
Abstract
Background
Percentage of excess weight loss (%EWL) is the most common metric used after bariatric surgery. However, there has been consistent argument against its use since it varies significantly by initial body mass index (BMI). This study aimed to validate the newly suggested percentage of alterable weight loss (%AWL) metric in Korean patients.
Methods
A retrospective review of the prospectively established database at Soonchunhyang University Seoul Hospital identified 165 patients who underwent primary laparoscopic Roux-en-Y gastric bypass (RYGB) and had at least 2-year follow-up weight loss results after surgery. Patients were classified into subgroups based on initial BMI, and their weight loss results expressed as BMI, %EWL, %AWL, and percentage of total weight loss (%TWL) were compared in terms of nadir weight and weight loss trajectory.
Results
The study cohort included 27 male (16.4%) and 138 female (83.6%) patients with a mean baseline BMI of 38.1 ± 5.4. Nadir weight was achieved at mean 24.1 ± 10.6 months postoperatively. Female patients required significantly longer to achieve nadir weight than male patients (16.2 vs. 22.4 months, p = 0.001), and they achieved less weight loss expressed as nadir BMI, %EWL, and %AWL. Of these metrics, only %AWL was not significantly influenced by preoperative BMI and showed the least variation (25.2%) for reporting weight loss.
Conclusion
The AWL metric can report weight loss regardless of baseline BMI in Korean patients undergoing RYGB; however, it must be validated in a larger population involving multiple centers from the Asia-Pacific area before being used clinically.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Weight loss is one of the important outcomes of bariatric surgery. The primary endpoint of bariatric surgery is clinically significant and sustained weight loss, which is considered a measure of efficacy following different surgical procedures and the postoperative determinant of success or failure. Therefore, it is paramount to establish a standardized metric to report weight loss to facilitate easy communication between different expert practitioners as well as provide an appropriate method of comparing various weight control options.
Percent excess weight loss (%EWL) has long been used as a comparative metric to evaluate weight loss outcomes following bariatric surgery [1, 2]. This measure represents the proportion of lost weight to the total amount of excess weight over the ideal weight; the ideal weight corresponds to the body mass index (BMI) of 25 kg/m2 since Deitel et al. redefined this metric in 2007 [3]. However, there has been a consistent argument against the use of %EWL since it shows significant variation by the baseline BMI of the patients and is rarely used in non-surgical studies [1, 4,5,6,7,8]. Percentage of total weight loss (%TWL) is the most commonly adopted method of weight loss reported in the field of medical treatment for obesity. Surgeons have recently advocated using %TWL after bariatric surgery because it is less associated with preoperative BMI and more intuitive than %EWL [8, 9]. It was recently adopted as a mandatory measure for reporting weight loss outcomes by leading bariatric scientific societies [10]. Still, %TWL is influenced by initial BMI as well, although to a lesser extent, and it might not be sufficient to represent the significance of reduced disease burden corresponding to the weight loss after treatment because this metric includes irreducible body mass which is not subjected to weight loss in the denominator of the calculation.
Recently, van der Laar et al. suggested an alternative metric of weight loss reporting, specifically the percentage of alterable weight loss (%AWL), which demonstrated consistent outcomes after Roux-en-Y gastric bypass (RYGB) regardless of the initial BMI [11, 12]. This metric introduced a new concept of alterable weight, which can be affected by therapeutic intervention. The authors asserted that this AWL metric is less likely to mislead the results after bariatric surgery and should be used in scientific research to enable an unequivocal comparison of the efficacy of operations.
In the present study, we aimed to validate the newly introduced %AWL metric in obese Korean patients who underwent laparoscopic RYGB.
Methods
A retrospective review of a prospectively established bariatric surgery database identified all consecutive patients who underwent primary laparoscopic RYGB between 2011 and November 2013. Among them, those patients who were followed up for at least 2 years were included in the present study. Approval for this review of hospital records was obtained from the institutional review board (SCHUH 2017-06-009-002), while the need for informed patient consent was waived.
The institutional guidelines for bariatric surgery at Soonchunhyang University Seoul Hospital in Korea followed the 2011 International Federation for the Surgery of Obesity—Asia-Pacific Chapter Consensus Statements; patients with a body mass index (BMI) ≥ 30 kg/m2 with inadequately controlled obesity-related comorbidities (e.g., diabetes, obstructive sleep apnea, hypertension, or obesity-related arthropathy) or with a BMI ≥ 35 kg/m2 were considered candidates for bariatric surgery. Procedure type was chosen on an individual basis in discussion with the patient considering their metabolic status, surgical risks, and long-term compliance.
