
Abstract
Background
Stress and burnout are common among doctors. Excess levels of stress have been shown to have detrimental personal and professional effects as well as a negative influence on patient care.
Aim
The aim of our pilot study was to assess the levels of burnout among a cohort of interns.
Methods
A voluntary written self-assessment of burnout levels was distributed to interns in two teaching hospitals. The Maslach Burnout inventory is a 22-question survey assessing the three components of the burnout syndrome—emotional exhaustion (EE), depersonalisation (DP) and personal achievement (PA).
Results
Twenty-seven surveys were distributed to interns in two hospitals with a 96.3 % (n = 26) response rate. The mean age was 25.1 years (range 24–31 years). 14 were medical interns, 12 were surgical interns at the time of completion. Overall, the mean EE score was 23.4 (range 11–29), representing moderate levels of EE. The mean DP score was 9.4 (range 4–14), representing moderate levels of DP. The mean PA score was 18.9 (range 12–29), representing high levels of PA. There were no significant differences noted between levels of EE, DP or PA among male or female interns, medical or surgical interns or those who worked in a peripheral or university hospital.
Conclusion
Burnout is reported among interns in our pilot study. Measures need to be taken to heighten awareness of burnout among doctors and to educate physicians regarding self-awareness and personal health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The stress response represents a bundle of adaptive behavioural, physiological, and cellular responses to a given stimulus [1]. Stress for doctors may arise from conducting complex procedures, mastering new technologies and working under time pressure with ever-decreasing experience [2]—all within an arena typically plagued by distractions and interruptions [3]. A certain degree of stress can facilitate task performance; however, a large body of psychological evidence from highly skilled professionals (e.g. doctors, pilots, military) attests that excessive levels can result in deterioration of abilities [4]. Stress can impair technical skills as well as vigilance, memory, and other cognitive processes in both experimental and naturalistic contexts [5].
Burnout is a professional psychological stress-induced syndrome defined by the three dimensions: emotional exhaustion, depersonalisation and low personal accomplishment [6]. Burnout is prevalent among doctors and certain specialities and certain grades are at higher risk [7]. Burnout has a detrimental effect on the physician’s quality of life and is associated with an increased risk of suicidal ideation [8]. It has also been linked to poorer quality of care, increased medical errors and lawsuits, decreased empathy, job withdrawal and absenteeism [9].
Graduation from medical school marks a sudden transition from a protected world into real life, where stress is inevitable. Without training, this transition too often results in distress and depression for those who first encounter stress in the unfavourable circumstances. Physicians do not sufficiently acknowledge stress in the work place and do not train for it [10]. As a result of a demanding health service, junior doctors are often exposed to clinical situations above their knowledge and experience and often have difficulties dealing with the personal repercussions.
The aim of this pilot study is to objectively assess burnout among a cohort of junior doctors working in the Irish health service and to identify the sources of stress in the workplace.
Methods
A voluntary anonymous questionnaire was distributed among all interns in two hospitals (one university hospital and one peripheral hospital). The survey was limited to interns (year one post-graduation from medical school) for the purpose of this pilot study. Internship is the only year in which all trainees are at the same level of experience. After internship, trainees may have different backgrounds having worked abroad, in research or previously in different fields thus widening their exposure and potentially increasing their ability to deal with hospital-related stresses. All surveys were completed during a 2-week period in the first 6 months of their intern year.
The Maslach Burnout Inventory (MBI) was used to assess burnout. The MBI was the instrument chosen due to its strong psychometric properties and also because it is the most widely used instrument by researchers to evaluate burnout in the literature [11].The Maslach Burnout Inventory (MBI) [12] is a 22-item questionnaire that is considered to be the gold standard measure for burnout. It evaluates the three independent dimensions of burnout: emotional exhaustion (range 0–54), depersonalisation (range 0–30) and personal accomplishment (range 0–48). Low (EE = 0–16, DP = 0–6, PA ≥ 39), average (EE = 17–26, DP = 7–12, PA = 32–38) and high scores (EE ≥ 27, DP ≥ 13, PA = 0–31) for each dimension are based on the low, medium and high centiles of scores from a study of 1,104 US doctors [6]. Respondents were asked if they were currently an intern in medicine or surgery and also to list the top three factors which they felt attributing to their degrees of burnout in the workplace (Fig. 1).

