
Abstract
Background
The report submitted is a detailed analysis of the happenings and outcomes of a two day deliberation that was organized in Trivandrum, India on the 9th and 10th August 2009.
Methods
Asian Consensus Meeting on Metabolic Surgery (ACMOMS) was the first ever meeting of its kind in Asia where 52 professionals involved in the field of bariatric surgery, metabolic surgery, diabetes, and medical research from countries across Asia and the GCC met at Trivandrum, India to vote for and create a new set of guidelines for the Asian genotype, which were different from the NIH guidelines set for bariatric surgery. The aim was to set culturally, geographically, and genetically relevant standards for the management of obesity and metabolic syndrome.
Results
It is known that Asians have a higher adiposity for a given level of obesity, and this is visceral obesity as compared to other populations. Currently, all over the world and in Asia as well, guidelines set by NIH in 1991 are being followed. Surgeons believe that NIH guidelines need to be revisited and modified. It is in light of these observations that the genesis of ACMOMS took place. At ACMOMS, it was recommended that the NIH guidelines are not suitable for Asians, and the BMI guidelines should be lowered for indication of surgery. Waist or waist–hip ratio must gain significance as compared to BMI alone in Asia.
Conclusions
The collective recommendations were submitted as a report to the executive committee for approval. As the Asia Pacific region consists of more than half of the world's population, the dire health and economic consequences of this epidemic demand urgent action from the medical fraternity in this region, and we hope that the recommendations will help to review the currently accepted guidelines.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Genesis of ACMOMS
Fifty-two professionals involved in the field of bariatric, metabolic surgery, diabetes, and medical research from countries across Asia and the GCC met at Trivandrum, India on the 9th and 10th August 2008. All these professionals mainly treat a population that has an Asian genotype. The aim of the meeting was to seek an expert consensus on the use of bariatric surgery or gastrointestinal metabolic surgery for the treatment of obesity and related type II diabetes mellitus [T2DM]. This was the first Asian meeting that brought together bariatric surgeons, endocrinologists, and research professionals on one platform. The meeting started with presentations by investigators from all across Asia. After this, 52 members comprising endocrinologists and bariatric surgeons voted on a host of questions. The collective recommendations were then forwarded to an executive committee (Appendix) comprising Dr. B. Saboo, Dr. H. Frydenburg, Dr. J. Dixon, Dr. M. A. Lakdawala, Dr. P. Chowbey, Dr. R. Hartung, Dr. S. Bandukwala and Dr. W. J. Lee.
This panel has now approved this report as a formal recommendation to be sent out as a collective Voice of Asia. This is an independent report of the panel. It reflects the views of the Asian surgical community based upon presentations and collective discussion at the time of the consensus and is subject to change over a period of time with advent of new concepts that may emerge through medical research. These recommendations have been endorsed by the Asia Pacific Chapter of IFSO and the Asia Pacific Metabolic and Bariatric Surgery Society (APMBSS).
Goals of ACMOMS
-
1.
To set culturally, geographically, and genetically relevant standards for the management of obesity and metabolic syndrome.
-
2.
To identify the usefulness of BMI as a principal criteria for identification of obesity in the Asian population.
-
3.
To identify waist circumference or waist–hip ratio as additional criteria for defining obesity in the Asian population.
-
4.
To set parameters to identify visceral or central obesity versus truncal obesity.
-
5.
To develop recommendations for development of ethical clinical studies for antidiabetes surgery.
Rationale for ACMOMS
Obesity has reached epidemic levels globally along with an alarming rise in the number of people with type 2 diabetes in the world. The number of people with diabetes worldwide is projected to increase from 171 million in 2000 to 366 million by 2030. In developing countries like India and China, this number is expected to increase from 84 million to 228 million by 2030. According to WHO, India and China along with some other southeast Asian countries are at the forefront of this epidemic. Many of those affected are children with potentially devastating repercussions [1].
People in Asia tend to develop diabetes and cardiovascular disease with a lesser degree of obesity, at younger ages, hence, suffer longer with complications of diabetes and cardiovascular disease and thus die sooner than people in other regions.
The dire health and economic consequences of this epidemic demands an urgent action from the Asian medical fraternity.
According to the international classification of WHO people with a BMI >25 are classified as overweight and those with a BMI of >30 are considered to be obese. The cutoff points of 23, 27.5, 32.5, and 37.5 kg/m2 have been added as points for public health action for the Asian population.
