
Abstract
Background
The association of obesity with atrial fibrillation (AF) and with ventricular arrhythmias is well documented.
Objective
The aim of this study was to investigate whether weight reduction by a laparoscopic sleeve gastrectomy has any effect on P wave dispersion (PWD), a predictor of AF, and corrected QT interval dispersion (CQTD), a marker of ventricular arrhythmias, in obese individuals.
Methods
In a prospective study, a total of 114 patients (79 females, 35 males) who underwent laparoscopic sleeve gastrectomy were examined. The patients were followed 1 year. PWD and CQTD values before and 3rd, 6th, and 12th months after the surgery were calculated and compared.
Results
There was a statistically significant decline in body mass index (BMI), PWD, and CQTD values among baseline, 3rd, 6th, and 12th months (p < 0.001 for all comparisons). Correlation analysis showed a statistically significant correlation between ΔPWD and ΔBMI (r = 0.719, p < 0.001), ΔPWD and Δleft ventricular end-diastolic diameter (LVEDD) (r = 0.291, p = 0.002), ΔPWD and Δleft atrial diameter (LAD) (r = 0.65, p < 0.001), ΔCQTD and ΔBMI (r = 0.266, p = 0.004), ΔCQTD and ΔLVEDD (r = 0.35, p < 0.001), ΔCQTD and ΔLAD (r = 0.289, p = 0.002). In multiple linear regression analysis, there was a statistically significant relationship between ΔPWD and ΔBMI (β = 0.713, p < 0.001), ΔPWD and ΔLVEDD (β = 0.174, p = 0.016), ΔPWD and ΔLAD (β = 0.619, p < 0.001), ΔCQTD and ΔBMI (β = 0.247, p = 0.011), ΔCQTD and ΔLVEDD (β = 0.304, p < 0.001), ΔCQTD and ΔLAD (β = 0.235, p = 0.009).
Conclusion
PWD and CQTD values of patients were shown to be attenuated after bariatric surgery. These results indirectly offer that there may be a reduction in risk of AF, ventricular arrhythmia, and sudden cardiac death after obesity surgery.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Obesity is widely accepted as a common public health problem and the estimated prevalence worldwide is 13% [1]. The relationship between obesity and many diseases, especially hypertension, diabetes mellitus, dyslipidemia, stroke, and coronary heart disease, has been clearly demonstrated [2]. The mortality due to all causes and cardiovascular causes increased throughout life in obese subjects [1] Apart from coronary heart disease, the association of obesity especially with atrial fibrillation (AF) and with ventricular arrhythmias is well documented [3, 4].
P wave dispersion (PWD) is defined as the difference between the widest and narrowest P wave durations in a record from a 12-lead electrocardiogram (ECG). The success of PWD in demonstration of atrial remodeling and prediction of AF has been shown in many studies [5]. Similarly, QT interval dispersion (QTD) is defined as the difference between the longest and shortest QT intervals measured in a 12-lead ECG. QTD is known to be associated with increased risk of sudden cardiac death and ventricular arrhythmia [6, 7].
Surgical methods in obesity treatment are increasingly used in recent years. With different surgical techniques, laparoscopic sleeve gastrectomy is one of the most preferred methods in obesity surgery nowadays and is an effective and reliable treatment and the success of this method in the treatment of obesity has been shown in many studies [8,9,10].
The aim of this study was to investigate whether weight reduction by a laparoscopic sleeve gastrectomy has any effect on PWD and QTD measurements in obese individuals.
Material and Method
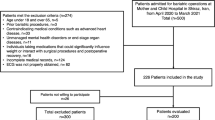
The study was designed as prospectively. Patients with a BMI > 40 kg/m2 who were previously tested but failed by non-surgical methods were considered to have an indication for surgery. A total of 129 patients (89 females, 40 males) who underwent laparoscopic sleeve gastrectomy between July 1, 2012, and December 31, 2015 were included into the study. Nine patients did not come to regular checkups, 2 patients had a diagnosis of coronary artery disease after the operation, 1 patient had a post-op AF, and 3 subjects did not want to continue to the study. The data for the remaining 114 patients (79 female, 35 male) were analyzed. Demographic, clinical, laboratory, and anthropometric measurements of the patients were recorded before and 3rd, 6th, and 12th months after the surgery. PWD and corrected QTD (CQTD) values before and 3rd, 6th, and 12th months after the surgery were calculated and compared.
