
Abstract
Background
Loss of body mass during a 24-h run was considered to be a result of dehydration.
Aims
We intended to quantify the decrease in body mass as a loss in fat mass or skeletal muscle mass and to quantify the change in hydration status.
Methods
Body mass, fat mass, skeletal muscle mass, haematocrit, plasma sodium and urinary specific gravity were measured in 15 ultra-marathoners in a 24-h run.
Results
Body mass decreased by 2.2 kg (p = 0.0009) and fat mass decreased by 0.5 kg (p = 0.0084). The decrease in body mass correlated to the decrease in fat mass (r = 0.72, p = 0.0024). Urinary specific gravity increased from 1.012 to 1.022 g/mL (p = 0.0005).
Conclusions
The decrease in body mass and the increase in urinary specific gravity indicate dehydration. The decrease in body mass was correlated to the decrease in fat mass and therefore not only due to dehydration.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
A decrease in body mass is considered to be the result of dehydration in marathoners [1, 2] and ultra-marathoners [3]. In a marathon with an average duration of about 3 h, body mass decreased by 2 kg [2]; in an ultra-marathon such as a 24-h run, body mass decreased by 2 kg [4] up to 2.5 kg [3]. This decrease in body mass is thought to be due to dehydration [1–3]. However, in recent field studies in ultra-endurance races, a decrease in fat mass [5] and skeletal muscle mass [6, 7] has been demonstrated as part of the decrease in body mass.
In a recent study at a 24-h run, the decrease in body mass was explained as a result of dehydration [3]; however, no indices of hydration status were determined. During the past, many indices such as change in body mass, haematological and urinary parameters, bioelectrical impedance analysis and skin-fold thickness have been developed to accurately assess hydration levels in humans [8, 9]. Although there is no ‘gold standard’ [10], it appears that changes in body mass, along with urine osmolality, urinary specific gravity, conductivity and colour of urine are among the most widely used indices [8]. The current evidence and opinions tend to favour urine indices as the most promising marker available [9] since haematological measurements such as plasma sodium or haematocrit are not as sensitive in detecting mild hypo-hydration [9, 11, 12]. Urine colour, urinary specific gravity and urinary osmolality are considered as valid indices of hydration status [12], where urinary specific gravity and urinary osmolality may be used interchangeably to determine hydration status [11]. Following Kavouras [8], an athlete is well hydrated with a urinary specific gravity <1.010 g/mL, minimally dehydrated with a urinary specific gravity between 1.010 and 1.020 g/mL, significantly dehydrated with a urinary specific gravity between 1.020 and 1.030 g/mL and seriously dehydrated with a urinary specific gravity >1.030 g/mL.
In long-distance triathlons and marathons, an association between excessive fluid intake and both body mass and plasma sodium concentration has been demonstrated [13–15]. In the case of fluid overload, body mass increased and plasma sodium concentration decreased [13, 15, 16]. Dehydration generally resulted in a decrease of body mass as has been noted in ultra-marathoners [3]. In cases of excessive fluid intake with fluid overload [17], we would expect a stable or increased body mass [16, 17], a decrease in plasma sodium concentration [16–19], an increase in plasma volume [19] and a decrease in haematocrit due to haemodilution [15].
Risk factors for fluid overload and subsequent exercise-associated hyponatremia are a slow running pace and high frequency of fluid intake [13, 20]. Due to the fact that ultra-runners compete at a rather low speed and may have many aid stations during a race [21, 22], fluid overload might occur, thus leading to an increase in body mass. The aim of this present study was therefore to quantify the decrease in body mass as a loss in fat mass or skeletal muscle mass in male ultra-runners in a 24-h run. In addition, we intended to quantify the change in hydration status using different parameters.
Materials and methods
Subjects
The organiser of the 24-h run in Basel, Switzerland, contacted all participants of the race in 2007 and asked them to participate in the investigation. Twenty-two out of the 86 male starters participated in our investigation. They all gave their informed written consent and the study was approved by the local Institutional Ethics Committee. Fifteen male athletes with (mean and standard deviation) 46.7 years (5.8), 71.1 kg (6.8), 1.76 m (0.07) and a BMI of 23.1 kg/m2 (1.84) out of our study group finished the 24-h run without a break. Seven runners retired because of medical problems (exhaustion, overuse injuries of the lower limbs, heat stroke) and did not complete the full 24 h.