It is a well known fact that body fat percentage of the Asian population is much higher as compared to their Caucasian counterparts. Asians are more prone to central obesity as shown by a greater waist circumference and waist–hip ratio. It is also widely acknowledged that the risk for metabolic syndrome starts at a relatively normal level of BMI i.e., at 22 to 23 kg/m2 [2]. As the Asia Pacific population constitutes almost half of the world population, these observations have far-reaching implications. In the wake of these observations, a universal BMI cutoff point based on western criteria for obesity is not appropriate.
In February 2000, the WHO-Western Pacific Region, International Association for the Study of Obesity and International Obesity Task Force published a joint statement and revised the classification of overweight and obesity for people in the Asia Pacific region. They suggested 23 and 25 kg/m2 as the ‘new’ corresponding cutoff levels for overweight and obesity, respectively, in adult Asians. Although most Asian countries are now using these revised cutoff levels as their guide for defining obesity, an international consensus is still lacking. The WHO endorses the rationale for different limits of BMI for the diagnosis of overweight and obesity in Asians for public health action but does not support a change in the current international guidelines.
Asian consensus meeting ACMOMS was organized to review the scientific data relevant to specific geographical and ethnic populations. The reviewed data reinforced that Asians have a higher incidence of health risks at a lower BMI. This called for a revision of the current guidelines for bariatric surgery in the Asian population. It was aimed to redefine cutoff points for BMI, waist circumference and waist to hip ratio.
The rationale of the meeting was to arrive at a consensus wherein guidelines specific to Asia could be formulated and accepted by local societies and associations. We understand that lowering the BMI cutoffs for surgery will lead to a significant rise in the percentage of obese population eligible for surgery, which will in turn have an enormous impact on the public health policies of individual countries. We hope to include almost 15% of the Asian population in the 23 to 25 kg/m2 BMI group at risk for metabolic syndrome but who are currently being denied the health benefit. We also hope that this will trigger policy action and lead to more stress on “prevention” of childhood as well as adult obesity.
The WHO defines obesity as a condition of excessive fat accumulation to the extent that health and well-being are affected. Obesity has been cited as a risk factor for many non communicable diseases. The obese have a higher propensity to develop T2DM, metabolic syndrome, dyslipidemia, gall bladder disease, and sleep apnea. It is also associated with a moderate risk of coronary heart disease, hypertension, osteoarthritis, and gout. Certain cancers, PCOD, and infertility are also associated with obesity.
Obesity is characterized by an excess body fat (BF), which is defined conventionally as BF >25% in males and >35% in females [3]. The BMI is normally used as a measure of obesity. The use of BMI is justified as the BMI correlates well with BF% and is hardly dependent on height.
In 1993, a WHO expert meeting proposed the following BMI cutoff points: 25.0–29.9 kg/m2 for overweight, 30–34.9 kg/m2 for grade 1 obesity, 35 to 39.9 kg/m2 for grade 2 obesity, and more than 40 as grade 3 obesity [3]. These cutoff points were based on observational studies in Europe and USA on the relationship between morbidity and mortality with BMI.
In the recent years, Asia has seen an unprecedented economic growth. Increase in the spending power of the consumer has led to a marked shift in lifestyle. Along with this affluence, the population has become more susceptible to obesity, which in turn has led to an increase in the incidence of non communicable diseases like T2DM and coronary heart disease. In 1997, Amos et al. estimated the total number of Asians suffering from T2DM to be around 30 million out of a total of 120 million diabetics in the world. It has been predicted that by 2010, the number of people with diabetes in Asia Pacific region would rise to 130 million out of a total of 236 million worldwide [4]. This would constitute more than half of the world's diabetic burden.
As per the WHO criteria, the prevalence of obesity in Asia Pacific region is less than the western countries. Recent studies have shown that health risks associated with obesity have been seen to occur at BMI as low as 22 to 23 kg/m2 in some Asian populations [2]. This implies that obesity associated health risks tend to occur at much lower threshold of BMI is Asians.
A study done by Deurenberg et al. in the year 2000 compared the relationship between body fat percentage and body mass index in three different ethnic groups in Singapore [5]. It showed that the body fat percentage in all three ethnic groups (Chinese, Malay, and Indians) was under predicted by BMI when an equation set in western population was used. The study revealed that the relationship between body fat percentage and BMI is different between Singaporeans and Caucasians as well as among the three ethnic populations. The study also suggested that if obesity is defined by body fat content and not by BMI then threshold for BMI to define obesity needs to be lowered. Most of the equations developed to calculate body fat from weight and stature have been developed in the Caucasian population.
