
Abstract
Internet Gaming Disorder (IGD) among adolescents has become an important public concern and gained more and more attention internationally. Recent studies focused on IGD and revealed brain abnormalities in the IGD group, especially the prefrontal cortex (PFC). However, the role of PFC-striatal circuits in pathology of IGD remains unknown. Twenty-five adolescents with IGD and 21 age- and gender-matched healthy controls were recruited in our study. Voxel-based morphometric (VBM) and functional connectivity analysis were employed to investigate the abnormal structural and resting-state properties of several frontal regions in individuals with online gaming addiction. Relative to healthy comparison subjects, IGD subjects showed significant decreased gray matter volume in PFC regions including the bilateral dorsolateral prefrontal cortex (DLPFC), orbitofrontal cortex (OFC), anterior cingulate cortex (ACC) and the right supplementary motor area (SMA) after controlling for age and gender effects. We chose these regions as the seeding areas for the resting-state analysis and found that IGD subjects showed decreased functional connectivity between several cortical regions and our seeds, including the insula, and temporal and occipital cortices. Moreover, significant decreased functional connectivity between some important subcortical regions, i.e., dorsal striatum, pallidum, and thalamus, and our seeds were found in the IGD group and some of those changes were associated with the severity of IGD. Our results revealed the involvement of several PFC regions and related PFC-striatal circuits in the process of IGD and suggested IGD may share similar neural mechanisms with substance dependence at the circuit level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Internet gaming disorder (IGD), defined as a compulsive-impulsive internet use disorder, has quickly increased in prevalence all over the world (Young 1998b), especially among adolescents (Bremer 2005). Adolescence, as a developmental stage, seems more vulnerable to IGD because of the immature cognitive control during this period (Pine et al. 2001; Silveri et al. 2004; Steinberg 2005). Adolescents with IGD were likely to have concurrent psychological disorders and executive deficits that would seriously affect their daily life (Romano et al. 2013; Zhou et al. 2012). IGD among adolescents has become an important public concern in many areas, e.g., Asia, Europe and USA (Cao et al. 2011; Dimitri et al. 2011; Durkee et al. 2012). It has drawn neuroimaging researchers’ attention around the world. However, due to the lack of enough comprehensive findings, the neural mechanism underlying IGD is still not clear and little is known about the treatment of IGD (Winkler et al. 2013).
In the past few decades, neuroimaging studies focused on IGD and have shown some common abnormalities in the IGD group by different methods (Ko et al. 2011; Hong et al. 2013; Lin et al. 2012; Yuan et al. 2013a; Yuan et al. 2011; Zhou et al. 2012; Kim et al. 2011). Using functional imaging, Ko et al. detected neural activation of several regions including the bilateral dorsolateral prefrontal cortex (DLPFC) and right anterior cingulate cortex (ACC) which underlie the craving experienced by exposing addicted people to gaming-related cues (Ko et al. 2011). Reduced resting state functional connectivity in cortico-subcortical circuits (24 % with the prefrontal) were observed in the IGD group by using the network-based statistical analysis (Hong et al. 2013). Interestingly, similar regions have also been detected in some morphology studies (Yuan et al. 2011, 2013a; Lin et al. 2012). In detail, reduced gray matter volume of DLPFC, orbitofrontal cortex (OFC) and ACC, together with thinner cortical thickness of OFC, had been revealed in IGD. Employing a tract-based spatial statistics (TBSS) analysis, significant reductions of fraction anisotropy (FA) in major white matter pathways, including orbito-frontal white matter and inferior fronto-occipital had been demonstrated in the IGD group (Lin et al. 2012). Furthermore, in a previous study, we also reported significant gray matter deficits in the bilateral DLPFC, supplementary motor area (SMA), OFC, and the left rostral ACC (rACC) in the IGD group and linked cognitive control deficits to the pathological features and behavioral impairments (Yuan et al. 2011). In conclusion, all studies mentioned above lead us to an important region, i.e., the frontal cortex, especially the prefrontal cortex (PFC), which may be implicated in the underlying pathology of IGD.
The PFC is connected to several subcortical regions and plays an important role in regulation of reward systems (Volkow et al. 2009). What’s more, its involvement in inhibitory control is regarded as a key role in drug seeking behaviors (Feil et al. 2010). Projections from several PFC regions such as the ACC, OFC and DLPFC to the striatum, passing through the pallidum and thalamus, constitute the prefrontal-striatal circuits, which are related to cognitive inhibitory control and stimulus–response habits (Volkow et al. 2013; Kober et al. 2010). Dysfunction of these circuits may be a possible underlying mechanism of addicted behaviors such as impaired inhibition-control and compulsive use despite the negative outcomes, which have been reported in subjects with IGD (Dong et al. 2010; Young 1998b). In addition, the PFC is connected to some resting state networks, including the dorsal attention networks and the default mode network, which is associated with cognitive control and working memory processes (Goldstein and Volkow 2011) that are impaired in subjects with IGD (Romano et al. 2013). Considered as a behavior addiction, IGD is similar to substance addictions in many domains (Grant et al. 2010), even the underlying neurobiological mechanisms (Winkler et al. 2013; Ko et al. 2012; Kim et al. 2011). Therefore, exploring the structural alteration of the PFC regions and their functional connectivity changes may be an entry point to reveal the potential pathology of IGD and act as a guide to its treatment.