Maslach Burnout Inventory—voluntary written self-assessment of stress and burnout assessing the three main components of the burnout syndrome—emotional exhaustion (EE), depersonalisation (DP) and personal achievement (PA)
Statistical analysis was performed using Graph-Pad Prism with unpaired t tests. A p value ≤ 0.05 was deemed statistically significant.
Results
Twenty-seven surveys were distributed to interns in two hospitals (n = 7 in the peripheral hospital, n = 20 in the university hospital) with a 96.3 % (n = 26) response rate. Of the respondents, 18 were female, 8 were male. The mean age was 25.1 years (range 24–31 years). Four had completed the graduate entry medical degree. Fourteen were medical interns and 12 were surgical interns at the time of completion.
Maslach Burnout Inventory (MBI)
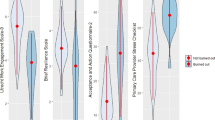
Overall, the mean emotion exhaustion (EE) score was 23.4 (range 11–29), representing a moderate levels of EE. The mean depersonalisation (DP) score was 9.4 (range 4–14), representing a moderate level of DP. The mean personal achievement (PA) score was 18.9 (range 12–29), representing high levels of PA (Figs. 2, 3, 4).

Emotional Exhaustion Subscale (high = 27 or over, moderate 17–26, low 0–16)

Depersonalisation Subscale (high = 13 or over, moderate 7–12, low 0–6)

Personal Achievement Subscale (high 0–31, moderate 32–38, low 39 or over)
Seventy-seven percent (n = 20) reported feeling ‘frustrated by my job’ and that they ‘feel like I am working too hard’ at least once a week or more. Forty-six percent (n = 12) ‘worry that this job is hardening me’ at least a few times a month. Thirty-eight percent (n = 10) reported that they ‘feel very energetic’ more than once a week. Ninety-two percent (n = 24) feel they are ‘positively influencing other people’s lives’.
There were no significant differences noted in mean levels of EE [M = 19.63 (SD) 6.7 vs. M = 22.2 (SD) 5.4, p = 0.31), DP (M = 8.67 (SD) 2.6 vs. M = 10.9 (SD) 2.6, p = 0.06] or PA [M = 19.61 (SD) 4.5 vs. M = 17.25 (SD) 3.4, p = 0.2] between male or female interns.
There were no significant differences noted in mean levels of EE [M = 22.79 (SD) 5.5 vs. M = 19.83 (SD) 6.1, p = 0.21], DP [M = 8.43 (SD) 2.8 vs. M = 10.42 (SD) 2.31, p = 0.06] or PA [M = 19.14 (SD) 4.4 vs. M = 18.58 (SD) 4.3, p = 0.75] between medical or surgical interns.
There were no significant differences in mean levels of EE [M = 20.43 (SD) 6.0 vs. M = 21.79 (SD) 5.9, p = 0.61], DP [M = 9.1 (SD) 3.8 vs. M = 10.21 (SD) 2.2, p = 0.58] or PA [M = 16.86 (SD) 3.9 vs. M = 19.63 (SD) 4.2, p = 0.14] between interns working a university hospital and a peripheral hospital.
Providing in-hospital ‘on-call’ cover was identified to be the most frequent contributor to stress (76.9 %, n = 20). Frequent and recurrent ‘bleeps’ regarding tasks deemed ‘non-urgent’ as well as ‘non-medical administrative work’ also featured frequently (57.7 %, n = 15). Lack of structured ‘breaks’ added to the stress of the day (38.5 %, n = 10). A heavy or excess ‘patient load’ was also an issue for some interns (26.9 %, n = 7).
Discussion
Burnout is evident among the cohort of interns even at an early stage in their career. Despite this and taxing work circumstances, there is a satisfactory level of personal achievement in the cohort which protects against the burnout syndrome. Factors previously associated with burnout in the workplace included insufficient personal or vacation time, feelings of incompetence or inadequacy as a doctor, excessive number of poor outcomes, difficulties with the patient–physician relationship and with issues related to dealing with patients’ families, emotions and particularly emotional dissonance and problems related to the working environment. Non-medical issues, i.e. bed management problems or administrative load affecting clinical workload were also additional sources of frustration [13–15]. Burnout syndrome may often decrease the quality of life both personally and professionally of healthcare professionals leading to anxiety, irritability, mood swings, insomnia, sense of failure, depression, drug addiction and suicide [16, 17]. The syndrome may also be associated with decreased job performance and stress-related health problems [16]. Ultimately, the syndrome can lead to the depersonalization of the provider–patient relationship and the work-life balance. Many international studies assessing burnout have been carried out in oncology settings due to the assumed high levels of stress and emotional exhaustion in this faculty. We have applied the same assessment to interns as it is also assumed that the new work setting is a stressful environment for the recent graduates.