Wang et al. demonstrated many errors when these equations are applied to Asian population, thus implying that there may be some other factors to play [6]. They observed a higher fat percentage and thicker subcutaneous fat in Asians for a given BMI. Their study also highlighted a need for race specificity in methods for estimating body composition by anthropometric measures.
In 2003, Chang et al. did a cross-sectional epidemiological survey in the Taiwanese subjects to compare the correlations of BMI and BF% with other ethnic groups [7]. They demonstrated that Taiwanese subjects have higher BF% compared to Caucasians. In their study, they reported that although by WHO standards prevalence of obesity was only 3.9% in Taiwanese population, the prevalence of diabetes and cardiovascular diseases was almost the same as western countries. Thus, suggesting that Asians may have lower BMI but higher visceral adiposity as compared to Caucasians.
BMI has the advantage of being an easy method to calculate the index of obesity though as seen in the studies cited above it is not necessarily the most accurate method. Body composition instead of body size is a more appropriate measure for obesity, thus once again emphasizing that a universal cutoff for BMI irrespective of differences in ethnicity is incorrect.
French physician Jean Vague was the first to suggest that ‘apples suffer more than pears’. He suggested that the cardiovascular and metabolic risk was higher in women with android obesity as compared to those with gynoid obesity [8]. Excess abdominal fat is an independent predictor of risk factors and morbidity of obesity-related diseases like type 2 diabetes, hypertension, hyperlipidemia, and other components of the metabolic syndrome. Asian Indians have an increased predisposition to diabetes [9] and coronary artery disease [10].
In 1991, Mc Keique et al. did a population survey in London, UK. The sample consisted of 3,193 men and 561 women aged 40 to 69 years [11]. It was observed that as compared to the European group, the South Asian group had a higher prevalence of diabetes, hypertension, and hypercholesterolemia. Mean waist to hip ratio was higher in the South Asian group suggesting a pronounced tendency to central obesity and thus corroborating the existence of an insulin resistance syndrome. This predisposition has been attributed to the ‘Asian Indian Phenotype’ [12] which is characterized by greater central body obesity as measured by greater waist circumference and waist to hip ratios. Thus, many Asians do not classify as obese by the WHO criteria calculated on the basis of BMI but can be considered metabolically obese.
The INTERHEART study also predicted that waist to hip ratio was a better predictor of cardiovascular events than BMI [13]. It also showed that the ‘hip’ is an independent ‘protective’ factor. Thus, increasing the significance of the waist to hip ratio where the numerator forms a risk factor and the denominator is a protective factor. Therefore, it suggested that the waist to hip ratio is a better predictor than waist alone.
Shelgikar et al. conducted a study in Pune and studied the relationship between BMI and WHR with plasma glucose concentrations in an oral glucose tolerance test (OGTT) [14]. On multivariate analysis, fasting as well as 2-h plasma glucose concentrations during OGTT were found to be related to waist–hip ratio (p less than 0.01) and subscapular fat thickness (p less than 0.01) but not to body mass index (or triceps fat thickness). Thus, suggesting that in native Indians, central obesity seems to be a more important association of hyperglycemia than generalized obesity.
Many theories have been put forth by various investigators to explain the higher adiposity levels in Asian population. Yajnik et al. suggested a possible genetic predisposition to increased adiposity in ‘thin’ Indians [15]. They also suggested that low birth weight babies had a higher chance of obesity in later life. They have shown that low birth weight babies had low muscle and visceral mass but a higher adiposity level as compared to their Caucasian counterparts. This body composition is influenced by maternal adiposity before pregnancy and by aspects of maternal nutritional intake and circulating nutrient concentrations during pregnancy. There are no strong paternal determinants of adiposity at birth. These babies were followed up over a period of 8 years at KEM Hospital, Pune. It was reported that those with a lower birth weight exhibited more insulin resistance at the end of 8 years [16]. Susceptibility to diabetes in the Asian population can also be attributed to the “thrifty” genotype, which enhanced survival in subsistence conditions of the past but is detrimental in the times of surplus such as now. It is much less of an asset in these times of abundance as compared to the days of less food and more physical work [17].
