
Abstract
Background
Diabetic Charcot neuroarthropathy (DCN) is a devastating complication for people with diabetes mellitus. The failure to diagnose DCN and institute treatment in the acute phase leads to permanent deformity and significant morbidity. There is a paucity of data on the prevalence and characteristics of patients who have developed this complication of diabetes.
Aims
To determine the prevalence, clinical characteristics and outcomes of patients with DCN from 2006 to 2012.
Methods
Case finding was performed by searching three independent lists for the period 2006–2012 including: SYNGO radiology database, HIPE database of hospital discharges, and, combined list from podiatry, endocrinology, vascular surgery and orthopaedic clinics. A consensus meeting with chart review was undertaken to confirm diagnosis of DCN. A proforma was completed from chart review to determine clinical characteristics, initial treatment and outcomes for patients with DCN.
Results
Forty cases of DCN were identified, resulting in an estimated period prevalence of 0.3 %. The majority of patients were male (68 %); most patients had T2DM (73 %). Mean ± SD for age was 58 ± 10 years and mean duration of diabetes was 15 ± 9 years. In the acute phase of DCN, offloading was performed in 50 %. Bisphosphonates were administered to 5 % and surgery undertaken in 5 % of cases. 38 % of patients developed subsequent foot ulceration and 20 % required amputation.
Conclusions
This is the first prevalence estimate of DCN in Ireland. These data suggest diagnosis of DCN is missed in the acute phase. There exists a significant risk of diabetic foot ulceration and amputation with DCN.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diabetic Charcot neuroarthropathy (DCN) is a devastating complication for people with diabetes mellitus. Acute Charcot’s disease (Charcot foot; neuropathic joint, neuroarthropathy) is an uncommon complication of distal symmetrical neuropathy, and is characterised by fracture and dislocation of the bones and joints of the foot [1]. A consensus statement from the American Diabetes Association stated that the nomenclature should describe the condition as Charcot neuroarthropathy or the Charcot foot [2]. The failure to diagnose DCN and institute treatment in the acute phase is thought to lead to more severe deformity and significant morbidity than may be expected with early specialist care. The true prevalence and incidence of DCN is unknown but it is estimated to affect 0.8–8 % of diabetic populations. This frequency increases up to 10 % of diabetic patients with neuropathy when radiographic findings are used. Although prospective studies are limited, incidence rates ranging from 3 to 11.7/1000 patients per year have been reported. Patients with DCN are usually in their fifth and sixth decades of life, 80 % of them having had diabetes for at least 10 years [2].
DCN is a clinical diagnosis and requires the presence of peripheral neuropathy and a swollen foot. Acute diabetic Charcot neuroarthropathy results in a swollen hot foot which is usually painless. There may or may not exist a history of trauma. X-rays may be normal initially but changes may occur rapidly within 3–4 weeks. In the absence of early and effective offloading, acute diabetic Charcot neuroarthropathy progresses into a chronic stage with reduction in temperature and permanent deformity. X-rays, MRI scans and isotope bone scans support the diagnosis. X-rays may be negative in the acute phase but if clinical suspicion remains high, urgent MRI should be performed [1]. The pathogenesis of DCN is not known, but it is thought that a subgroup of patients with distal symmetrical neuropathy is at risk and that the condition is triggered in this group by local inflammation. This inflammation may be caused by minor trauma, surgery, infection or earlier ulceration [1]. Initial treatment of acute DCN is offloading of the affected foot. This is achieved through a non-removable below-knee cast or cast-walker and is an essential part of management [3]. Bisphosphonates have been shown to be effective for reducing bone turnover markers and skin temperature in some studies [4–6]. Despite these observations, the long-term clinical benefit, in reducing deformity and ulceration, of non-removable offloading or bisphosphonate therapy has not yet been proven [1, 7]. Surgical treatment is based on expert opinion and retrospective case series. Surgery has generally been advised for resecting infected bone (osteomyelitis), removing bony prominences that could not be accommodated with therapeutic footwear or custom orthoses, or correcting deformities that could not be successfully accommodated with therapeutic footwear, custom ankle/foot orthoses, or a Charcot restraint orthotic walker (CROW) [1, 7].
The development of a register for DCN provides information on the management, prevalence and natural history of DCN. Multi-disciplinary care has been shown effective in the treatment of diabetic foot syndrome [8]. Ultimately, along with structured diabetic podiatric care this should lead to improved outcomes. The aim of this study was to perform an observational retrospective analysis to estimate the prevalence of DCN. Further analysis of demographics, attendance at an MDT and outcome data of patients was also assessed.