Delta (Δ) values were obtained by subtracting the 12th-month values from the baseline values for BMI, fasting plasma glucose (FPG), total cholesterol (TC), low density lipoprotein (LDL), high density lipoprotein (HDL), triglyceride, systolic blood pressure (SBP), diastolic blood pressure (DBP), left ventricular end-diastolic diameter (LVEDD), left atrial diameter (LAD), PWD, and CQTD.
Using standard 2 dimensional (2D) and Doppler evaluation according to the recommendations of the American Society of Echocardiography [11] and European Association of Cardiovascular Imaging performed echocardiographic evaluation. The ejection fraction (EF) was calculated by the modified Simpson method. In this study, LVEDD and LAD were measured in the parasternal long axis imaging.
The following patients were excluded from the study: patients with a known AF or AF history, ventricular arrhythmia history (ventricular tachycardia or ventricular fibrillation), known coronary heart disease, heart failure, genetic arrhythmic syndromes, hypertrophic cardiomyopathy, permanent pacemaker, dialysis-requiring renal failure, chronic liver disease, autoimmune diseases, pulmonary hypertension, and chronic obstructive pulmonary disease, and patients who do not want to participate in the study.
Calculation of QTD with Electrocardiogram Characteristics and PWD
All patients were drawn and recorded with standard ECG (25 mm/s and 10 mm/mV) and 50 mm/s and 10 mm/mV specific ECGs. ECG was performed when patient was in the supine position and the electrodes were withdrawn at standard sites [12]. In the ECG taken at high speed, the duration of the P wave in all the leads was measured at 3 consecutive heart beats, and the average of the measured values was used to calculate the P wave duration in each derivation. The PWD was calculated by subtracting the value of the lead at which the peak of the P wave was measured from the value of the lead at which the lowest was measured. Similarly, in high-velocity ECGs, the QT interval was measured in all the leads and the corrected QT (CQT) was calculated with the Bazett formula (CQT = QT(s)/√RR(s)). In each derivation, CQT was calculated at 3 consecutive heart beats and averages of these 3 measurements were obtained. The difference between the highest measured CQT and the lowest measured lead was calculated and the corrected QTD (CQTD) was calculated. Both PWD and CQTD measurements were made at different times by 2 different cardiologists and the averages of the values found by these 2 operators were taken.
Operative Technique
Under general anesthesia, the patient was positioned supine at reverse Trendelenburg position. The 15-mm port was located in right upper quadrant near the midline location. The other of these ports in right upper quadrant was 10-mm port. Two 5-mm ports were placed in the left upper quadrant laterally, and in the right upper quadrant. A liver retractor was placed in the epigastric region. The greater curvature of the stomach was devascularized by a harmonic scalpel. The division of all vessels adjacent to the greater curvature was continued up to the left crus of the diaphragm. A complete mobilization of the fundus in this area was performed and the stomach is attached only by the lesser curvature. After the placement of 32- to 36-French bougie in the stomach and positioned along the lesser curvature, 4 or 5 laparoscopic endostapler was applied through the greater curvature. Endostapler was applied according to the length of the greater curvature. Then a methylene blue leak test was performed. The specimen was removed through the 15-mm trocar site in an endobag. Finally 15-mm port site was closed primarily.
Statistical Analyses
Variables are presented as mean±SD or median (range, interquartile range [IQR]) for continuous data and as proportion for categorical data. Continuous variables with normal distribution were analyzed with repeated measures ANOVA. The Kolmogorov-Smirnov test was used to identify whether continuous variables were normally distributed. Two-sided p values < 0.05 were considered significant. The degrees of association between continuous variables were evaluated by using Pearson’s or Spearman’s correlation tests as appropriate. Independent determinants of PWD and QTD were determined by standard multiple linear regression analysis. A two-sided p < 0.05 was accepted as significant. Statistical analysis was performed using commercially available computer program (SPSS version 21.0 for Windows; SPSS, Inc., Chicago, Illinois, US).