A direct implication of the above arguments is that developing countries like those in South East Asia will have a younger population afflicted with diabetes as compared to the developed countries. The complications associated with diabetes, like retinopathy, neuropathy, nephropathy, diabetic foot, etc. will also set in at an earlier age. This implies that the disease will affect the most productive age group of society. It has been estimated that by 2025, the Asia Pacific region will have more than half of the world's diabetic population. Countries like India and China put together will have more individuals with diabetes than the rest of the world. Considering their large populations and lacking healthcare systems, it will not be unrealistic to say that the most deprived sections of the society will be worst hit by this epidemic. The far-reaching consequences in terms of health and economic losses warrant an immediate action from the medical fraternity in this region and world over.
BMI cutoff points have been used to trigger policy actions, facilitate prevention programs, and to measure the effect of interventions. They have also been used to identify candidates for screening and decide treatment modalities [18]. That BMI underestimates obesity in Asians is an established fact now. The current cutoff of 25 kg/m2 is not an adequate basis for defining the high risk group susceptible to the comorbidities of obesity.
In 2007, Gupta et al. concluded in their study that there is a continuous positive relationship of all markers of obesity (BMI, waist and waist hip ratio) with hypertension, diabetes, and metabolic syndrome. Waist–hip ratio also correlated with lipid abnormalities [19]. They showed that WHR >0.9 in men and >0.8 in women is associated with a significant increase in multiple risk factors. It was the first Indian study where the importance of waist size as a marker of cardiovascular risk factor was evaluated. There was also a significant increase in prevalence of hypertension, diabetes, and metabolic syndrome at waist size >90 cm in men and >80 cm in women. These levels were lower than those suggested by the US National Cholesterol Education Program (ATP-III) 10 where the cutoff levels were >102 cm for men and >88 cm for women [20].
Thus, it is clear that the quest for an optimal method to define obesity leads us to a combination of BMI, waist, and waist–hip ratio. In the Asian setting, none of these parameters in isolation can be considered as an adequate measure of obesity.
Risk associated with obesity can best be defined when all three parameters are used in conjunction; however, it is important to standardize the method of calculating each of them.
Measurement of BMI is relatively free of mathematical errors as it can be calculated by taking the height and weight (weight in kg/height in meter2) of a person. It correlates well with body fat percentage and is easy to calculate. Other methods of calculating the body fat percentage require sophisticated equipment and techniques and cannot be used in a wider setting. Due to its wider applicability, it has been used as a measure for body fat percentage in most studies. BMI also has its demerits, as sometimes in very short and very tall subjects, it can miscalculate the body fat percentage as also in Asians with predominant central obesity. It is also not very useful as a measure of childhood obesity as children are in the growth phase.
A CT or MRI scan at L3/L4 level provides an accurate measurement of visceral fat. It is costly and difficult to use them as a screening measure and thus reduce their applicability in the wider clinical settings. Waist circumference and waist to hip ratio are used as simpler measures of visceral obesity. However, it is extremely important to standardize the technique of measurement in terms of the anatomical landmarks. The WHO (1995) recommended methods as follows. For waist or abdominal circumference, the subject stands with feet 25–30 cm apart, weight evenly distributed. Measurement is taken midway between the inferior margin of the last rib and the crest of the ileum in a horizontal plane. The measurer sits by the side of the subject and fits the tape snugly but not compressing soft tissues. Circumference is measured to the nearest 0.1 cm. For hip circumference, the measure is taken around the pelvis at the point of maximal protrusion of the buttocks.
Treatment options for obesity include diet, pharmacological therapy, and behavioral changes. All these options have shown poor long-term results in the treatment of morbid obesity [21]. Bariatric surgery is the only proven method effective in maintaining long-term weight loss [22]. So, should we offer surgical treatment to patients below BMI 35 who also have type 2 diabetes mellitus or other components of the metabolic syndrome?
In diabetic patients, control of blood sugar depends on patient compliance to the treatment, which can be quite challenging at times. Efficacy of various diets and weight control plans has been questioned time and again. Oral hypoglycemic agents also have long-term side effects. It has been observed that blood glucose control eventually deteriorates over time.
In the Asian setting, the increased cost for maintaining control with intensive medical management is one of the factors that deter the patient from achieving the goal of sustained euglycemia. A complex disease such as diabetes impacts many other related and unrelated health problems and the resources used in their treatment. In 2003, the American Diabetes Association described the direct medical costs associated with treatment of diabetes and its complications. According to this paper, the median annual direct medical costs for subjects with diet-controlled type 2 diabetes, BMI 30 kg/m2, and no microvascular, neuropathic, or cardiovascular complications were $1,700 for white men and $2,100 for white women. A 10-kg/m2 increase in BMI, treatment with oral antidiabetic or antihypertensive agents, diabetic kidney disease, cerebrovascular disease, and peripheral vascular disease were each associated with 10–30% increases in cost. Insulin treatment, angina, and MI were each associated with 60–90% increases in cost. Dialysis was associated with an 11-fold increase in cost [23]. The onetime cost of bariatric surgery in Asian countries ranges from $8,000 to $11,000. When we compare this to the recurring annual cost of medical treatment, surgery is definitely a more economical option.