Detailed surgical procedures of RYGB were described in our previously published report [13]. Baseline demographics of the enrolled patients including age, sex, and BMI at the time of the operation and anthropometric data at any follow-up time point were collected from the database and the hospital medical records. The nadir BMI of each patient, which was defined as the lowest BMI during the postoperative visits within the two postoperative years, was also identified and collected separately.
Individual relative weight loss is calculated with three different relative metrics using the formula 100% × (initial BMI − postoperative or nadir BMI)/(initial BMI – “a”) with a respective reference BMI value of “a”: a = 0 for %TWL, a = 23 for %EWL [3]. Since the upper limit of normal BMI in the Asian population is 23 kg/m2, a reference value of 23 instead of 25 was adopted to calculate %EWL in the present study [14]. A reference value “a” of 13 was used to calculate the universal %AWL, while gender-specific AWL was drawn by using a = 17 for males and a = 10 for females as proposed by van de Laar et al. [15]. Thus, four datasets of the same nadir outcome are formed for %EWL, %TWL, %AWL, and BMI.
The enrolled patients were classified into subgroups based on their initial BMI. First, they were classified into two halves of lower (1H) and higher BMI (2H) groups and then into four quadrants (1 – 4Q) of even patient numbers in each group. The baseline characteristics and weight loss outcomes expressed in BMI, %EWL, %AWL, and %TWL were compared between the subgroups in terms of nadir weight as well as weight loss trajectory. The difference between sexes in terms of relative weight loss metrics was also analyzed.
Additionally, the reference BMI value “a’ with the lowest variation coefficient was identified based on the same calculating method as van de Laar adopted to identify the inert portion of the Korean patients undergoing LRYGB, which refers to the body part presumed not to be affected by the surgical procedures.
The statistical analysis was performed using SPSS version 18 for Windows (SPSS Inc., Chicago, IL, USA). The mean ± standard deviation or median (range) of the variables was calculated and compared between the subgroups. The chi-square test or Fisher’s exact test was used to analyze categorical variables, while Student’s t test, Mann-Whitney U test, or analysis of variance was used to examine continuous variables. All tests were two-tailed and p values < 0.05 were considered significant.
Results
A total of 165 patients (27 men [16.4%], 138 women [83.6%]; mean age, 37 years) were identified eligible for this study and followed up for 32.9 ± 8.2 months (Table 1). The initial BMI of the total patients was 38.1 ± 5.4 kg/m2.
It took a mean 21.4 months for the patients to reach their nadir BMI of 26.6 ± 4.1 kg/m2 after the surgery (Table 2). This nadir result could be transformed into different values using different outcome metrics: 81% in EWL, 30% in TWL, 45.9% in universal AWL, and 42.8% in gender-specific AWL. There was a statistically significant difference between the sexes in terms of the time required to reach nadir weight, nadir BMI itself, and nadir EWL. Female patients seemed to show better weight loss results in terms of EWL (68.1 ± 15.4 vs. 83.5 ± 26.8%, p < 0.001) and universal AWL (41.8 ± 9.5 vs. 46.8 ± 11.9%, p = 0.041). However, gender-specific AWL revealed the reverse result, which also was statistically significant (49.3 ± 10.8 vs. 41.5 ± 10.5%, p = 0.001), while the result expressed in TWL was similar between the sexes (28.1 ± 7.1 vs. 30.3 ± 7.9%, p = 0.176).
When the patients were divided into subgroups based on their initial BMI, the benchmark BMI for dichotomous division was 37.3; 34.2 and 41.7 served as additional cut-off points for quadrant subgrouping in the present cohort (Table 3). The baseline characteristics were compared between the subgroups and there was no significant difference in age among the subgroups. However, the proportion of male patients gradually increased with the baseline BMI (p = 0.031, linear by linear association).