Results
A total of 114 patients, 79 women (69%) and 35 men (31%), were included into the study. Baseline clinical, and demographic, anthropometric, and laboratory values of the patients are summarized in Table 1. There was a statistically significant difference in BMI values among baseline, 3rd, 6th, and 12th months (p < 0.001). When PWD and CQTD measurements were compared, there were statistically significant differences among baseline, 3rd, 6th, and 12th months (p < 0.001 for both groups).
Baseline, 3rd, 6th, 12th months BMI, PWD, and CQTD values of patients and their comparisons are summarized in Table 2. When the data including BMI, PWD, and CQTD values in the 3rd month were compared with baseline, there was a statistically significant difference. This significant difference was also observed when the same variables in the 6th month were compared with the 3rd month as well as the variables of the 12th month were compared with the 6th month (p < 0.001 for all groups). Figure 1 shows the change of BMI, PWD, and CQTD during the follow-up period. Table 3 summarizes the values of BMI, blood pressures, echocardiographic measurements, and glycemic and lipid profiles of our study population at the end of the 12th month. Table 4 shows the results of correlation analyses and linear regression analysis between ΔBMI, ΔFPG, ΔSBP, ΔDBP, ΔLVEDD, ΔLAD, ΔTC, ΔLDL, ΔHDL, Δtriglyceride parameters and ΔPWD, and ΔCQTD. Correlation analysis showed a statistically significant correlation between ΔPWD and ΔBMI, ΔLVEDD, ΔLAD (r = 0.719, p < 0.001, r = 0.265, p = 0.004, r = 0.624, p < 0.001, respectively), between ΔCQTD and ΔBMI, ΔLVEDD, ΔLAD (r = 0.266, p = 0.004, r = 0.36, p < 0.001, r = 0.287, p = 0.002) as shown in Fig. 2. No significant correlation was found between other variables. In multiple linear regression analysis, there was a statistically significant relationship between ΔPWD and ΔBMI, ΔLVEDD, ΔLAD (β = 0.713, p < 0.001, β = 0.17, p = 0.023, β = 0.596, p < 0.001, respectively), between ΔCQTD and ΔBMI, ΔLVEDD, ΔLAD (β = 0.247, p = 0.011, β = 0.323, p < 0.011, β = 0.236, p = 0.008, respectively).

Change of BMI, PWD, and CQTD values of subjects during the follow-up period (BMI body mass index, CQTD corrected QT interval dispersion, PWD P wave dispersion)

Correlation analysis between ΔPWD, ΔCQTD and ΔBMI, ΔLVEDD, ΔLAD (BMI body mass index, CQTD corrected QT interval dispersion, LAD left atrial diameter, LVEDD left ventricular end-diastolic diameter, PWD P wave dispersion)
Discussion
This is the first study that investigated PWD and CQTD measurements in patients who underwent bariatric surgery. We showed that PWD and CQTD values of patients were attenuated after bariatric surgery. These results indirectly offer that there may be a reduction in risk of AF, ventricular arrhythmia, and sudden cardiac death after obesity surgery, since PWD and CQTD are predictors of these adverse events The reduction in these risks was seem to be directly related to the decrease in BMI and was independent of changes in FPG, SBP, DBP, and cholesterol levels.