Resting-state functional MRI (fMRI) is a noninvasive imaging method, which reflects spontaneous brain activity by detecting low frequency fluctuations in blood oxygen level-dependent (BOLD) signals (Fox and Raichle 2007). At the resting state, functionally related classes of cortical and subcortical regions, which have correlated spontaneous fluctuations, consist of the human brain’s intrinsic functional networks (Seeley et al. 2009). The resting-state method has been widely used to detect the intrinsic functional architecture of the brain (Jin et al. 2013) and has been extensively employed in studies of several serious diseases, such as migraine (Xue et al. 2012; Yu et al. 2012), schizophrenia (Meda et al. 2012), Alzheimer’s disease (Brier et al. 2012) and heroin addiction (Yuan et al. 2010a, b). What’s more, abnormal resting-state functional connectivity within frontostriatal circuits has already been detected to predict disease severity and treatment outcomes in substance abusers (Yuan et al. 2010a; Zhang et al. 2011). Decreased frontostriatal circuits resting state functional connectivity was correlated with the duration of heroin addiction (Yuan et al. 2010a) and the Fagerström Test of Nicotine Dependence (FTND) in smokers (Zhang et al. 2011). Therefore, neuronal activity changes during the resting state may be a biomarker to reveal the progress of IGD. Although several studies had pointed out the resting state functional connectivity abnormalities in IGD, few studies focused on the relationship between the PFC resting state patterns with internet activities.
In the present study, we used a larger sample size to improve the effectiveness of the results and focused on three purposes as follows: 1) to identify frontal regions, especially PFC regions with gray matter changes in the IGD group by VBM analysis; 2) to detect abnormal resting-state functional connectivity of those regions with structural abnormalities; and 3) to investigate associations between abnormal resting-state functional connectivity and some clinical symptoms. By combining structural and functional methods, we aimed to explore the possible role of the PFC in IGD.
Methods
Ethics statement
All procedures were approved by the Ethical Committee of Xi’an Jiaotong University and were conducted in accordance with the Declaration of Helsinki. All participants and their parents gave written informed consent.
Subjects
The IGD participants were asked to satisfy the diagnostic criteria of IGD in DSM-5 (5), i.e., to be diagnosed with IGD a person has to endorse at least five (or more) of the nine criteria over a 12-month period. Additionally, according to the estimation of Young’s online internet addiction test (IAT) (Young 1998a), which was a modification of the earlier 8 item scale, and it had been proven as a valid implement for assessing Internet addiction (Jelenchick et al. 2012; Barke et al. 2012). It consists of 20 questions that are associated with personal internet use and measures the degree to which the internet affects one’s daily life ranging from a 1 (Rarely) to 5 (always) response or 0 (never) to each question. Individuals who scored more than 50 points were considered to be troubled with problematic internet use. In the present study, adolescents who met the DSM-5 IGD criteria and scored more than 50 points in the IAT were selected into the IGD group. Finally, twenty five freshman and sophomore college students with internet addiction and twenty one age, gender, and years of education matched students were recruited in our study (Table 1). All of them participated in online games such as “League of Legends” as their major online behavior. We chose the individuals with proper internet use and scored 20 to 30 points in the IAT as the control group (Xing et al. 2014). For each individual, a questionnaire was designed to assess Internet gaming activities, including ‘How many internet games do you play?’, ‘How many hours on average do you spend on Internet gaming per day?’, ‘How many days on average do you spend on Internet gaming per week?’. All recruited participants in the present study were native Chinese speakers and right-handed. Exclusion criteria for both groups were 1) any neurological disorders; 2) any drug abuse, tobacco and alcohol intake by urine drug screening; 3) any physical illness; and 4) menstrual period or pregnancy in women; 5) any medication use during last 6 months.
Data acquisition
MR scanning was performed on a 3-T GE scanner with an eight-channel phase-array head coil at the Mental Health Center, the First Affiliated Hospital of the Medical College, Xi’an Jiaotong University. For each subject, a high-resolution structural image was acquired using a three-dimensional MRI sequence with a voxel size of 1 mm3 employing an axial fast spoiled gradient recalled sequence (data matrix, 256 × 256; field of view, 256 mm × 256 mm; TR = 1900 ms; TE = 2.26 ms). The resting-state functional images were obtained using echo planar imaging (30 contiguous slices with a slice thickness of 5 mm; flip angle, 90°; field of view, 240 mm × 240 mm; data matrix, 64 × 64; total volumes, 180; TR = 2000 ms; TE = 30 ms). During the 6 min 10s resting scan, subjects were instructed to stay awake with their eyes closed and to not think during the scan. After scanning, the subjects were asked whether they remained awake or not during the scan.
