
Abstract
We describe a robotic repair of a large Morgagni congenital diaphragmatic hernia in a 12-month-old infant using the da Vinci surgical robot.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Robotic surgery is new technology which has been shown to be very promising for a number of applications in adults. The variety of uses in adults and children is expanding rapidly as more systems are being used around the world. Morgagni congenital diaphragmatic hernia (M-CDH) defects have been closed robotically using the da Vinci surgical robot (Intuitive Surgical, Sunnyvale, CA, USA) in a few case reports, but exclusively in the adult population.
Case report
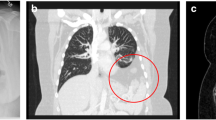
A 12-month-old 10.2 kg girl with a long history of non-specific mild irritability was referred by her local physician with suspicion of reflux. The parents had notice an occasional foul smelling burping but no other significant symptoms. She had no prior history of emesis, constipation, feeding intolerance, or any pulmonary symptoms. A chest X-ray revealed an air-fluid level in the mediastinum and a GI contrast study confirmed the presence of a Morgagni diaphragmatic defect (Fig. 1). She was taken to the operating room electively for repair.

Contrast study demonstrating a Morgagni CDH, lateral view
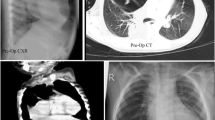
The three-arm version of the standard da Vinci surgical robot was used for the procedure. Three robotic ports were used including one 5-mm camera port at the umbilicus and two 5-mm robotic instrument ports. The 5 mm robotic camera was a standard two-dimensional (2D) robotic camera made specifically for use with the da Vinci. The camera was set in a 30° upward-looking position. Upon entering the abdomen the viscera had already spontaneously reduced from the defect. A hernia sac was present. Instead of excising the sac, we elected to incorporate the hernia sac into the repair by imbricating the sac into the suture closure. The defect was closed with interrupted 2–0 non-absorbable suture in an interrupted horizontal mattress fashion (Fig. 2). Surgeon console time was 91 min and the entire procedure was completed in 119 min. No intraoperative or postoperative complications occurred. The patient was started on a diet on the evening of surgery and discharged home on post-op day #1. There has been no evidence of recurrence in follow-up at nine months.

Intraoperative photograph showing closure of the defect
Discussion
The M-CDH is a rare anterior defect that accounts for less than 5% of all congenital diaphragmatic hernias [1]. Although this defect is occasionally found in infancy, it is usually discovered later in life. Some patients present with a vague epigastric complaint and a chest X-ray or abdominal film demonstrate the defect. Occasionally, these defects are found incidentally while investigating some unrelated issue. Closure is recommended because of the potential risk of incarceration or obstruction. In the open technique the defect is usually closed utilizing an upper midline abdominal incision. Recently, a few case reports have been published utilizing laparoscopy for both adults and children (Table 1).
The first reported case of a laparoscopic closure of an M-CDH in a child was published in 2000 [8]. Since then, a handful of individual cases and a few small laparoscopic series have been reported (Table 1). However, only one robotic repair of an M-CDH in a child has been reported [9], and that patient had their M-CDH closed using the Zeus robotic system. The Zeus was a robotic platform that was manufactured by Computer Motion until 2004. In the summer of 2004, Intuitive Surgical purchased Computer Motion and the Zeus system was no longer manufactured and soon disappeared from clinical use. No parts or service have been available since the merger and the Zeus seems to have been relegated to laboratory use in the few centers that still have them. Meanwhile, the da Vinci has been used to close M-CDH defects in adults. Recently, we reported the first robotic foramen of Bochdalek CDH (B-CDH) closure in a 2.2 kg newborn [10]. But no reports have been published regarding M-CDH closure using the da Vinci in children.
The advantages of the da Vinci robot over standard laparoscopic instruments include more degrees of freedom, tremor filtration, improved optics with the option of either 3D or 2D viewing, and absence of the fulcrum effect. The fulcrum effect is caused by the pivoting of a laparoscopic instrument as it passes through a trocar. For example, in order for the surgeon to move the laparoscopic instrument upward and to the left, the surgeon needs to move the instrument downward and to the right. This opposite movement phenomenon is completely absent in robotic surgery as the finger, hand, and wrist movements at the console are translated to the instruments directly. Furthermore, the robotic instrument articulations can bend a full 90° in all directions. Standard laparoscopic instruments do not have this capability. Neither does the human hand on wrist extension or varus/valgus movements. Additionally, fine motor filtering in the robotic software eliminates hand tremor from the console. Finally, the optical advantage of the da Vinci robot over standard laparoscopy is impressive with the 3D reconstruction.
Limitations of the robot include the size of the 3D camera, among several other issues. The diameter of the current da Vinci 3-D camera is 12 mm and the advantage of the optics has to be considered with the disadvantage of the large camera diameter. Fortunately, a smaller camera with a diameter of only 5 mm is also available for the da Vinci. But this camera provides only a 2D image. A new 3D camera with a diameter of 8.5 mm is in development and is likely to be commercially available by the time this paper is published. However, for now, we generally prefer the 5 mm camera in children less than 10 kg.
This case report demonstrates that robotic surgery is safe and effective for closing an M-CDH, even in small children. Discussion and publication of case reports like this one and preliminary series as they become available will help us assess this technology for use in children. A concerted effort by pediatric surgeons in reporting robotic procedures will help demonstrate the useful applications of robotic surgery as well as limitations.
References
Sahnoun L, Ksia A, Jouini R, et al. (2006) Morgagni hernia in infancy: report of 7 cases. Arch Pediatr 13(10):1316–1319 (epub Aug 17, 2006)
Newman-Heiman N, Kleiner O, Finaly R et al (2007) Minimally invasive surgery approach for diaphragmatic Morgagni hernia in children. Harefuah 146(4):260–261, 319
Holcomb GW 3rd, Ostlie DJ, Miller KA (2005) Laparoscopic patch repair of diaphragmatic hernias with Surgisis. J Pediatr Surg 40(8):E1–E5
Azzie G, Maoate K, Beasley S et al (2003) A simple technique of laparoscopic full-thickness anterior abdominal wall repair of retrosternal (Morgagni) hernias. J Pediatr Surg 38(5):768–770
Ozmen V, Gun F, Polat C et al (2003) Laparoscopic repair of a morgagni hernia in a child: a case report. Surg Laparosc Endosc Percutan Tech 13(2):115–117
de Vogelaere K, de Backer A, Delvaux G (2002) Laparoscopic repair of diaphragmatic Morgagni hernia. J Laparoendosc Adv Surg Tech 12(6):457–460
Ponsky TA, Lukish JR, Nobuhara K et al (2002) Laparoscopy is useful in the diagnosis and management of foramen of Morgagni hernia in children. Surg Laparosc Endosc Percutan Tech 12(5):375–3757
Lima M, Domini M, Libri M et al (2000) Laparoscopic repair of Morgagni–Larrey hernia in a child. J Pediatr Surg 35(8):1266–1268
Knight CG, Gidell KM, Lanning D et al (2005) Laparoscopic Morgagni hernia repair in children using robotic instruments. J Laparoendosc Adv Surg Tech A 15(5):482–486
Meehan JJ, Sandler A (2007) Robotic repair of a Bochdalek congenital diaphragmatic hernia in a small neonate: robotic advantages and limitations. J Pediatr Surg 42(10):1757–1760
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Meehan, J.J., Torres, J.E. Robotic repair of Morgagni congenital diaphragmatic hernia in an infant. J Robotic Surg 2, 97–99 (2008). https://doi.org/10.1007/s11701-008-0081-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-008-0081-y