The race
The 19th edition of the 24-h run in Basel took place on 12 and 13 May 2007. Runners from all over Europe started at noon on 12 May, where they had to run as many laps of 1,141.86 m as possible on a flat asphalt course. The weather was fine and dry and the temperature varied between 10°C (night) and 31°C (noon). The athletes could take food and beverages ad libitum from an abundant buffet being provided by the organiser as well as their own food from their support crews. The organiser offered apples, bananas, oranges, dried fruit, potatoes, rice, cookies, bread, various snacks, pasta, porridge, soup, water, tea, isotonic drinks, fruit juices, cola, broth, and coffee. Athletes were mainly eating and drinking ‘on the run’ and recorded their fluid intake during the run.
Measurements and calculations
Immediately before the start of the race and directly after the race, every participant underwent anthropometric measurements and collection of blood and urinary samples in order to determine body mass, skeletal muscle mass, percent body fat, haematocrit, plasma volume, plasma sodium and urinary specific gravity. Body mass was measured using a commercial scale Beurer BF 15 (Beurer GmbH, Ulm, Germany) to the nearest 0.1 kg. Skeletal muscle mass was determined using the anthropometric method according to Lee et al. [23] and body fat percentage following Ball et al. [24]. In these methods, muscle mass and body fat were estimated using skin-fold thicknesses and limb circumferences. Samples of urine were collected for determination of urinary specific gravity using URYXXON® 300 (Macherey–Nagel, GmbH, Düren, Germany). At the same time, capillary blood samples were drawn at the fingertip to determine haematocrit and plasma sodium using i-STAT® 1 System (Abbott Laboratories, Abbott Park, IL, USA). All capillary blood sampling was performed in a standing position. Standardisation of posture prior to blood collection was respected since postural changes can influence blood volume and therefore haemoglobin concentration and haemtocrit [9]. The values of haemoglobin, haematocrit, erythrocytes, leucocytes and platelets increase with the change of the body position from recumbent to sitting and to erect. Haemoglobin and the haematocrit can significantly increase when the subjects assume a more erect position, probably as a result of the increased hydrostatic pressure. Changes in plasma volume were determined from the pre- and post-race haematocrit (H) values according to Beaumont with % Δ plasma volume = [100/(100 − H pre)] × [100(H pre − H post)/H post] [25]. Energy expenditure during the race was estimated using a stepwise calculation using body mass, mean velocity and time spent during performance [26]. As an example, an athlete with 73 kg body mass running at an average speed of 8 km/h for 24 h expended 9.7 (=average energy expenditure in kcal/min for a 73 kg man while running) × 1,440 (=minutes in 24 h) = 13,968 kcal.
Statistical analysis
Results are presented as mean (95% confidence interval). Non-parametric methods were used as not all parameters were ideally normally distributed. The one-sample Wilcoxon signed rank test was used to check for significant changes (∆) in the parameters before and after the race. Spearman correlation analysis was performed to assess univariate association between ∆ in anthropometric variables and ∆ in laboratory data. For all statistical tests, significance was set at a level of 0.05.
Results
Performance and energy expenditure
The runners achieved an average distance of 180.7 km (164.4–196.6), within a range from 136 to 225 km. The athletes were running at an average speed of 7.5 km/h (6.8–8.2) and expended an estimated energy of 13,286 kcal (12,358–14,214) during the 24 h.
Change in body composition
Body mass decreased highly significantly (p = 0.0009) by 2.2 kg (Table 1). In two athletes, body mass increased by 0.1 and 1.1 kg, in the other 13 runners, body mass decreased between 0.1 and 5.1 kg. Fat mass decreased significantly by 0.5 kg (p = 0.0084) whereas skeletal muscle mass showed no changes (p = 0.93). Race performance was not correlated to ∆ body mass (r = −0.11, p = 0.68), ∆ fat mass (r = 0.23, p = 0.41) or ∆ skeletal muscle mass (r = −0.15, p = 0.60). ∆ Body mass was significantly and positively correlated to ∆ fat mass (r = 0.72, p = 0.0024) (Fig. 1). ∆ Fat mass was neither correlated to the estimated energy expenditure (r = 0.06, p = 0.82) nor to the average running speed (r = 0.23, p = 0.41).