VBM analysis
An FSL-VBM protocol was employed for the structural data processing with the FMRIB Software Library (FSL) 4.1 software (http://www.fmrib.ax.ac.uk/fsl) (Smith et al. 2004). All structural images were brain-extracted with the brain extracting tool (BET) and then tissue segmented into gray matter, white matter, and cerebrospainal fluid (CSF) using the FMRIB’s automated segmentation tool (FAST) V4.1. The gray matter images were then aligned to MNI152 standard space and then followed by a nonlinear registration that employed a b-spline representation of the registration warp field. The resulting images were averaged to create a study-specific template, to which the native gray matter images were then nonlinearly re-registered. Next, the registered gray matter image was modulated by dividing the Jacobian of the warp field and smoothed with isotropic Gaussian kernels (full-width half-maximum (FWHM) = 5 mm). Permutation-based non-parametric testing with 5000 random permutations was used to build statistical maps between the IGD group and control group. Analysis of covariance (ANCOVA) was employed with age, education and gender effects as covariates (p < 0.05, FWE correction). The correlation analysis was employed to investigate the possible relationship between the VBM findings and IAT.
Resting state functional connectivity analysis
The preprocessing steps of each subjects’ resting-state fMRI data were performed using both AFNI (Automated Functional Neuro-Imaging) (http://afni.nimh.nih.gov/afni) and FSL (for FMRIB Software Library) (http://www.fmrib.ox.ac.uk/fsl/) software. Data preprocessing consisted of the following steps: 1) The first five volumes were discarded to allow for signal stabilization, 2) slice timing and head motion correction, 3) time series de-spiking, 4) spatial smoothing with an isotropic Gaussian kernel (6 mm FWHM), 5) intensity normalization, 6) band-pass filtering (0.01Hz-0.1Hz), 7) removing linear drift artifacts and high-frequency noise, 8) transformation from the individual resting-state fMRI space to the MNI152 standard space, and 9) regressing out nuisance signals (six motion parameters, global mean, white matter, and CSF signals). The white matter and CSF signals were extracted from the VBM segmentation and then calculated for regression analysis. We chose the regions of the PFC with gray matter deficits as our seeds and detected their functional connectivity employing a method based on a seeding voxel correlation approach (Yuan et al. 2010a). For each cortical regions generated by VBM analysis, a 6 mm radius sphere was drawn choosing the peak t-value voxels as the center. The white matter voxels were removed and then the averaged fMRI time series for total gray matter voxels of the cortical regions with structural deficits was considered as the seeding reference time series. Correlation analyses were performed between the seeds and the rest of the brain in a voxel-wise measure and the resultant r value maps were transformed to approximate Gaussian distribution with a Fisher’s z transformation. A two independent-sample t test was employed to detect the comparison of the z value map between the IGD group and control group controlling for age, education and gender effects. To investigate the possible effect of structural abnormalities on the resting state results, for each seed, we additionally included the gray matter deficits as the covariate in the two-sample t test of resting state functional connevtivity analysis.
Correlation analysis
To investigate the association between the resting state functional connectivity findings of these regions and IGD, regression analysis was employed to calculate the correlation coefficients between the functional connectivity and the internet activity behavioral measurements in the Table 1, including age, gender and education as covariates. The relationship between the decreased gray matter of the PFC regions and reduced frontostriatal circuits functional connectivity were also assessed in IGD.
Results
VBM results
Compared with healthy controls, IGD subjects showed significant decreased gray matter volume in the frontal regions including the bilateral DLPFC, OFC, ACC, the right SMA and cerebellum after controlling for age and gender effects (p < 0.05, FWE corrected) (Table 2). No regions showed higher gray matter volume than healthy controls (Fig. 1). No significant correlation was found between the gray matter volume of any area and IAT.

VBM results. reduced gray matter volume in IGD subjects, (1-p) corrected p-value images (p < 0.05, FWE corrected)
Resting-state results
According to the VBM results in the present study, we chose seven regions including the bilateral DLPFC, OFC, ACC and the right SMA as our seed region. Compared with healthy controls, IGD subjects showed decreased functional connectivity between several regions and our seeds. No regions showed significant increased functional connectivity with our seeds in IGD subjects. Significant resting state functional connectivity analysis differences of each seed regions between the two groups were described as the following (Figs. 2 and 3).

One sample t test for functional connectivity analysis of seed regions. (p < 0.05, FWE corrected)

Functional analysis results. Reduced functional connectivities of the seven seeds during the resting state of subjects with IGD and healthy controls (p < 0.05, FWE corrected)
ACC
Significant decreased functional connectivity of the left ACC was observed in the bilateral pallidum, thalamus, right caudate, and putamen in IGD subjects.
Significant decreased functional connectivity of the right ACC was observed in the bilateral pallidum, putamen, thalamus, right caudate, and SMA.
OFC
Significant decreased functional connectivity of the left OFC was observed in the bilateral caudate and thalamus in IGD subjects.
Significant decreased functional connectivity of the right OFC was observed in the bilateral caudate, thalamus and the right pallidum in IGD subjects.
DLPFC
Significant decreased functional connectivity of the left DLPFC was observed in the bilateral pallidum, thalamus, right caudate, and occipital lobe in IGD subjects.
Significant decreased functional connectivity of the right DLPFC was observed in the bilateral thalamus and temporal lobe in IGD subjects.
