
Abstract
Vitamin B12 dosage in multivitamin supplementation in the current literature is quite variable. There is no consensus about the optimal treatment of vitamin B12 deficiency. A systematic literature search on different supplementation regimes to treat perioperative vitamin B12 deficiencies in bariatric surgery was performed. The methodological quality of ten included studies was rated using the Newcastle Ottawa scale and ranged from moderate to good. The agreement between the reviewers was assessed with a Cohen’s kappa (0.69). The current literature suggests that 350 μg oral vitamin B12 is the appropriate dose to correct low vitamin B12 levels in many patients. Further research must focus on a better diagnosis of a vitamin B12 deficiency, the optimal dose vitamin B12 supplementation, and clinical relevance next to biochemical data.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vitamin B12 deficiencies are common after bariatric surgery. Schilling et al. estimated the prevalence of vitamin B12 deficiency to be 12–33% [1]. Other researchers have suggested a much greater prevalence of vitamin B12 deficiency in up to 75% of postoperative Roux-en-Y gastric bypass (RYGB) patients. However, most reports have shown approximately 35% of postoperative RYGB patients as vitamin B12 deficient [1–6]. Experts have noted the significance of a functional/subclinical deficiency in the low-normal vitamin B12 range (defined as vitamin B12 levels between 140 and 200 pmol/l) that does not exhibit clinical evidence of deficiency. The methylmalonic acid (MMA) assay is the preferred marker of vitamin B12 status because metabolic changes often precede low vitamin B12 levels in the progression to deficiency. The evidence for the optimal vitamin B12 supplementation regimen after bariatric surgery is lacking [9]. The dose of vitamin B12 in multivitamin (MV) supplementation in the current literature shows a wide range of variety. There is also no consensus about the optimal treatment of a vitamin B12 deficiency.
This systematic review specifically focuses on vitamin B12 supplementation regimes after bariatric surgery. To disclose, we studied the current scientific knowledge regarding the following:
-
the effect of additional vitamin B12 supplementation in this patient population
-
the effect of different vitamin B12 supplementation regimens on blood levels of vitamin B12
Methods
A systematic multidatabase literature search was conducted. The patient population of interest were all patients before or after bariatric surgery. The intervention studied was vitamin B12 supplementation compared to no supplementation (or different supplementation vitamin B12 regimen). Outcome measures were blood levels of vitamin B12.
Pubmed, Embase, Medline, and The Cochrane Library were searched from the earliest date of each database up to December 2015. The search string used for the literature search used the following keywords and was modified for each database: bariatric surgery OR metabolic surgery OR sleeve gastrectomy OR roux-en-y gastric bypass OR mini gastric bypass OR omega loop gastric bypass OR biliopancreatic diversion OR duodenal switch OR single anastomosis duodeno-ileal bypass AND vitamin B12 supplementation AND blood levels vitamin B12.
Authors HS and SP screened and selected studies on the basis of title and abstract, separately. After primary selection, authors (HS and SP) reviewed the full text of the selected studies and determined suitability for inclusion, based on the established selection criteria. For further eligible studies, cross-references were screened. Disagreements were solved by discussion with each other and the senior author (JS) until consensus was reached.
Inclusion Criteria
-
Randomized controlled trial, prospective or retrospective cohort study
-
Patients who were scheduled for bariatric surgery or patients postbariatric
-
All surgical procedures were included (Laparoscopic Gastric banding, Vertical Banded Gastroplasty, Roux-en Y Gastric Bypass, Omega Loop Bypass, Duodenal Switch, biliopancreatic diversion, single anastomosis duodeno-ileal bypass)
-
Outcome measure of interest was vitamin B12 levels
Exclusion Criteria
-
Cross-sectional studies
-
Studies looking at prebariatric and/or postbariatric patients with renal insufficiency
-
Postbariatric body contouring surgery and vitamin B12 supplementation
For rating the methodological quality, the Newcastle-Ottawa scale for non-randomized trials (NOS) was used [10]. Stars awarded for each quality item serve as a quick visual assessment. Stars are awarded such that the highest quality studies are awarded up to nine stars. The NOS assigns up to a maximum of nine points for the least risk of bias in three domains: (1) selection of study groups (four points), (2) comparability of groups (two points), and (3) ascertainment of exposure and outcomes (three points) for case–control and cohort studies, respectively.