A few studies conducted in low BMI subjects with type 2 diabetes mellitus or other components of the metabolic syndrome suggest good results. In a study conducted in Brazil, Cohen et al. reported a 100% resolution of T2DM in their series of 37 patients with BMI from 30 to 35 [24]. All patients had undergone laparoscopic RYGB in their series. None of the patients needed antidiabetic therapy postoperatively. The duration of diabetes was less than 10 years in all patients in their series. Only one of the patients in their series continued to be on a mild dose of antihypertensives in their study.
Mingrone et al. reported a case of a young diabetic woman of normal weight who underwent biliopancreatic diversion for chylomicronemia and whose plasma insulin and blood glucose levels were normalized within 3 months, even though she gained weight due to an unrestricted diet rich in sugar and lipids [25]. Noya et al. reported remission of T2DM in 9 of 10 moderately obese (mean BMI, 33.2) diabetic patients undergoing BPD [26].
In a landmark paper in 2006, O'Brien and Dixon et al. showed that in mildly to moderately obese patients (BMI, 30 to 35 kg/m2), laparoscopic adjustable gastric banding is a safe and effective procedure to achieve weight loss, for the resolution of metabolic syndrome, and improving the quality of life. They reported a 97.3% resolution in metabolic syndrome postoperatively [27]. They showed that quality of life improved statistically significantly in the operated group as compared to the non-operated group. In 2007, results of laparoscopic sleeve gastrectomy in morbidly obese Korean patients were published. In this paper, 100% resolution of diabetes was reported at the end of 6 months along with improvement in other comorbidities [28].
Dr W.J. Lee from Taiwan has also reported similarly good resolution of T2DM in patients with BMI between 30 and 35 kg/m2 with a mini-gastric bypass. He reported significant and sustained weight loss with successful treatment of T2DM up to 87.1% [29]
Despite these advances in and gastrointestinal metabolic surgery and such good resolution of T2DM, it is still not considered as a treatment option for T2DM in major reviews of therapy [30].
The risk of surgery seems miniscule when it is weighed against the risk of uncontrolled diabetes that leads to complications like nephropathy, retinopathy, cardiovascular problems, and amputations in the long term. Additional studies are needed to determine the best surgical procedure for obese patients in Asia. There is a need for more randomized controlled trials weighing the benefits of surgery in this subgroup versus best medical treatment.
Defining terms
“Bariatric surgery vs. gastrointestinal metabolic surgery”: Some preferred the use of the term bariatric surgery as the accepted norm. But on referring to the terminology used at the Rome Diabetes Surgery summit, it was concluded that all questions pertaining to BMI above 35, be referred to as bariatric surgery and below 35 as GI metabolic surgery.
“Appropriate suitable candidates”: This was added to validate the reality that for certain patients, major surgery of any type is out of question.
“Inadequately controlled by life style and medical therapy”: It was decided not to elaborate what this meant at the present juncture. It was pointed out that control was different from severity.
Asian consensus meeting on metabolic surgery: results
At the end of the meeting, a series of questions were posed to the participants. The questions were put up on the screen as a template with three options in most cases.
Yes, no, or undecided. All members were given individual voting meters. All the answers were put up at the end of the voting to avoid bias in answering the next question. The voting members were given 1min to vote per question. There were 52 voting members per question. The final voting result is mentioned below.
-
1.
Bariatric surgery is the indicated treatment option for control of obesity in appropriate surgical candidates who have failed conservative non-surgical attempts at weight loss for BMI >35?
Yes, 98%; No, 0%; Undecided, 2%
-
2.
Bariatric surgery is the indicated treatment option for Type 2 DM in appropriate surgical candidates with BMI >35?
Yes, 92.16%; No, 5.88%; Undecided, 1.96%
-
3.
Gastrointestinal metabolic surgery is the indicated treatment for Type 2 DM in appropriate surgical candidates who are inadequately controlled by lifestyle and medical therapy in BMI 30 to 35?
Yes, 81.48%; No, 11.11%; Undecided, 7.41%
-
4.
Gastrointestinal metabolic surgery is the appropriate surgery for T2DM in those patients with BMI 30 to 35 who are controlled by medical therapy?
