
Abstract
Purpose
The benefits of physical activity for cancer survivors are increasingly recognised and smartphone applications are available to assist them to become more physically active. Cancer clinicians, however, lack confidence about which physical activity apps to recommend as evidence on their quality and content is limited. Therefore, we reviewed freely available commercial physical activity/fitness apps to systematically assess their behavioural change content and quality of their design.
Methods
Systematic searches of the app stores for Apple and Android operating systems were conducted and apps were screened to identify free apps appropriate for cancer survivors. Quality was assessed using the Mobile App Rating Scale (MARS) and behavioural content was evaluated using the Behavioural Change Techniques Taxonomy (BCTT).
Results
Of 341 apps identified, 67 were judged appropriate for cancer survivors and 46% combined aerobic and strength/stretching content. The overall number of behavioural change techniques (BCT) included was 3.96 (SD = 2.09), with the most frequent being ‘feedback on behaviour’ and ‘goal setting behaviour’. The mean scores for objective and subjective quality were 4.11 (SD = 0.59) and 3.07 (SD = 0.91) respectively (range 0 to 5). Finally, a modest positive correlation was found between the number of BCT and the quality of engagement, awareness and knowledge as assessed by the MARS.
Conclusion
Only a fifth of retrieved physical activity apps contained potentially suitable content for people affected by cancer. Overall, most apps we reviewed appeared to perform well in terms of their objective quality, but less well at promoting knowledge and awareness or help seeking related to physical activity.
Implications for Cancer Survivors
Many physical activity apps are available but the combined use of MARS and BCTT suggests that not all of them are suitable to the needs is a promising and feasible approach for assessing the applicability, usability and content of physical activity of apps employed by cancer survivors and this study is a first step toward developing a guide.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Most cancer survivors are not physically active, with fewer than 25% meeting physical activity guidelines (150 mins of moderate intensity activity a week) [1]. Participation in exercise or physical activity declines considerably during cancer treatment and tends to remain low afterwards [2]. This is concerning because there is considerable evidence that sustaining or increasing physical activity after a cancer diagnosis can have a beneficial impact on the quality of life, ongoing symptoms, physical functioning and fatigue [3]. Cancer survivors are also at increased risk of developing new conditions (osteoporosis, diabetes, cardiovascular problems) [4] for which exercise may offer a protective effect. Furthermore, the evidence is accruing indicating physical activity reduces the risk of cancer recurrence and improves survival [5, 6].
In light of this evidence, most clinical guidelines for follow-up and survivorship care highlight the importance of promoting physical activity and exercise with cancer survivors [7, 8], but offer few recommendations about how this can be achieved in practice. The wider evidence on physical activity suggests successful and sustainable interventions are underpinned by behavioural change theory (BCT) [9], include aspects of goal setting, prompts, self-monitoring and encouragement of independent exercise [10, 11]. However, whilst interventions are effective at increasing physical activity in the short term, many studies have a limited follow-up period or involve supervised activity and/or require attendance at specialist gyms, potentially limiting acceptability and longer-term economic sustainability [12, 13].
The use of smartphone apps has become part of everyday life for many people. In developed economies, > 80% of the adult population own smartphones [14]. A key part of the app market is Health and Fitness with > 165,000 such apps on the two major operating systems (OS): App store for iOS and Google Play for Android. There are many potential advantages to using Smartphone apps to promote physical activity. For example, they are accessible, often customizable to the needs of the users and can often provide scheduled prompts [15]; all of which have been shown to be important in achieving physical activity goals, and thereby provide a form of ‘virtual’ exercise supervision [10]. However, most ‘off-the-shelf’, commercially available apps on the market do not formally draw on behavioural change theories in promoting physical activity and lack evidence of efficacy through randomised controlled trials [16]. The limited published research on the content of physical activity promoting apps suggests there is considerable variability across apps in the types of behavioural change techniques (BCT) employed [17]. A content review of apps to promote physical activity in healthy adults found that on average apps included only five behavioural change techniques (range 2–8), out of a possible 23 [18] with comparable content across free and paid for apps and the two main OS.
Whilst many cancer patients will not have access to an exercise rehabilitation programme or be able to afford a gym membership, physical activity apps appear acceptable to cancer patients [19, 20]. Moreover, there is anecdotal evidence that, like the general population, cancer patients are increasingly using smartphone apps to try and increase their physical activity [21].
