctly, and if it is worn by the worker. Compliance is often low [27] and has been associated with several factors, including lack of awareness of safety precautions [28]. The role of worker education is vital in this regard. Of note, in a study of school cleaners, rates of self-reported asthma symptoms being worse at work than at home were found to be higher in those who did not receive or understand work safety training [29]. Canada’s Workplace Hazardous Materials Information System includes safety training, product labeling, and provision of material safety data sheets, and in the United States, the Occupational Safety and Health Administration regulations include Right to Know legislation.
A further consideration in primary prevention is avoiding the introduction of new sensitizing products into work processes. Each year, new sensitizers are reported to cause OA; if these could be predicted, then perhaps other, nonsensitizing substances could be used instead. In general, it is very likely that any inhaled protein will be a potential respiratory sensitizer, but it is not as easy to predict new chemical sensitizers. Many highly reactive low molecular weight chemicals are respiratory sensitizers, and attempts have been made to predict capacity to cause sensitization by examining the presence of two or more reactive components (such as the N–C=O found in diisocyanate compounds) among known chemical sensitizers and developing predictors that are then applied to a validation group of chemicals and subsequently externally validated [30•]. Attempts also have been made to develop animal models of sensitization that may be predictive of human exposures [31, 32], but no publications to date have prospectively indicated the outcome of these predictive methods in practice.
Finally, although host factors (atopy, some genetic markers, and smoking) have been associated with development of OA with some agents, these factors to date are not sufficiently predictive to exclude workers from jobs with sensitizing agents. However, those identified as being at greater risk may benefit from closer monitoring during medical surveillance (discussed subsequently) and from education to identify early symptoms suggesting sensitization. Host factors such as severe, preexisting asthma may lead to preplacement relocation if further sensitization and worsening of the underlying asthma may be particularly hazardous for the worker.
Secondary Prevention
Secondary prevention consists of medical surveillance to allow early detection of workers who have been sensitized to occupational agents or early detection of OA, preferably at a time when removal from further exposure may result in disease resolution. Most programs consist of periodic respiratory questionnaires, immunologic tests when feasible (skin tests or in vitro assays), and spirometry.
Benefits for the individual worker relate to the early diagnosis of occupational sensitization or disease at a time when intervention (usually removal from further exposure to the sensitizer) is most likely to minimize subsequent morbidity and possibly mortality. The health benefit for OA from early detection and removal from further exposure versus ongoing exposure to the work sensitizer is supported by findings from systematic reviews in the United Kingdom and North America [33, 34].
In addition to these benefits from interventions for individual workers, positive immunologic findings, even without clinical disease, can reflect inadequately controlled exposures in the workplace. This can trigger investigation and correction, with the subsequent benefit of primary prevention of further sensitization and disease in coworkers, as has been applied in the detergent industry using skin prick test results with detergent enzyme extracts [35]. When positive skin tests are detected, some detergent companies initiate an investigation into workplace exposures to enzymes in the area of the affected workers so that corrective measures can be taken to reduce exposures.
Respiratory benefits of a medical surveillance program are intuitive, and early detection of those with OA with removal from further exposure is generally accepted as important, but nevertheless, relatively little evidence is available to assess the effectiveness of such programs. One difficulty is that occupational medical surveillance programs for OA are seldom (if ever) conducted as isolated interventions. As has been noted, the occupational setting does not lend itself to randomized controlled studies [36]. There often is concurrent exposure surveillance (as in the Ontario diisocyanate surveillance program [37]) plus actual reduction of exposure as primary prevention. In addition, worker education commonly accompanies medical surveillance programs, so these workers may be more adherent to safety measures at work, which could reduce rates of exposure and sensitization. These could also lead to earlier self-recognition of work-related asthma symptoms and earlier discussion of these with a personal physician (separate from the surveillance program), which may also lead to early referral and investigation for OA and an earlier diagnosis than may have occurred without the worker education and understanding [38, 39•].