Increased LV diastolic dysfunction, increased sympathetic activation, increased inflammation, and increased infiltration of the atrium with adipocytes in obese patients may explain the increased incidence of AF in obese patients [13, 14]. Several studies have shown the importance of weight reduction in obese patients in the treatment of AF. In a study conducted by Abed et al. showed that weight reduction in obese patients has been shown to reduce the severity and frequency of AF symptoms and also to be beneficial in the improvement of cardiac remodeling [15]. Another study by Pathak et al. has shown that weight reduction in obese patients with risk factor modification increases success in AF ablation [16]. Jamaly et al. investigated 4021 obese individuals with sinus rhythm and no history of AF. This study showed that the risk of new onset AF was reduced in obese patients undergoing bariatric surgery. They speculated that weight reduction could affect various factors that might result in an improvement in cardiac geometry and function leading to attenuation of AF episodes. Our findings support their data by showing that the weight reduction favorably affects LAD [17]. In another study by Falchi et al., weight reduction has been shown to correlate with a reduction in PWD [18]. Another result of the study was that ΔPWD and ΔBMI, ΔLVEDD, and ΔLAD were positively correlated. Furthermore, in multiple linear regression analysis, there was a statistically significant relationship between ΔPWD and ΔBMI, ΔLVEDD, ΔLAD. In previous studies, it was shown that obesity is independently associated with increased left ventricular hypertrophy and left atrial size in adults. The possible causes of these increases are hypertension, volume overload, and deterioration of left ventricular diastolic dysfunction. In the Framingham Heart Study were found that obese patients have an increased risk of developing AF, and this risk was associated with the increase in left atrial size [19]. The results of these studies support our study findings. In our study, PWD value was calculated as 34.2 ± 3.3 msn at 12 months after bariatric surgery and this value is still above normal [20], but it should not be forgotten that the mean BMI of the patients was 31.6 ± 4.8 kg/m2 after 12 months of follow-up and that these patients were still in the obese category.
The relationship between obesity and sudden cardiac death has been well known since ancient times. Hippocrates’ observations have shown that more sudden deaths are seen in overweight people than in non-overweight people [21]. Large-scale population studies of modern medicine have been shown that the risk of sudden cardiac death is high in obese individuals [22]. The relationship between ventricular arrhythmias leading to sudden cardiac death and obesity is multifactorial. The association of obesity with ventricular remodeling, ventricular dilatation, hypertrophy, and diastolic dysfunction are well known [23, 24]. In patients with ventricular arrhythmia, fat infiltration in the myocardium [25], which may trigger ventricular arrhythmias with slow conduction of electrical current, has been demonstrated. In another small-scale study of rats, it has been shown that obesity caused by high-fat diet, results in arrhythmogenic gene expression [26]. All these possible mechanisms may explain the high risk of ventricular arrhythmias and sudden cardiovascular death in obesity. Although the relationship between ventricular arrhythmia and sudden cardiac measurement is clearly shown in obesity, there is no large-scale study showing whether weight reduction can reduce this risk. Increased QTD was shown to be a predictor of ventricular arrhythmia and increased risk of sudden cardiac death [6, 7]. Therefore, reduction in CQTD in the patients who underwent bariatric surgery might have salutary effects in preventing ventricular arrhythmias and sudden cardiac death. This reduction is also well correlated with reduction in BMI and was independent in improvements of metabolic factors.
Patients may be informed that there is indirect evidence that there may be a reduction in developing new arrhythmic events after successful obesity surgery.
Study Limitations
Our study has some limitations. The patients were not followed with respect to the frequency of developing AF or ventricular arrhythmias. Furthermore, patients with known arrhythmias were not included in the study. Periodic Holter monitoring before and after surgery could have helped to detect arrhythmic events even though the expected frequency of arrhythmic events in these particular subjects is probably very low. Holter monitoring could demonstrate the improvement in arrhythmic events following weight reduction. Some of the patients were using antihypertensive, antidiabetic, and antidyslipidemic drugs. The use of these drugs could hide the extent of improvement in metabolic markers after obesity surgery. This may affect the results of correlation analysis. In addition, measurement of blood pressure once during visits may not reflect blood pressure profile of the patients. The subjects have been followed 12 months and the long-term results are unknown. More patients and longer-term follow-up study may be needed.
Conclusion
PWD and CQTD values after obesity surgery are decreased with weight loss. This decrease was correlated with a decrease in BMI and was independent of improvement in metabolic values.
References
Jensen MD, Ryan DH, Apovian CM, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines.; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014;63(25 Pt B):2985–3023.
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980– 2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81.
Hatem SN. Atrial fibrillation and obesity: not just a coincidence. J Am Coll Cardiol. 2015;66(1):12–3.
Narayanan K, Zhang L, Kim C, et al. QRS fragmentation and sudden cardiac death in the obese and overweight. J Am Heart Assoc 2015;4(3):e001654.
Okutucu S, Aytemir K, Oto A. P-wave dispersion: what we know till now? JRSM Cardiovasc Dis 2016:21;5:2048004016639443.