This presents a conundrum for the cancer health professional when patients ask for their recommendations with regard to using such apps. The absence of randomised controlled trials, the fast moving pace of the technology and apparent variability in the behavioural change content all presents a challenge for cancer professionals wanting to make recommendations based on best available evidence, as they would in their clinical practice [16]. Other key aspects of physical activity app development, such as reviews of quality, aesthetics and features have received limited attention but are an important consideration if an individual continues to engage with an app and sustain levels of physical activity [22].
This study aimed to review freely available commercial ‘off-the-shelf’ fitness apps available on the two largest OS and to systematically assess the content and quality of selected physical activity apps and examine the relationship between app quality, number of app features and BCT. We will use this information to inform the development of an internet-based machine learning algorithm using text analytics and qualitative user testing studies by cancer survivors and cancer clinicians. The aim to help cancer health professionals personalises advice on the suitability of commercial fitness apps for people living with and beyond cancer.
Methods
Search strategy
Our methods sought to replicate the way a patient might access a fitness (exercise and physical activity) app. Searches were conducted in the Health and Fitness category of iOS App Store (Apple) and Google Play (Android) in the UK. We followed the same principles in both OS to make it as systematic as possible, between January and February 2017 using an Apple iPad mini 3 and Samsung Galaxy S6.
Free apps available in iOS, Google Play or both stores were included in this review. Initial screening was based on an apps’ marketing material and, where this was unclear, apps were downloaded for further evaluation. Two researchers (RMP, JH) independently used and extracted data on the app content. Apps were downloaded to Apple, Android or both devices (where available). Inclusion criteria were apps that (i) targeted adults; (ii) focused on physical activity, exercise or sedentary behaviour; (iii) were free to download and use and (iv) were available in English. Apps were excluded if they focused (i) on one body part, (ii) on diet/food intake (with no exercise component), (iii) were not physical activity-based (e.g. hypnosis, meditation); (iv) required a wearable device to be used and (v) were inappropriate for cancer survivors for the following reasons: (a) included exercises unsuitable for cancer patients to undertake independently (e.g. heavy weight lifting which may be contraindicated if bone metastases are present and require careful professional supervision) and (b) included negative content (e.g. excessively underweight or sexualised body images/text, unsubstantiated claims about effectiveness/ability of app to increase longevity).
Data extraction
Both researchers (RMP, JH) independently screened retrieved apps based on marketing material and extracted data onto a study-specific coding form and checked for duplicate listings of the same app (i.e. the same app could have different names in iOS or Play store). Data extracted included app name, OS, content description and reason for exclusion, if appropriate. After screening, apps were downloaded and used by the researchers, with reasons for exclusion after download being noted. Included apps were installed on the device for 7 days and the type of physical activity [23], quality assessment [24] and behavioural change content [25] was assessed. Data was extracted using a study-specific proforma. Throughout this process, any disagreements regarding inclusion or content evaluation were resolved by discussion and/or consultation with a third reviewer (JA).
App quality assessment
The objective and subjective quality of each app were assessed by consensus between two researchers (JH & RMP), using the Mobile App Rating Scale (MARS) developed by Stoyanov et al. [24]. MARS includes 19 objective items covering four domains: engagement, functionality, aesthetics and information. Finally, six app-specific content classification items, from the MARS instrument designed for application to a health context, were included (awareness, knowledge, attitudes, increase intention, help seeking and behaviour change). All items are rated on a 5-point scale (1, inadequate; 2, poor; 3, acceptable; 4, good; 5, excellent) with possible total scores being 0–5 for objective and subjective items. Mean scores were calculated for each domain (engagement, functionality, aesthetics and information) and overall app quality was calculated by averaging the aggregated mean for all domains.
Behavioural change content assessment
The behavioural change techniques utilised in each app were assessed using the Behavioural Change Techniques (BCT) Taxonomy, version 1, originally developed by Michie et al. [25], which has been shown to be a comprehensive, valid and reliable approach for assessing techniques for changing behaviour in general [26] as well as health apps [17, 18] promoting physical activity [27, 28]. Scheoppe et al. [22] have applied a dichotomous scoring system to BCT to indicate the absence (0) or presence (1) of each technique, permitting a total BCT score per app (possible score 0–93) to be generated.
Statistical analysis
Total scores for each app on each domain of the MARS and the BCT Taxonomy were calculated. Descriptive statistics are presented by OS, whilst ANOVA was used to test for differences in MARS domains scores between operating systems (Android, iOS or both). To determine if there was any relationship between app quality and BCT content (Bardus et al., 2016), Spearman’s rank correlation was used to determine any associations between MARS total scores and the number of BCT’s. All statistical analyses were conducted using IBM SPSS version 25.0 with significance levels set at p < 0.05.