Examples of medical surveillance programs (along with other interventions) that have been associated with declines in OA include medical surveillance for OA in diisocyanate workers in Ontario [40]. This program was mandated by legislation in 1983, and analyses of workers’ compensation claims following the establishment of the program indicated an initial increase in claims (consistent with greater case finding) followed by a sustained fall (not observed for OA claims due to other asthma-causing agents) [16]. This was consistent with reduced disease that may have resulted from better control of exposures and/or earlier diagnoses when disease may have been mild and may have cleared with relocation, thus eliminating the need for a compensation claim. An additional impressive finding was an association with an earlier time to diagnosis after establishment of the medical surveillance program [16]. However, in that study, the time to diagnosis of other causes of OA also decreased during the same period, suggesting that other factors also may have contributed, such as better knowledge and awareness of OA among primary physicians (perhaps related to educational programs and publications covering this topic).
Other studies that have demonstrated the ability of medical surveillance programs to detect OA include reports among bakers [41], enzyme workers [25], platinum workers [42], and workers exposed to acid anhydrides [43].
Although it has been difficult to determine the relative benefit of a formal medical surveillance program compared with factors such as concurrent education and exposure control, it also has been difficult to determine which component(s) of a program itself may be most useful and how often components of the program should be administered. Most programs include a respiratory questionnaire to detect symptoms consistent with asthma. Although some questions for asthma items have been validated, there is no generally accepted and validated questionnaire for medical surveillance of OA. It also may be relevant to detect work-related nasal symptoms, as they often precede the development of OA and at the least may suggest the need for closer monitoring of that worker.
A disadvantage of questionnaires is the possibility of reduced sensitivity if symptoms are present but not reported, as was suggested in some studies of bakery workers [44, 45]. This may be expected to occur more often in workplaces with low job security, in which the affected worker cannot be accommodated in a safe area at the company without exposure to the sensitizer and may risk a pay cut or job loss if the diagnosis is reached (eg, for those in a small company). Conversely, the potential also exists for overreporting of symptoms on a questionnaire. Therefore, additional objective tests as part of surveillance are desirable, preferably those with good test characteristics.
Spirometry is commonly included in medical surveillance for asthma. There are standard criteria for testing [46], but airflow limitation is not specific for asthma, and because asthma is characterized by variable airflow limitation, a normal test result does not exclude asthma, especially if it is performed at a time during which the worker is not symptomatic. It may be expected that performance at the end of shift toward the end of a working week would increase the sensitivity of the test, but no comparative studies have addressed this, and it may not be practical for a large workforce. Any additional potential value of spirometry in promoting accurate symptom reporting on the questionnaire has not been reported.
Immunologic tests also are often included when feasible, but test characteristics vary widely with different high molecular weight occupational antigen/allergen preparations [3]. Very few standardized allergen preparations are available for high molecular weight occupational allergens. Few low molecular weight sensitizers can be used for in vivo or in vitro immunologic tests (exceptions are acid anhydrides and complex platinum salts), and the test characteristics for most are suboptimal for medical surveillance.
Obvious costs associated with medical surveillance include financial costs of the program, such as questionnaire administration, skin tests, and/or in vitro immunologic tests, plus the personnel performing pulmonary function tests. Subsequent costs accrue in a subset of participants with additional follow-up diagnostic medical assessments and tests resulting from abnormalities that were found on the initial tests (of which some will be true positive surveillance results and some may be borderline or false-positive results).
Other short-term costs relate to lost work or personal time for the participants due to surveillance (eg, time for completing questionnaires and tests and lost work time if the employee needs to be removed from a job and cannot be accommodated in a different work area in the company while awaiting further physician determination of fitness for the job). There is also the potential loss of income for those who need to be removed from exposure, even if they are compensated.
Relative effectiveness of a medical surveillance program (Table 2) will be decreased if the tools used in the surveillance program have low specificity and a high false-positive rate, resulting in unnecessary additional tests and work reduction or work loss among those with the false-positive tests. Tests with low sensitivity also increase the cost-to-benefit ratio by failing to detect disease at an early stage, when intervention measures may be most effective in preventing later medical impairment. Timing of surveillance measures to occur more frequently during periods in which sensitization occurs more commonly (the first few years of exposure) is expected to increase effectiveness.