DE Maria E, Curnis A, Garyfallidis P, et al. QT dispersion on ECG Holter monitoring and risk of ventricular arrhythmias in patients with dilated cardiomyopathy. Heart Int. 2006;2(1):33.
Higham PD, Campbell RW. QT dispersion. Br Heart J. 1994;71(6):508–10.
Azagury DE, Morton JM. Bariatric surgery: overview of procedures and outcomes. Endocrinol Metab Clin North Am. 2016;45:647–56.
Nocca D, Loureiro M, Skalli EM, et al. Five-year results of laparoscopic sleeve gastrectomy for the treatment of severe obesity. Surg Endosc. 2017;31(8):3251–7.
Kehagias I, Zygomalas A, Karavias D, et al. Sleeve gastrectomy: have we finally found the holy grail of bariatric surgery? A review of the literature. Eur Rev Med Pharmacol Sci. 2016;20(23):4930–42.
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28:1–39.
Kligfield P, Gettes LS, Bailey JJ, et al. Recommendations for the standardization and interpretation of the electrocardiogram: part I: the electrocardiogram and its technology a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2007;49(10):1109–27.
Russo C, Jin Z, Homma S, et al. Effect of obesity and overweight on left ventricular diastolic function: a community-based study in an elderly cohort. J Am Coll Cardiol. 2011;57:1368–74.
Pathak RK, Middeldorp ME, Meredith M, et al. Long-term effect of goal-directed weight management in an atrial fibrillation cohort: a long-term follow-up study (LEGACY). J Am Coll Cardiol. 2015;65:2159–69.
Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310(19):2050–60.
Pathak RK, Middeldorp ME, Lau DH, et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. 2014;64(21):2222–31.
Jamaly S, Carlsson L, Peltonen M, et al. Bariatric surgery and the risk of new-onset atrial fibrillation in Swedish obese subjects. J Am Coll Cardiol. 2016;68(23):2497–504.
Falchi AG, Grecchi I, Muggia C, et al. Weight loss and P wave dispersion: a preliminary study. Obes Res Clin Pract. 2014;8(6):e614–7.
Goudis CA, Korantzopoulos P, Ntalas IV, et al. Obesity and atrial fibrillation: a comprehensive review of the pathophysiological mechanisms and links. J Cardiol. 2015;66(5):361–9.
Aytemir K, Ozer N, Atalar E, et al. P wave dispersion on 12-lead electrocardiography in patients with paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. 2000;23(7):1109e12.
Mann WN. Hippocrates in ancient and modern times. Guys Hosp Gaz. 1952;66(1661):108–13.
Noheria A, Teodorescu C, Uy-Evanado A, et al. Distinctive profile of sudden cardiac arrest in middle-aged vs. older adults: a community-based study. Int J Cardiol. 2013;168:3495–9.
Alpert MA. Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. Am J Med Sci. 2001;321:225–36.
Morse SA, Bravo PE, Morse MC, et al. The heart in obesity-hypertension. Expert Rev Cardiovasc Ther. 2005;3:647–58.
Molinari G, Sardanelli F, Zandrino F, et al. Adipose replacement and wall motion abnormalities in right ventricle arrhythmias: evaluation by MR imaging. Retrospective evaluation on 124 patients. Int J Card Imaging. 2000;16:105–15.
Ashrafi R, Yon M, Pickavance L, et al. Altered left ventricular ion channel transcriptome in a high-fat-fed rat model of obesity: insight into obesity-induced arrhythmogenesis. J Obes. 2016;2016:7127898.
Acknowledgments
The authors would like to thank their cardiology fellows due to value contributions.
Funding
This study was approved by Baskent University Institutional Review Board and Ethics Committee and supported by Baskent University Research Funding (KA 16/281).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
After giving detailed information about the study, informed consent (writing) was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Yılmaz, M., Altın, C., Tekin, A. et al. Assessment of Atrial Fibrillation and Ventricular Arrhythmia Risk after Bariatric Surgery by P Wave/QT Interval Dispersion. OBES SURG 28, 932–938 (2018). https://doi.org/10.1007/s11695-017-2923-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2923-z