Yes, 55.20%; No, 36.80%; Undecided, 8%
-
5.
Gastrointestinal metabolic surgery is the indicated treatment option for those candidates who are inadequately controlled by lifestyle and medical management for their dyslipidemia and hypertension with BMI 30 to 35?
Yes, 50.94%; No, 41.51%; Undecided, 7.55%
-
6.
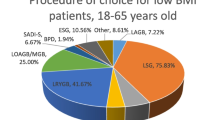
In Asians with Class I obesity with BMI 27.5 to 30 in conjunction with waist >80 cm in females and >90 cm in males; would you recommend Gastrointestinal Metabolic surgery?
Yes, 66.67%; No, 18.52%; Undecided, 14.81%
-
7.
If you do recommend surgery, then should it be done as a research project?
Yes, 68.18%; No, 31.82%
-
8.
Would you operate for T2DM inadequately controlled by lifestyle and medical therapy in BMI <27.5?
Yes, 28.3%; No, 58.49%; Undecided, 13.21%
-
9.
Should research be carried out only by high volume centers [i.e., more than 100 bariatric cases per year] with results closely monitored by an external agency and a centralized data collection agency?
Yes, 62.26%; No, 33.96%; Undecided, 3.77%
-
10.
Do you think there is need for more randomized clinical trials comparing best medical management vs. surgery for Type 2 DM in BMI <30?
Yes, 86.96%; No, 2.17%; Undecided, 10.87%
-
11.
Significance of BMI, 18.87%; BMI waist, 32.08%; BMI (waist:hip ratio), 47.17%; waist, 1.89%
Summary of Voting Results
The voting results reflect the gradual change in the thought process of the Asian surgical community. A positive response of more than two thirds of the voting majority was considered as approved. Most surgeons believe that the NIH guidelines are not good enough for the Asia Pacific region. For the Asian patients, BMI criteria must be lowered to 35 kg/m2 for the indication of bariatric surgery. Most surgeons consider T2DM as a more severe comorbidity as compared to hypertension or dyslipidemia. The voting results also reflect that the waist circumference or waist hip ratio must be given more significance for defining obesity along with BMI in Asia. Hence, guidelines for bariatric/gastrointestinal metabolic surgery in Asia must also recognize the importance of waist circumference and waist hip ratio along with BMI. All the participants agreed on the need for more randomized controlled clinical trials comparing best medical management with surgery for diabetic patients with BMI less than 30 kg/m2.
Recommendations
-
1.
Bariatric/gastrointestinal metabolic surgery should be considered as a treatment option for obesity in people with Asian ethnicity with BMI more than 35 kg/m2 with or without comorbidities.
-
2.
Bariatric/gastrointestinal metabolic surgery should be considered as a treatment option for obesity in people with Asian ethnicity above a BMI of 32 kg/m2 with comorbidities.
-
3.
Bariatric/gastrointestinal metabolic surgery should be considered as a treatment option for obesity in people with Asian ethnicity above a BMI of 30 kg/m2 if they have central obesity (waist circumference more than 80 cm in females and more than 90 cm in males) along with at least two of the additional criteria for metabolic syndrome: raised triglycerides, reduced HDL cholesterol levels, high blood pressure and raised fasting plasma glucose levels.
-
4.
Any surgery done on diabetic patients with a BMI less than 30 kg/m2 should be strictly done only under study protocol with an informed consent from the patient. The nature of these surgeries should be considered as yet purely experimental only as part of research projects with prior approval of the ethics committee.
References
Hossain P, Kawar B, El Nahas M. Obesity and diabetes in the developing world—a growing challenge. N Engl J Med. 2007;356:3.
Ko GTC, Tang JSF. Waist circumference and BMI cut-off based on 10-year cardiovascular risk: evidence for central pre-obesity. Obesity. 2007;15(11):2832–40.
World Health Organisation. Physical status: the use and interpretation of anthropometry. Technical Report Series 854, Geneva; 1995.
Amos A, McCarty D, Zimmet P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabetic Med. 1997;14 Suppl 5:S1–S85.
Deurenberg-Yap M, Schmidt G, van Staveren WA, et al. The paradox of low body mass index and high body fat percentage among Chinese, Malays and Indians in Singapore. Int J Obese Relat Metab Disord. 2000;24(8):1011–7.
Wang J, Thornton JC, Russell M, et al. Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr. 1994;60:23–8.