Methods
The study investigated the patients attending the catchment area of Saint Vincent’s University Hospital, Dublin in the southeast catchment area. This included St. Columcille’s hospital, Loughlinstown, County Dublin and St. Michael’s hospital Dun Laoghaire, County Dublin. The case finding was performed by searching three independent lists for the period 2006–2012 including: (1) SYNGO radiology database. The SYNGO© radiology information system (Siemens Dublin, Ireland) is an electronic radiology system used to view, report and store data utilised in hospitals in Ireland. The terms Charcot, diabetes, diabetes mellitus, neuropathic joint and neuroarthropathy were used as search terms for identifying cases in the SYNGO database. (2) Hospital Inpatient Enquiry (HIPE) database of hospital inpatient discharges and (3) combined list from podiatry, endocrinology, vascular surgery and orthopaedic clinics. This was obtained by contacting all podiatrists, endocrinologists, orthopaedic surgeons and vascular surgeons in St. Vincent’s University hospital. After identification of the subjects, a consensus meeting with chart review was undertaken to confirm diagnosis of DCN. This was performed by a consultant endocrinologist, specialist registrar in endocrinology and a senior diabetes podiatrist. A diagnosis of Charcot joint was taken as the diagnosis when Charcot was documented in the medical chart. A prerequisite was that the patient had documented neuropathy, a deformed joint, and evidence of DCN characteristics from radiology reports. A proforma was completed from chart review to determine clinical characteristics, initial treatment and outcomes for patients with DCN (Fig. 1). Data were recorded for diabetes type, duration and presence of macro- or microvascular complications. Data were anonymised and the audit form was registered with the St. Vincent’s University Hospital audit department. The estimated prevalence was based on the total number of patients with DCN in the catchment area divided by the estimated population of patients with diabetes in the catchment area recorded for 2013.

Audit proforma template
Results
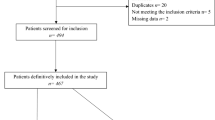
The study identified 40 cases of DCN from 2006 to 2012. The HIPE search identified 12 patients. The yield from searching the SYNGO database was 15 patients. The yield from attendances at clinic visits was 32. The initial yield from using search terms in the SYNGO database search was 503, however, following review of reports and confirmation by chart review, the final yield was 15. There was overlap noted between lists with 40 the total number of patients identified. The estimated prevalence of diabetes mellitus in Wicklow and south Dublin catchment area for 2013 is 15,608 resulting in an estimated period prevalence for DCN of 0.3 %.
Figure 2 describes the typical X-ray findings of a patient with a mid-foot Charcot joint.

X-rays of DCN. a Weight-bearing X-ray of charcot joint, b antero-posterior view of charcot joint. In the mid-foot, Lisfranc fracture or dislocation develops with bony fragmentation of the tarso-metatarsal joints and collapse of the longitudinal arch. X-rays reveal demineralisation, bone destruction and periosteal reaction
Table 1 describes the clinical characteristics of patients with diabetes mellitus and DCN. The presence of peripheral vascular disease was determined by clinical examination, the use of ankle-brachial indices and toe pressure testing. From review of the medical records, 2 % of patients had documented peripheral vascular disease. Coronary artery disease, defined as either myocardial infarction or coronary artery stent insertion was present in 18 %. A history of a cerebrovascular accident was present in 5 % of cases. The presence of neuropathy was determined by standard clinical examination using a 10 g monofilament and 128 Hz tuning fork assessment. From review of the medical records, 100 % of patients had documented peripheral neuropathy. The study demonstrated that 100 % of patients had plain X-rays performed, 38 % underwent MRI imaging of the affected foot and 15 % had isotope bone scans performed. The anatomical distribution of DCN revealed 78 % of DCN were mid-foot in location and 22 % of cases of DCN affected the ankle joint or hind-foot. DCN involved the right foot in 60 % of cases and the left foot in 37.5 % of cases. There was one case of bilateral Charcot joint (2.5 %).
It was recorded what healthcare professional made the initial diagnosis of DCN and 35 % of cases were diagnosed by an endocrinologist, 20 % of cases diagnosed by a podiatrist, 20 % diagnosed by an orthopaedic surgeon and 15 % by a vascular surgeon. It was not identified who diagnosed DCN in 10 % of cases. There were 25 % of cases reviewed at MDT and 43 % were diagnosed within the final 2 years of the analysis.
In the acute phase of DCN, 50 % of patients received no treatment. Offloading was administered in 50 % of cases. Offloading was performed usually by rest, total contact casting, or total contact insole. Non-removable total contact casting was used in 22.5 % of subjects in the total case series. Bed-rest was advised in 10 % of cases of acute DCN. Bisphosphonates therapy was initiated in the acute phase for 5 % of patients. Bisphosphonates were used in conjunction with offloading. Surgery was performed in the acute phase in 5 % of cases. A Charcot restraint orthotic walker (CROW) was prescribed in 2.5 % of patients.