Two authors (HS and SP) separately assessed the NOS scale of the included studies. A Cohen’s kappa score was calculated to determine the level of agreement between authors HS and SP. A Cohen’s kappa score <0.20 indicates a poor agreement, 0.21–0.40 a fair agreement, 0.41–0.60 a moderate agreement, 0.61–0.80 a good agreement, and 0.81–1.00 a very good agreement [16].
Measurement Unit of Vitamin B12 Levels
All the included vitamin B12 levels were calculated in one general unit (pmol/L), if possible.
Results
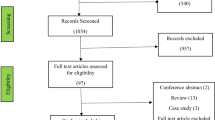
The primary literature search produced 532 results, including 37 duplicates. After selection on title and abstract, 19 studies were found possibly relevant. Nine studies were excluded, 5 of them were conference abstracts, 2 of them were not online available, 1 study did not use MV supplementation, and 1 study consisted of a survey among bariatric surgeons. Due to heterogeneity in patient populations, the small sample size of the included studies and lack of standardized reporting of outcome measures (type of supplementation regime and dose of vitamin B12 in the prescribed supplementation), a meta-analysis was not conducted. In total, 10 studies were included in this systematic review.
Figure 1 outlines our search strategy. The methodological quality of the included studies ranged from moderate to good, indicated by the NOS scale (Table 1). A Cohen’s kappa of 0.69 reflected a good agreement between authors HS and SP. Table 2 gives an overview of the results of the included studies.

PRISMA Flowchart
Study Characteristics
Of all the included studies, 1 study was a triple-blind randomized controlled trial [23], 4 studies were prospective cohort studies [9, 11, 12, 15], and 5 studies were retrospective cohort studies [6, 13, 14, 17, 18]. In total, 10 studies consisted of 1277 participants.
Intervention and Follow-up Length
The length of the intervention ranged from 3 months to 10 years postoperative. Intervention and follow-up length of all studies were described in Table 3.
Vitamin B12 Supplementation
In 8 studies, the dose of vitamin B12 in the MV supplementation was different (Table 4). The studies of Ramos et al. [18] and Brolin et al. [6] lacked the dose of vitamin B12 of MV supplements.
Outcomes of Laboratory Tests of Vitamin B12
Outcomes of laboratory tests are described in Table 5. All vitamin B12 levels were calculated in pmol/L, except the studies of Brolin et al. [6] and Ramos et al. [18], which was suspected to have used wrong measurement units for indicating a vitamin B12 deficiency. Therefore, the original measurement units of the studies were used in this paragraph. Reference ranges of vitamin B12 levels of all studies are described in Table 3.
Complaints and Clinical Effects
All included studies did not control the vitamin B12 deficient-related complaints. Clinical relevance of the deployed supplementation regime has not been studied in all manuscripts.
Discussion
This systematic review highlights the current evidence on the effects of MV or additional vitamin B12 supplementation in patients after bariatric surgery. Vitamin B12 supplementation has an effect on the intracellular vitamin B12 content, and in the optimal dosage, it can prevent vitamin B12 deficiency. However, vitamin B12 deficiencies preoperatively are not uncommon in morbidly obese people. In the study of Dogan et al. [23], vitamin B12 deficiency was diagnosed in 9 patients (6.1%) and 3 patients (5.2%) in the study of Donadelli et al. [9] had a vitamin B12 deficiency in the preoperative period. This is not clearly reported in the other 8 studies.
There is no consensus about the optimal dosage of vitamin B12 supplementation after bariatric surgery worldwide. ASMBS guidelines advise oral vitamin B12 supplements of 350 to 500 μg, and if necessary, intramuscular (IM) injections of 1000 μg per month [24]. The ACCE/TOS/ASMBS guidelines advise that oral supplementation with crystalline vitamin B12 at a dosage of 1000 μg daily or more may be used to maintain normal vitamin B12 levels. Intranasally administered vitamin B12, 500 μg weekly, may also be considered. Parenteral (IM or subcutaneous) vitamin B12 supplementation, 1000 μg/month to 1000–3000 μg every 6 to 12 months, is indicated if vitamin B12 sufficiency cannot be maintained using oral or intranasal routes [25].