Medical surveillance’s effectiveness also depends on the extent of worker participation and rate of detection of sensitization. Brant et al. [45] reported on a three-stage medical surveillance program among a supermarket company with more than 300 in-store bakeries and about 3,000 workers in the United Kingdom. Participation in the program among bakeries was high, with 92% of bakeries participating. The program started with a questionnaire (completed by 77%), then requested a blood sample for serologic tests for specific IgE antibodies to bakery allergens among those who had work-related respiratory symptoms, but only 61% of these undertook the blood test (with a positive result in 41%). The surveillance estimate was that 1% of employees had work-related respiratory symptoms with specific IgE antibodies. In contrast, the estimate of prevalence was 4% in an independent cross-sectional survey in a subset of the same bakeries, with 93% worker participation in the testing [41]. The findings illustrate reduced participation in “real life” surveillance compared with a research study, perhaps from fear of the consequences of abnormal test results. Similarly, Mackie [47] reported on the efficacy of a United Kingdom-wide health surveillance program (that did not include immunologic tests) provided in the automotive repair industry for workers exposed to diisocyanates. Among a subset of workers referred to primary care physicians from the program for further assessment, only half attended, and of those referred to see a specialist, only 63% attended.
Finally, in addition to expecting better participation, it is likely that the socioeconomic loss after diagnosis will be less in a larger company, in which workers can be removed from the relevant exposure but continue to work with reassignment to a nonexposed area, versus smaller companies, in which affected workers may only leave the company or remain exposed to the sensitizer.
A model to determine costs and benefits from medical surveillance for diisocyanates was reported by Wild et al. [48]. Factors included the time to diagnosis with and without surveillance, disease progression with and without removal from ongoing exposure, chance of removal from exposure with and without diagnosis, and chance of recovery from asthma with and without removal from exposure. Costs included lost productivity; diagnosis costs for screening and confirmation of diagnosis; and medical/absenteeism costs with symptomatic disease, chronic disease, and disabling disease. There were limited studies from which the estimates for this model could be produced for each variable, and some were estimated by expert opinion only. The model indicated that most costs related to disability of affected workers with OA. A sensitivity analysis showed that surveillance was most cost-effective in settings with a high incidence of OA, with greater risk of disability where surveillance expedited diagnosis compared with no surveillance and where affected workers were then rapidly removed from further exposure to the sensitizer. Costs in the model were divided into costs for the employer (including costs of running the program) and costs to society (mostly from disability and lost productivity). The estimate for effectiveness, when calculated in that model as a threshold of $50,000 per quality-adjusted life-year, showed cost-effectiveness from a societal perspective if occupational sensitization was 1.1% or more per year, and from an employer perspective if sensitization rates were 1.9% or more per year. A previous empiric proposal by Baur et al. [49] suggested that medical surveillance programs be mandatory in workplaces/occupations in which asthma incidence is at least double that of the general population, and be recommended, but not mandatory, for incidence rates that are increased but less than double those of the general population.
Relative risks for asthma of 2.55 have been demonstrated in high-risk occupations (baking, hairdressing, nursing, cleaners and caretakers, painters and spray painters, electrical processers, welding, metal work, agriculture and forestry, plastics or rubber industry, chemical industry) compared with a reference group of professional, clerical, and administrative workers (clearly exceeding the empiric criteria presented by Baur et al. [49]) [4]. However, most of these occupations do not currently have routine medical surveillance programs for OA, and for several of these, there is no reliable immunologic test to include. The decision as to initiation of a formal medical surveillance program in such occupations may include practical considerations of implementation, and currently, little evidence is available to aid in such a decision. A possible alternative approach (eg, for nurses and other health care workers) may be the provision of good worker education as to possible causes of asthma from work, early symptoms, and action to take to assist in early diagnosis (eg, via occupational health programs or clinics, and provision of information to primary care physicians). Unfortunately, no formal studies have addressed this approach in comparison with a surveillance program.