SMA
Significant decreased functional connectivity between several regions and the rSMA was found in IGD subjects, including the bilateral caudate, thalamus, putamen, and insular cortex.
It is worthy to note that similar results were observed when considered the gray matter deficits as the covariate, which suggested that the functional connectivity results were independent of the altered brain volume in the current study.
Correlation results
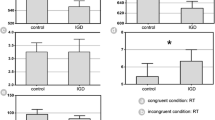
The functional connectivity between right ACC and left putamen (r = −0.6068, p = 0.0013), left OFC and left caudate (r = −0.5263, p = 0.0069), left DLPFC and left pallidum (r =−0.6712, p = 0.0002) were negatively correlated with the IAT scores of the IGD subjects after FWE corrections for multiple comparasions (Fig. 4). No significant correlations were detected in controls. We found no significant correlation between the VBM findings and resting state functional connectivity results.

Correlation analysis results. Negative correlations between abnormal functional connectivities and IAT scores in the IGD group. The r and p-values represent the peak correlation
Discussion
IGD is newly considered as a serious public concern and is soon to be prevalent all over the world, especially east Asia (Dimitri et al. 2011; Young 1998b; Durkee et al. 2012; Cao et al. 2011; Kim et al. 2011). Data from the China Youth Internet Association (announcement on February 2, 2010) demonstrated that about 14 % of Chinese urban youths is suffering internet addiction now (http://www.zqwx.youth.cn/). IGD is soon becoming a common mental health problem among Chinese adolescents, and it seriously affects the individual’s psychological well-being, as well as academic and work performance (Young 1998b). What’s more, in the latest edition, DSM-5, IGD is recommended as an area that needs further study. In the present study, by combining VBM and resting state functional connectivity, we revealed both structural and functional abnormalities in several PFC regions in subjects with IGD and further investigated the associations between the functional abnormalities and the severity of IGD. Our results suggested the involvement of PFC in the underlying pathology of IGD and provided a possible target for the treatment of IGD.
Consistent with our previous study (Yuan et al. 2011), decreased grey matter volume in bilateral ACC, OFC, DLPFC and the rSMA were found in IGD subjects after controlling age and gender effects in the present study. Also, we found significant decreased functional connectivities between our seeds and the temporal and occipital regions. More importantly, we detected a significant dysfunction in the PFC regions that involved some important prefrontal-striatal circuits, passing through the pallidum and thalamus, i.e., the ACC-striatal, OFC-striatal and DLPFC-striatal circuits. These circuits were firstly reported in PET studies of substance-dependent subjects, such as cocaine (Volkow et al. 1993), alcohol (Volkow et al. 2006), and even obese subjects (Volkow et al. 2008). These studies demonstrated that impaired dopamine (DA) function in the striatum was associated with reduced baseline glucose metabolism in the frontal cortex regions. Later, functional connectivity studies also detected abnormal connectivities in drug abusers and obese subjects and suggested abnormal connectivity between PFC and striatal regions which might underlie the pathological states in drug addiction (Hanlon et al. 2011). In a previous review, Volkow et al. put forward several unbalanced neuronal circuits in drug addicted subjects including several prefrontal-striatal circuits which may reflect observable behaviors that characterize the addiction (compulsive drug consumption, impaired self-control, and behavioral inflexibility) (Volkow et al. 2013). Our results suggested that changes in these circuits found in substance-dependent subjects were also observed in people with IGD. Dysfunction of these prefrontal-striatal circuits in the IGD group may be a possible underlying mechanism of their addictive behaviors that are similar to drug abuse.
The ACC-striatal circuit
The projection from the ACC to the ventral striatum through the pallidum and thalamus, which is defined as the ACC-striatal circuit, is associated with some cognitive control processes, such as error and conflict detection and urgent inhibition control (Feil et al. 2010). The involvement of the ACC in some cognitive control tasks have already been demonstrated in both substance abuse subjects and internet addicts (Forman et al. 2004; Dong et al. 2010). In addition, the ACC is related to craving for drugs and online gaming cues (Ko et al. 2011; Zhang et al. 2011) and contributes to estimating whether behavioral responses should be emitted and the intensity of those responses (Kalivas and Volkow 2005). Therefore, the ACC-striatal circuits play an important role in the assessment of consequences and error detection in addictive behaviors (Volkow et al. 2013). Our functional results suggested dysfunction of the ACC circuit including the pallidum, thalamus and the dorsal but not the ventral striatum (caudate and putamen), which is, at least partially related to the theory mentioned above. Similar results have been found in smokers (Hong et al. 2009), and this may be caused by the progression of the addiction. Addiction was thought to be related to the initial ACC control over the ventral striatum, which as the processes continued, were replaced by dorsal striatal activity which was habit driven (Everitt and Robbins 2005). Our results revealed abnormalities of these circuits during the resting state and the correlation results suggested the severity of IGD may be modulated by these circuits.