However, definitive conclusions cannot be made after this systematic review, because of the heterogeneity of MV supplementation or additional vitamin B12 IM injection regimes and timing of this additional vitamin B12 IM injections. Besides that, all the included studies did not control the vitamin B12 deficient-related complaints. Clinical relevance has not been studied in all manuscripts. These data are needed to examine whether biochemical benefits of vitamin B12 supplementation are correlated with clinical improvement. Besides that, surgical techniques affect the absorption of vitamin B12. Intrinsic factor (IF) is produced by the parietal cells of the stomach, and IF is needed to absorb vitamin B12 in the terminal ileum.
In this review, laparoscopic sleeve gastrectomy (LSG), RYGB, and vertical-banded gastroplasty (VBG) are discussed. LSG patients have reduced production of stomach acid and reduced availability of IF. In RYGB patients, a vitamin B12 deficiency loss of IF and acid secretion in the stomach is expected. The remnant stomach and duodenum are eliminated from the digestion process as well. The VBG serve only to restrict and decrease food intake and do not interfere with the normal digestive process. In this procedure, the upper stomach near the esophagus is stapled vertically to create a small pouch along the inner curve of the stomach. The outlet from the pouch to the rest of the stomach is restricted by a band.
Two interesting findings were found in the included studies. First, in 4 included studies, a dose of 350 μg vitamin B12 per day was used [12, 14, 15, 23]. In the study of Moore et al. [15], vitamin B12 levels of all patients were increased 3 months postoperatively. In the study of Dogan et al. [23], high-dose vitamin B12 supplements result in fewer vitamin B12 deficiencies compared with standard MV supplements. The study of Homan et al. [14] showed that high-dose vitamin B12 supplement is more effective than is a standard MV supplement to reduce the number of patients with vitamin B12. In the study of Rhode et al. [12], serum levels of vitamin B12 were >150 pmol/L after 6 months in 95% of the patients.
Secondly, all the other studies used MV supplementation with a dose of vitamin B12 ranging from 3 to 12 μg per day [9, 17] or unknown dose of vitamin B12 [6, 18]. The studies of Brolin et al., Donadelli et al., and Gasteyger et al. showed many vitamin B12 deficiencies in the follow up [6, 9, 17]. Contrary results were found in the study of Ramos et al. [18]; the vitamin B12 levels are within the reference standards. However, the dose of vitamin B12 in his study was unknown.
Vitamin B12 Supplementation
Dose of vitamin B12 in the MV supplementation in all included studies is varied from 1 μg/day to high-dose supplementation with 350–600 μg/day. MV supplements with 350 μg vitamin B12 per day can maintain normal-high vitamin B12 levels in many patients [12, 14, 15, 23]. The body’s storage will be depleted much faster in patients using standard MV supplementation with a low dose of vitamin B12. As regards the supplementation regimes with an oral vitamin B12 dosage <350 μg/day, eight of the included studies showed persistence of deficiencies even after a period supplementation of vitamin B12 [6, 9, 11–14, 17, 23]. In one study [6], no dosage of vitamin B12 was measured; in the other studies, the dosage of vitamin B12 was lower than <350 μg/day [9, 11–14, 17, 23]. In two included studies, IM injections belong to the standard MV supplementation regime with a low dose of vitamin B12 [11, 13]. The dose of the IM injections is equal but the frequency of the given IM injections is also different (Table 4). In the study of Aasheim et al. [11], two patients developed vitamin B12 deficiency and in the study of Capoccia et al. [13], vitamin B12 levels decreased in many patients, which suggests that both of this regimens were not optimal.