Results
App selection and description
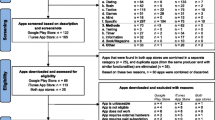
A total of 341 apps were identified. Of these, 112 were downloaded, used and assessed for eligibility resulting in 67 apps being included (Fig. 1). Notable reasons for exclusion after download included those requiring wearables to be used (n = 5), those with inappropriate content for people with cancer (due to negative body images/unfounded claims of effectiveness, n = 4) and apps that appeared to be free to use from the marketing material but on download were not (n = 3). Over half the apps were available on both operating systems (n = 37) (Table 1). Many apps included a combination of aerobic/strength or stretching (46%, n = 34), or solely aerobic content (39%, n = 26). A fifth of eligible fitness apps also included a diet/calorie intake component (18%, n = 12).

Flowchart of app search process
App quality
The MARS objective and subjective quality scores were 4.11 (SD = 0.59) and 3.07 (SD = 0.91), respectively (Table 1). Subjective quality and three of the four objective qualities were significantly higher for fitness apps available via iOS (Table 2, Online Supplementary Table 1). The MARS study-specific content classification varied by the operating system, suggesting a trend for those available on iOS to target attitudes and help seeking, compared to those on Android (Table 2, Online Supplementary Table 1).
Behaviour change techniques
Overall, the mean number of BCT present was 3.96 (SD = 2.09). Figure 2 shows the BCT most commonly included in the apps; of the 93 BCT, nine were used in at least fifth of fitness apps. Two BCTs were evident in more than half of all apps: ‘feedback on behaviour’ and ‘goal-setting behaviour’. There were no significant differences between the numbers of BCT present on either operating systems (data not presented but available on request).

Percentage of BCT in included apps
The percentage of BCT used in combination ranged from 1.5 to 49.3% (Table 3). ‘Goal-setting behaviour’ was frequently used in combination with ‘feedback on behaviour’ (49.3%), and similarly ‘goal-setting outcomes’ was often used in combination with ‘feedback on behaviour’ (35.8%). Other combinations of BCT present in > 20% of apps are shown in Table 3.
App quality and BCT
There was a moderate positive association between the number of BCTs and the quality of engagement, awareness and knowledge from the MARS domains (Table 4). Correlation coefficients for the number of BCT and MARS domains of information, subjective quality and increase attention indicate a weak association (Table 4).
Discussion
Whilst many hundreds of exercise and fitness apps are commercially available, of those retrieved in this study, only a fifth contained potentially suitable content for people affected by cancer. Most focused on aerobic-based activities and they tended to include goal setting, monitoring and feedback. This may be reassuring for health professionals as there is good evidence that goal setting and self-monitoring are important for successfully changing health-related behaviours, at least in the short term [29]. Similar to previous research, our study found that overall, only a limited number of BCT are currently utilised in commercially available apps, although with an average number of 3.9, this was similar [30] or greater than that found in earlier reviews [18], perhaps suggesting that app developers are incorporating a more diverse range of BCT. There is some evidence that for sustained changes, other person-centred BCT (motivational, autonomy) become more important for maintaining lifestyle improvements [29], and presently these approaches seem relatively underutilised.
We are not aware of any other studies that have applied the MARS within healthcare, and this tool provided important insights into app usability, an often-overlooked aspect in the health context but a vital component for sustained engagement. Overall, most apps appeared to perform well in terms of their objective quality (engagement, functionality, aesthetics and information), but less well at promoting knowledge and awareness or help seeking related to physical activity.
We found some tentative evidence that apps available on Android only perform less well in terms of content and quality but this requires further assessment. Of course, people affected by cancer could just look at product reviews to determine which app is best to use. Whilst reviews certainly provide useful information, we think that for apps to be recommended by health professional more robust criteria are required, particularly when marketing algorithms, can be manipulated and market research suggests that more than half of reviews on OS for apps are fake [31].
Some limitations of this study should be noted. Our search was restricted to free apps; this was deliberate because we did not want to include those that would incur a cost to people affected by cancer when evidence of effectiveness is so limited. However, we recognise that usage is rarely truly ‘free’ and payment is via data access; in reality, some patients may prefer to pay, and indeed payment may incentivise commitment to a programme. Our findings are limited because we assessed the content of BCT and not if the behaviour was changed or the apps’ effectiveness. However, we think it is likely that health professionals would feel more confident in recommending apps with the sound theoretical basis and established quality.