The OFC-striatal circuit
The OFC is an important part of the prefrontal cortex and is connected to some striatal regions including the caudate and nucleus accumbens, which associate the OFC with reward function (Schoenbaum et al. 2006). What’s more, the OFC-striatal circuit is highly involved in decision making and regulation of impulsivity (Volkow et al. 2013). Dysfunction of this circuit was widely reported in substance-dependent individuals and was considered important in perceiving outcomes in guiding decision-making and subsequent behaviors (Tanabe et al. 2009; Feil et al. 2010). Similar to substance addicts, adolescents with IGD also exhibited behaviors caused by degraded performance in decision-making, i.e., constant compulsive internet seeking behaviors despite of their awareness of negative outcomes (Yuan et al. 2013a). Otherwise, the OFC circuits play an important role in impulse inhibition during the Go/No-Go task (Horn et al. 2003), in which subjects with IGD have worse performance than the controls (Dong et al. 2010). Our functional connectivity results of the OFC circuit suggested a possible underlying mechanism of this impaired cognitive behavioral performance and the correlation results implied that there was a potential relationship between the degree of dysfunction and the severity of IGD.
The DLPFC-striatal circuit
The DLPFC circuit plays a complex role in several dimensions such as planning, organization, set shifting and attention (Feil et al. 2010). It is usually involved in cognitive inhibitory tasks and updating and selecting information appropriate for the tasks (Blasi et al. 2006; Bunge et al. 2001). What’s more, one thing to be noted is that the DLPFC is repeatedly reported to be related to cue-induced craving in both substance and behavior addiction disorders (Ko et al. 2011; Kober et al. 2010; Crockford et al. 2005; Ko et al. 2012). Ko et al. reported activation of the DLPFC for gaming cues and suggested its role in making plans to go gaming (Ko et al. 2011). Later, Kober et al. further demonstrated involvement of the DLPFC–striatal pathway in effective regulation of craving in smokers and suggested its role in neural dynamics parallel to those involved in regulating other emotions (Kober et al. 2010). In conclusion, Feil et al. put forward a theory that this circuit could contribute to regulating the integration and selection of both cognitive and goal-motivated behavior (Feil et al. 2010). Thus, our results suggested that the dysfunction of this circuit at the resting state and the correlation with the severity might be related to improper behavioral choices such as seeking internet use regardless of the negative outcomes.
SMA-related circuits
In the present study, we found decreased functional connectivity between several subcortical regions and the rSMA in IGD subjects, including the bilateral caudate, pallidum, thalamus, and putamen. Our results suggested that the SMA seems to be a potential important region in addictive behaviors. In a recent review, Volkow et al. suggested its involvement in an inferior frontal gyrus (IFG) circuit which is associated with conflict resolution and response inhibition (Volkow et al. 2013), together with the caudate, pallidum, thalamus and IFG. Furthermore, the SMA is the output of the hyperdirect dopaminergic pathways between the IFG and the thalamus (from SMA into the pallidum) by which basal ganglia modulate other frontal-subcortical circuits (Feil et al. 2010). Dysfunction of this circuit in individuals with IGD will affect their reward-related dopaminergic nervous systems. In addition, we also detected abnormal functional connectivities between the right SMA and the insular cortex. These two regions were included in an important resting state network—the salience network which regulates the function of other networks when rapid changes in behavior are required (Bonnelle et al. 2012). In conclusion, our results revealed significant abnormality in the functional connectivity of the SMA-related circuits which may affect other brain networks.
It is worthy to note that the main findings in current study were located within the frontostriatal circuits. More importantly, correlation analysis demonstrated that the abnormal resting state functional connectivity within frontostriatal circuits, i.e., right ACC - left putamen, left OFC - left caudate, left DLPFC - left pallidum, were associated with their severity measured by IAT score in IGD group. The implication of frontostriatal circuits with addiction had been revealed and its association with addiction severity had already been detected in smokers (Zhang et al. 2011). Here we extend the frontostriatal circuits abnormities to the IGD by showing its resting state functional connectivity correlation with IAT. Therefore, we suggested that neuronal activity changes during the resting state within frontostriatal circuits may be a biomarker of severity of IGD. Additionally, more and more evidence revealed the critical roles of the frontostriatal circuits during cognitive control (Liston et al. 2006). Regardless of whether IGD is conceptualized as a behavioral addiction, it is speculated to be associated with impaired cognitive control (Yuan et al. 2013b, 2015; Xing et al. 2014). Rationally, we suggested that the frontostriatal circuits resting state functional connectivity abnormalities might be associated with the cognitive control deficits in IGD. Evidently, the more accurate roles of frontostriatal circuits in IGD should be investigated by more comprehensive experiment design in the future.
Limitations
The present study employed a cross-sectional design and the question arises whether these differences were a consequence or precondition of IGD. Whether it is pre-existing and pre-disposing to IGD or whether IGD alters brain structure can not be solved in the current study. In contrast with the substance abuse disorder, animal studies had found that drugs produce toxicity through chemical effects that in turn cause reduced brain grey matter (Goldstein and Volkow 2002). However, this mechanism would not appear to be operating in behavioral addictions. The relationship between the VBM and RSFC findings was also assessed in the current study. No significant Pearson correlation was detected. Additionally, we controlled the structural deficits when comparing the RSFC abnormalities. Similar results were observed, which demonstrated that the functional connectivity results were independent of the altered brain volume in the current study. However, we should not avoid the possibility that some complicated mechanisms exist in the coupling of the structural and functional findings in the current study. Motion artifacts would influence resting state connectivity results, although we including motion parameters as covariates. Due to the large number of seed regions, some consideration should be provided (e.g., Bonferroni corrections) for the resting state results in the future. Therefore, the results should be explained with caution. More comprehensive and imaging methods are necessary to investigate these issues.