Burnout is defined as a syndrome of depersonalization (DP), emotional exhaustion (EE) and a sense of low personal accomplishment (PA) [6]. The MBI assess all three facets of burnout. Crude scores for EE, DP and PA provided by the MBI are difficult to interpret; therefore, several investigators have adopted the criteria proposed by Grunfeld et al. [19] to diagnose the presence of burnout syndrome. According to these criteria, the burnout syndrome is deemed present if at least one of the dimensions (EE, DP or PA) is severely abnormal [19]. In our study, moderate levels of EE (range 17–26) and DP (range 9–13) are seen, similar to previously published levels. Contrary to this high levels of PA (range ≥ 31) are described, which is protective of the burnout syndrome. It is reassuring to see that despite the challenges faced by interns in our hospital settings, they still achieve a sense of personal accomplishment. Senior doctors have a role to play in encouraging a sense of personal achievement and camaraderie within hospital teams and to have an awareness of stress and burnout among juniors.
In 2010, Siegrist et al. [18] attempted to assess variations in stress levels among healthcare professionals in three different health systems—a largely private insurance-based system (USA), a government-supported, tax-based system (UK) and a mixed system with corporatist and federalist features, administered by social security agencies (Germany). The assessment of a stressful psychosocial work environment was based on the effort–reward imbalance model. The highest level of work stress was reported by physicians in Germany and the lowest level by physicians in the UK, with US physicians reporting intermediate levels. Differences were largely due to the reward component of the model, both financially and work circumstances. This finding was not modified when the impact of physician characteristics (gender, level of clinical experience) and of features of physicians’ work environment were examined (solo versus group practice, staff/physician ratio, time constraints regarding patient appointments, resources available to physicians). Lower levels of administrative and clinical autonomy were associated with higher work stress in all countries, most markedly in the US and the UK system [20]. This study highlights that despite vastly varied health systems and work structures that stress in the healthcare work place is unanimous. A sense of equality on the effort–reward model is paramount to physician satisfaction which in turn affects patient care and physician personal satisfaction.
The interns in this study reported that the causes of their stress included ‘on-call’ requirements, ‘non-urgent’ or ‘non-medical’ tasks, ‘lack of breaks’ and a ‘heavy patient load’. In an attempt to address factors which cause stress to our interns, further analysis is needed to assess why these are stressful and what strategies could be put in place to enhance interns coping skills and to reduce these demands at such an early stage in their careers with limited experience, a lack of leadership or ‘presumed’ lack of support can be an issue. The current health service is under pressure on all fronts with each hospital stretched to their limits. More supervision and defined structure for interns may help ease their passage through an already pressurised first year in the workplace.
To the best of our knowledge, this is the first study and assessment of burnout in junior doctors in an Irish setting. This pilot study needs to be carried out on a broader scale across all grades and specialties to fully ascertain the problem of stress in our young doctors. Managing the risk of burnout is a serious challenge facing physicians today. A culture of self-awareness needs to be fostered and appropriate channels to deal with physician health problems need to be developed, with peer support groups playing an important role in developing coping strategies [20]. It is well established that suicide rates within the medical profession are higher than among the general population [21, 22] and the health service needs to have a heightened awareness of this and be conscious of warning signs or signs of burnout in the doctors.
Limitations
This study was proposed as a pilot study and for this reason was limited to a small sample. Interns were selected as the study group given that it is the only grade that has uniform limited experience. By selecting one grade of junior doctors, this may not be representative of the population of non-consultant hospital doctors as a whole. The fact that the study was carried out in the first 6 months of the intern year may be one reason why high stress levels were identified. As doctors progress in their careers, they may become more accustomed to the busy stressful work environment which is a novel experience to may medical graduates. Interval completion of the same questionnaire and longitudinal analysis may reveal a better picture regarding the development of coping skills and change in burnout levels over the training period. This observation was performed in a subjective manner without objective analysis of factors which may predict burnout; however, we hoped to assess the levels of burnout from the interns’ point of view during this taxing transition from medical school to the busy working environment. Individual personality assessment, past medical history (including evidence of mental illnesses), personal support structures or degree of coping skills were not assessed which play a significant part in individuals’ coping mechanisms. Further studies with larger numbers across all grades are needed to assess stress and burnout among trainees in this country.