Our review was selective (identifying popular apps) and different time/strategy may have yielded different results. However, we believe this was a strength because our goal was realism and we were trying to replicate authentically how most users search for and find fitness apps most popular on operating systems. A strength of this study is that we searched across both main operating systems; apps were independently evaluated and rated by trained researchers.
Strategies for health professionals wanting to prescribe apps to patients have been outlined [21] including standardising their identification, evaluation and selection to maximise their utility, safety and impact. Although we agree this may be best practice, in reality, this may not be practical for most busy healthcare providers, whatever their professional background. This may be made easier if an online/automated system could recommend potential apps tailored to the needs of individual survivors. This study has provided useful contextual information for the development of an automated internet-based machine learning algorithm using text analytics to search databases and make recommendations suited to the needs and preferences of people affected by cancer and is a useful preliminary step ahead of testing apps with people affected by cancer.
References
National Health Service. Physical activity guideline for adults. United Kingdom: National Health Service; 2015. Available at https://www.nhs.uk/live-well/exercise/. Accessed 12 Dec 2018.
Javaheri PA, Nekolaichuk C, Haennel R, Parliament MB, McNeely ML. Feasibility of a pedometer-based walking program for survivors of breast and head and neck cancer undergoing radiation therapy. Physiother Can. 2015;67(2):205–13. https://doi.org/10.3138/ptc.2014-24O.
Courneya KS, Friedenreich CM. Physical activity and cancer: an introduction. Recent Results Cancer Res. 2011;186:1–10. https://doi.org/10.1007/978-3-642-04231-7_1.
Khan NF, Mant D, Carpenter L, Forman D, Rose PW. Long-term health outcomes in a British cohort of breast, colorectal and prostate cancer survivors: a database study. Br J Cancer. 2011;105(S1):S29–37. https://doi.org/10.1038/bjc.2011.420.
Van Blarigan EL, Meyerhardt JA. Role of physical activity and diet after colorectal cancer diagnosis. J Clin Oncol. 2015;33(16):1825–34. https://doi.org/10.1200/JCO.2014.59.7799.
Van Zutphen M, Winkels RM, van Duijnhoven FJ, van Harten-Gerritsen SA, Kok DE, van Duijvendijk P, et al. An increase in physical activity after colorectal cancer surgery is associated with improved recovery of physical functioning: a prospective cohort study. BMC Cancer. 2017;17(1):74. https://doi.org/10.1186/s12885-017-3066-2.
Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, Schwartz AL, et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin. 2012;62(4):243–74. https://doi.org/10.3322/caac.21142.
Jorgensen ML, Young JM, Solomon MJ. Optimal delivery of colorectal cancer follow-up care: improving patient outcomes. Patient Relat Outcome Meas. 2015;6:127–38. https://doi.org/10.2147/PROM.S49589.
Husebø AM, Dyrstad SM, Søreide JA, Bru E. Predicting exercise adherence in cancer patients and survivors: a systematic review and meta-analysis of motivational and behavioural factors. J Clin Nurs. 2013;22(1–2):4–21. https://doi.org/10.1111/j.1365-2702.2012.04322.x.
Turner RR, Steed L, Quirk H, Greasley RU, Saxton JM, Taylor SJ, et al. Interventions for promoting habitual exercise in people living with and beyond cancer. Cochrane Database Syst Rev. 2018;(9):CD010192. https://doi.org/10.1002/14651858.CD010192.pub3.
Bourke L, Homer KE, Thaha MA, Steed L, Rosario DJ, Robb KA, et al. Interventions to improve exercise behaviour in sedentary people living with and beyond cancer: a systematic review. Br J Cancer. 2014;110(4):831–41. https://doi.org/10.1038/bjc.2013.750.
Lowe SS, Watanabe SM, Baracos VE, Courneya KS. Physical activity interests and preferences in palliative cancer patients. Support Care Cancer. 2010;18(11):1469–75. https://doi.org/10.1007/s00520-009-0770-8.
Tsianakas V, Harris J, Ream E, Van Hemelrijck M, Purushotham A, Mucci L, et al. CanWalk: a feasibility study with embedded randomised controlled trial pilot of a walking intervention for people with recurrent or metastatic cancer. BMJ Open. 2017;7(2):e013719. https://doi.org/10.1136/bmjopen-2016-013719.