Outcome data for patients who had progressed through the acute phase was recorded. At the time of analysis 10 % of patients underwent corrective orthopaedic surgery, 38 % of patients developed subsequent foot ulceration and 20 % required amputation. In patients who did not receive any offloading in the acute phase, 47 % had subsequent ulceration, 23 % required lower limb amputation and 5 % underwent corrective surgery to remove deformity.
In patients who received offloading in the acute phase, 40 % developed subsequent ulceration, 17 % required lower limb amputation and 11 % underwent corrective surgery to remove deformity at the time of analysis. The amputations reported in the study were all major amputations and all below-knee amputations. There were no trans-metatarsal amputations or minor amputations.
Further outcome analysis of patients was performed and outcomes were determined for subjects who either underwent offloading with a non-removable total contact cast, a removable offloading device or those who did not receive offloading. Of the eight subjects who were treated with a non-removable total contact cast 75 % (6) did not develop ulceration or amputation, 25 % (2) developed ulceration and 12.5 % (1) underwent amputation. Of the 12 patients who received offloading, but not with a non-removable total contact cast, 66 % (8) developed ulceration, 16 % (2) underwent amputation and 16 % (2) did not develop ulceration or undergo amputation.
There was significantly less ulceration in those subjects who received offloading with a non- removable total contact cast as compared to subjects who received a removable offloading device. There was no significant difference in amputation outcomes between the two groups. No significant difference was demonstrated in ulceration or amputation outcomes when removable or non-removable offloading was compared to no-offloading.
Statistical analysis was performed using the Chi-square test (MiniTab 17™ software).
Conclusions
This is the first prevalence estimate of DCN in Ireland. A strength of this estimate is the use of three independent lists which increases the number of cases identified. Previous work by Game et al. analysed cases of acute Charcot foot using an internet-based questionnaire [1]. Cases were not confirmed from chart review and diagnostic criteria were not specified. The prevalence of DCN in the current study is lower than is reported in the literature, however, the methodology used in this retrospective analysis is robust as cases were confirmed using chart review.
It is possible that there is under ascertainment of DCN in the population with diabetes mellitus in the catchment area, as the diagnosis is frequently missed. Healthcare providers may not be familiar with the diagnosis or the characteristic presentation. X-rays may not be performed in patients presenting with the clinical complex of neuropathy, erythema, swelling and increased temperature affecting the foot of a patient with diabetes mellitus. As the population of people diagnosed with diabetes mellitus increases, the prevalence of patients with this condition will likely increase.
The characteristics of patients are similar to previous studies with a documented long duration of diabetes, suboptimal glycaemic control and the presence of peripheral neuropathy in the majority of patients. The HbA1c at diagnosis (as reported in Table 1) does not reflect the average glycaemic control over the previous 15 years, which was the average duration of diabetes mellitus in the study population. On review of previous available laboratory reports, the HbA1c of the study population was greater than 53 mmol/mol, indicating chronic suboptimal glycaemic control. This results in consequent increased risk of complications, specifically neuropathy. This presence of long-term suboptimal glycaemic control in the study population is supported by the result that 100 % of the study population demonstrated evidence of diabetic peripheral neuropathy.
Our data report that 50 % of DCN did not have offloading treatment instituted in the acute phase. Based on this observation, and as discussed above, it is postulated the reason is that the diagnosis is made after the acute phase. This may be due to the patient with acute DCN not presenting for medical attention or that the diagnosis was missed, and in the absence of offloading, a chronic Charcot foot with structural deformity developed. Offloading is the most effective treatment for acute DCN and can arrest the progression of the condition and prevent the resultant permanent deformity [2].
The results suggest that there is benefit in improving outcomes when offloading is implemented in the acute phase. There was a significant difference observed in the study population with less ulceration in those who received non-removable total contact casting offloading as compared to those who received removable offloading devices. This is likely due to non-compliance with removable offloading devices. The prevention of ulceration is seen as a critical outcome benefit as it will reduce the risk of subsequent amputation. Consensus management guidelines for acute DCN recommend offloading as the gold standard of care [1, 7]. Our results support the use of a non-removable total contact cast as the optimal offloading strategy in the acute phase of DCN. It is acknowledged, however, that no significant difference was demonstrated in ulceration or amputation when removable or non-removable offloading was compared to no-offloading, this is likely not the true case as the numbers in the case series are small and a larger cohort would provide more definitive information.