Chang C-J, Wu C-H, Chang C-S, et al. Low body mass index but high percent body fat in Taiwanese subjects: implications of obesity cutoffs. Int J Obes. 2003;27:253–9.
Vague J. Sexual differentiation, a factor affecting the forms of obesity. Presse Med. 1947;30:339–40.
Wild S, Roglic G, Green A, et al. Global prevalence of diabetes, estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53.
Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in developing countries. Circulation. 1998;97:596–601.
McKeigue PM, Shah B, Marmot MG. Relation of central obesity and insulin resistance with high diabetes prevalence and cardiovascular risk in South Asians. Lancet. 1991;337(8747):971–3.
Joshi R. Metabolic syndrome—emerging clusters of the Indian phenotype. J Assoc Physicians India. 2003;51:445–6.
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries [the INTERHEART study]: case-control study. Lancet. 2004;364(9438):937–52.
Shelgikar KM, Hockaday TD, Yajnik CS. Central rather than generalized obesity is related to hyperglycaemia in Asian Indian subjects. Diabet Med. 1991;8:712–7.
Yajnik CS. Obesity epidemic in India: intrauterine origins? Proc Nutr Soc. 2004;63:387–96.
Bavdekar A, Yajnik CS, Fall CHD, et al. The insulin resistance syndrome [IRS] in eight-year old Indian children: small at birth, big at 8 years or both? Diabetes. 2000;48:2422–9.
Neel JV. Diabetes mellitus: a ‘thrifty’ genotype rendered detrimental by ‘progress’? Am J Hum Genet. 1962;14:353–62.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63.
Gupta R, Rastogi P, Sarna M, et al. Body-mass index, waist-size, waist–hip ratio and cardiovascular risk factors in urban subjects. J Assoc Physicians India. 2007;55:621–7. www.japi.org.
National Cholesterol Education Program. Third report of the National Cholesterol Education Program Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel-III). Circulation. 2002;106:3143–421.
Goldstein DJ. Beneficial health effects of modest weight loss. Int J Obes. 1992;16:397–415.
National Institutes of Health. Gastrointestinal surgery for severe obesity: national institutes of health consensus conference statement. Am J Clin Nutr. 1992;55:6159.
Brandle M, Zhou H, Smith BRK, et al. The direct medical cost of type 2 diabetes. Diabetes Care. 2003;26:2300–4.
Cohen R, Pinheiro J, Correa J, et al. Laparoscopic Roux en-y gastric bypass for BMI less than 35 kg/m2: a tailored approach. Surg Obes Relat Dis. 2006;2(3):401–4
Mingrone G, De Gaetano A, Greco AV, et al. Reversibility of insulin resistance in obese diabetic patients: role of plasma lipids. Diabetologia. 1997;40:599–605.
Noya G, Cossu ML, Coppola M, et al. Biliopancreatic diversion preserving the stomach and pylorus in the treatment of hypercholesterolemia and diabetes type II: results in the first 10 cases. Obes Surg. 1998;8:67–72.
O’brien P, Dixon JB, Laurie C, et al. Treatment of mild to moderate obesity with laparoscopic adjustable Gastric banding or an intensive medical program a randomized trial. Ann Intern Med. 2006;144:625–33.
Han SM, Kim WW, Hyun Oh J. Results of laparoscopic sleeve gastrectomy (LSG) at 1 year in morbidly obese Korean patients. Obes Surg. Online publication.
Lee WJ, Wang W, Lee YC, et al. Effect of laparoscopic mini-gastric bypass for T2DMMellitus: comparison of BMI >35 and <35 kg/m2. J Gastrointest Surg. 2008;12:945–52.