If MV supplementation with high dose of vitamin B12 may improve the vitamin B12 levels in many patients, IM injections as a standard regime is not necessary and because of this, many patients were unnecessarily loaded with IM injections. This seems like contradictory advice, but to determine whether IM injections of vitamin B12 are necessary, we need to focus on the combination of vitamin B12 and MMA. This is essential to assess whether there is an absolute functional deficiency of vitamin B12, because of the failure rate of the current vitamin B12 assays between 22 and 35% [7, 8, 19, 20] and therefore whether it is necessary to add IM injections to the standard supplementation regime. Besides that, these data are subjective and it is unclear if patients take their supplements daily. Lifelong compliance of daily supplement intake is hard to achieve. To measure adequate intake of MV supplementation, one can monitor the serum concentration of highly absorbable vitamins. Some investigators have reported that low folate levels reflect non-adherence to MV supplementation because the amount of the supplemented folic acid properly corrects low serum folate levels [9, 23]. Only two studies have looked at compliance of MV supplementation intake and distinction in processing these data [14, 23].
Outcomes of Laboratory Tests of Vitamin B12 and MMA
Vitamin B12 assays that are currently used to diagnose clinical vitamin B12 deficiency have a failure rate of 22–35% [7, 8, 19, 20]. This failure rate may be due to the fact that 80% of the vitamin B12 in plasma is bound to the transport protein haptocorrin. This percentage is biologically unavailable and cannot be absorbed by the cells, which means that plasma vitamin B12 concentrations poorly correlate with the bioavailable intracellular vitamin B12 content [8, 21, 22]. Measuring vitamin B12 is a poor predictor for a functional vitamin B12 status. In the study of Smelt et al. [8], more vitamin B12 deficiencies were found when MMA was included in the diagnosis. When a vitamin B12 level is between 140 and 200 pmol/l, additional MMA levels should be measured to determine whether there is functional vitamin B12 deficiency. In this review, no included study used the additional parameter MMA. Given the high failure rate of vitamin B12 assays, many vitamin B12 deficiencies will be untreated.
Study Limitations
First, the following limitations are present when evaluating the literature: (1) heterogeneous patient populations being studied, (2) non-comparable vitamin B12 from supplements being evaluated, (3) lack of many data (some studies lacked of gender, age, reference range of vitamin B12 levels, actual vitamin B12 levels after intervention, lack of dose of vitamin B12 in MV supplementation), and (4) lack of well-designed prospective cohort and randomized controlled studies for the right use of vitamin B12 in postbariatric patients. Secondly, only biochemical data was measured and clinical relevance was not demonstrated.
Conclusion
In bariatric surgery, vitamin B12 deficiencies have a high prevalence. Unfortunately, there is no consensus about MV supplementation and any additional vitamin B12 supplementation. The current literature suggests that 350 μg of oral vitamin B12 is the appropriate oral dose to correct low serum vitamin B12 levels in many patients. A lifelong follow-up regimen seems necessary, because MV supplementation with a high dose of vitamin B12 cannot prevent all deficiencies. Further research must focus on a better diagnosis of vitamin B12 deficiency with possible additional parameters like MMA, the right dose of vitamin B12 supplementation, and the clinical relevance beside biochemical data.
References
Schilling RD, Gohdes PN, Hardie GH. Vitamin B12 deficiency after gastric bypass for obesity. Ann Intern Med. 1984;101:501–2.
Kushner R. Managing the obese patient after bariatric surgery: a case report of severe malnutrition and review of the literature. JPEN J Parenter Enteral Nutr. 2000;24:126–32.
Brolin RE, LaMarca LB, Henler HA, et al. Malabsorptive gastric bypass in patients with super-obesity. J Gastrointest Surg. 2002;6:195–203.
Rhode BM, Arseneau P, Cooper BA, et al. Vitamin B12 deficiency after gastric surgery for obesity. Am J Clin Nutr. 1996;63:103–9.
MacLean LD, Rhode BM, Shizgal HM. Nutrition following gastric operations for morbid obesity. Ann Surg. 1983;198:347–55.
Brolin RE, Gorman JH, Gorman RC, et al. Are vitamin B12 and folate deficiency clinically important after roux-en-y gastric bypass? J Gastrointest Surg. 1998;2(5):436–42.