All patients had X-rays performed. X-rays may be normal early in the disease and MRI imaging demonstrates higher sensitivity and specificity, however, MRI scans were only performed in 38 % of patients. It is evident that patients with DCN present to a variety of medical and surgical specialities. Bisphosphonates were administered in 5 % of cases of acute DCN. The evidence for benefit in use of bisphosphonates in acute DCN is inconclusive. Bisphosphonates are known to reduce temperature but do not reduce time to removal of pressure relieving treatments. Some studies have suggested that bisphosphonates may in fact lengthen the resolution phase of the disease. Despite demonstrating a short term reduction in temperature and bone turnover markers, the current available data are too weak to support the use of bisphosphonates as a routine treatment for acute Charcot neuroparthropathy [4–7, 9].
Significant burden to individual patients and healthcare system resources is highlighted by 38 % of patients developing subsequent foot ulceration and 20 % required amputation. The outcome of ulceration is similar to previous reported case series, where ulceration was recorded at 35 %, with ulceration in our study at 38 % [1]. The abnormally shaped foot observed in chronic DCN results in increased mechanical pressure points throughout the foot. This, in parallel with significant peripheral neuropathy results in unperceived injury and increased risk of ulceration and amputation.
The development of a nationwide register would further inform healthcare providers on the incidence, cost and potentially the aetiology of DCN. To increase the recognition of the disease and improve management, the development of a register and the introduction of a dedicated Charcot clinic would improve outcomes. The provision of educational workshops to healthcare providers would also increase the recognition of the acute Charcot joint and allow the early implementation of offloading strategies.
In addition, the foot burden accruing to the patient in terms of diabetic foot ulceration and amputation due to late presentation is large. The introduction of an expanded podiatry service and formal diabetic foot MDT appears to have had a positive impact on detection rates and enhanced management plans for those patients developing DCN.
References
Game FL, Catlow R, Jones GR, Edmonds ME, Jude EB, Rayman G, Jeffcoate WJ (2012) Audit of acute Charcot’s disease in the UK: the CDUK study. Diabetologia 55:32–35
Rogers LC, Frykberg RG, Armstrong DG, Boulton AJ, Edmonds M, Van GH, Hartemann A, Game F, Jeffcoate W, Jirkovska A, Jude E, Morbach S, Morrison WB, Pinzur M, Pitocco D, Sanders L, Wukich DK, Uccioli L (2011) The Charcot foot in diabetes. Diabetes Care 34(9):2123–2129
Gouveri E, Papanas N (2011) Charcot osteoarthropathy in diabetes: a brief review with an emphasis on clinical practice. World J Diabetes 2(5):59–65
Jude EB, Selby PL, Burgess J, Lilleystone P, Mawer EB, Page SR, Donohoe M, Foster AV, Edmonds ME, Boulton AJ (2001) Bisphosphonates in the treatment of Charcot neuroarthropathy: a double-blind randomised controlled trial. Diabetologia 44:2032–2037
Pitocco D, Ruotolo V, Caputo S, Mancini L, Collina CM, Manto A, Caradonna P, Ghirlanda G (2005) Six-month treatment with alendronate in acute Charcot neuroarthropathy. Diabetes Care 28:1214–1215
Anderson JJ, Woelffer KE, Holtzman JJ, Jacobs AM (2004) Bisphophonates for the treatment of Charcot neuroarthropathy. J Foot Ankle Surg 43:2285–2289
Richard JL, Almasri M, Schuldiner S (2012) Treatment of acute Charcot foot with bisphosphonates: a systematic review of the literature. Diabetologia 55(5):1258–1264
Rubio JA, Aragón-Sánchez J, Jiménez S, Guadalix G, Albarracín A, Salido C, Sanz-Moreno J, Ruiz-Grande F, Gil-Fournier N, Álvarez J (2014) Reducing major lower extremity amputations after the introduction of a multidisciplinary team for the diabetic foot. Int J Low Extrem Wounds 13(1):22–26
Jeffcoate WJ, Game F, Cavanagh PR (2005) The role of proinflammatory cytokines in the cause of neuropathic osteoarthropathy (acute Charcot foot) in diabetes. Lancet 366:2058–2061
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
There was no funding obtained for this study.
Conflict of interest
No author has a conflict of interest to declare.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. The project was reviewed by the institutional audit committee at St. Vincent’s University Hospital and approval was obtained to proceed with data collection.
Rights and permissions
About this article

Cite this article
O’Loughlin, A., Kellegher, E., McCusker, C. et al. Diabetic charcot neuroarthropathy: prevalence, demographics and outcome in a regional referral centre. Ir J Med Sci 186, 151–156 (2017). https://doi.org/10.1007/s11845-016-1508-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-016-1508-5