Tertiary Prevention
Tertiary prevention involves medical management of OA to minimize impairment and also includes workers’ compensation programs themselves. Evidence-based reviews have concluded that removal from further exposure to the sensitizing agent carries the best prognosis. The outcome is best when this occurs with early diagnosis and with milder asthma at the time of diagnosis [34]. Other environmental and pharmacologic management is as for other asthma.
Population Surveillance
The above preventive measures have addressed specific workplaces or exposures. At the population level, public health surveillance programs (as opposed to medical surveillance) in which there is reporting of identified or suspected OA to a central organization (such as the SENSOR [Sentinel Event Notification System for Occupational Risks] program active in some states, or the SWORD [Surveillance of Work-related and Occupational Respiratory Disease] and Shield [Midland Thoracic Society’s Surveillance Scheme for Occupational Asthma] programs in the United Kingdom) can provide information as to new or changing importance of causes of OA, raising awareness and thereby facilitating diagnosis and the introduction of primary and secondary preventive measures. Similarly, publication of clinic or compensation claim reviews and epidemiologic studies can raise awareness and intervention.
Finally, for health care providers, the development of guidelines, consensus statements, and continuing medical education regarding work-related asthma, the symptoms that should lead to suspicion of diagnosis, and the importance of recognition should lead to an earlier diagnosis and better outcome of OA in their patients.
Conclusions
OA is preventable. Primary prevention remains the best approach, if it is feasible. Because primary prevention is not always successful, secondary prevention by medical surveillance has some evidence to support benefit for those working with some common occupational sensitizers. Optimizing worker education as to the potential for OA and early symptoms to suspect this, as well as ongoing education of health care professionals may also lead to earlier diagnosis and better prognosis.
References
Papers of particular interest, published recently, have been highlighted as • Of importance
Orriols R, Costa R, Albanell M, et al.: Reported occupational respiratory diseases in Catalonia. Occup Environ Med 2006, 63:255–260.
Elder D, Abramson M, Fish D, et al.: Surveillance of Australian workplace Based Respiratory Events (SABRE): notifications for the first 3.5 years and validation of occupational asthma cases. Occup Med (Lond) 2004, 54:395–399.
Tarlo SM, Balmes J, Balkissoon R, et al.: Diagnosis and management of work-related asthma: American College of Chest Physicians consensus statement. Chest 2008, 134:1S–41S.
Kogevinas M, Zock JP, Jarvis D, et al.: Exposure to substances in the workplace and new-onset asthma: an international prospective population-based study (ECRHS-II). Lancet 2007, 370:336–341.
Balmes J, Becklake M, Blanc P, et al.: American Thoracic Society statement: occupational contribution to the burden of airway disease. Am J Respir Crit Care Med 2003, 167:787–797.
Toren K, Blanc PD: Asthma caused by occupational exposures is common—a systematic analysis of estimates of the population-attributable fraction. BMC Pulm Med 2009, 9:7.
Gautrin D, Cartier A, Howse D, et al.: Occupational asthma and allergy in snow crab processing in Newfoundland and Labrador. Occup Environ Med 2010, 67:17–23.
Walusiak J, Hanke W, Gorski P, Palczynski C: Respiratory allergy in apprentice bakers: do occupational allergies follow the allergic march? Allergy 2004, 59:442–450.
Folletti I, Forcina A, Marabini A, et al.: Have the prevalence and incidence of occupational asthma and rhinitis because of laboratory animals declined in the last 25 years? Allergy 2008, 63:834–841.
Bakerly ND, Moore VC, Vellore AD, et al.: Fifteen-year trends in occupational asthma: data from the Shield surveillance scheme. Occup Med (Lond) 2008, 58:169–174.
Tarlo SM, Liss GM: Diisocyanate-induced asthma: diagnosis, prognosis, and effects of medical surveillance measures. Appl Occup Environ Hyg 2002, 17:902–908.