Conclusion
Taken together, the present study detected abnormal structural deficits in several PFC regions and dysfunctional prefrontal-striatal networks in IGD. We observed extensive abnormal prefrontal-striatal circuits in people with IGD, which were associated with the severity. Our results revealed the involvement of several PFC regions in the process of IGD and suggested IGD may share a similar neural mechanism with substance dependence at the circuit level. Further studies will investigate structural connections with behavioral performances of cognitive tasks in subjects with IGD.
References
Barke, A., Nyenhuis, N., & Kröner-Herwig, B. (2012). The German version of the internet addiction test: a validation study. Cyberpsychology, Behavior and Social Networking, 15(10), 534–542.
Blasi, G., Goldberg, T. E., Weickert, T., Das, S., Kohn, P., Zoltick, B., et al. (2006). Brain regions underlying response inhibition and interference monitoring and suppression. European Journal of Neuroscience, 23(6), 1658–1664.
Bonnelle, V., Ham, T. E., Leech, R., Kinnunen, K. M., Mehta, M. A., Greenwood, R. J., et al. (2012). Salience network integrity predicts default mode network function after traumatic brain injury. Proceedings of the National Academy of Sciences, 109(12), 4690–4695.
Bremer, J. (2005). The internet and children: advantages and disadvantages. Child and Adolescent Psychiatric Clinics of North America, 14(3), 405.
Brier, M. R., Thomas, J. B., Snyder, A. Z., Benzinger, T. L., Zhang, D., Raichle, M. E., et al. (2012). Loss of intranetwork and internetwork resting state functional connections with Alzheimer’s disease progression. The Journal of Neuroscience, 32(26), 8890–8899.
Bunge, S. A., Ochsner, K. N., Desmond, J. E., Glover, G. H., & Gabrieli, J. D. (2001). Prefrontal regions involved in keeping information in and out of mind. Brain, 124(10), 2074–2086.
Cao, H., Sun, Y., Wan, Y., Hao, J., & Tao, F. (2011). Problematic internet use in Chinese adolescents and its relation to psychosomatic symptoms and life satisfaction. BMC Public Health, 11(1), 802.
Crockford, D. N., Goodyear, B., Edwards, J., Quickfall, J., & El-Guebaly, N. (2005). Cue-induced brain activity in pathological gamblers. Biological Psychiatry, 58(10), 787–795.
Dimitri, C., Megan, M., Lauren, J., Mon, M., & Chuan, Z. (2011) Problematic internet usage in US college students: a pilot study. BMC Medicine, 9.
Dong, G., Lu, Q., Zhou, H., & Zhao, X. (2010). Impulse inhibition in people with Internet addiction disorder: electrophysiological evidence from a Go/NoGo study. Neuroscience Letters, 485(2), 138–142.
Durkee, T., Kaess, M., Carli, V., Parzer, P., Wasserman, C., Floderus, B., et al. (2012). Prevalence of pathological internet use among adolescents in Europe: demographic and social factors. Addiction, 107(12), 2210–2222.
Everitt, B. J., & Robbins, T. W. (2005). Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nature Neuroscience, 8(11), 1481–1489.
Feil, J., Sheppard, D., Fitzgerald, P. B., Yücel, M., Lubman, D. I., & Bradshaw, J. L. (2010). Addiction, compulsive drug seeking, and the role of frontostriatal mechanisms in regulating inhibitory control. Neuroscience & Biobehavioral Reviews, 35(2), 248–275.
Forman, S. D., Dougherty, G. G., Casey, B., Siegle, G. J., Braver, T. S., Barch, D. M., et al. (2004). Opiate addicts lack error-dependent activation of rostral anterior cingulate. Biological Psychiatry, 55(5), 531–537.
Fox, M. D., & Raichle, M. E. (2007). Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nature Reviews Neuroscience, 8(9), 700–711.
Goldstein, R. Z., & Volkow, N. D. (2002). Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. American Journal of Psychiatry, 159(10), 1642–1652.
Goldstein, R. Z., & Volkow, N. D. (2011). Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nature Reviews Neuroscience, 12(11), 652–669.
Grant, J. E., Potenza, M. N., Weinstein, A., & Gorelick, D. A. (2010). Introduction to behavioral addictions. The American Journal of Drug and Alcohol Abuse, 36(5), 233–241.
Hanlon, C. A., Wesley, M. J., Stapleton, J. R., Laurienti, P. J., & Porrino, L. J. (2011). The association between frontal–striatal connectivity and sensorimotor control in cocaine users. Drug and Alcohol Dependence, 115(3), 240–243.