The weight loss results in the different outcome metrics were compared between the subgroups using the nadir BMI values (Fig. 1). Two groups of lower (1H) and higher (2H) BMI showed significant differences in nadir BMI, EWL, and TWL; the lower BMI group reached an EWL of 92.9% calculated with nadir BMI, while the higher BMI group showed an EWL of only 68.9%, which was significantly poorer weight loss outcome (p ≤ 0.001). In the meantime, their outcomes in nadir universal AWL and gender-specific AWL were similar between the groups (p = 0.325 and p = 0.625, respectively) (Fig. 1a). Similar outcomes were demonstrated upon comparison on the four quadrant subgroups divided evenly based on the baseline BMI. The nadir %EWL outcomes showed a statistically significant gradual decrease from 102.3% down to 67.7% along with an increase in baseline BMI (p < 0.001; Fig. 1b). The reverse outcomes were noted in nadir %TWL, gradual increase in TWL as baseline BMI increased, although the difference seemed less prominent than that in %EWL (p = 0.006). However, %AWL, both in universal and in gender-specific metrics, showed consistent outcomes among the subgroups regardless of initial BMI.

Comparison of the different metrics between subgroups divided by initial BMI. a Comparison between the two subgroups of lower (1H) vs. higher BMI (2H). b Comparison among four quadrant subgroups from the lightest (1Q) to the heaviest quarter (4Q) with even patient numbers. BMI, body mass index; TWL, total weight loss; EWL, excess weight loss; AWL, alterable weight loss
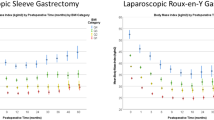
Chronological weight loss outcomes were depicted on comparison of the lower (1H) and higher (2H) BMI groups (Fig. 2). The change in BMI showed parallel trajectories with similar negative slopes between the two groups; the higher BMI group steadily showed higher BMI values than the lower BMI group throughout the follow-up period. This result translated into steadily better %EWL in the higher BMI group throughout the follow-up period. On the other hand, the weight loss outcomes expressed in %TWL or %AWL (whether in universal or gender-specific metrics) showed no statistically significant differences between the two groups.

Chronological changes in the different weight loss metrics. a Body mass index (BMI), b excess weight loss (EWL), c total weight loss (TWL), d alterable weight loss (AWL) in the universal metric, e AWL in the gender-specific metric
The variation coefficient of each metric was calculated of the present study cohort. Among all metrics, universal AWL had the lowest variation coefficient of 25.2% (Table 4). Furthermore, various values of “a” were used to determine the reference value with the lowest variation coefficient in the present Korean study cohort, similarly as Van der Laar had evaluated [15]. As shown in Table 4, a reference value of 11 demonstrated the lowest variation coefficient between the values of 9 to 13.
Discussion
Since the purpose of bariatric and metabolic surgery has been broadened from simple weight loss to concomitant metabolic control in recent years, patients with a lower BMI and concurrent type 2 diabetes are going to be eligible for surgery. Particularly in the Asia-Pacific region, the indications for bariatric surgery and metabolic surgery are modified to include those with a lower BMI than in European or American countries because the Asian population is more vulnerable to obesity-related metabolic diseases with a higher proportion of body fat at the same BMI. However, the conventional metric measuring weight loss, i.e., %EWL, does not properly reflect this change since it adopts the upper limit of normal BMI (which is 23 kg/m2 in Asians) as a reference value in the calculation. It might exaggerate the contribution of weight loss to metabolic improvement in patients with lower BMI after metabolic surgery because this metric would demonstrate superior outcomes in terms of %EWL compared to those with higher BMI. Therefore, it is necessary to devise a proper metric that is universally applicable in various patient populations with different baseline BMI values and various ethnicities to report the surgical outcomes without deviation, particularly in the lower BMI population.
Van der Laar et al. suggested a novel metric drawn from the large study cohort of Bariatric Outcome Longitudinal Database (BOLD), which consisted primarily of Caucasians. [12] They aimed to determine the proper reference value with the same formula previously used calculating the variation coefficient for each adopted reference value “a.” They suggested that a value “a” of 13 represents the inert part of the body mass that cannot be influenced by surgical measures regardless of sex and demonstrated that adopting this value resulted in the lowest variation in weight loss outcomes among patients with different BMI levels at baseline. Therefore, we aimed to validate this formula (%AWL) in Korean patients undergoing RYGB.