• Delclos GL, Gimeno D, Arif AA, et al.: Occupational risk factors and asthma among health care professionals. Am J Respir Crit Care Med 2007, 175:667–675. This large, cross-sectional survey of health care workers confirmed the findings of other studies showing that NRL was a risk factor for OA only prior to 2000, consistent with changes in glove use. Cleaning and aerosolized medications were significant risk factors throughout the study period.
Liss GM, Tarlo SM: Natural rubber latex-related occupational asthma: association with interventions and glove changes over time. Am J Ind Med 2001, 40:347–353.
Allmers H, Schmengler J, Skudlik C: Primary prevention of natural rubber latex allergy in the German health care system through education and intervention. J Allergy Clin Immunol 2002, 110:318–323.
Buyantseva LV, Liss GM, Ribeiro M, et al.: Diisocyanates and non-diisocyanates induced asthma in Ontario. Am J Resp Crit Care Med 2008, 177:A526.
Tarlo SM, Liss GM, Yeung KS: Changes in rates and severity of compensation claims for asthma due to diisocyanates: a possible effect of medical surveillance measures. Occup Environ Med 2002, 59:58–62.
Eng A, 'T Mannetje A, Douwes J, et al.: The New Zealand workforce survey II: occupational risk factors for asthma. Ann Occup Hyg 2010, 54:154–164.
Obadia M, Liss GM, Lou W, et al.: Relationships between asthma and work exposures among non-domestic cleaners in Ontario. Am J Ind Med 2009, 52:716–723.
Medina-Ramon M, Zock JP, Kogevinas M, et al.: Asthma symptoms in women employed in domestic cleaning: a community based study. Thorax 2003, 58:950–954.
Banauch GI, Dhala A, Alleyne D, et al.: Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Am J Resp Crit Care Med 2005, 33:S102–S106.
Feldman DM, Baron SL, Bernard BP, et al.: Symptoms, respirator use, and pulmonary function changes among New York City firefighters responding to the World Trade Center disaster. Chest 2004, 125:1256–1264.
Liss GM, Tarlo SM, Doherty J, et al.: Physician diagnosed asthma, respiratory symptoms, and associations with workplace tasks among radiographers in Ontario, Canada. Occup Environ Med 2003, 60:254–261.
Fujita H, Ogawa M, Endo Y: A case of occupational bronchial asthma and contact dermatitis caused by ortho-phthalaldehyde exposure in a medical worker. J Occup Health 2006, 48:413–416.
Tarlo SM, Easty A, Eubanks K, et al.: Outcomes of a natural rubber latex control program in an Ontario teaching hospital. J Allergy Clin Immunol 2001, 108:628–633.
Schweigert MK, Mackenzie DP, Sarlo K: Occupational asthma and allergy associated with the use of enzymes in the detergent industry—a review of the epidemiology, toxicology and methods of prevention. Clin Exp Allergy 2000, 30:1511–1518.
Bush RK, Wood RA, Eggleston PA: Laboratory animal allergy. J Allergy Clin Immunol 1998, 102:99–112.
Macfarlane E, Chapman A, Benke G, et al.: Training and other predictors of personal protective equipment use in Australian grain farmers using pesticides. Occup Environ Med 2008, 65:141–146.
Tam V, Fung I: A study of knowledge, awareness, practice and recommendations among Hong Kong construction workers on using personal respiratory protective equipment at risk. Open Constr Build Technol J 2008, 2:69–81.
Ricciuto DR, Obadia M, Liss GM, Tarlo SM: The effect of workplace safety training and comprehension on the incidence of occupational asthma among indoor cleaners. Chest 2006, 130:155S.
• Seed M, Agius R: Further validation of computer-based prediction of chemical asthma hazard. Occup Med (Lond) 2010, 60:115–120. A quantitative structure-activity relationship model previously described by this group showed good global predictive value for identifying respiratory asthmagens among a validation set of asthmagenic chemicals, identified agents from studies published since 1995, and control set of chemicals.
Dearman RJ, Kimber I: Cytokine fingerprinting and hazard assessment of chemical respiratory allergy. J Appl Toxicol 2001, 21:153–163.