The decrease in body mass was significantly and positively related to the decrease in fat mass (r = 0.72, p = 0.0024)
Fluid intake
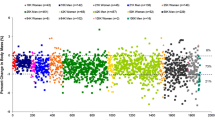
The competitors consumed a total of 15.1 L (12.3–17.9) during the race, equal to 0.62 L/h (0.51–0.75). Fluid intake was significantly and negatively correlated to the average running speed in the race (r = −0.87, p < 0.0001) (Fig. 2). ∆ body mass was not related to the hourly fluid intake (r = 0.03, p = 0.90). Total fluid intake and ∆ plasma sodium were not related (r = −0.03, p = 0.92).

Hourly fluid intake and average running speed during the race were significantly and negatively related (r = −0.87, p < 0.0001)
Change in blood and urinary parameters
Pre- and post-race values of haematocrit (p = 0.37) and plasma sodium (p = 0.27) did not differ significantly whereas urinary specific gravity increased significantly (p = 0.0005) (Table 2). Plasma volume increased by 4.9% (−3.8 to 13.7). ∆ Plasma sodium was not related to the increase in PV (r = −0.18, p = 0.52). Post-race urinary specific gravity was not related to the hourly fluid intake (r = −0.05, p = 0.87) and ∆ body mass was not correlated to ∆ urinary specific gravity (r = −0.21, p = 0.44). Race performance was neither related to post-race urinary specific gravity (r = 0.15, p = 0.59) nor to Δ urinary specific gravity (r = 0.08, p = 0.76).
Discussion
The main finding in this investigation was that these ultra-runners became dehydrated with a decrease in body mass and an increase in urinary specific gravity as expected. However, the decrease in body mass was not only due to dehydration since we found a significant association between the decrease in body mass and the decrease in fat mass. Furthermore, no fluid overload occurred although fluid intake was related to running speed. In the case of an excessive fluid intake with fluid overload [17], we would expect a stable or increased body mass [16, 17], a decrease in plasma sodium concentration [16–19] and the increase in body mass should be positively related to fluid intake. Since body mass decreased, plasma sodium showed no changes and the change in body mass was not related to fluid intake, no fluid overload occurred in these ultra-marathoners.
Change in body mass
Body mass decreased in 13 of the 15 athletes so that a significant decrease in body mass resulted. The loss of 2.2 kg in body mass is comparable with the results of Fellmann et al. [4] demonstrating a decrease of 2.1 kg body mass (1.0) in a 24-h run, corresponding to 3.1% (1.5). In the study of Kao et al. [3], body mass was reduced by 2.48 kg (1.8) corresponding to 5.07% body mass (2.6).
In contrast to recent findings of Kao et al. [3], where ∆ body mass was related to race intensity, race performance was not associated to ∆ body mass in this race. An explanation might be the difference in performance. Our athletes achieved 180.7 km (164.4–196.6) which was less than the result of Kao et al. [3] where the athletes reached 199.4 km (37). A further finding is that the decrease in body mass was not only due to dehydration since we found a significant decrease in fat mass. Whilst Kao et al. [3] postulated that ∆ body mass was a result of dehydration due to speed in the race, we could demonstrate a positive correlation between ∆ body mass and ∆ fat mass and found no association between decrease in body mass and running speed.
Parameters of hydration status
Our runners lost 2.6% in body mass and their post-race urinary specific gravity was 1.022 g/mL. According to Kavouras [8], this was equal to a significant dehydration. The change in urinary specific gravity was statistically significant, however, the magnitude of this change was very small and both pre- and post-measurements fall within the normal range. Race performance was neither related to post-race urinary specific gravity nor to Δ urinary specific gravity. We assume that the change in urinary specific gravity was of no clinical significance regarding the association with physical performance.
Athletes in such a long race run at a rather slow pace and they drink a lot during running and breaks [27] so that a fluid overload might occur [28] with haemodilution and changes in electrolytes [29]. Although fluid intake was dependent upon running speed, no fluid overload with increase in body mass and decrease in plasma sodium occurred. The hourly intake of 0.62 L (0.51–0.75) of fluids was not sufficient to prevent from dehydration; however, no fluid overload resulted with this average hourly amount. In the state of fluid overload we might expect a decrease in plasma sodium which was not found in these athletes.