The analyses of our data obtained from Korean patients also revealed a considerable discrepancy among the results expressed in the different weight loss reporting metrics. As anticipated, patients with a lower BMI had much smaller excess weight exceeding the reference BMI value of 23 than those with a higher BMI; therefore, weight loss outcomes expressed in %EWL appear to be more favorable in those patients with a lower BMI. However, using a reference value of 13 instead of 23, as shown in the universal %AWL, changed the final results, showing compatible outcomes among patients with different baseline BMI levels. The weight loss outcomes expressed in %TWL were also significantly influenced by the initial BMI as well but in the reverse pattern of those in EWL, showing superior results in patients with a higher BMI in the present study, although the difference was much less exaggerated. The present study demonstrated that AWL minimized the deviation that resulted from the baseline BMI in Korean patients after RYGB. We previously demonstrated the similar results as those of Korean patients who underwent laparoscopic sleeve gastrectomy, which showed the %EWL and %TWL both induced deviation in weight loss outcomes but that %AWL was consistent regardless of baseline BMI [7, 16].
The analyses to calculate the variation coefficient for different reference value “a” showed that the lowest variation coefficient can be achieved using a reference value of 11 in our study cohort. Van der Laar demonstrated that the reference value of 13 showed the lowest variation coefficient in the previous study. In an Asian population, the inert part of the body that cannot be affected by surgical procedures seems to be smaller compared to that of Caucasians. Nonetheless, it is necessary to establish a common and clinically relevant metric that is universally applicable across different ethnicities, and the %AWL metric based on the average inert BMI of 13 appeared to fit the Asian population. This new metric enabled the demonstration of consistent weight loss outcomes regardless of the baseline BMI despite different inert BMI values in Korean patients.
A recent study showed that the postoperative improvement of type 2 diabetes after gastric bypass matched postoperative weight loss expressed as %AWL and %TWL but not as %EWL [17]. Although the AWL metric may not be readily understandable by patients and providers in clinical practice, it is expected to facilitate a precise prediction of weight loss as well as metabolic effect regardless of baseline BMI in patients undergoing bariatric surgery. Furthermore, it would be useful to identify a more accurate prediction model of diabetes remission after metabolic surgery based on an unbiased weight loss reporting method.
Although this is the first study from Asia to validate the AWL metric, there are several limitations. First, the number of patients included in the present was insufficient to generalize the concept of AWL in all Asian population. It was difficult to delineate the clinical relevance of AWL in terms of improved metabolic profiles or quality of life following bariatric surgery due to the small number of patients with concurrent comorbidities. Still, the present study at least demonstrated the potential that the AWL metric can serve as a better option of reporting weight loss with the least deviation derived from the baseline BMI in Asian population as well.
In conclusion, the AWL metric can be used to report weight loss regardless of baseline BMI in Korean patients undergoing RYGB. However, this metric must be further validated in a larger population involving multiple centers from the Asia-Pacific area before it can be used clinically. Furthermore, it should be further evaluated whether this AWL metric can be applied universally in Asian patients undergoing other types of bariatric procedures, including patients with a much lower BMI who underwent surgery for metabolic purposes.
References
Dixon JB, McPhail T, O'Brien PE. Minimal reporting requirements for weight loss: current methods not ideal. Obes Surg. 2005;15(7):1034–1039. PubMed Epub 2005/08/18. eng. https://doi.org/10.1381/0960892054621053.
Oria HE, Carrasquilla C, Cunningham P, et al. Guidelines for weight calculations and follow-up in bariatric surgery. Surg Obes Relat Dis: Off J Am Soc Bariatric Surg. 2005;1(1):67–68. PubMed Epub 2006/08/24. eng. https://doi.org/10.1016/j.soard.2004.12.005.
Deitel M, Gawdat K, Melissas J. Reporting weight loss 2007. Obes Surg. 2007;17(5):565–8. https://doi.org/10.1007/s11695-007-9116-0.
Higa KD, Boone KB, Ho T, et al. Laparoscopic Roux-en-Y gastric bypass for morbid obesity: technique and preliminary results of our first 400 patients. Arch Surg (Chicago, Ill : 1960). 2000;135(9):1029–33. discussion 33-4. PubMed Epub 2000/09/12. eng
Biertho L, Steffen R, Ricklin T, et al. Laparoscopic gastric bypass versus laparoscopic adjustable gastric banding: a comparative study of 1,200 cases. J Am Coll Surg 2003;197(4):536–544; discussion 44-5. PubMed Epub 2003/10/03. eng, doi: https://doi.org/10.1016/S1072-7515(03)00730-0.