Hong, L. E., Gu, H., Yang, Y., Ross, T. J., Salmeron, B. J., Buchholz, B., et al. (2009). Association of nicotine addiction and nicotine’s actions with separate cingulate cortex functional circuits. Archives of General Psychiatry, 66(4), 431–441.
Hong, S.-B., Zalesky, A., Cocchi, L., Fornito, A., Choi, E.-J., Kim, H.-H., et al. (2013). Decreased functional brain connectivity in adolescents with internet addiction. PLoS ONE, 8(2), e57831.
Horn, N., Dolan, M., Elliott, R., Deakin, J., & Woodruff, P. (2003). Response inhibition and impulsivity: an fMRI study. Neuropsychologia, 41(14), 1959–1966.
Jelenchick, L. A., Becker, T., & Moreno, M. A. (2012). Assessing the psychometric properties of the Internet Addiction Test (IAT) in US college students. Psychiatry Research, 196(2–3), 296–301.
Jin, C., Yuan, K., Zhao, L., Zhao, L., Yu, D., Deneen, K. M., et al. (2013). Structural and functional abnormalities in migraine patients without aura. NMR in Biomedicine, 26(1), 58–64.
Kalivas, P. W., & Volkow, N. D. (2005). The neural basis of addiction: a pathology of motivation and choice. American Journal of Psychiatry, 162(8), 1403–1413.
Kim, S. H., Baik, S.-H., Park, C. S., Kim, S. J., Choi, S. W., & Kim, S. E. (2011). Reduced striatal dopamine D2 receptors in people with Internet addiction. NeuroReport, 22(8), 407.
Ko, C. H., Liu, G. C., Yen, J. Y., Chen, C. Y., Yen, C. F., & Chen, C. S. (2011). Brain correlates of craving for online gaming under cue exposure in subjects with Internet gaming addiction and in remitted subjects. Addiction Biology, 18(3), 559–569.
Ko, C.-H., Liu, G.-C., Yen, J.-Y., Yen, C.-F., Chen, C.-S., & Lin, W.-C. (2012). The brain activations for both cue-induced gaming urge and smoking craving among subjects comorbid with Internet gaming addiction and nicotine dependence. Journal of Psychiatric Research, 47(4), 486–493.
Kober, H., Mende-Siedlecki, P., Kross, E. F., Weber, J., Mischel, W., Hart, C. L., et al. (2010). Prefrontal–striatal pathway underlies cognitive regulation of craving. Proceedings of the National Academy of Sciences, 107(33), 14811–14816.
Lin, F., Zhou, Y., Du, Y., Qin, L., Zhao, Z., Xu, J., et al. (2012). Abnormal white matter integrity in adolescents with Internet Addiction Disorder: a tract-based spatial statistics study. PLoS ONE, 7(1), e30253.
Liston, C., Watts, R., Tottenham, N., Davidson, M. C., Niogi, S., Ulug, A. M., et al. (2006). Frontostriatal microstructure modulates efficient recruitment of cognitive control. Cerebral Cortex, 16(4), 553–560.
Meda, S. A., Gill, A., Stevens, M. C., Lorenzoni, R. P., Glahn, D. C., Calhoun, V. D., et al. (2012). Differences in resting-state functional magnetic resonance imaging functional network connectivity between schizophrenia and psychotic bipolar probands and their unaffected first-degree relatives. Biological Psychiatry, 71(10), 881–889.
Pine, D., Cohen, P., & Brook, J. (2001). Emotional reactivity and risk for psychopathology among adolescents. CNS Spectrums, 6(1), 27.
Romano, M., Osborne, L. A., Truzoli, R., & Reed, P. (2013). Differential psychological impact of internet exposure on internet addicts. PLoS ONE, 8(2), e55162.
Schoenbaum, G., Roesch, M. R., & Stalnaker, T. A. (2006). Orbitofrontal cortex, decision-making and drug addiction. Trends in Neurosciences, 29(2), 116–124.
Seeley, W. W., Crawford, R. K., Zhou, J., Miller, B. L., & Greicius, M. D. (2009). Neurodegenerative diseases target large-scale human brain networks. Neuron, 62(1), 42.
Silveri, M. M., Tzilos, G. K., Pimentel, P. J., & Yurgelun‐Todd, D. A. (2004). Trajectories of adolescent emotional and cognitive development: effects of sex and risk for drug use. Annals of the New York Academy of Sciences, 1021(1), 363–370.
Smith, S. M., Jenkinson, M., Woolrich, M. W., Beckmann, C. F., Behrens, T., Johansen-Berg, H., et al. (2004). Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage, 23, S208.
Steinberg, L. (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74.
Tanabe, J., Tregellas, J. R., Dalwani, M., Thompson, L., Owens, E., Crowley, T., et al. (2009). Medial orbitofrontal cortex gray matter is reduced in abstinent substance-dependent individuals. Biological Psychiatry, 65(2), 160–164.
Volkow, N. D., Fowler, J. S., Wang, G. J., Hitzemann, R., Logan, J., Schlyer, D. J., et al. (1993). Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse, 14(2), 169–177.