Vanoirbeek JA, Mandervelt C, Cunningham AR, et al.: Validity of methods to predict the respiratory sensitizing potential of chemicals: a study with a piperidinyl chlorotriazine derivative that caused an outbreak of occupational asthma. Toxicol Sci 2003, 76:338–346.
Nicholson PJ, Cullinan P, Taylor AJ, et al.: Evidence based guidelines for the prevention, identification, and management of occupational asthma. Occup Environ Med 2005, 62:290–299.
Beach J, Rowe B, Blitz S, et al.: Diagnosis and Management of Work-related Asthma. Summary, Evidence Report/Technology Assessment. AHRQ Clearinghouse. Silver Springs, MD: Agency for Healthcare Research and Quality; 2005. [AHRQ publication no. 06-E003-1.]
Sarlo K, Kirchner DB: Occupational asthma and allergy in the detergent industry: new developments. Curr Opin Allergy Clin Immunol 2002, 2:97–101.
Nicholson PJ: How to undertake a systematic review in an occupational setting. Occup Environ Med 2007, 64:353–358.
Ontario Ministry of Labour: Regulation respecting isocyanates made under the Occupational Health and Safety Act, 1980. Revised statutes of Ontario Chapter 321. 1983; Ontario regulation 455/83.
Poonai N, van Diepen S, Bharatha A, et al.: Barriers to diagnosis of occupational asthma in Ontario. Can J Public Health 2005, 96:230–233.
• Santos MS, Jung H, Peyrovi J, et al.: Occupational asthma and work-exacerbated asthma: factors associated with time to diagnostic steps. Chest 2007, 131:1768–1775. This questionnaire study identified factors associated with longer than median time to diagnosis among participants with OA. The identified factors (that potentially could indicate groups in which to particularly focus preventive efforts) were male sex, being older, being unmarried, having low education, and being the sole income earner. Lack of awareness of an association of symptoms with work and lack of knowledge of the Workplace Hazardous Materials Information System program were also associated with a longer time to diagnosis, suggesting inadequate worker safety training as a risk factor.
Tarlo SM: Prevention of occupational asthma in Ontario. Can J Physiol Pharmacol 2007, 85:167–172.
Brant A, Berriman J, Sharp C, et al.: The changing distribution of occupational asthma: a survey of supermarket bakery workers. Eur Respir J 2005, 25:303–308.
Merget R, Caspari C, Dierkes-Globisch A, et al.: Effectiveness of a medical surveillance program for the prevention of occupational asthma caused by platinum salts: a nested case-control study. J Allergy Clin Immunol 2001, 107:707–712.
Grammer L, Shaughnessy M, Kenamore B: Utility of antibody in identifying individuals who have or will develop anhydride-induced respiratory disease. Chest 1998, 114:1199–1202.
Gordon SB, Curran AD, Murphy J, et al.: Screening questionnaires for bakers’ asthma—are they worth the effort? Occup Med (Lond) 1997, 47:361–366.
Brant A, Nightingale S, Berriman J, et al.: Supermarket baker’s asthma: how accurate is routine health surveillance? Occup Environ Med 2005, 62:395–399.
Miller MR, Hankinson J, Brusasco V, et al.: Standardisation of spirometry. Eur Respir J 2005, 26:319–338.
Mackie J: Effective health surveillance for occupational asthma in motor vehicle repair. Occup Med (Lond) 2008, 58:551–555.
Wild DM, Redlich CA, Paltiel AD: Surveillance for isocyanate asthma: a model based cost effectiveness analysis. Occup Environ Med 2005, 62:743–749.
Baur X, Stahlkopf H, Merget R: Prevention of occupational asthma including medical surveillance. Am J Ind Med 1998, 34:632–639.
Disclosure
Dr. Tarlo has received research grant support from Ontario and British Columbia workers’ compensation systems. No other potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tarlo, S.M., Liss, G.M. Prevention of Occupational Asthma. Curr Allergy Asthma Rep 10, 278–286 (2010). https://doi.org/10.1007/s11882-010-0118-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11882-010-0118-y