Biron S, Hould FS, Lebel S, et al. Twenty years of biliopancreatic diversion: what is the goal of the surgery? Obes Surg. 2004;14(2):160–164. PubMed Epub 2004/03/17. eng. https://doi.org/10.1381/096089204322857492.
Park JY, Kim YJ. Efficacy of laparoscopic sleeve gastrectomy in mildly obese patients with body mass index of 30-35 kg/m(2). Obes Surg. 2015;25(8):1351–1357. PubMed Epub 2015/02/07. eng. https://doi.org/10.1007/s11695-015-1575-0.
Karmali S, Birch DW, Sharma AM. Is it time to abandon excess weight loss in reporting surgical weight loss? Surg Obes Relat Dis: Off J Am Soc Bariatric Surg. 2009;5(4):503–506PubMed Epub 2009/07/28. eng. https://doi.org/10.1016/j.soard.2009.04.014.
Hatoum IJ, Kaplan LM. Advantages of percent weight loss as a method of reporting weight loss after Roux-en-Y gastric bypass. Obesity (Silver Spring, Md). 2013;21(8):1519–25. PubMed Pubmed Central PMCID. Epub 2013/05/15. eng
Brethauer SA, Kim J, el Chaar M, et al. ASMBS Clinical Issues Committee. Standardized outcomes reporting in metabolic and bariatric surgery. Sur Obes Relat Dis: Off J Am Soc Bariatric Surg. 2015;11(3):489–506. PubMed Epub 2015/06/22. eng. https://doi.org/10.1016/j.soard.2015.02.003.
van de Laar AW, Dolle MH, de Brauw LM, et al. Validating the alterable weight loss (AWL) metric with 2-year weight loss outcome of 500 patients after gastric bypass. Obes Surg. 2014;24(7):1085–1089. PubMed Epub 2014/02/25. eng. https://doi.org/10.1007/s11695-014-1203-4.
van de Laar AW. Algorithm for weight loss after gastric bypass surgery considering body mass index, gender, and age from the Bariatric Outcome Longitudinal Database (BOLD). Surg Obes Relat Dis: Off J Am Soc Bariatric Surg. 2014;10(1):55–61. PubMed Epub 2013/10/15. eng. https://doi.org/10.1016/j.soard.2013.05.008.
Park JY, Kim YJ. Laparoscopic Roux-en-Y gastric bypass in obese Korean patients: efficacy and potential adverse events. Surg Today. 2016;46(3):348–355. PubMed Epub 2015/04/29. eng. https://doi.org/10.1007/s00595-015-1170-y.
Organization WH. The Asia-Pacific perspective: redefining obesity and its treatment. Health Communications Australia: Sydney; 2000.
van de Laar AW, de Brauw M, Bruin SC, et al. Weight-independent percentile chart of 2880 gastric bypass patients: a new look at bariatric weight loss results. Obes Surg. 2016;26(12):2891–2898. PubMed Epub 2016/05/04. eng. https://doi.org/10.1007/s11695-016-2200-6.
Park JY, Kim YJ. Reply to the Letter to Editor entitled “the %EBMIL/%EWL double-booby trap. A comment on studies that compare the effect of bariatric surgery between heavier and lighter patients”. Obes Surg. 2016;26(3):614–616. PubMed Epub 2015/12/02. eng. https://doi.org/10.1007/s11695-015-1970-6.
van de Laar AW, de Brauw LM, Meesters EW. Relationships between type 2 diabetes remission after gastric bypass and different weight loss metrics: arguments against excess weight loss in metabolic surgery. Surg Obes Relat Dis: Off J Am Soc Bariatric Surg. 2016;12(2):274–282. PubMed Epub 2015/10/20. eng. https://doi.org/10.1016/j.soard.2015.07.005.
Acknowledgements
This research was supported by the Soonchunhyang University Research Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Informed Consent
The need for patient informed consent for this retrospective study was waived by the institutional review board.
Ethical Approval
This study was approved by the institutional ethics committee of Soonchunhyang University Seoul Hospital and has been performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Park, J.Y., Kim, Y.J. Validation of the Alterable Weight Loss Metric in Morbidly Obese Patients Undergoing Gastric Bypass in Korea. OBES SURG 28, 1704–1710 (2018). https://doi.org/10.1007/s11695-017-3084-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-3084-9