Volkow, N. D., Wang, G.-J., Begleiter, H., Porjesz, B., Fowler, J. S., Telang, F., et al. (2006). High levels of dopamine D2 receptors in unaffected members of alcoholic families: possible protective factors. Archives of General Psychiatry, 63(9), 999.
Volkow, N. D., Wang, G.-J., Telang, F., Fowler, J. S., Thanos, P. K., Logan, J., et al. (2008). Low dopamine striatal D2 receptors are associated with prefrontal metabolism in obese subjects: possible contributing factors. NeuroImage, 42(4), 1537–1543.
Volkow, N., Fowler, J., Wang, G., Baler, R., & Telang, F. (2009). Imaging dopamine’s role in drug abuse and addiction. Neuropharmacology, 56, 3–8.
Volkow, N. D., Wang, G.-J., Tomasi, D., & Baler, R. D. (2013). Unbalanced neuronal circuits in addiction. Current Opinion in Neurobiology, 23(4), 639–648.
Winkler, A., Dörsing, B., Rief, W., Shen, Y., & Glombiewski, J. A. (2013). Treatment of internet addiction: a meta-analysis. Clinical Psychology Review, 33(2), 317–329.
Xing, L., Yuan, K., Bi, Y., Yin, J., Cai, C., Feng, D., et al. (2014). Reduced fiber integrity and cognitive control in adolescents with internet gaming disorder. Brain Research, 1586, 109–117.
Xue, T., Yuan, K., Zhao, L., Yu, D., Zhao, L., Dong, T., et al. (2012). Intrinsic brain network abnormalities in migraines without aura revealed in resting-state fMRI. PLoS ONE, 7(12), e52927.
Young, K. S. (1998a). Caught in the net: How to recognize the signs of internet addiction--and a winning strategy for recovery. New York: Wiley.
Young, K. S. (1998b). Internet addiction: the emergence of a new clinical disorder. CyberPsychology & Behavior, 1(3), 237–244.
Yu, D., Yuan, K., Zhao, L., Zhao, L., Dong, M., Liu, P., et al. (2012). Regional homogeneity abnormalities in patients with interictal migraine without aura: a resting‐state study. NMR in Biomedicine, 25(5), 806–812.
Yuan, K., Qin, W., Dong, M., Liu, J., Sun, J., Liu, P., et al. (2010a). Gray matter deficits and resting-state abnormalities in abstinent heroin-dependent individuals. Neuroscience Letters, 482(2), 101–105.
Yuan, K., Qin, W., Liu, J., Guo, Q., Dong, M., Sun, J., et al. (2010b). Altered small-world brain functional networks and duration of heroin use in male abstinent heroin-dependent individuals. Neuroscience Letters, 477(1), 37–42.
Yuan, K., Qin, W., Wang, G., Zeng, F., Zhao, L., Yang, X., et al. (2011). Microstructure abnormalities in adolescents with internet addiction disorder. PLoS ONE, 6(6), e20708.
Yuan, K., Cheng, P., Dong, T., Bi, Y., Xing, L., Yu, D., et al. (2013a). Cortical thickness abnormalities in late adolescence with online gaming addiction. PLoS ONE, 8(1), e53055.
Yuan, K., Jin, C., Cheng, P., Yang, X., Dong, T., Bi, Y., et al. (2013b). Amplitude of low frequency fluctuation abnormalities in adolescents with online gaming addiction. PLoS ONE, 8(11), e78708.
Yuan, K., Qin, W., Yu, D., Bi, Y., Xing, L., Jin, C., et al. (2015). Core brain networks interactions and cognitive control in internet gaming disorder individuals in late adolescence/early adulthood. Brain Structure and Function. doi:10.1007/s00429-014-0982-7.
Zhang, X., Salmeron, B. J., Ross, T. J., Gu, H., Geng, X., Yang, Y., et al. (2011). Anatomical differences and network characteristics underlying smoking cue reactivity. NeuroImage, 54(1), 131–141.
Zhou, Z., Yuan, G., & Yao, J. (2012). Cognitive biases toward internet game-related pictures and executive deficits in individuals with an internet game addiction. PLoS ONE, 7(11), e48961.
Acknowledgments
This paper is supported by the Project for the National Key Basic Research and Development Program (973) under Grant nos. 2014CB543203, 2011CB707700, 2012CB518501, the National Natural Science Foundation of China under Grant nos. 81401478, 81401488, 81227901, 81271644, 81271546, 81101036, 81101108, 31200837, 81301281, the Natural Science Basic Research Plan in Shaanxi Province of China under Grant no. 2014JQ4118, and the Fundamental Research Funds for the Central Universities under the Grant nos. 8002-72125760, 8002-72135767, 8002-72145760, the Natural Science Foundation of Inner Mongolia under Grant no. 2012MS0908. General Financial Grant the China Post- doctoral Science Foundation under Grant no. 2014 M552416. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Chenwang Jin and Ting Zhang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Jin, C., Zhang, T., Cai, C. et al. Abnormal prefrontal cortex resting state functional connectivity and severity of internet gaming disorder. Brain Imaging and Behavior 10, 719–729 (2016). https://doi.org/10.1007/s11682-015-9439-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11682-015-9439-8