Limitations of the present study and applications for future investigations
This study is limited to the rather small sample of 15 participants although Kao et al. [3] also had only 19 males in their study. However, a larger sample with athletes running at a higher speed might have more clearly shown the decrease in fat mass depending upon race intensity as has been demonstrated in ultra-triathletes [30]. Although the determination of urinary indices are suggested as reliable parameters of hydration status [8, 9], studies have documented that urinary indices are not accurate measures of ‘real-time’ hydration status and the determination of plasma osmolality would be a better marker of hydration status in the situation of acute dehydration [31, 32]. Furthermore, the determination of sodium content in consumed fluids and food might show a potential association with post-race plasma sodium concentration. Although fluid intake was assessed, the association between fluid intake and ambient temperature might demonstrate that athletes drink more during the heat compared during the cold of the night. In one athlete, the calculated fat mass increased by ~1 kg, in two others by ~0.1 kg. The anthropometric method to determine fat mass is based upon the determination of skin-fold thicknesses. In that subject with the increase in fat mass, the skin-fold thicknesses increased post-race at pectoral, triceps, subscapular, suprailiacal, thigh and calf site. In a recent study where this method was applied, skin-fold thicknesses at pectoral site increased and showed no decrease at the thigh whereas the other skin-fold thicknesses decreased [30]. Presumably the skin-fold thickness was influenced post-race by subcutaneous oedema [33] and thus the immediate measurement post-race of skin-fold thicknesses may be affected by an oedema.
Conclusions
A 24-h run led to a significant decrease in body mass. This decrease in body mass correlated to a significant decrease in fat mass. Urinary specific gravity increased significantly. Although the decrease in body mass and the increase in urinary specific gravity indicated dehydration, the athletes may relatively have been over hydrated as indicated by the nonsignificant decrease in haematocrit and the nonsignificant increase in plasma sodium. A correct determination of the decrease in body mass including reduced fat mass in ultra-runners in a 24-h run can only be obtained after reaching pre-race hydration status, when they are presumably euvolemic, for the post-race measurements.
References
Pastene J, Germain M, Allevard AM, Gharib C, Lacour JR (1996) Water balance during and after marathon running. Eur J Appl Physiol 173:49–55
Whiting PH, Maughan RJ, Miller JD (1984) Dehydration and serum biochemical changes in marathon runners. Eur J Appl Physiol 52:183–187
Kao WF, Shyu CL, Yang XW et al (2008) Athletic performance and serial weight changes during 12- and 24-hour ultra-marathons. Clin J Sport Med 18:155–158
Fellmann N, Bedu M, Giry J et al (1989) Hormonal, fluid, and electrolyte changes during a 72-h recovery from a 24-h endurance run. Int J Sports Med 10:406–412
Knechtle B, Wirth A, Knechtle P, Rosemann T (2009) An ultra-cycling race leads to no decrease in skeletal muscle mass. Int J Sports Med 30:163–167
Knechtle B, Duff B, Amtmann G, Kohler G (2008) An ultra-triathlon leads to a decrease of body fat and skeletal muscle mass—the Triple Iron Triathlon Austria 2006. Res Sports Med 16:97–110
Knechtle B, Kohler G (2007) Running 338 km within 5 days has no effect on body mass and body fat but reduces skeletal muscle mass—the Isarrun 2006. J Sports Sci Med 6:401–407
Kavouras SA (2002) Assessing hydration status. Curr Opin Clin Nutr Metab Care 5:519–524
Shireffs SM (2003) Markers of hydration status. Eur J Clin Nutr 57:S6–S9
Armstrong LE (2007) Assessing hydration status: the elusive gold standard. J Am Coll Nutr 26:575S–584S
Armstrong LE, Maresh CM, Castellani JW et al (1994) Urinary indices of hydration status. Int J Sport Nutr 4:265–279
Armstrong LE, Soto JA, Hacker FT Jr, Casa DJ, Kavouras SA, Maresh CM (1998) Urinary indices during dehydration, exercise, and rehydration. Int J Sport Nutr 8:345–355