Deloitte. Global mobile consumer trends: second edition. London: Deloitte Touche Tohmatsu Limited; 2017. Available at https://www2.deloitte.com/global/en/pages/technology-media-and-telecommunications/articles/gx-global-mobile-consumer-trends.html. Accessed December 12, 2018
Turner-McGrievy GM, Hales SB, Schoffman DE, Valafar H, Brazendale K, Weaver RG, et al. Choosing between responsive-design websites versus mobile apps for your mobile behavioral intervention: presenting four case studies. Transl Behav Med. 2017;7(2):224–32. https://doi.org/10.1007/s13142-016-0448-y.
Harris J, Cheevers K, Armes J. The emerging role of digital health in monitoring and supporting people living with cancer and the consequences of its treatments. Curr Opin Support Palliat Care. 2018;12(3):268–75. https://doi.org/10.1097/SPC.0000000000000362.
Yang CH, Maher JP, Conroy DE. Implementation of behavior change techniques in mobile applications for physical activity. Am J Prev Med. 2015;48(4):452–5. https://doi.org/10.1016/j.amepre.2014.10.010.
Middelweerd A, Mollee JS, van der Wal CN, Brug J, Te Velde SJ. Apps to promote physical activity among adults: a review and content analysis. Int J Behav Nutr Phys Act. 2014;11(1):97. https://doi.org/10.1186/s12966-014-0097-9.
Short CE, Finlay A, Sanders I, Maher C. Development and pilot evaluation of a clinic-based mHealth app referral service to support adult cancer survivors increase their participation in physical activity using publicly available mobile apps. BMC Health Serv Res. 2018;18(1):27. https://doi.org/10.1186/s12913-017-2818-7.
IJsbrandy C, Ottevanger PB, Tsekou Diogeni M, Gerritsen WR, van Harten WH, Hermens RPMG. Review: effectiveness of implementation strategies to increase physical activity uptake during and after cancer treatment. Crit Rev Oncol Hematol. 2018;122:157–63. https://doi.org/10.1016/j.critrevonc.2017.09.005.
Boudreaux ED, Waring ME, Hayes RB, Sadasivam RS, Mullen S, Pagoto S. Evaluating and selecting mobile health apps: strategies for healthcare providers and healthcare organizations. Transl Behav Med. 2014;4(4):363–71. https://doi.org/10.1007/s13142-014-0293-9.
Schoeppe S, Alley S, Rebar AL, Hayman M, Bray NA, Van Lippevelde W, et al. Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: a review of quality, features and behaviour change techniques. Int J Behav Nutr Phys Act. 2017;14(1):83. https://doi.org/10.1186/s12966-017-0538-3.
Health Improvement Directorate. General practise physical activity questionnaire. London: National Health Service; 2009. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/192453/GPPAQ_-_guidance.pdf. Accessed 12 Dec 2018
Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth. 2015;3(1):e27. https://doi.org/10.2196/mhealth.3422.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. https://doi.org/10.1007/s12160-013-9486-6.
Michie S, Wood CE, Johnston M, Abraham C, Francis JJ, Hardeman W. Behaviour change techniques: the development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol Assess. 2015;19(99):1–188. https://doi.org/10.3310/hta19990.
Nyman SR, Adamczewska N, Howlett N. Systematic review of behaviour change techniques to promote participation in physical activity among people with dementia. Br J Health Psychol. 2018;23(1):148–70. https://doi.org/10.1111/bjhp.12279.
Pears S, Morton K, Bijker M, Sutton S, Hardeman W, Programme Team VBI. Development and feasibility study of very brief interventions for physical activity in primary care. BMC Public Health. 2015;15:333. https://doi.org/10.1186/s12889-015-1703-8.
Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42. https://doi.org/10.1186/s12966-017-0494-y.
Roberts AL, Fisher A, Smith L, Heinrich M, Potts HWW. Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv. 2017;11(6):704–19. https://doi.org/10.1007/s11764-017-0632-1.
Siegel E. Fake reviews in Google Play and Apple App Store. Washington: Apptentive; 2014. https://www.apptentive.com/blog/2014/05/27/fake-reviews-google-play-apple-app-store/. Accessed 12 Dec 2018
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The procedures performed in this study do not require ethical approval.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Martín Payo, R., Harris, J. & Armes, J. Prescribing fitness apps for people with cancer: a preliminary assessment of content and quality of commercially available apps. J Cancer Surviv 13, 397–405 (2019). https://doi.org/10.1007/s11764-019-00760-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-019-00760-2