American Diabetes Association. Standards of medical care in diabetes—2008. Diabetes Care. 2008;31(1):S12–54.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Executive Committee Members
Chair: Dr. Bansi Saboo, Endocrinologist, Hon Secretary RSSDI, Gujarat, India; Dr. Harry Frydenberg, Bariatric Surgeon, Epsworth Training Center, President: International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO), Melbourne, Australia; Dr. John Dixon, Head of Clinical Research, Centre for Obesity Research and Education and Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, Australia; Dr. M. A. Lakdawala, Bariatric Surgeon, Chief: Department of Minimal Access Surgery, Saifee Hospital, Mumbai, Founder, Centre of Obesity & Diabetes Support, Vice President: Obesity and Metabolic Surgery Society of India [OSSI], Mumbai, India; Dr. Pradeep Chowbey, Bariatric Surgeon, President Elect: IFSO APC, Governor, Society of Endoscopic and Laparoscopic Surgeons of Asia (ELSA), Chairman, Minimal access, Metabolic and Bariatric Surgery Centre, Sir Gangaram Hospital, New Delhi, India; Dr. Rolf Hartung, Consultant Surgeon, Head of General Surgery, Dubai Hospital, Government of Dubai and Associate Professor of Surgery, Dubai Medical College, Dubai; Dr. S. Bandukwala, Physician, Saifee Hospital, Lilavati Hospital, Mumbai, India; Dr. S. Joshi, Endocrinologist; Lilavati Hospital, Vice President RSSDI, President Elect AAIRO, Mumbai, India; Dr. W.J. Lee, Bariatric Surgeon, President: Asia Pacific Bariatric Surgery Society (APBSS), Director, Asia Pacific Endoscopy Bariatric Surgical Center, Professor of Surgery, National Taiwan University, Chairman, Asia Pacific Bariatric Surgical Group, President, Taiwan Association for Endoscopic Surgery, Taiwan.
Speakers at the Summit
Organizer and Convenor: Dr. M. A. Lakdawala, Bariatric Surgeon, Chief: Department of Minimal Access Surgery, Saifee Hospital, Mumbai, Founder, Centre of Obesity & Diabetes Support, Vice President: Obesity and Metabolic Surgery Society of India [OSSI], Mumbai, India.
Co-Convenor: Dr. Pradeep Chowbey, Bariatric Surgeon, President Elect: IFSO APC, Governor, Society of Endoscopic and Laparoscopic Surgeons of Asia [ELSA], Chairman, Minimal access, Metabolic and Bariatric Surgery Centre, Sir Gangaram Hospital, New Delhi, India
Keynote speakers: All the members of the executive committee were speakers at the summit. Dr. Ashok Damodaran, MS, DNB, Pakar Perunding Bedah, Hospital Sebu, Malaysia; Dr. Anton Cheng, FRCS (Ed), FRACS, Senior Consultant, Department of surgery, Alexandra Hospital, Singapore; Dr. Hildegardes C. Dineros, Bariatric and metabolic surgeon, Healing hand clinic and St. Luke’s Medical center, Philippines; Dr. Prashant Mathur, DCH, DNB, PhD, MNAMS, Assistant Director General, Division of non communicable diseases, Indian council of medical research, New Delhi, India; Dr. Faruq Badiuddin, MS, FRCS, Consultant Surgeon, Wellness medical center, Rosary medical center, Village medicenter, Dubai; Dr. Wilfred Lik Man Mui,MBChB, FRCS (Ed), FRACS, Union Hospital, Hongkong; Dr. Chih-Kun Huang, Chief- International Endoscopic Obesity Center, E-Da Hospital and I- Shou University, Taiwan; Dr. Sang Moon Han, MD, Assistant Professor, Department of surgery, College of medicine, Pochon, CHA University-CHA General Hospital, Korea; Prof. Paisal Pongchairerks, MD, FICS, FRCS,Thai board of general Surgery, Thailand; Dr. Mahendra Narwaria, MS, Asian institute of gastroenterology surgery, President- Obesity and metabolic surgery society of India; Dr. Ramen Goel, MS, Wockhardt hospital and Bombay hospital, India; Dr. Surendra Ugale, MS, Kirloskar hospital, Hyderabad, India; Dr. S. Sheikh, MD, Consultant endocrinologist, Saifee hospital, Mumbai, India; Dr. S. Goel, MD, Consultant anesthetist, Saifee Hospital, Center for Obesity and Diabetes Support, Mumbai, India.
Summit Organizing Committee
Dr. Yasin Kazi, MS, Consultant surgeon, Center for Obesity and Diabetes Support, Mumbai, India; Dr. Aparna Govil Bhasker, Consultant surgeon, Center for Obesity and Diabetes Support, Mumbai, India; Payal Batra, Consultant nutritionist, Center for Obesity and Diabetes Support, Mumbai, India; Sneha Jain, Consultant nutritionist, Center for Obesity and Diabetes Support, Mumbai, India.
Rights and permissions
About this article
Cite this article
Lakdawala, M., Bhasker, A. Report: Asian Consensus Meeting on Metabolic Surgery. Recommendations for the use of Bariatric and Gastrointestinal Metabolic Surgery for Treatment of Obesity and Type II Diabetes Mellitus in the Asian Population. OBES SURG 20, 929–936 (2010). https://doi.org/10.1007/s11695-010-0162-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-010-0162-7