Almond CS, Shin AY, Fortescue EB et al (2005) Hyponatremia among runners in the Boston Marathon. N Engl J Med 352:1550–1556
Irving RA, Noakes TD, Buck R et al (1991) Evaluation of renal function and fluid homeostasis during recovery from exercise-induced hyponatremia. J Appl Physiol 70:342–348
Stumpfle KJ, Lehmann DR, Case HS, Hughes SL, Evans D (2003) Change in serum sodium concentration during a cold weather ultradistance race. Clin J Sport Med 13:171–175
Noakes TD, Sharwood K, Speedy D et al (2005) Three independent biological mechanisms cause exercise-associated hyponatremia: evidence from 2,135 weighed competitive athletic performances. Proc Natl Acad Sci USA 102:18550–18555
Speedy DB, Faris JG, Hamlin M, Gallagher PG, Campbell RG (1997) Hyponatremia and weight changes in an ultradistance triathlon. Clin J Sport Med 7:180–184
Hew TD (2005) Women hydrate more than men during a marathon race: hyponatremia in the Houston marathon: a report on 60 cases. Clin J Sport Med 15:148–153
Speedy DB, Noakes TD, Kimber NE et al (2001) Fluid balance during and after an Ironman triathlon. Clin J Sport Med 11:44–50
Chorley J, Cianca J, Divine J (2007) Risk factors for exercise-associated hyponatremia in non-elite marathon runners. Clin J Sport Med 17:471–477
Knechtle B, Duff B, Schulze I, Rosemann T, Senn O (2009) Anthropometry and pre race experience of finishers and non-finishers in a multi-stage ultra-endurance run—Deutschlandlauf 2007. Percept Mot Skills 109:105–118
Knechtle B, Duff B, Schulze I, Kohler G (2008) A multi-stage ultra-endurance run over 1,200 km leads to a continuous accumulation of total body water. J Sport Sci Med 7:357–364
Lee RC, Wang Z, Heo M, Ross R, Janssen I, Heymsfield SB (2000) Total-body skeletal muscle mass: development and cross-validation of anthropometric prediction models. Am J Clin Nutr 72:796–803
Ball SD, Altena TS, Swan PD (2004) Comparison of anthropometry to DXA: a new prediction equation for men. Eur J Clin Nutr 58:1525–1531
van Beaumont W (1972) Evaluation of hemoconcentration from hematocrit measurements. J Appl Physiol 31:712–713
ASCM (1995) Guidelines for exercise testing and prescription, 3rd edn. Williams and Wilkins, Philadelphia, PA, pp 277
Noakes T (2002) Hyponatremia in distance runners: fluid and sodium balance during exercise. Curr Sports Med Rep 1:197–207
Noakes TD, Sharwood K, Collins M, Perkins DR (2004) The dipsomania of great distance: water intoxication in an Ironman triathlete. Br J Sports Med 38:E16
Kaminsky LA, Paul GL (1991) Fluid intake during an ultramarathon running race: relationship to plasma volume and serum sodium and potassium. J Sports Med Phys Fitness 31:417–419
Knechtle B, Schwanke M, Knechtle P, Kohler G (2008) Decrease in body fat during an ultra-endurance triathlon is associated with race intensity. Br J Sports Med 42:609–613
Kovacs EM, Senden JM, Brouns F (1999) Urine color, osmolality and specific electrical conductance are not accurate measures of hydration status during postexercise rehydration. J Sports Med Phys Fitness 39:47–53
Popowski LA, Oppliger RA, Patrick Lambert G, Johnson RF, Kim Johnson A, Gisolf CV (2001) Blood and urinary measures of hydration status during progressive acute dehydration. Med Sci Sports Exerc 33:747–753
Knechtle B, Wirth A, Knechtle P, Rosemann T (2009) Increase of total body water with decrease of body mass while running 100 km nonstop—formation of edema? Res Q Exerc Sport 80:593–603
Acknowledgments
We thank the crew of ‘Sri Chinmoy Marathon Team Switzerland’ for their generous support and the athletes for their promptitude to collect data during the race. For their help in translation, we thank Matthias Knechtle, Lausanne, Switzerland, and Mary Miller from Stockton-on-Tees, Cleveland in England, crew member of an ultra-endurance support crew.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Knechtle, B., Wirth, A., Knechtle, P. et al. Do ultra-runners in a 24-h run really dehydrate?. Ir J Med Sci 180, 129–134 (2011). https://doi.org/10.1007/s11845-010-0500-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-010-0500-8