Conclusion
Burnout is common among junior doctors in our study. Further studies across all levels of NCHDs are needed to assess stress and burnout levels among doctors working in the Irish health service. Measures need to be taken to heighten the awareness of burnout in our workforce and educate doctors regarding self-awareness and symptoms of burnout.
References
Cuesta JM, Singer M (2012) The stress response and critical illness. A review. Crit Care Med. 40(12):3283–3289
Wetzel CM, Kneebone RL, Woloshynowych M et al (2006) The effects of stress on surgical performance. Am J Surg 191(1):5–10
Sevdalis N, Forrest D, Undre S et al (2008) Annoyances, disruptions, and interruptions in surgery: the Disruptions in Surgery Index (DiSI). World J Surg 32(8):1643–1650
Flin R, O’Connor P, Crichton M (2008) Safety at the sharp end: a guide to non-technical skills. Ashgate, Aldershot
Hassan I, Weyers P, Maschuw K et al (2006) Negative stress coping strategies among novices in surgery correlate with poor virtual laparoscopic performance. Br J Surg 93(12):1554–1559
Maslach C, Jackson SE (1986) The measurement of experienced burnout. J Occup Behav. 2:99–113
Blanchard P, Truchot D, Albiges-Sauvin L et al (2010) Prevalence and causes of burnout amongst oncology residents: a comprehensive nationwide cross-sectional study. Eur J Cancer 46(15):2708–2715
Dyrbye LN, Thomas MR, Massie FS et al (2008) Burnout and suicidal ideation among US medical students. Ann Intern Med 149(5):334–341
Prins JT, Hoekstra-Weebers JE, Van de Wiel HB et al (2007) Burnout among Dutch medical residents. Int J Behav Med. 14:119–125
Dudley HA (1990) Stress in junior doctors. 1 stress and support. BMJ 301(6743):75–76
Cordes CL, Dougherty TW (1993) A review and an integration of research on job burnout. Acad Manag Rev. 18(4):621–656
Maslach C, Schaufeli WB, Leiter MP (2001) Job burnout. Annu Rev Psychol. 52:397–422
Trufelli DC, Bensi CG, Garcia JB et al (2008) Burnout in cancer professionals: a systematic review and meta-analysis. Eur J Cancer Care (Engl) 17:524–531
Lyckholm L (2001) Dealing with stress, burnout, and grief in the practice of oncology. Lancet Oncol. 2:750–755
Mount BM (1986) Dealing with our losses. J Clin Oncol 4:1127–1134
Parker PA, Kulik JA (1995) Burnout self- and supervisor-rated job performance, and absenteeism among nurses. J Behav Med 18(6):581–599
Gundersen L (2001) Physician burnout. Ann Intern Med 135(2):145–148
Siegrist J, Shackelton R, Link C et al (2010) Work stress of primary care physicians in the US, UK and German health care systems. Soc Sci Med 71(2):298–304
Grunfeld E, Whelan TJ, Zitzelsberger L et al (2000) Cancer care workers in Ontario: prevalence of burnout, job stress and job satisfaction. CMAJ 163(2):166–169
Rogers C, Malone KM (2009) Stress in Irish dentists: developing effective coping strategies. J Ir Dent Assoc. 55(6):304–307
Meltzer H, Griffiths C, Brock A et al (2008) Patterns of suicide by occupation in England and Wales: 2001–2005. Br J Psychiatry 193(1):73–76
Agerbo E, Gunnell D, Bonde JP et al (2007) Suicide and occupation: the impact of socio-economic, demographic and psychiatric differences. Psychol Med 37(8):1131–1140
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nason, G.J., Liddy, S., Murphy, T. et al. A cross-sectional observation of burnout in a sample of Irish junior doctors. Ir J Med Sci 182, 595–599 (2013). https://doi.org/10.1007/s11845-013-0933-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-013-0933-y