Sumner AE. Elevated methylmalonic acid and total homocysteine levels show high prevalence of vitamin B12 deficiency after gastric surgery. Ann Intern Med. 1996;124:469–76.
Smelt HJM, Smulders JF, Said M, et al. Improving bariatric patient aftercare outcome by improved detection of a functional vitamin B12 deficiency. Obes Surg. 2015; doi:10.1007/s11695-015-1952-8.
Donadelli SP, Junqueira-Franco MVM, de Mattos Donadelli CA, et al. Daily vitamin supplementation and hypovitaminosis after obesity surgery. Nutr. 2012;28(4):391–6.
Wells G.A., Shea B., O’Conell D., et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomized studies in meta-analysis.
Aasheim ET, Johnson LK, Hofso D, et al. Vitamin status after gastric bypass and lifestyle intervention: a comparative prospective study. Surg Obes Relat Dis. 2012;8(2):169–75.
Rhode BM, Tamin H, Gilfix BM, et al. Treatment of vitamin B12 deficiency after gastric surgery for severe obesity. Obes Surg. 1995;5(2):154–8.
Capoccia D, Coccia F, Paradiso F, et al. Laparoscopic gastric sleeve and micronutrients supplementation: our experience. J of Obes. 2012; doi:10.1155/2012/672162.
Homan J, Schijns W, Aarts EO, et al. An optimized multivitamin supplement lowers the number of vitamin and mineral deficiencies three years after roux-en-y gastric bypass: a cohort study. Surg Obes Rel Dis. 2015; doi:10.1016/j.soard.2015.12.010.
Moore CE, Sherman V. Effectiveness of B vitamin supplementation following bariatric surgery: rapid increases of serum vitamin B12. Obes Surg. 2015;25:694–9.
Altman D. Practical statistics for medical research. Chapman and Hal. London. 1991.
Gasteyger C, Suter M, Gaillard RC, et al. Nutritional deficiencies after roux-en-y gastric bypass for morbid obesity often cannot be prevented by standard multivitamin supplementation. Am J Clin Nutr. 2008;87:1128–33.
de Jesus Ramos NMCP, Magno FCCM, Cohen L, et al. Weight loss and nutritional anemia in patients submitted to roux-en-y gastric bypass on use of vitamin and mineral supplementation. Arq Bras Cir Dig. 2015;28(1):44–7.
Carmel R, Brar S, Agrawal A, et al. Failure of assay to identify low cobalamin concentrations. Clin Chem. 2000;46(12):2017–25.
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367:385–91.
Solomon LR. Disorders of cobalamin metabolism: emerging concepts in pathophysiology, diagnosis and treatment. Blood Rev. 2007;3:113–30.
Hvas AM, Nexo E. Holotranscobalamin: a first choice assay for diagnosing early vitamin B12 deficiency? J Int Med. 2005;257:289–98.
Dogan K., Aarts, E.O., Koehestanie, P. et al. Optimization of vitamin supplementation after roux-en-y gastric bypass surgery can lower postoperative deficiencies: a randomized controlled trial. Medicine. 2014;93(25). doi:10.1097/MD.0000000000000169.
Aills L, Blankenship J, Buffington C, et al. ASMBS allied health nutritional guidelines for surgical weight loss patient. Surg Obes Relat Dis. 2008;4:73–108.
Mechanick J.I., Youdim A., Jones D.B., et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update. Surg Obes Relat Dis. 2013;9(2):159–91.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Author 3 reports educational grants from Medtronic and FitForMe. Author 1 and author 2 have nothing to disclose.
Funding
None.
Ethical Approval
For this type of study, formal consent is not required.
Additional information
Author Contributions
Study design and data collection: HS, SP
Drafting and revision of the manuscript: HS, SP, JS
Final approval: HS, SP, JS
Rights and permissions
About this article

Cite this article
Smelt, H., Pouwels, S. & Smulders, J. Different Supplementation Regimes to Treat Perioperative Vitamin B12 Deficiencies in Bariatric Surgery: a Systematic Review. OBES SURG 27, 254–262 (2017). https://doi.org/10.1007/s11695-016-2449-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2449-9